

Skin nonmelanocytic tumor
Carcinoma (nonadnexal)
Keratoacanthoma / SCC keratoacanthoma type
Authors: Mary Dick, M.D., Poonam Sharma, M.B.B.S.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 7 June 2021
Last staff update: 22 September 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Keratoacanthoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Dick M, Sharma P. Keratoacanthoma / SCC keratoacanthoma type. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocytickeratoacanthoma.html. Accessed May 2nd, 2024.
Definition / general
- Keratoacanthoma (KA) is a well differentiated, cutaneous squamous cell carcinoma, which often spontaneously regresses
- Regression is thought to be due to immune mediated destruction of squamous cells
- For lesions that are entirely resected, can diagnose as "well differentiated squamous cell carcinoma, keratoacanthoma type”
- For lesions that are not entirely histologically examined, can diagnose as "well differentiated squamous cell carcinoma with features of keratoacanthoma”
Essential features
- Common, represents approximately up to 30% of cases of cutaneous squamous cell carcinoma (SCC)
- Dome shaped tumor with central keratinous plug in sun exposed areas
- May become large, up to 10 cm (called giant KA)
- Good prognosis; vast majority of cases spontaneously regress
Terminology
- Agglomerate KA (variant)
- KA centrifugum (variant)
- Giant KA (variant)
- Subungual KA (variant)
- Intraoral KA (variant)
ICD coding
Epidemiology
- Older adults, mean age mid 60s (Indian J Dermatol 2011;56:435)
- M:F = 3:1 (Indian J Dermatol 2011;56:435)
Sites
- Head and neck most common sites, followed by extremities (Open Access Maced J Med Sci 2018;6:531)
Pathophysiology
- Tumor stems from follicular infundibulum related to chronic solar (UV) damage (Indian J Dermatol 2011;56:435)
- Undergoes 3 clinical stages: proliferative, mature, involutional / resolving (Arch Craniofac Surg 2015;16:92)
Clinical features
- Typically solitary but may present with multiple tumors (Acta Biomed 2019;90:580)
Diagnosis
- Excisional biopsy preferred to show suggestive histopathology
Prognostic factors
- Nonfatal tumor
- Can regress; however, final size prior to regression is difficult to predict (J Am Acad Dermatol 2016;74:1220)
- Recurrence is uncommon with surgical removal
- Self limited proliferation with low probability of malignant transformation (more often associated with perineural invasion) (Acta Biomed 2019;90:580)
Case reports
- 34 year old woman with rapidly growing conjunctival mass (Rev Hosp Clin Fac Med Sao Paulo 2004;59:135)
- 56 year old man with giant variant keratoacanthoma of the cheek (Arch Craniofac Surg 2015;16:92)
- 61 year old man with rapidly occurring forearm keratoacanthoma over 11 days (Cutis 2015;95:E7)
- 74 year old man with keratoacanthoma of the palm (Cureus 2018;10:e2331)
- 79 year old man with keratoacanthoma of the forehead with venous invasion (Dermatol Pract Concept 2012;2:204a03)
- 92 year old man with keratoacanthoma of the left cheek with perineural invasion (Acta Biomed 2019;90:580)
Treatment
- Monitoring for spontaneous regression; often leaves atrophic hypopigmented scar (Indian J Dermatol 2011;56:435)
- Typically treated with complete surgical excision; Mohs surgery performed dependent on location (Ann Dermatol 2011;23:357)
- Electrosurgery, cryosurgery, laser surgery, systemic or topical chemotherapy occasionally utilized (J Dent (Shiraz) 2014;15:91)
- Radiotherapy can be utilized with reoccurrence or potential large cosmetic disfigurement with surgery; typically not utilized in young adult patients (J Am Acad Dermatol 1990;23:489)
Clinical images
Images hosted on other servers:

Large face tumor

Palm tumor

Forehead lesion
Gross description
- Typically large, scaly, dome shaped tumor with central keratinous plug
Microscopic (histologic) description
- Low power magnification shows large, well differentiated squamous tumor with central keratin filled crater
- Surrounding epidermis forms a lip around the invaginating crateriform tumor
- Tumor is composed of bland squamous cells with abundant eosinophilic or glassy cytoplasm and enlarged hyperchromatic to vesicular appearing nuclei
- Mitotic activity and cellular atypia are usually seen at the periphery of tumor
- Intraepidermal neutrophilic microabscesses and keratin horn pearls are seen within the tumor
- Regressing tumors show epidermal atrophy, bland cytologic features, dermal inflammation and fibrosis at the periphery of tumor
Microscopic (histologic) images
Contributed by Poonam Sharma, M.B.B.S.
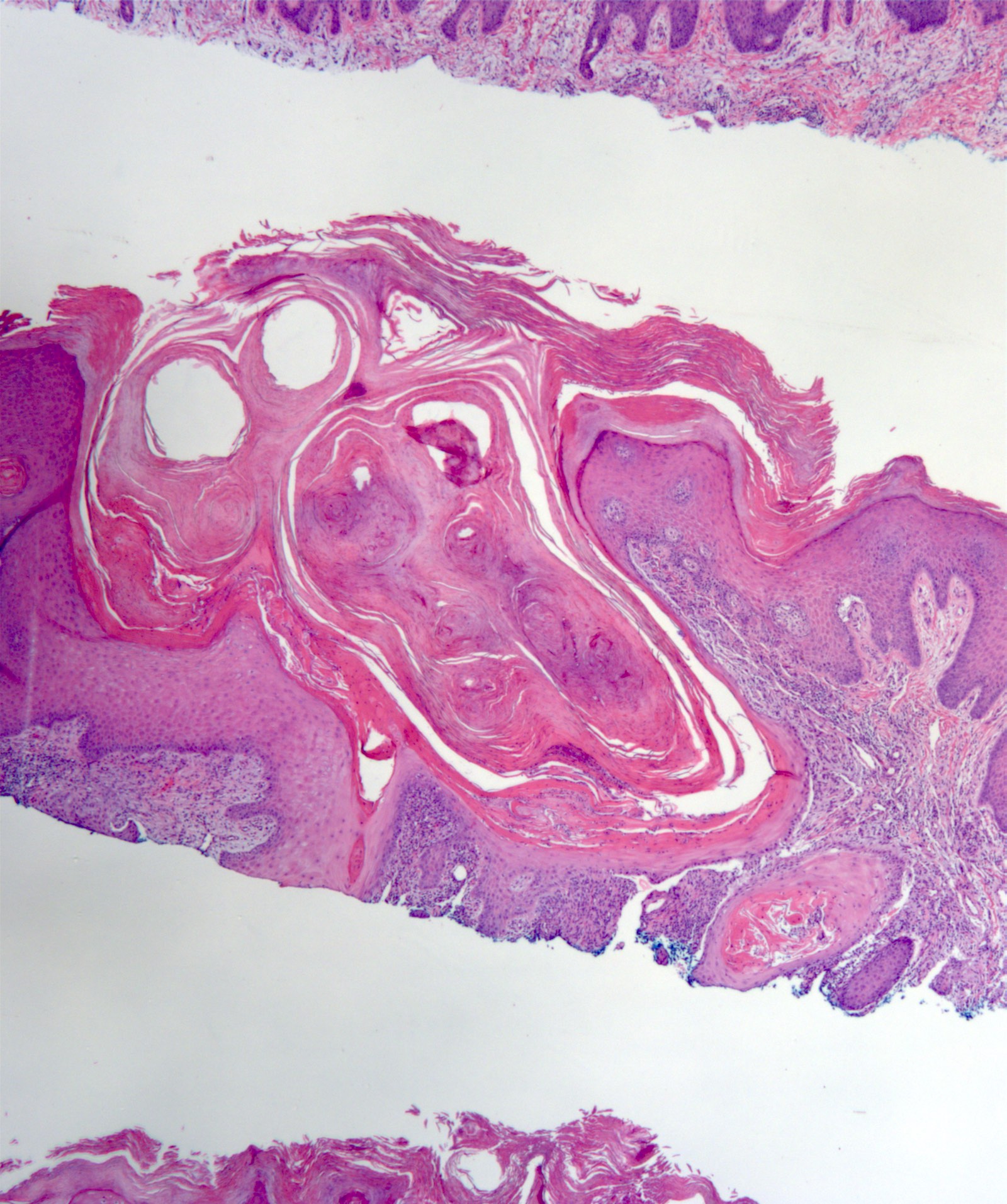
Central crater
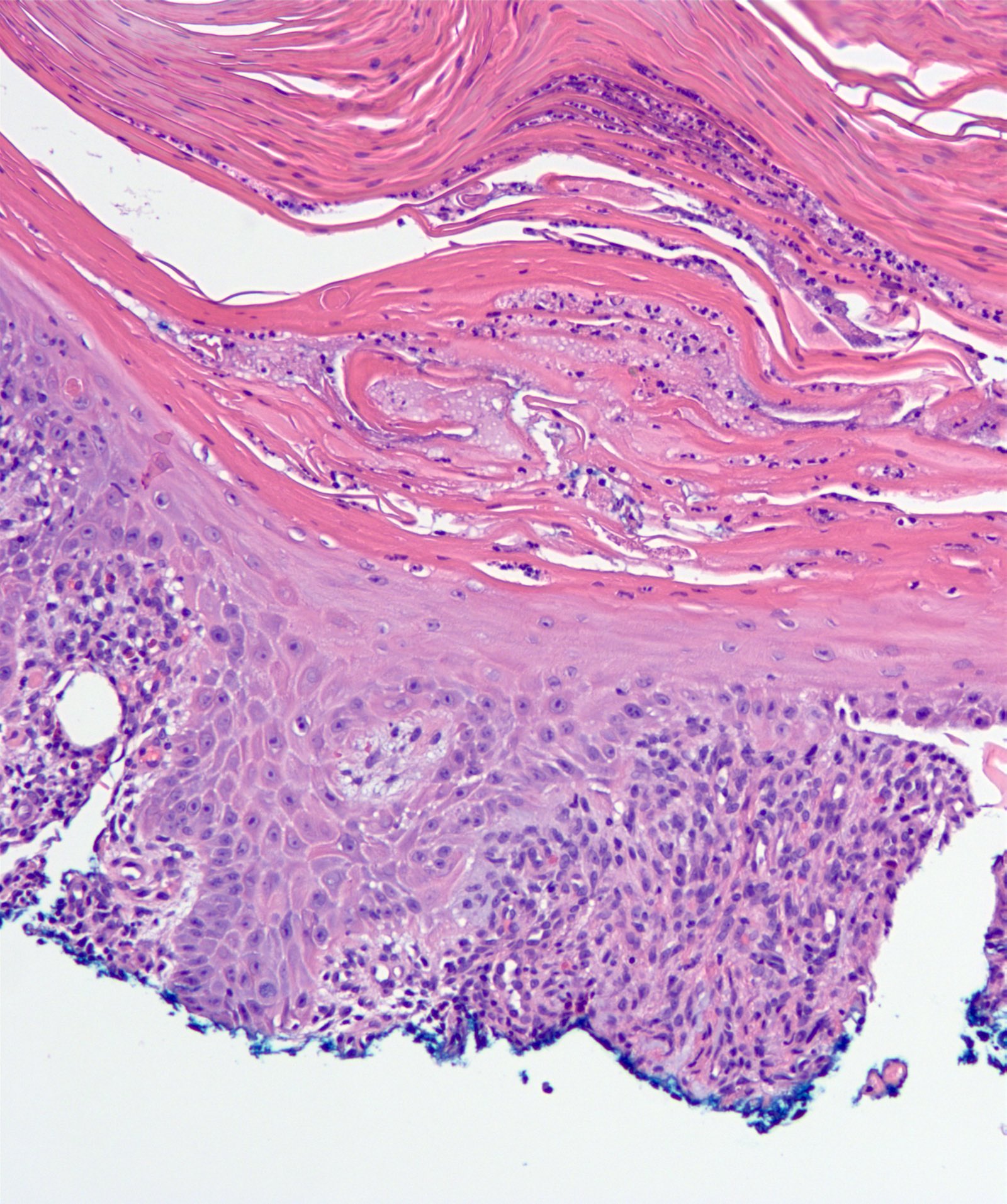
Bland squamous cells
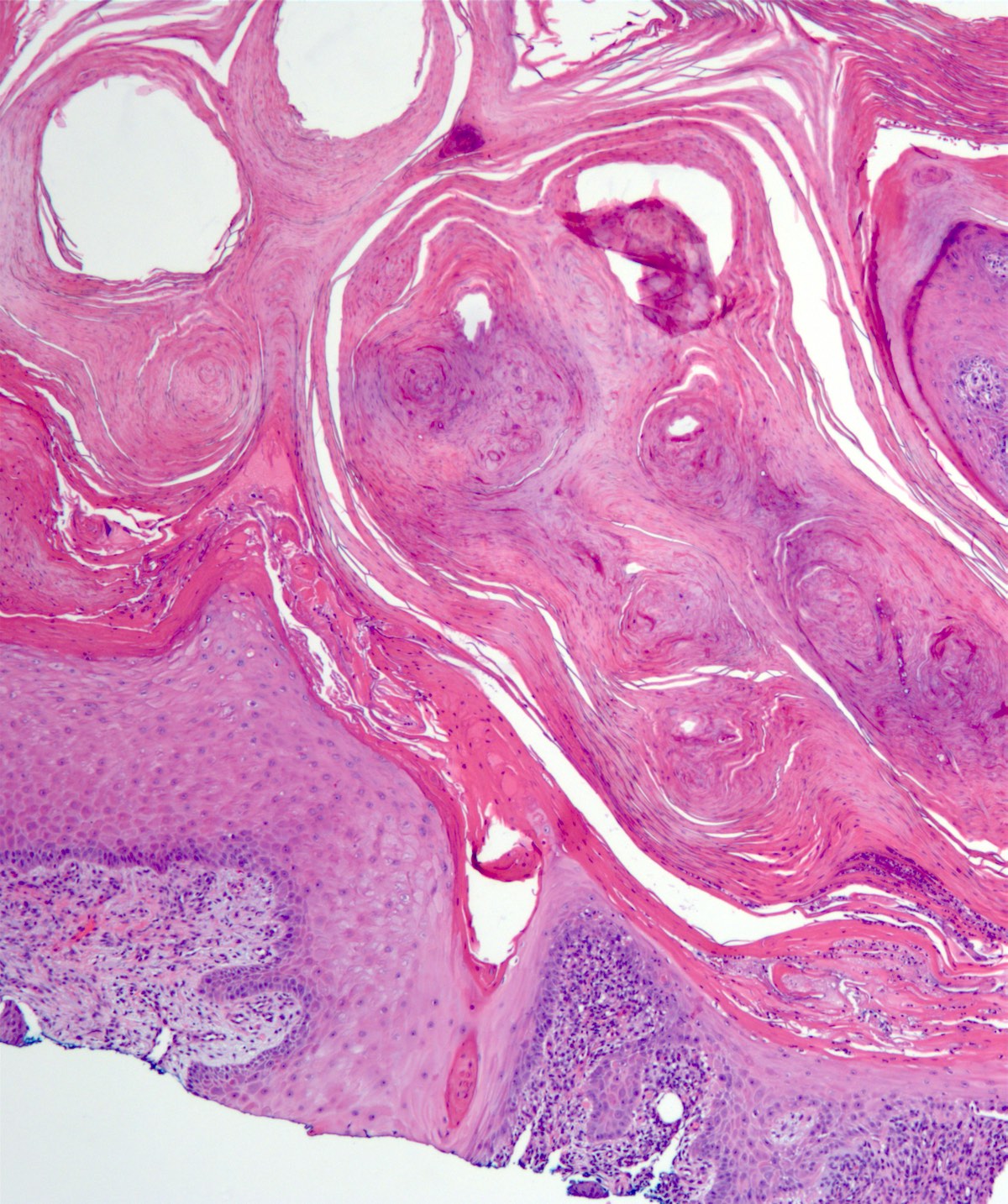
Whorl of laminated keratin
Virtual slides
Images hosted on other servers:

Invaginated, keratin filled tumor
Positive stains
- Ki67 in tumor lobule basal cells (Oncol Lett 2017;13:2539)
- CK17 in the suprabasal cells with central staining pattern (Oncol Lett 2017;13:2539)
- PAS in outer root sheath of hair follicle and epithelial tumor cells (Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119:310)
- CK6 and CK10 in tumor islands (Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119:310)
- CK14 epithelial basal layer (Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119:310)
- CK10 spinous and granular layers (Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119:310)
Negative stains
- Ki67 in suprabasal cells (Oncol Lett 2017;13:2539)
- CK17 weak / negative in tumor lobules (Oncol Lett 2017;13:2539)
Molecular / cytogenetics description
- Transforming growth factor beta receptor 1 can cause multiple self healing squamous epithelioma (MMSE); most common cause of multiple KA
- Germline mutations of hMSH2 and hMLH1 mismatch repair genes causing Muir-Torre syndrome have been implicated in solitary and multiple KA formation
- BRAF kinase inhibitors utilized to treat KA has been reported to induce reactive KA by paradoxical activation of the ERK MAPkinase pathway
- Reference: Exp Dermatol 2016;25:85
Videos
Keratoacanthoma
Sample pathology report
- Skin, left cheek (clinical keratoacanthoma), excision:
- Well differentiated squamous cell carcinoma, keratoacanthoma type (see comment)
- Comment: Well differentiated hyperplastic squamous epithelium with crater-like depression with keratin horn pearls present centrally. Enlarged hyperchromatic vesicular nuclei present along with glassy appearing cytoplasm.
Differential diagnosis
- Conventional, well differentiated squamous cell carcinoma:
- Shows greater cellular atypia and mitotic activity
- Intraepidermal neutrophilic microabscesses and tissue eosinophilia less common
- May be difficult to distinguish in superficial biopsies
- Verrucous carcinoma:
- Shows prominent endophytic and exophytic growth
- Lacks central crateriform architecture
- Also has bland cytologic features
- May be difficult to distinguish in superficial biopsies
Board review style question #1
A 62 year old man presents with a single, solitary, skin colored tumor that has a crater-like appearance with central keratin buildup on his left forearm. It appeared spontaneously and has grown rapidly over the past 3 weeks. It is painless to the touch but is cosmetically displeasing. He has no other skin conditions. The tumor is excised and a microscopic image is shown above. Which of the following is true concerning this skin lesion?
- It is a variant of basal cell carcinoma
- The underlying cause for this tumor is typically due to a genetic mutation
- The malignant potential of this tumor is high and it must be removed immediately
- This tumor has the potential to completely spontaneously regress
Board review style answer #1
D. This tumor has the potential to completely spontaneously regress. This is a well differentiated squamous cell carcinoma, keratoacanthoma type.
Comment Here
Reference: Keratoacanthoma
Comment Here
Reference: Keratoacanthoma
Board review style question #2
A 70 year old male farmer presents with a skin tumor on his cheek that has grown quickly over the past month. It has a crater-like appearance without arborizing telangiectasias on dermatoscopy. Biopsy shows that the tumor is mainly composed of bland squamous cells with intraepidermal neutrophilic microabscesses and keratin horn pearls under the microscope. Which of the following is true concerning this skin tumor?
- Peripheral palisading and clefting are also likely to be seen under the microscope
- It has overlapping features of squamous cell carcinoma
- Due to its rapid growth, this tumor is likely to metastasize
- Excessive UV damage plays no role in pathogenesis
Board review style answer #2
B. It has overlapping features of squamous cell carcinoma. The lesion is a keratoacanthoma.
Comment Here
Reference: Keratoacanthoma
Comment Here
Reference: Keratoacanthoma
