Colon
Noninfectious colitis
Collagenous colitis
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.


Last author update: 3 August 2020
Last staff update: 25 February 2021
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Collagenous colitis[TI] review[PT]

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Van Treeck BJ, Hagen CE. Collagenous colitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/coloncollagenous.html. Accessed October 2nd, 2025.
Definition / general
- Form of microscopic colitis clinically associated with chronic watery diarrhea and histologically characterized by colonic intraepithelial lymphocytosis, surface mucosal damage, lamina propria inflammation and a subepithelial collagen band
Essential features
- Subtype of microscopic colitis in which patients present with chronic watery diarrhea and normal or nearly normal endoscopic findings
- Pathophysiology and etiology are unclear but thought to be multifactorial with a possible luminal antigen triggering inflammation and mucosal damage in a genetically predisposed individual
- Histology is characterized by a subepithelial collagen band, intraepithelial lymphocytosis, mixed inflammation in the lamina propria and surface mucosal damage with preserved crypt architecture
ICD coding
- ICD-10: K52.831 - Collagenous colitis
Epidemiology
- Wide age range including children but typically affects adults 50 - 70 years old (Am J Gastroenterol 2017;112:78)
- Strong female predominance (F:M = 9:1) (Am J Gastroenterol 2015;110:265, Am J Gastroenterol 2017;112:78)
- Incidence is 4.14 per 100,000 person years (Am J Gastroenterol 2015;110:265)
- Possible increased prevalence in Caucasians (Am J Gastroenterol 2017;112:78)
Sites
- Colon (right > left / rectum) (Clin Gastroenterol Hepatol 2020;18:2003, Neth J Med 2005;63:137)
Pathophysiology
- Poorly understood
- Presumed mechanism includes a dysregulated immune reaction to an unknown luminal antigen (medication, dietary factor, infectious agent, other) in a genetically predisposed individual (Lancet Gastroenterol Hepatol 2019;4:305)
- Watery diarrhea is a result of inhibited sodium channel upregulation, downregulation of tight junctions and colonocyte aquaporins and bile acid malabsorption (Lancet Gastroenterol Hepatol 2019;4:305)
Etiology
- Strong association with certain medications
- NSAIDs, aspirin, proton pump inhibitors, H2 receptor antagonists, selective serotonin reuptake inhibitors, among others (Am J Gastroenterol 2017;112:78)
- Other specific etiologies are unknown
Clinical features
- Symptoms include chronic or intermittent watery diarrhea, abdominal pain, weight loss, arthralgias, myalgias, fecal urgency, incontinence and fatigue (Am J Gastroenterol 2017;112:78, Frontline Gastroenterol 2019;10:388)
- Colonoscopy is normal or has mild nonspecific findings such as erythema or edema
- Rarely, mucosal tears or perforation can occur during endoscopy, likely as a result of decreased colonic wall compliance (Dig Liver Dis 2017;49:1073)
- Association with other autoimmune diseases (Lancet Gastroenterol Hepatol 2019;4:305, Am J Gastroenterol 2017;112:78, Frontline Gastroenterol 2019;10:388):
- 4.3% of patients with celiac disease also have microscopic colitis
- Also associated with type 1 diabetes, psoriasis and autoimmune thyroiditis
- Smoking is a risk factor (Scand J Gastroenterol 2011;46:1334, Frontline Gastroenterol 2019;10:388)
Diagnosis
- Colonoscopy with colon biopsies are required for diagnosis
- At least 2 biopsies from the ascending, transverse, descending and sigmoid colon are recommended due to patchy involvement of the colon (Am J Gastroenterol 2009;104:774, Am J Gastroenterol 2017;112:78)
Prognostic factors
- Symptomatic remission ranges from 2 - 92% (Am J Gastroenterol 2017;112:78)
- Spontaneous remission may occur in up to 15% of patients (Am J Gastroenterol 1997;92:57)
- If remission is achieved, repeat colonoscopy with biopsy not usually necessary (Frontline Gastroenterol 2019;10:388)
- No increased risk of colorectal adenocarcinoma (J Clin Med 2019;8:1942)
Case reports
- 49 and 61 year old women with collagenous colitis occurring in the setting of inflammatory bowel disease (Gastroenterol Rep (Oxf) 2019;7:218)
- 68 year old woman with melanoma and anti-PD1 induced collagenous colitis (Melanoma Res 2016;26:308)
- 72 year old man with pseudomembranous collagenous colitis (ACG Case Rep J 2016;3:e187)
- 80 year old woman presenting with spontaneous colon perforation in the setting of collagenous colitis (BMC Gastroenterol 2016;16:124)
Treatment
- Discontinuation of any offending medications (Am J Gastroenterol 2017;112:78)
- Antidiarrheals such as loperamide, diphenoxylate or bismuth subsalicylate
- For more severe symptoms, corticosteroids such as budesonide can be used
- Surgical intervention is a last resort
Clinical images
Images hosted on other servers:

Mucosal tears

Endoscopic findings
Microscopic (histologic) description
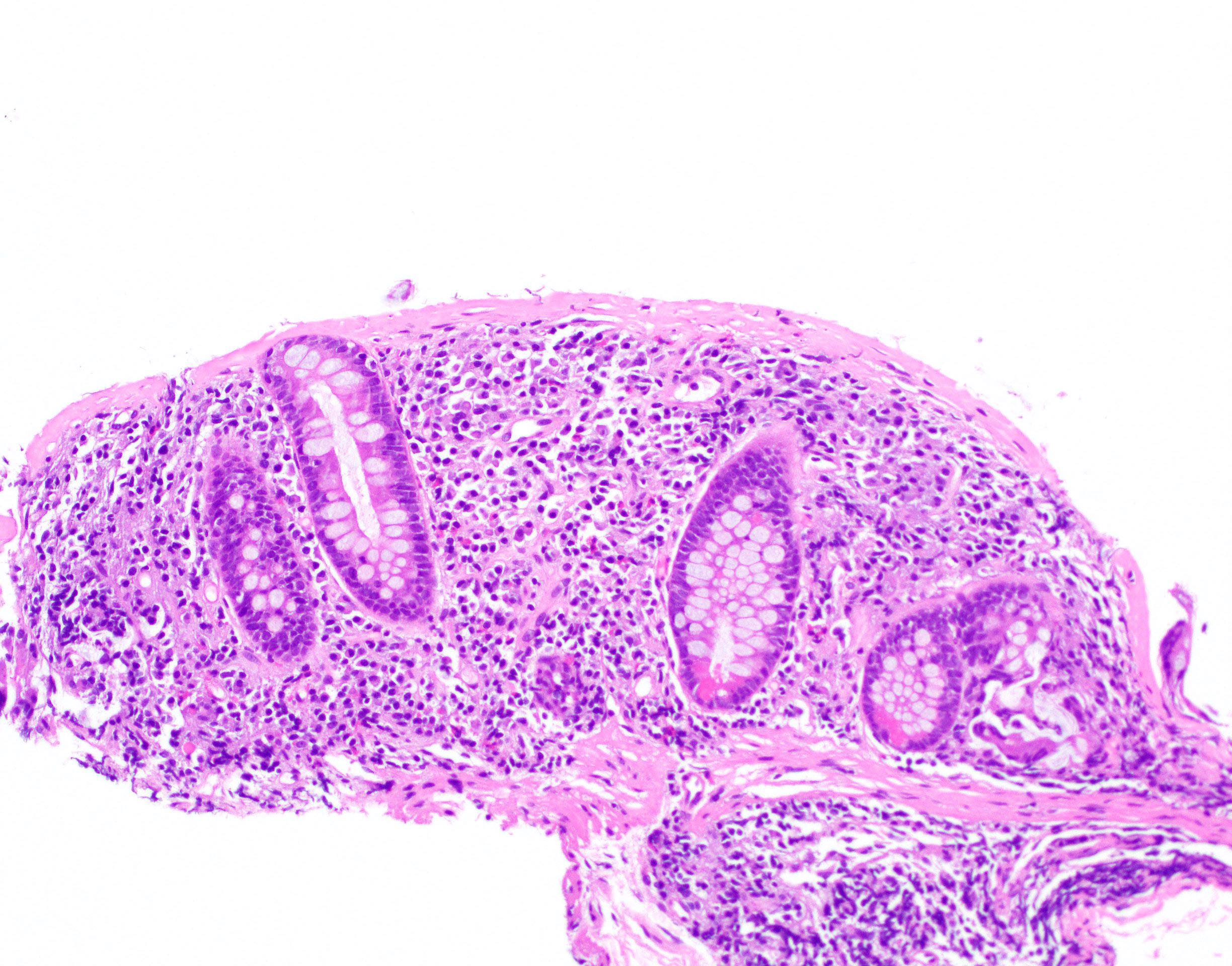
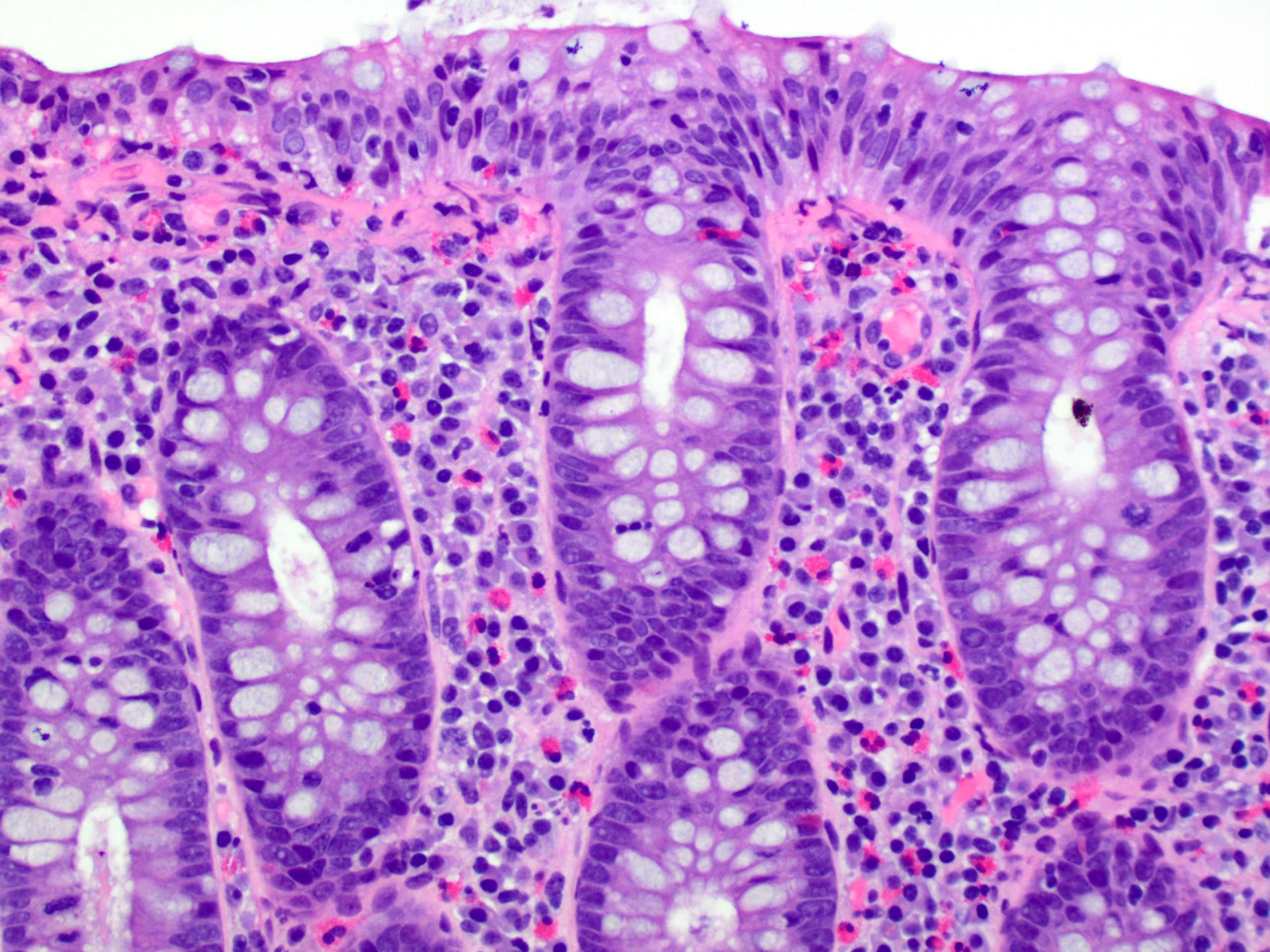
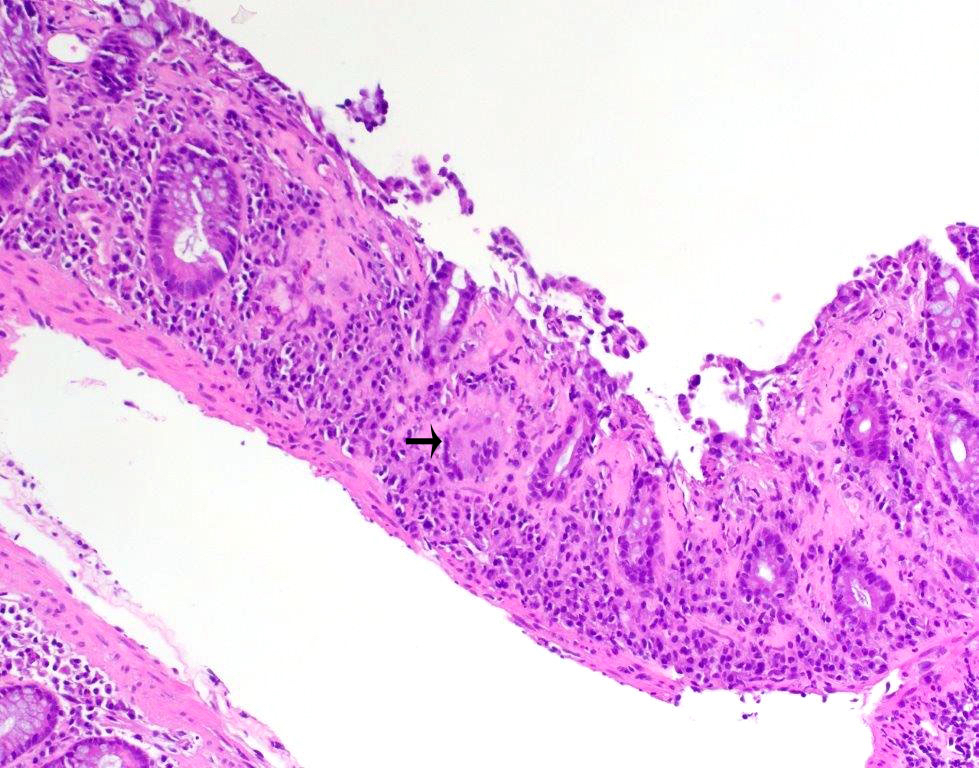
- Thickened subepithelial collagen band, usually with capillary, red blood cell and inflammatory cell entrapment (Histopathology 2015;66:613)
- Collagen band typically > 10 microns
- Occasional cases can have an irregular collagen band that is < 10 microns; some have labeled such cases as "incomplete collagenous colitis"
- Trichrome stain can be useful in equivocal cases
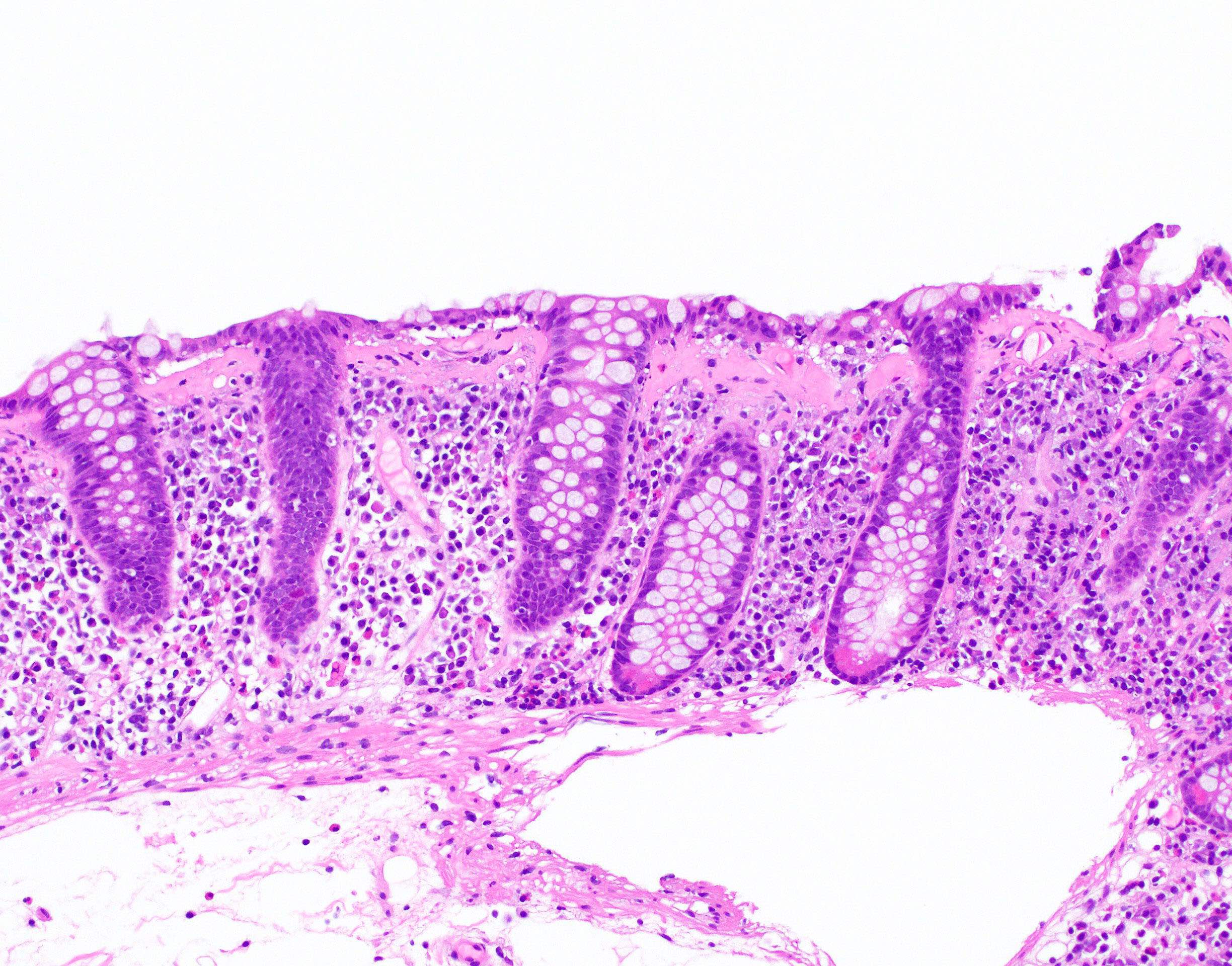
- Surface mucosal damage with loss of mucin, flattening and detachment
- Increased lamina propria inflammation composed of lymphocytes, plasma cells and eosinophils
- Neutrophilic inflammation can be seen but is typically not prominent
- Increased intraepithelial lymphocytes; may be mild (< 20 per 100 epithelial cells)
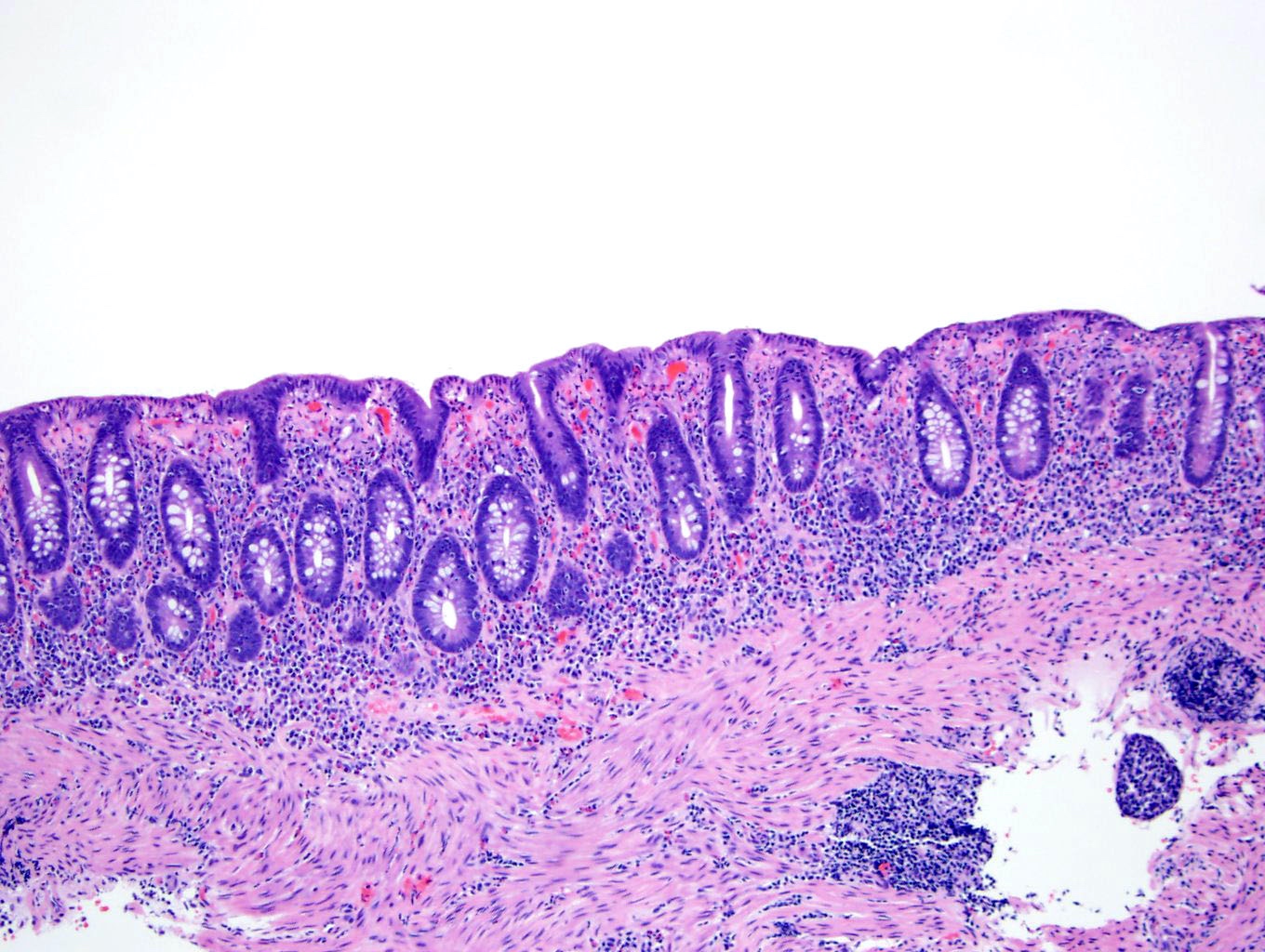
- Crypt architecture is preserved or minimally distorted
- Paneth cell metaplasia can be seen
- Up to 8% of cases can have crypt atrophy or irregularity (Am J Surg Pathol 2002;26:1414)
- Subepithelial multinucleated giant cells can be seen but have no clinical significance (Pathology 2008;40:671)
- Pseudomembranous collagenous colitis has been described; unclear whether truly a variant of collagenous colitis or due to superimposed infection or medication injury (Dig Dis Sci 2004;49:1763, Pathol Res Pract 2013;209:735)
Microscopic (histologic) images
Contributed by Catherine E. Hagen, M.D.
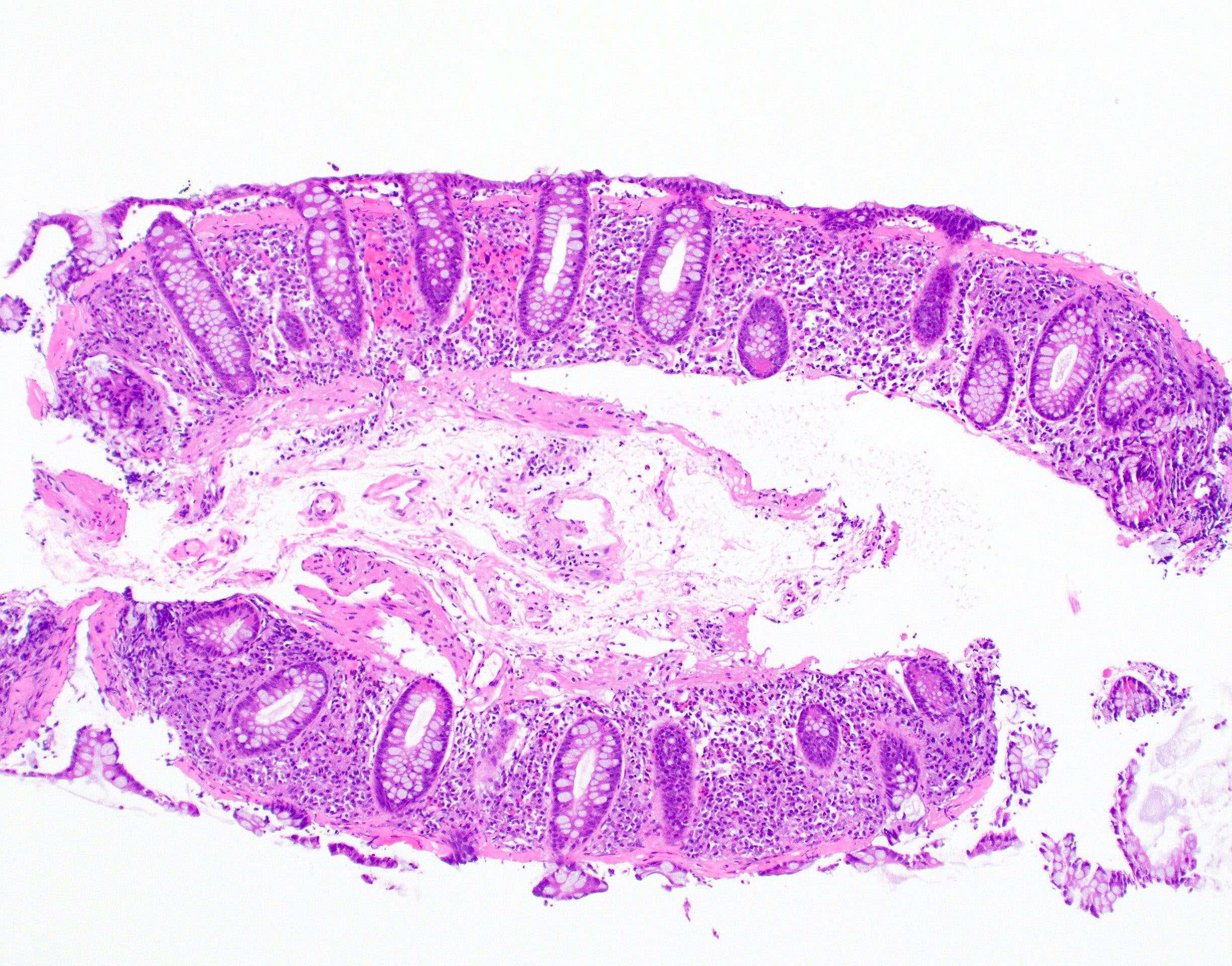
Preserved architecture
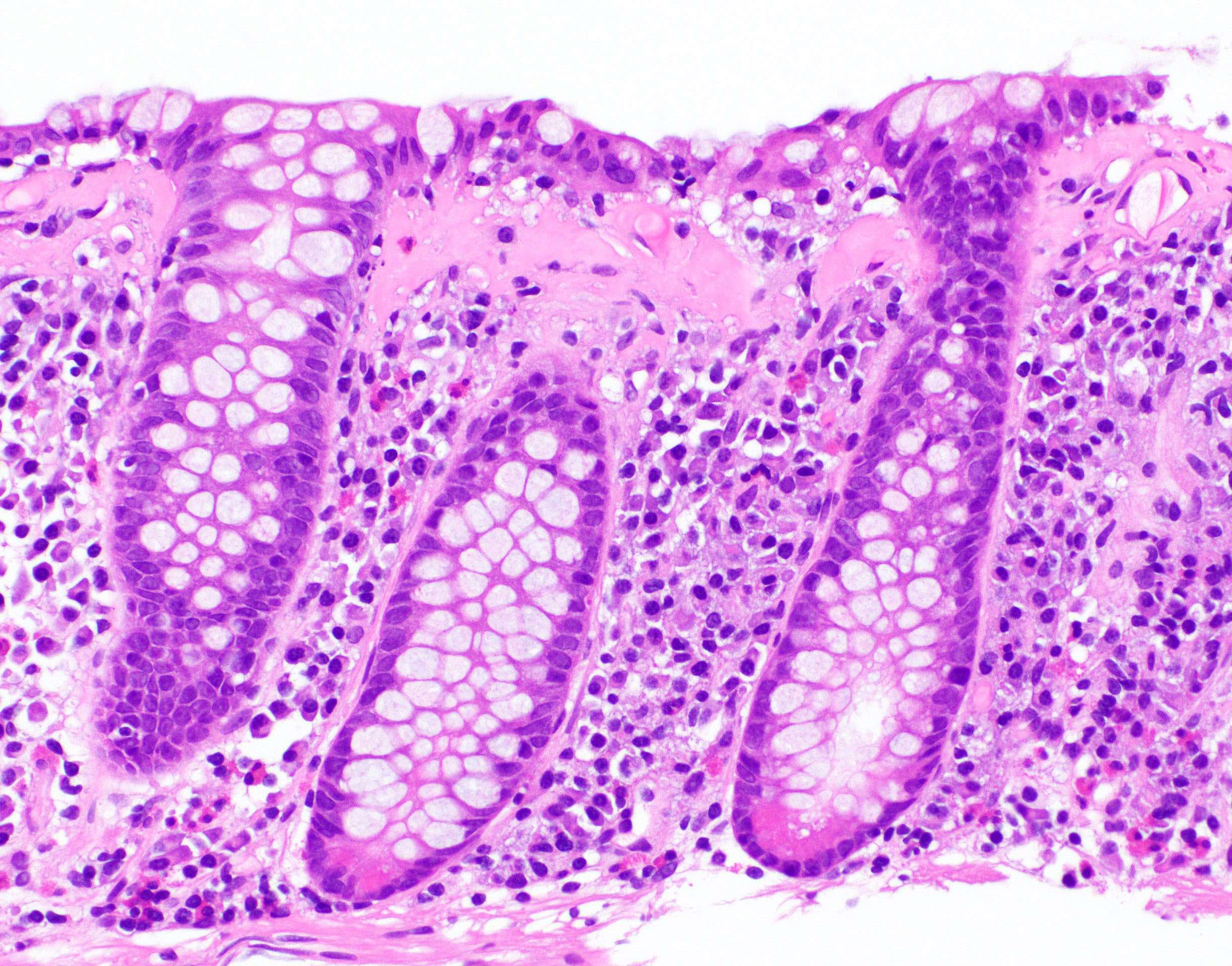
Thickened subepithelial collagen
Epithelial detachment
Equivocal collagen
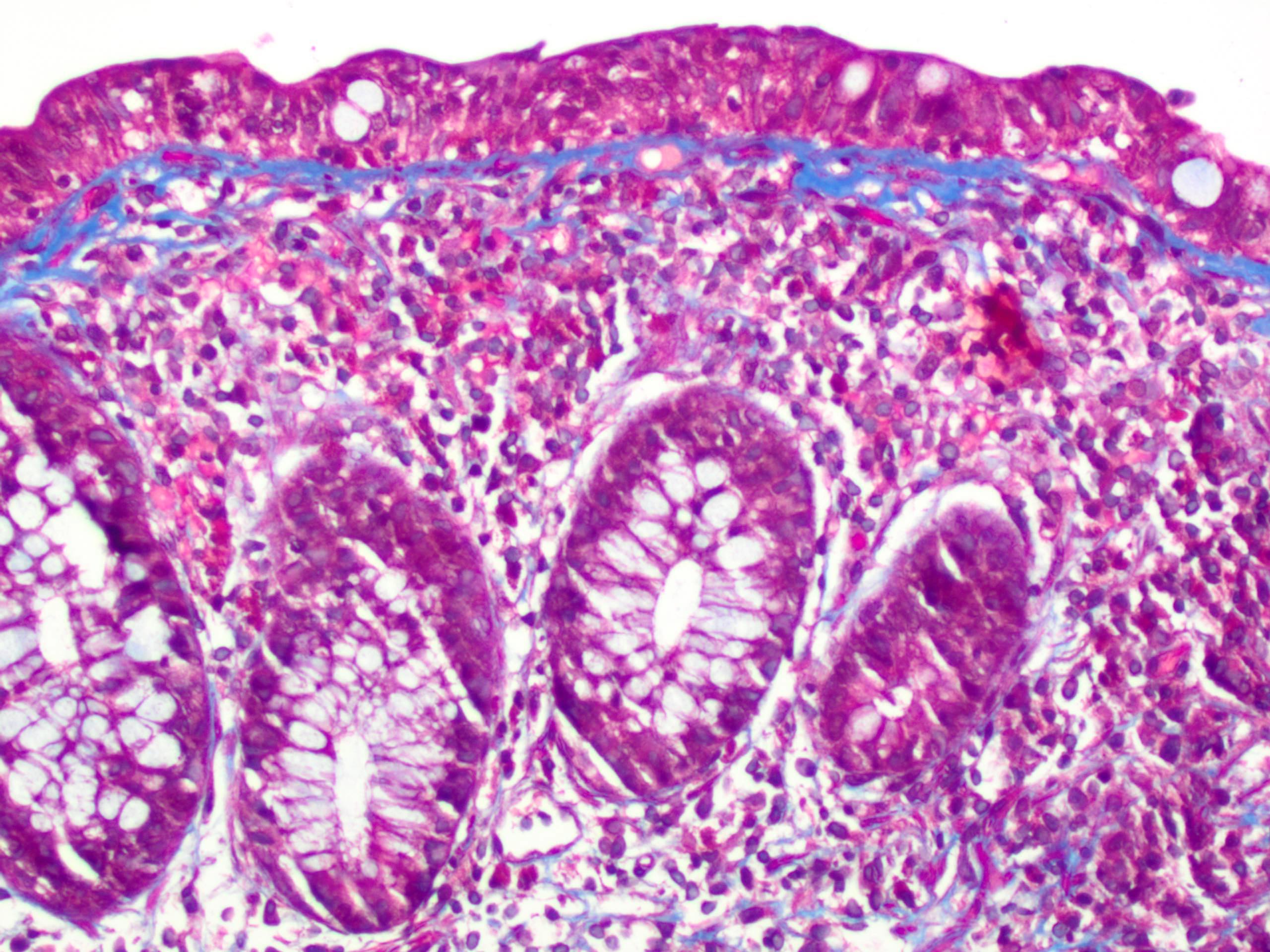
Trichrome stain
Giant cell
Crypt atrophy
Virtual slides
Images hosted on other servers:

Collagenous colitis biopsy
Positive stains
- Masson trichrome stain highlights the subepithelial collagen band
- CD3 highlights intraepithelial lymphocytes
- Tenascin immunohistochemical stain also highlights the collagen band (Histopathology 2015;66:613)
Negative stains
- Congo red stain
Sample pathology report
- Colon, random, biopsies:
- Colonic mucosa with a thickened subepithelial collagen band, increased intraepithelial lymphocytes and surface epithelial injury, consistent with collagenous colitis
Differential diagnosis
- Lymphocytic colitis:
- Lack of subepithelial collagen band and greater number of intraepithelial lymphocytes
- Inflammatory bowel disease:
- Lack of subepithelial collagen band
- Architectural distortion and prominent neutrophilic inflammation
- Endoscopic evidence of inflammation and clinical history of bloody diarrhea
- Chronic ischemic colitis:
- Diffuse lamina propria hyalinization as opposed to a discrete subepithelial collagen band
- Withered, injured crypts
- Amyloidosis:
- Usually surrounds blood vessels, though rarely may create a subepithelial layer mimicking collagenous colitis
- Congo red stain is positive
- Lack of surface epithelial injury and inflammation
Practice question #1
A 55 year old female with a 1 year history of chronic watery diarrhea presents for evaluation. Stool ova / parasites and culture are negative for infectious organisms. Colonoscopy is performed and reveals a grossly normal appearing colon. The biopsy histology is shown. Which of the following diagnoses is correct?
- Collagenous colitis
- Crohn's colitis
- Irritable bowel syndrome
- Lymphocytic colitis
Practice answer #1
Practice question #2
A 57 year old female was recently diagnosed with collagenous colitis. Which of the following is a characteristic histologic feature of collagenous colitis?
- Architectural distortion
- Cryptitis and crypt abscess
- Granulomas
- Mixed lamina propria inflammation
Practice answer #2
