Liver & intrahepatic bile ducts
Viral hepatitis
Epstein-Barr virus hepatitis
Authors: Alicia Cuber, D.O., Shefali Chopra, M.D.
Editorial Board Member: Kimberley J. Evason, M.D., Ph.D.


Last staff update: 23 September 2025 (update in progress)
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Epstein-Barr virus hepatitis

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Cuber A, Chopra S. Epstein-Barr virus hepatitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liverebv.html. Accessed September 25th, 2025.
Definition / general
- Epstein-Barr virus (EBV) hepatitis can occur in both immunocompetent and immunocompromised individuals
- Typically presents as a subclinical, self limited infection in immunocompetent individuals with infectious mononucleosis but may be severe and potentially fatal in immunocompromised patients
Essential features
- Characteristically shows a diffuse, single file lymphocytic infiltrate along the sinusoids (resembling a string of beads); a classic but nonspecific finding
- Mixed moderate inflammatory infiltrates in portal tracts composed primarily of cytotoxic CD8+ T cells
- Hepatocyte injury is very mild irrespective of the degree of inflammation with only rare acidophil bodies
- EBV encoded RNA (EBER) in situ hybridization positive
ICD coding
- ICD-10: B27.00 - gammaherpesviral mononucleosis without complication
Epidemiology
- In most cases of EBV related mononucleosis, the liver is involved; however, it is often subclinical or self limited
- In immunocompromised patients (i.e., transplant recipients, HIV / AIDS patients or patients on immunosuppressive medication for various autoimmune diseases), there is a higher risk for severe EBV hepatitis
Sites
- In cases associated with infectious mononucleosis, as commonly seen in immunocompetent individuals, EBV involvement typically includes the lymph nodes, tonsils and spleen
Etiology
- EBV is a double stranded DNA virus, which is a member of the herpesviridae family (human herpesvirus 4)
- Viral tropism in liver is generally limited to lymphocytes (predominantly B cells)
- Following EBV infection, remains latent in memory B cells
- Reference: Am J Surg Pathol 2007;31:1403
Clinical features
- Ranges from asymptomatic to nonspecific symptoms, such as fatigue, malaise, abdominal pain, back pain, arthralgias, night sweats and sore throat (Am J Surg Pathol 2007;31:1403)
- Hepatomegaly and jaundice can occasionally occur
Diagnosis
- EBV hepatitis is typically diagnosed through a combination of clinical presentation, laboratory findings and (in some select cases) microscopic examination of a liver biopsy
- Elevated levels of liver transaminases as well as EBV serology are needed for diagnosis
- EBV antibodies (like viral capsid antigens [VCA] IgM and IgG) can help confirm an active EBV infection
- Biopsy can be performed though not needed for diagnosis
- Reference: Am J Surg Pathol 2007;31:1403
Laboratory
- Elevated serum transaminases, which may be transient or mild (2 - 3 times upper limit of normal); occasionally 5 - 10 times upper limit of normal
- Jaundice reported in minority of cases
- Positive monospot test for heterophile antibodies (limited in specificity and sensitivity)
- Positive IgM antibodies to viral capsid antigens typically disappear in 4 - 6 weeks; IgG antibodies to VCA appear in initial month of illness and IgG antibodies to EB nuclear antigen 1 appear in convalescent stage
- PCR for EBV viral load (usually reserved for immunocompromised patients)
- Peripheral lymphocytosis, atypical lymphocytes may be present
- Reference: Arch Pathol Lab Med 2018;142:1191
Prognostic factors
- In most cases of EBV related mononucleosis, liver involvement is present but is either subclinical and self limited or manageable with supportive treatment
- Can be recurrent or chronic lasting > 6 months associated with poor prognosis
Case reports
- 1 year old girl with jaundice and maculopapular rash (JPGN Rep 2021;2:e089)
- 20 year old woman with right upper quadrant abdominal pain (Clin Case Rep 2024;12:e9357)
- 64 year old woman with EBV hepatitis masquerading as drug reaction with eosinophilia and systemic symptoms (DRESS) (Cureus 2023;15:e33782)
Treatment
- Supportive treatment
- Role of corticosteroids and antiviral medications is unclear at this time
Microscopic (histologic) description
- Diffuse single file lymphocytic sinusoidal infiltrate (or string of beads pattern)
- Portal tracts expanded by predominantly lymphocytic infiltrate composed primarily of cytotoxic CD8+ T cells, intermixed natural killer cells and few EBV infected B cells
- Atypical lymphocytes are often present in both portal tract and sinusoidal infiltrates
- Lobular architecture remains generally intact and there is minimal to mild hepatocyte injury
- Occasionally, epithelioid granulomas or fibrin ring granulomas may be seen
- Less common features include endothelialitis, bile duct damage and erythrophagocytosis
- Reference: Arch Pathol Lab Med 2018;142:1191
Microscopic (histologic) images
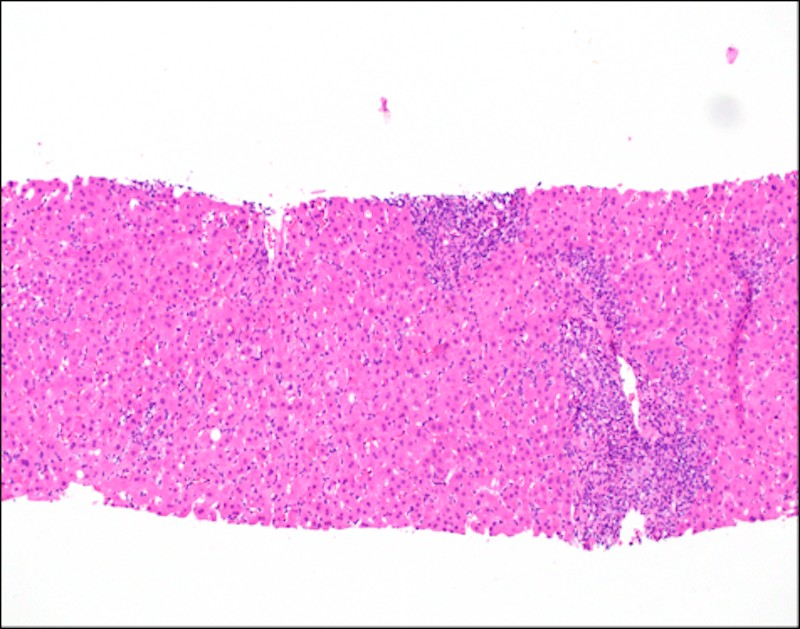
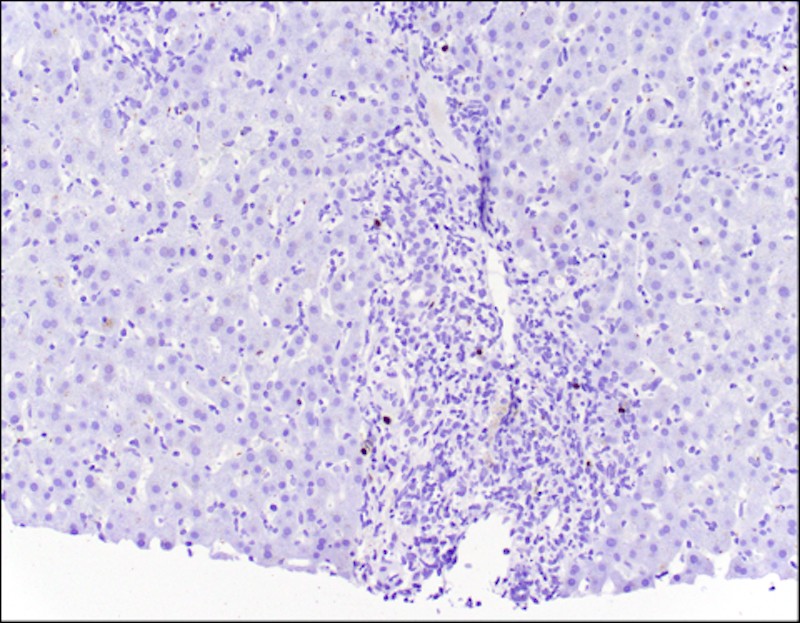
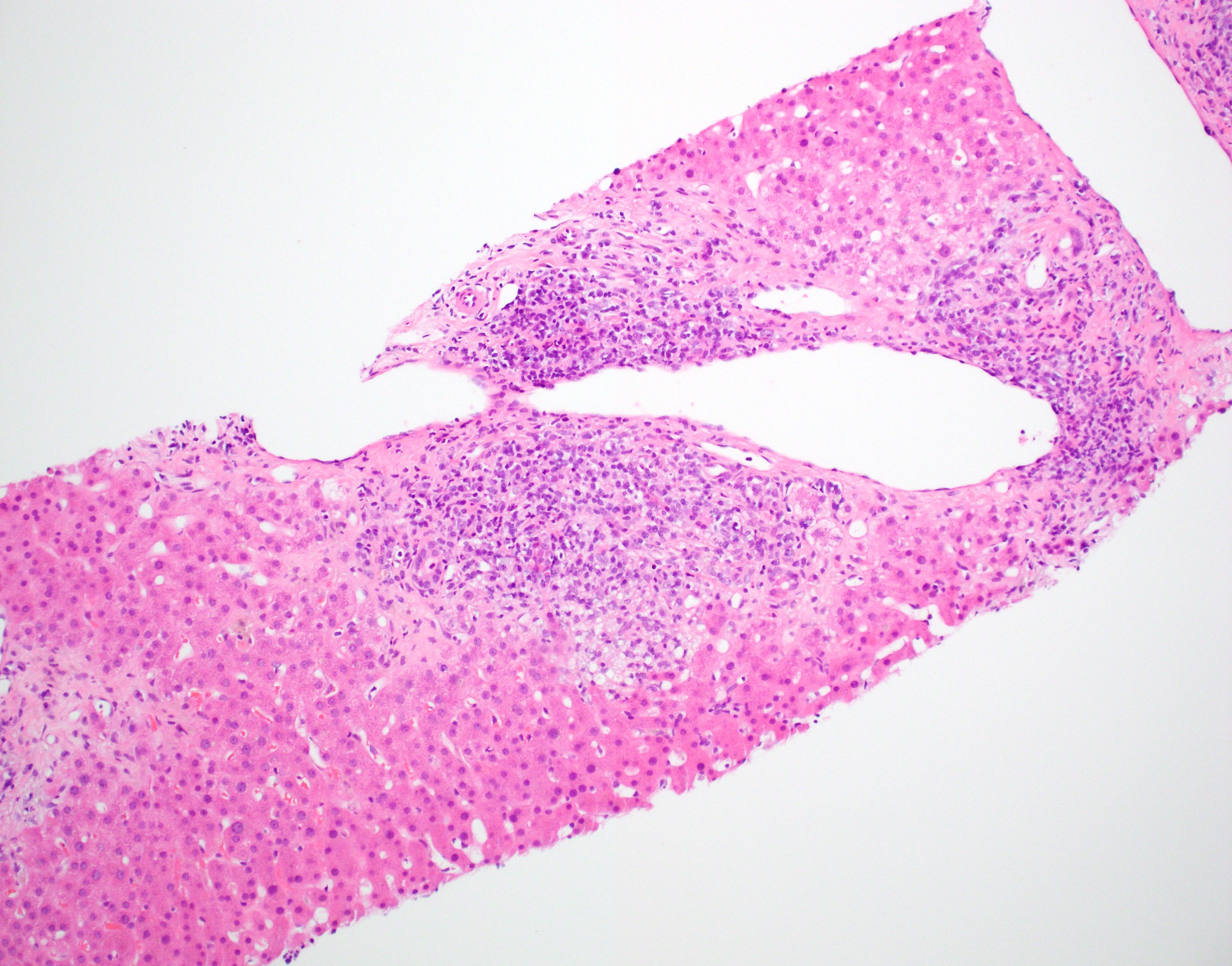
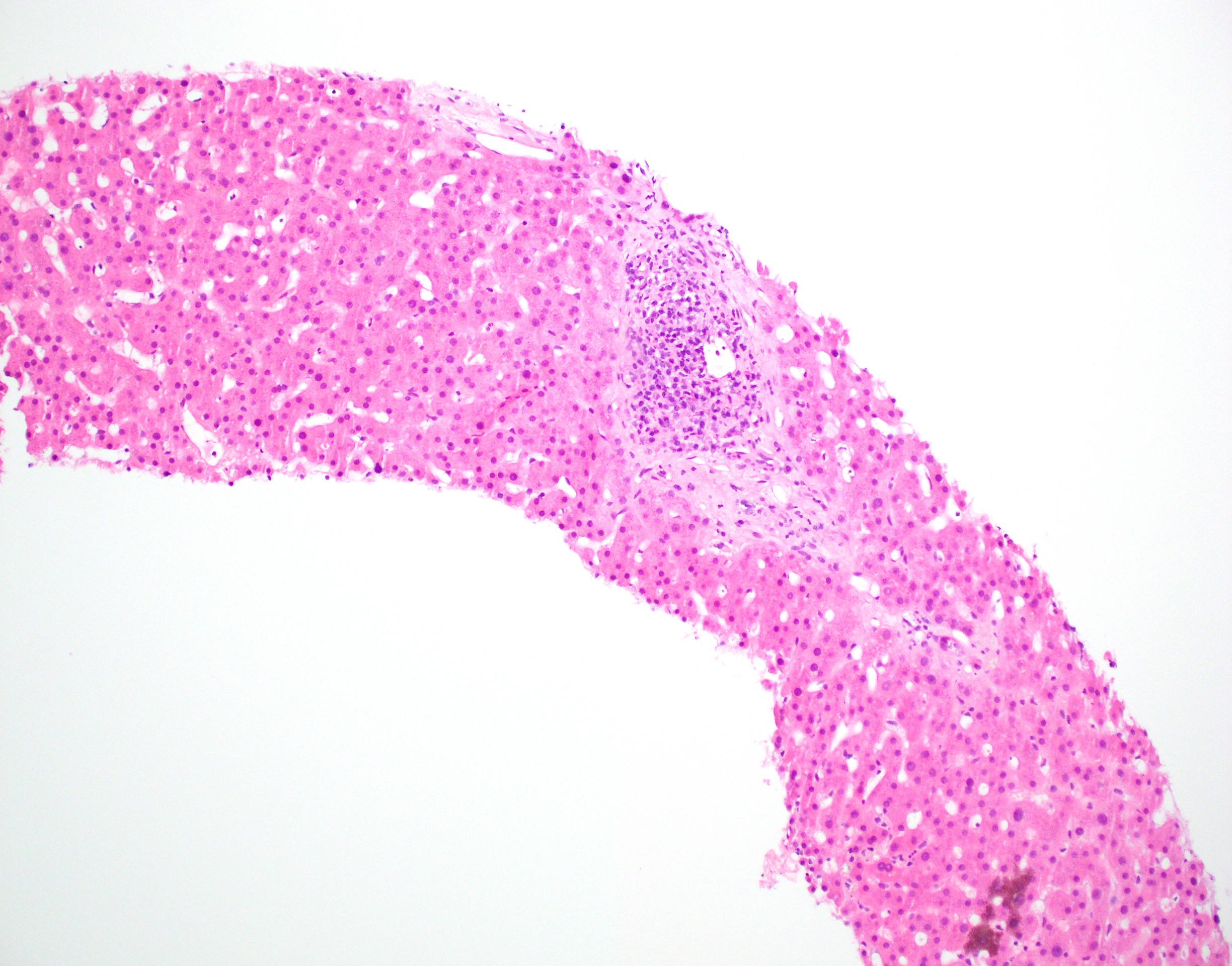
Contributed by Alicia Cuber, D.O.
Sinusoidal lymphocytic infiltrate
Sinusoidal lymphocytic infiltrate with EBER ISH
Portal lymphocytic infiltrate
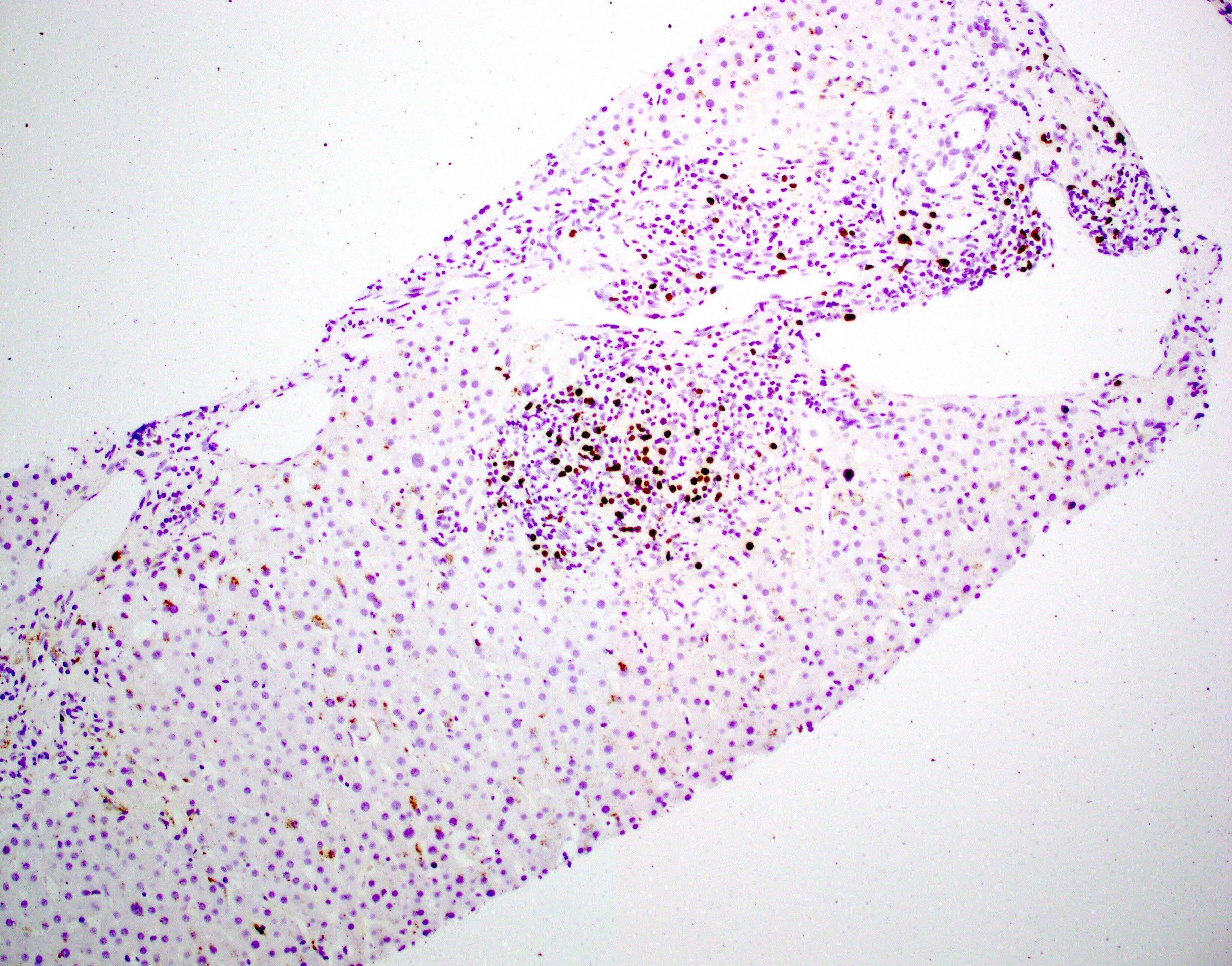
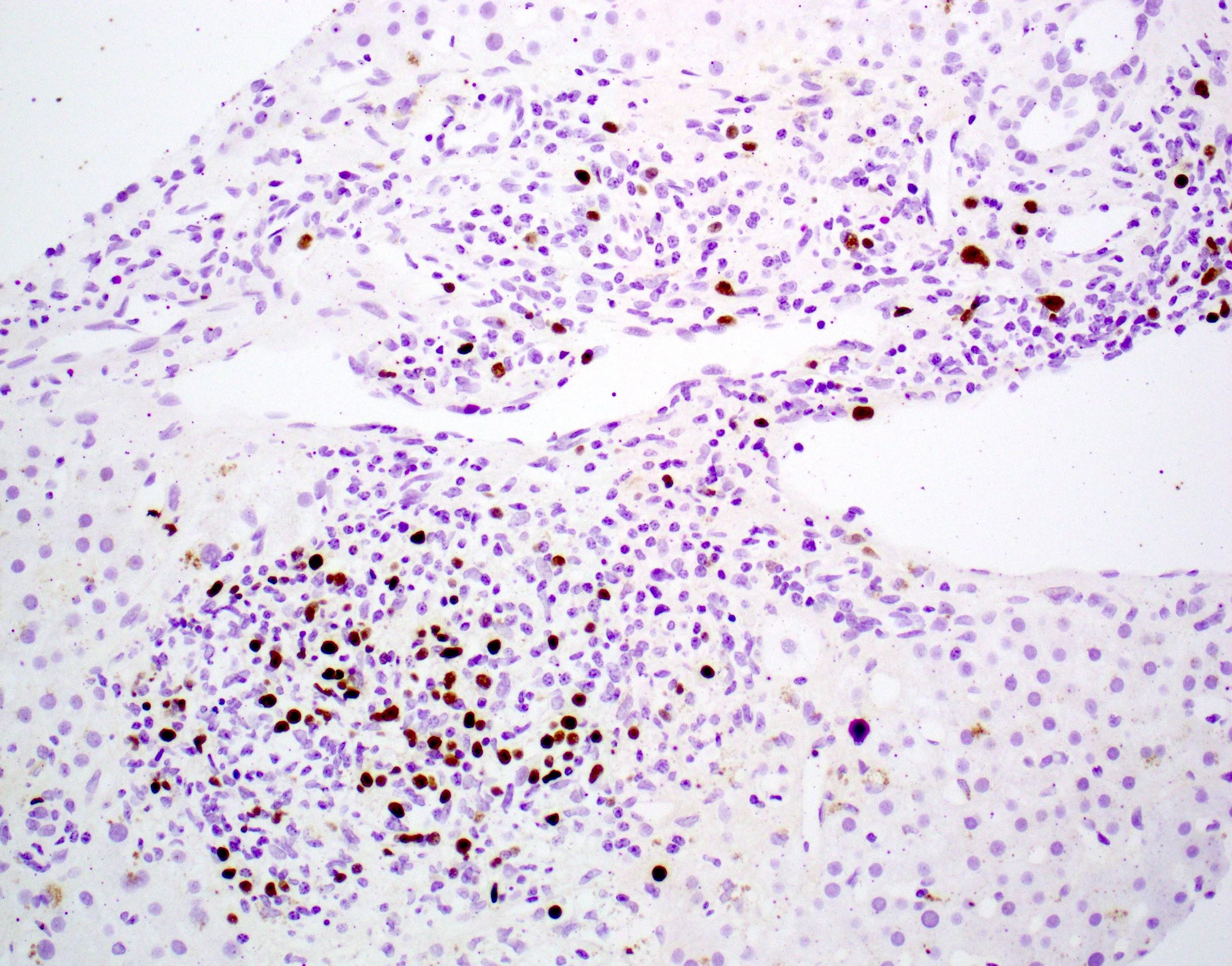
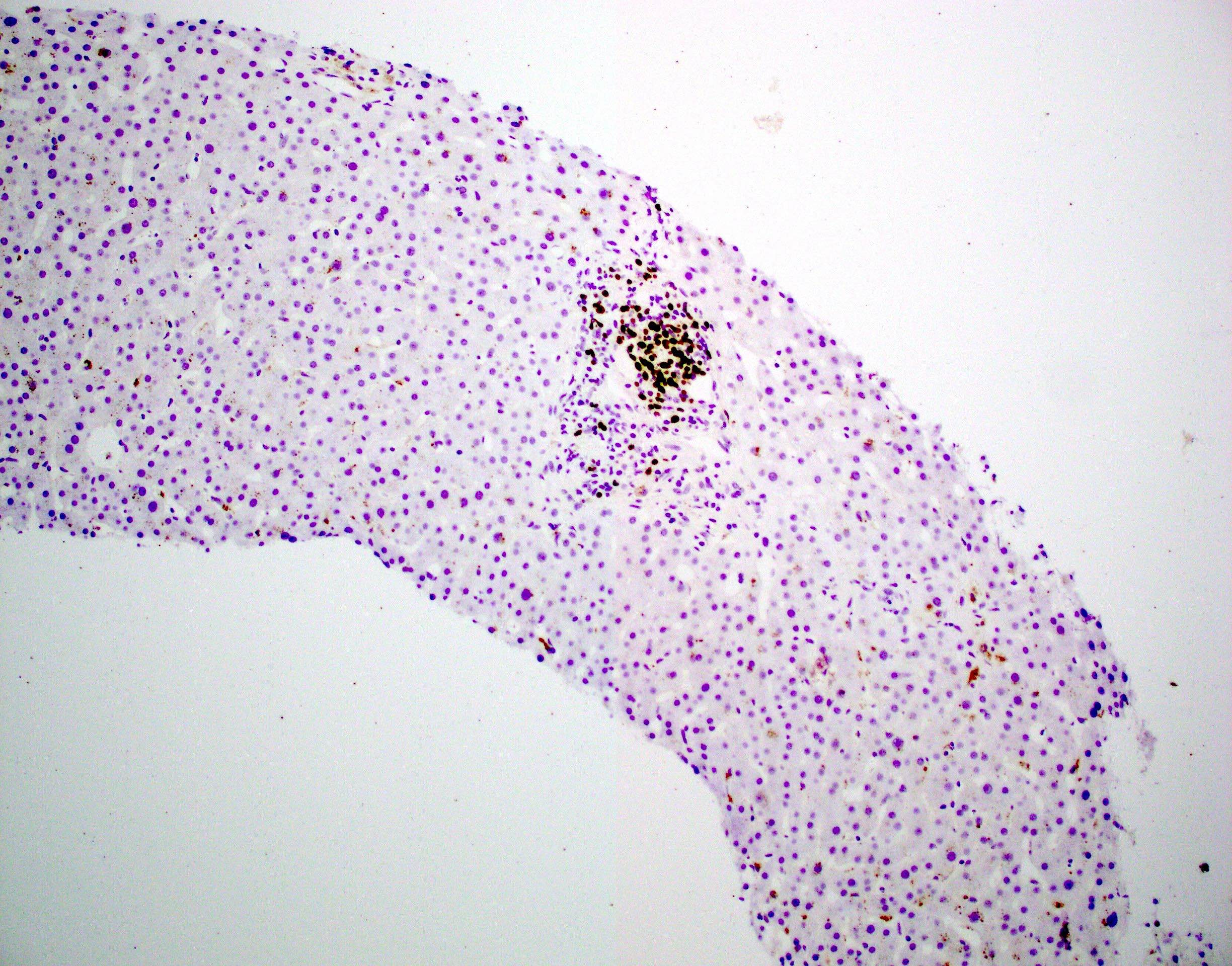
Portal lymphocytic infiltrate with EBER ISH
Positive stains
- EBV encoded RNA (EBER) in situ hybridization
Sample pathology report
- Liver, core needle biopsy:
- Consistent with Epstein-Barr virus (EBV) hepatitis (see comment)
- Comment: EBER ISH highlights few positive cells in portal tracts.
Differential diagnosis
- Autoimmune hepatitis:
- Autoimmune hepatitis will have more lobular activity and more severe hepatocyte damage; plasmacytosis is also noted, in contrast to EBV hepatitis, which is primarily lymphocytic
- Presence of positive EBV serologies helps to distinguish the entities
- Autoimmune hepatitis will have more lobular activity and hepatocyte damage as well as plasmacytosis compared to EBV hepatitis
- Acute cellular rejection in transplant recipients:
- In acute cellular rejection, portal infiltrates are mixed and will have eosinophils, neutrophils and plasma cells present as compared to EBV hepatitis, which is mostly lymphocytic
- Acute rejection will have more severe bile duct injury and venular endotheliitis more often
- Lymphoproliferative disorders:
- Hepatosplenic T cell lymphoma (HSTL):
- Primarily involves the sinuses of the liver, similar to the sinusoidal infiltration of atypical T cells in EBV hepatitis; however, portal tract involvement is minimal or absent in HSTL
- Posttransplant lymphoproliferative disorder:
- Map-like expansion of portal tracts
- Would have kappa (K) or lambda (L) light chain restriction, immunoglobulin gene rearrangements and flow cytometry abnormalities
- Hepatosplenic T cell lymphoma (HSTL):
- Drug induced liver injury:
- Lacks positive EBV serologies and EBER ISH positivity
- Review of medication for hepatotoxic drugs associated with sinusoidal lymphocytosis such as phenytoin, para-aminosalicylate and dapsone
- Cytomegalovirus (CMV) hepatitis:
- Can produce a mononuclear pattern
- Would have a viral cytopathic effect
- Lacks positive EBV serologies and EBER ISH positivity
Additional references
Practice question #1
An 18 year old man presents with complaints of fatigue and mild abdominal pain. On physical examination, the abdomen is soft with mild splenomegaly. The histopathology of ultrasound guided liver biopsy is depicted in the image shown above. What characteristic finding is seen?
- Cytoplasmic and nuclear inclusions
- Foci of geographic necrosis
- Mixed portal tract infiltrate of predominantly eosinophils
- Single file sinusoidal lymphocytes
Practice answer #1
D. Single file sinusoidal lymphocytes. The image shows sinusoidal lymphocytes arranged in a single file or string of beads pattern, which is a key feature of EBV hepatitis. Answer C is incorrect because the infiltrate is lymphocytic, not predominantly eosinophilic. Answer A is incorrect because cytoplasmic and nuclear viral inclusions are characteristic of cytomegalovirus (CMV) hepatitis (cytoplasmic and nuclear inclusions) or herpes simplex virus (HSV) hepatitis (mostly nuclear inclusions), not EBV. Answer B is incorrect because in EBV hepatitis, hepatocyte injury is typically minimal with only rare acidophil bodies.
Comment Here
Reference: Epstein-Barr virus hepatitis
Comment Here
Reference: Epstein-Barr virus hepatitis
Practice question #2
The histopathology of a liver biopsy is depicted in the image above. Based on findings in the image, what further ancillary study would be most useful for diagnosis?
- CD3 IHC
- CMV IHC
- EBER ISH
- HSV IHC
Practice answer #2
C. EBER ISH. The image shows sinusoidal lymphocytes arranged in a single file or string of beads pattern, which is a key feature of EBV hepatitis. EBER ISH will be positive in these cases.
Answers B and D are incorrect because there is no viral cytopathic effect seen to indicate the need for viral stains.
Answer A is incorrect because CD3 IHC can be used in the workup for hepatosplenic T cell lymphoma (HSTL) but in the image, there is a portal lymphocytic infiltrate, which would not be expected in HSTL.
Comment Here
Reference: Epstein-Barr virus hepatitis
Comment Here
Reference: Epstein-Barr virus hepatitis
