Pancreas
General
Cytology
Editorial Board Member: Catherine E. Hagen, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.

Last author update: 2 February 2021
Last staff update: 16 June 2021
Copyright: 2020-2025, PathologyOutlines.com, Inc.
PubMed Search: Pancreas[TI] cytology[TI] full text[SB]
Table of Contents
Definition / general | Essential features | Sites | Clinical features | Diagnosis | Cytology description | Cytology images | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Policarpio-Nicolas MLC. Cytology. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/pancreascytology.html. Accessed August 14th, 2025.
Definition / general
- Normal and nonneoplastic findings in pancreas cytology
- Preparations:
- Conventional smears or touch preparation stained with Diff-Quik, Papanicolaou
- Liquid based (thin prep)
- Cytospin
- Cell block (for immunohistochemistry and molecular)
- Cyst fluid (chemistry, tumor markers, molecular)
Essential features
- Normal cellular elements:
- Acinar
- Ductal
- Islet cells (rare)
- Contaminants during procedure:
- Bile
- Gastric epithelium
- Duodenal epithelium
- Hepatocytes
- Mesothelial cells
- Procedures:
- Pancreas image guided fine needle aspiration (FNA)
- Bile duct brushing
- Percutaneous interventional guided FNA
Sites
- Head / uncinate, body and tail of pancreas
Clinical features
- General settings: patients with suspected neoplasia of the pancreaticobiliary tract should receive the following (Diagn Cytopathol 2014;42:325)
- Clinical history and physical examination, including identifying risk factors for malignant causes and for benign explanations for a stricture or cyst (e.g. chronic pancreatitis, primary sclerosing cholangitis / inflammatory bowel disease, autoimmune disease, etc.)
- Laboratory studies (e.g. serum bilirubin and alkaline phosphatase)
- Selective use of serum tumor markers (CA19-9 and CEA)
- Imaging studies
- Serum IgG4 when autoimmune disease is suspected
- Clinical indications for pancreas FNA
- Pancreatic mass / cyst on imaging (Diagn Cytopathol 2014;42:325)
- Unexplained acute pancreatitis in older patients
- Newly diagnosed late onset diabetes mellitus
- Jaundice, pruritus, cholestasis unexplained by underling hepatobiliary disease or choledocholithiasis
- Anorexia, weight loss, abdominal pain radiating to the back
- Clinical indications for bile duct brushing
- Obstructive jaundice (Acta Cytol 2016;60:167)
- Distal common bile duct stricture
- Proximal / complex hilar stricture
- Screening patients with primary sclerosing cholangitis for biliary neoplasia (Endoscopy 2016;48:432)
Diagnosis
- Common diagnostic procedures utilized in the procurement of pancreatic cytology samples:
- Endoscopic ultrasound (EUS) guided FNA for pancreatic mass / lesions
- Endoscopic retrograde cholangiopancreatography (ERCP) and percutaneous transhepatic cholangiography (PTC) are used to obtain brushing or aspiration from the common bile duct and pancreatic duct stricture / mass
Cytology description
Normal
Nonneoplastic contaminants
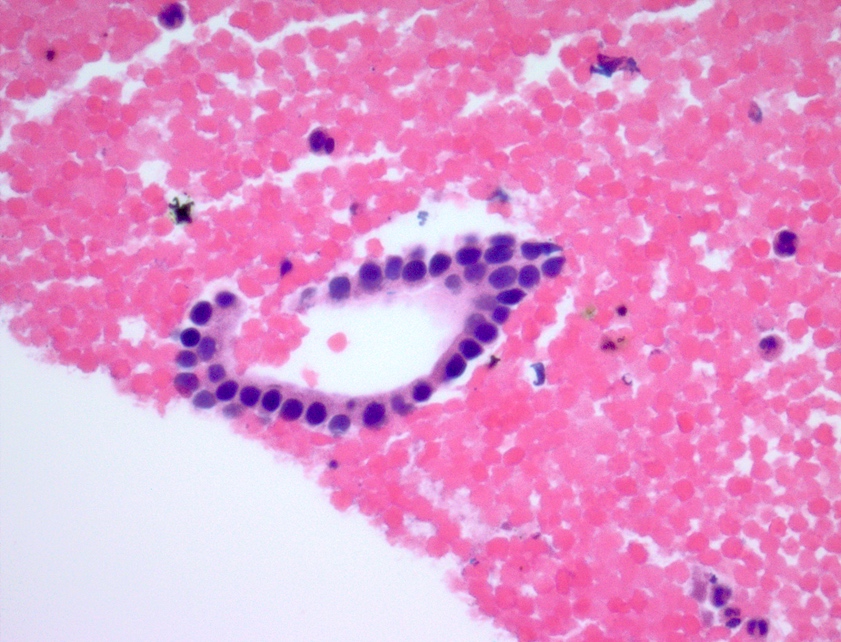
- Bile duct
- Monolayered flat sheets arranged in honeycomb pattern
- Cuboidal to columnar cells
- Bland appearing basally located nuclei imparting a picket fence appearance
- Scant pale cytoplasm
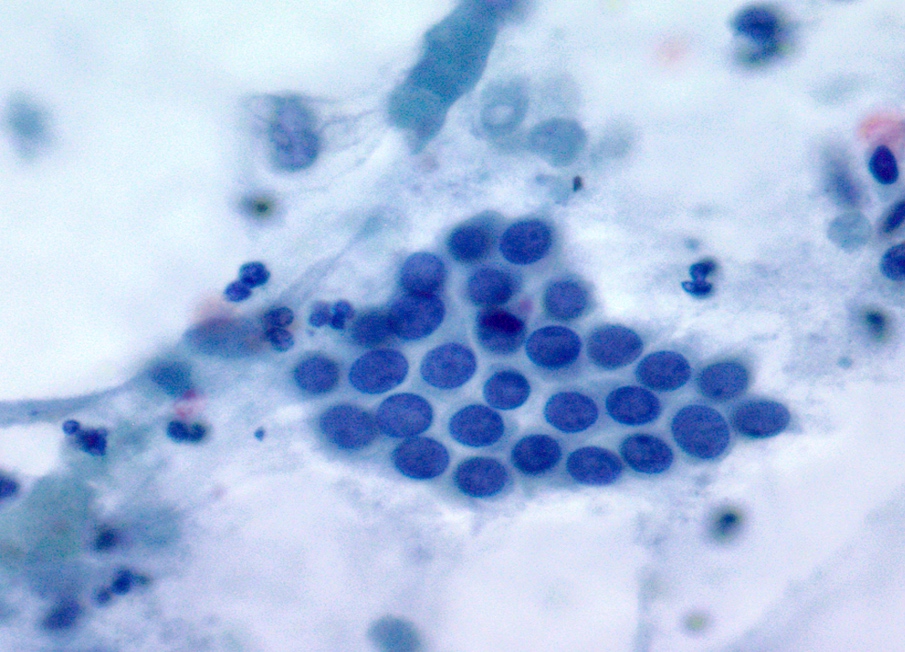
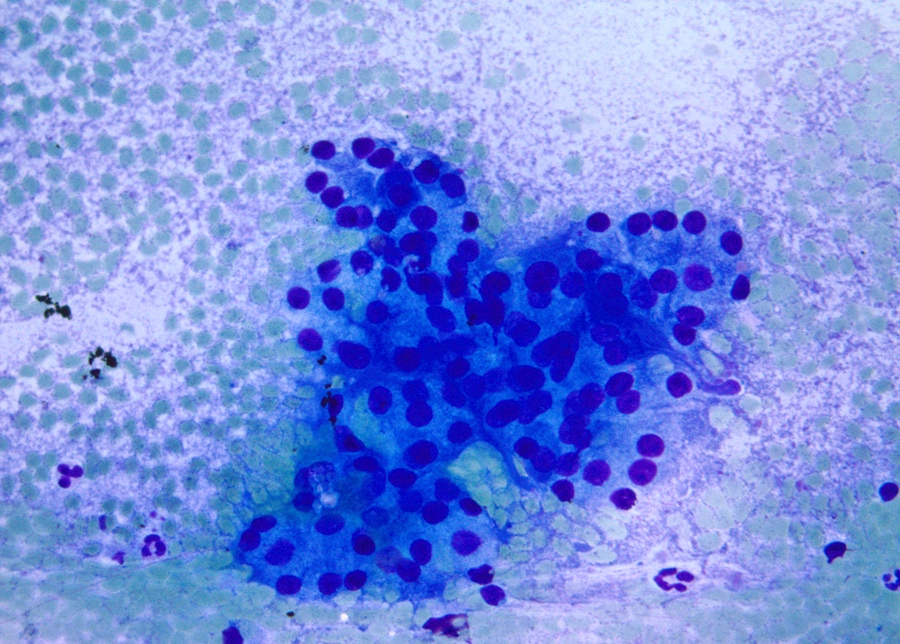
- Acinar cells
- Pyramidal to triangle shaped cells arranged singly, in clusters or grape-like appearance occasionally embedded in fibroconnective tissue
- Abundant granular cytoplasm
- Round central to eccentric nuclei
- Occasional nucleoli
- Islet cells
- Infrequently seen in normal pancreas
Nonneoplastic contaminants
- Bile: seen in biliary specimens
- Duodenal epithelium: seen in EUS guided transduodenal FNA for lesions in pancreatic head and uncinate
- Flat sheets (honeycomb) arrangement, occasional singly scattered cells
- Uniformly round, bland appearing evenly spaced nuclei
- Scant pale cytoplasm
- Goblet cells present (Diagn Cytopathol 2005;33:381)
- Gastric epithelium: present in transgastric EUS FNA for pancreatic lesions in the body and tail
- Flat sheets arranged in monolayered (honeycomb) pattern (Diagn Cytopathol 2005;33:381)
- Cells with uniformly round, evenly spaced bland appearing nuclei
- Pale cytoplasm with well defined cell border
- Surface epithelium lined by tall columnar cells with basally located nuclei and cytoplasm filled with abundant mucin
- Hepatocytes: contaminant in procedures using percutaneous interventional guided FNA
- Polygonal cells with well defined cell borders and abundant granular cytoplasm
- May have intracytoplasmic pigment (bile, lipofuscin or iron)
- Centrally located nuclei, prominent nucleoli
- Occasional intranuclear inclusions
- Mesothelial cells: contaminant in procedures using percutaneous interventional guided FNA
- Polygonal cells arranged in flat sheets
- Moderate amount of cytoplasm (dense in the center and pale in periphery)
- Clear spaces in between cells intercellular windows
- Single to occasionally binucleated to multinucleated round to oval nuclei
Cytology images
Contributed by Maria Luisa C. Policarpio-Nicolas, M.D.
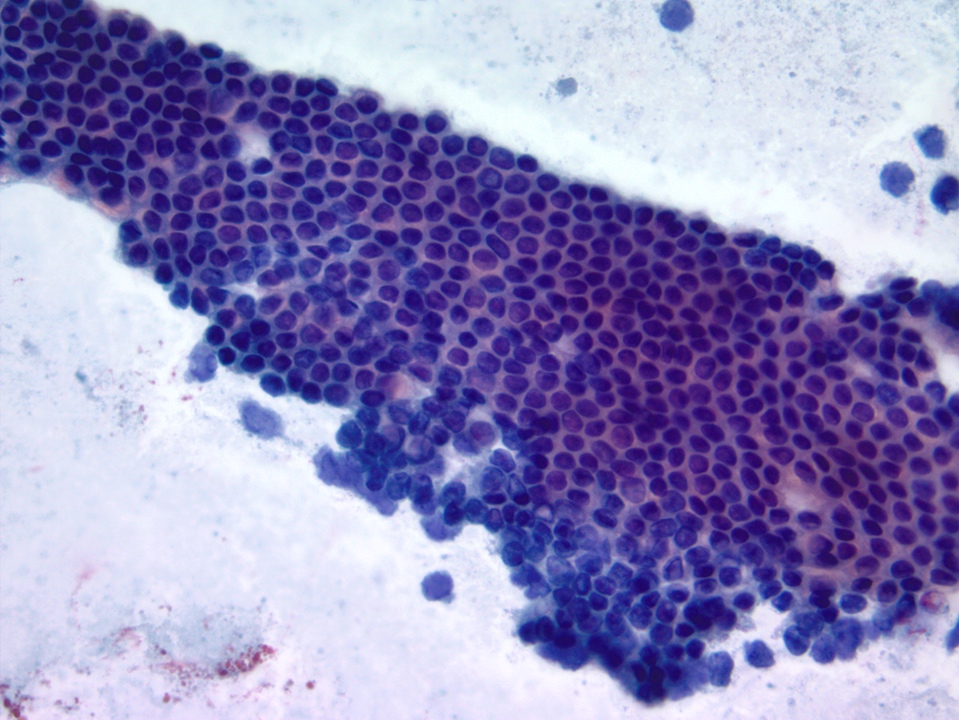
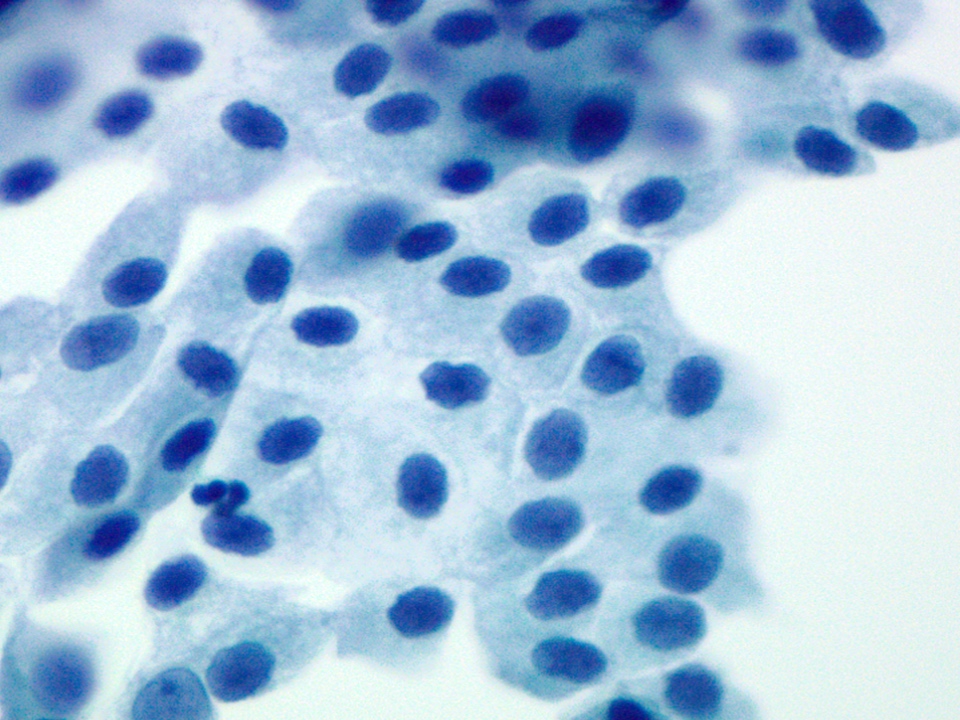
Ductal cells with bland nuclei
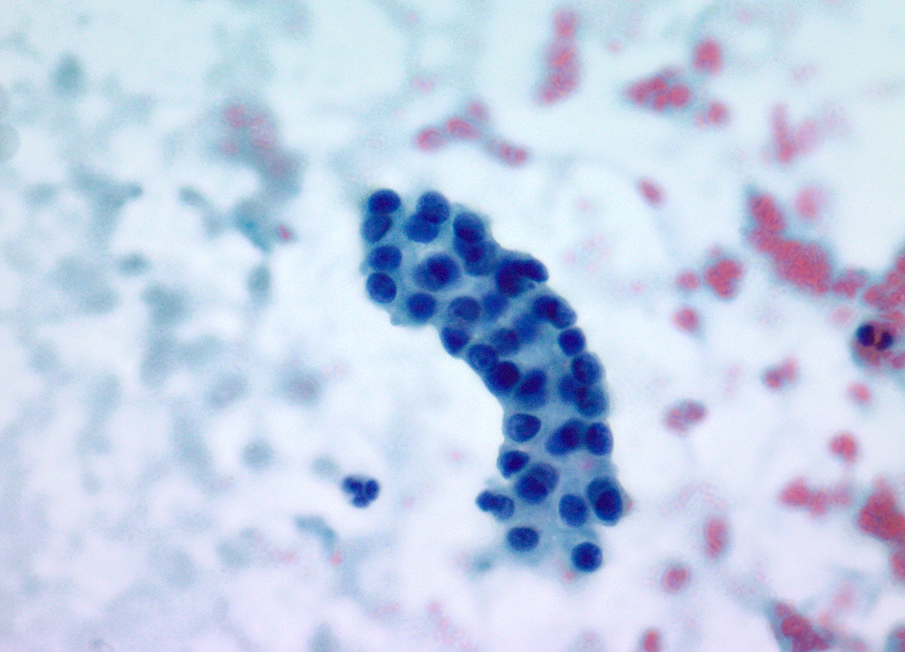
Ductal cells with tubule formation
Ductal epithelium cell block
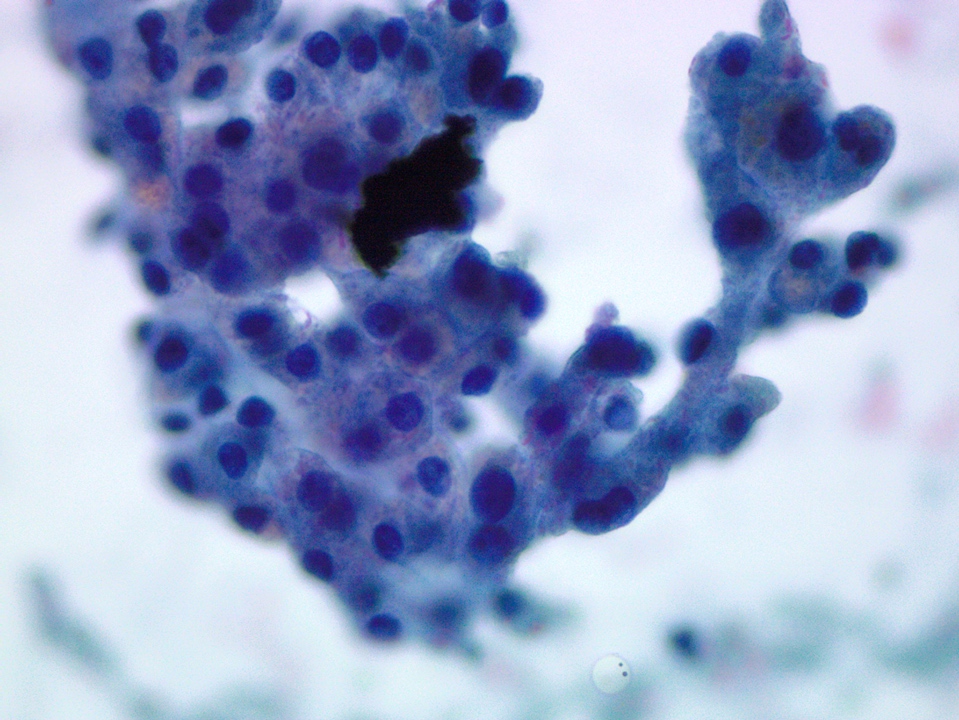
Clusters of acinar cells
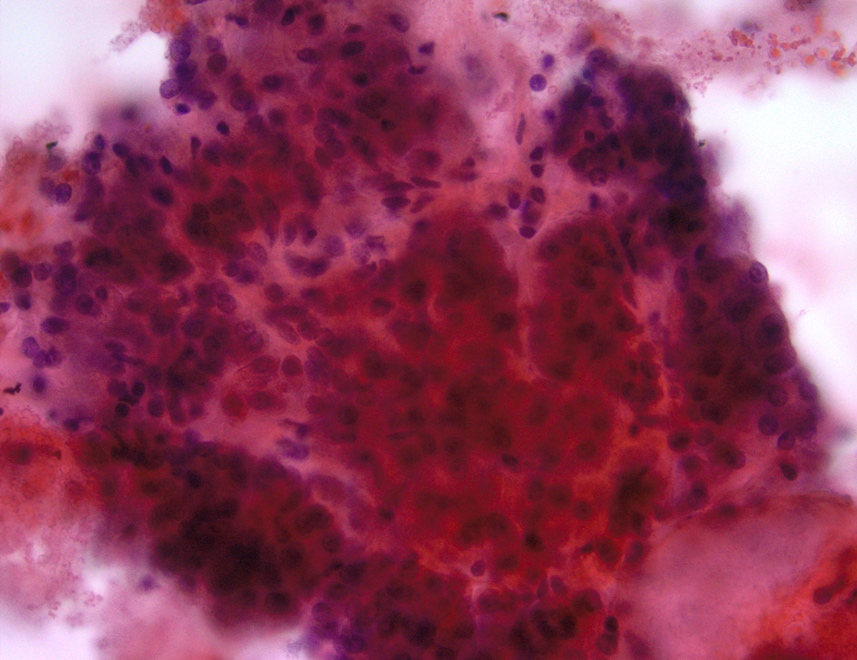
Acini in grape-like arrangement
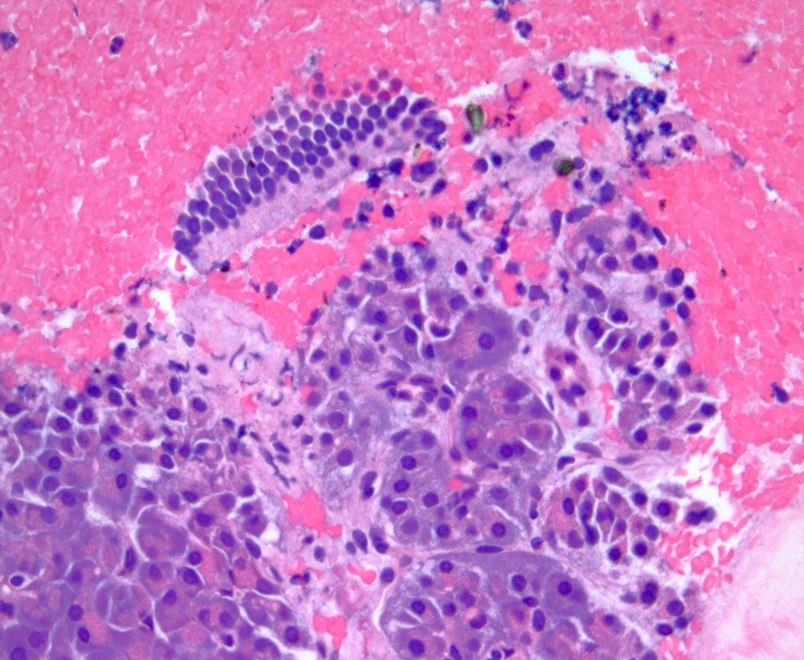
Acinar and ductal cells histology

Gastric epithelium
Duodenal epithelium with goblet cells
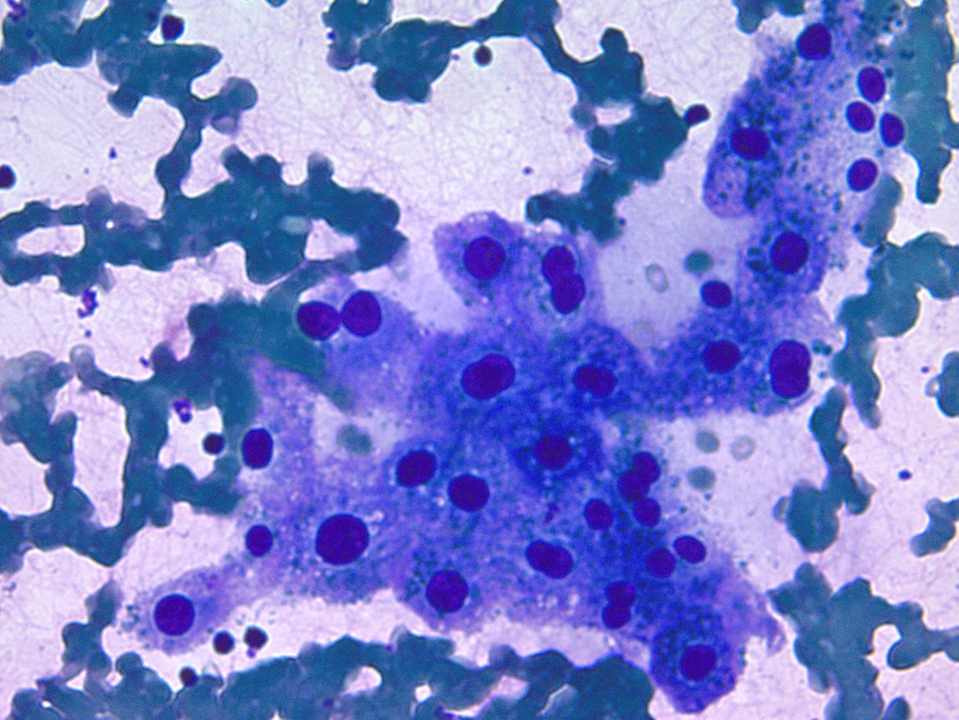
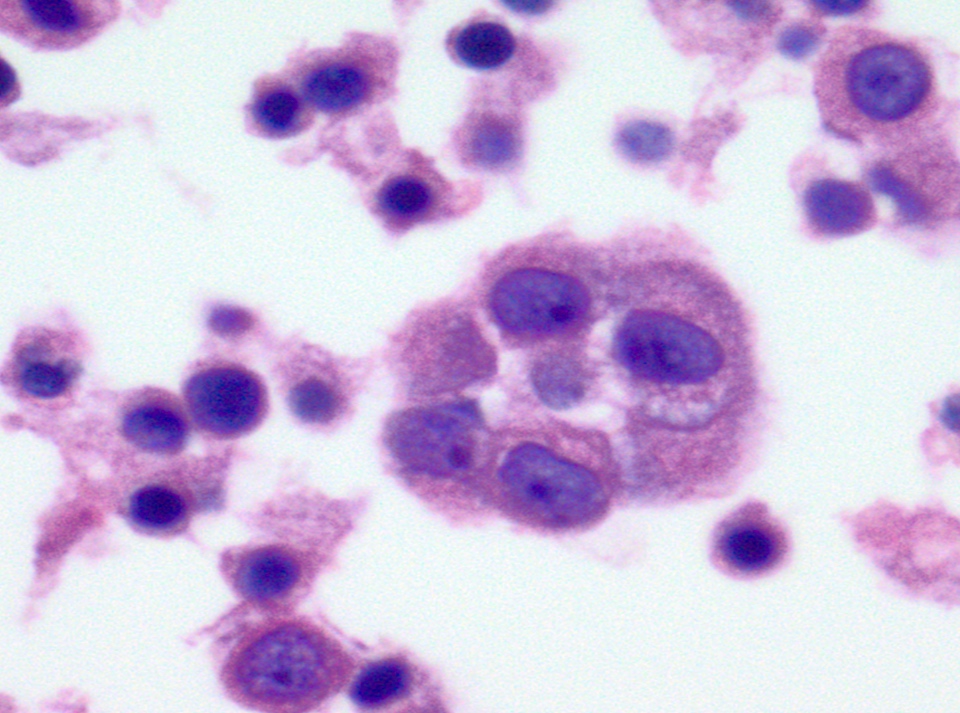
Hepatocytes with intracytoplasmic pigment
Hepatocytes with bile
Mesothelial cells in sheets
Mesothelial cells with intercellular windows
Sample pathology report
- Pancreas, head, endoscopic ultrasound guided fine needle aspiration:
- Nondiagnostic
- Normal acinar and ductal epithelium. The biopsy does not explain the well defined pancreatic mass seen on imaging (Cytojournal 2014;11:3).
Differential diagnosis
- Acinar carcinoma:
- Highly cellular, small to moderate sized loose groups, numerous single cells and stripped round nuclei, prominent acinar formation, little anisonucleosis, prominent nucleoli (Diagn Cytopathol 2006;34:367)
- Ductal adenocarcinoma:
- 3 dimensional to glandular arrangement of tumor cells, loss of polarity, moderate to marked variation in nuclear size (4:1 ratio), small to large prominent nucleoli, singly scattered tumor cells, mitotic figures (few to many)
- Low grade neoplastic mucinous cyst (intraductal papillary mucinous neoplasm, mucinous cystic neoplasm):
- On cytomorphology alone, it is extremely difficult to distinguish gastric contamination from a neoplastic mucinous cyst
- If background mucin is present, a note / comment can be added (see below)
- Note / comment: Benign appearing mucinous epithelium is present from this transgastric FNA in a background of extracellular mucin. The morphology of the cells is nonspecific and may represent low grade dysplasia or gastric contamination. No high grade atypia is identified and no necrosis is present (Pitman: The Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology, 2015).
Practice question #1
The above image is an FNA sample from the pancreatic head. Which of the following choices represents the image in the sample?
- Acinar cells
- Ductal cells
- Islet cells
- Malignant cells
Practice answer #1
Practice question #2
Which is the method used to procure a cytology sample from a bile duct stricture?
- Endoscopic ultrasound guided
- CT guided
- Endoscopic retrograde cholangiopancreatography
- MRI guided
Practice answer #2
