Pancreas
Cystic and intraductal lesions
Mucinous cystic neoplasm (MCN)
Authors: Enoch Kuo, M.D., Raul S. Gonzalez, M.D.
Editorial Board Member: Catherine E. Hagen, M.D.


Last author update: 15 April 2021
Last staff update: 1 May 2025
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Mucinous cystic neoplasm pancreas

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1Cite this page: Kuo E, Gonzalez RS. Mucinous cystic neoplasm (MCN). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/pancreasmcn.html. Accessed October 2nd, 2025.
Definition / general
- Benign or potentially low grade malignant cystic epithelial neoplasm composed of cells which contain intracytoplasmic mucin (ICD-O: 8470/0 [Accessed 18 February 2021])
- WHO classification:
- MCN with low grade dysplasia (adenoma)
- MCN with high grade dysplasia (carcinoma in situ)
- MCN with invasive carcinoma
Essential features
- Cystic neoplastic lesion that is a precursor to pancreatic adenocarcinoma
- May harbor invasive carcinoma
- Presence of associated ovarian type stroma
ICD coding
Epidemiology
- Almost always women (> 95%); mean age of 45 years (Ann Surg 2008;247:571)
Sites
- Distal pancreas (> 95%) (Ann Surg 2008;247:571)
- Can also occur in the liver and gallbladder
- Metastases usually restricted to abdominal cavity; metastases to ovary may simulate primary ovarian tumors
Pathophysiology
- Ectopic ovarian stroma is thought to be seeded from primordial ovarian cells at early stages of embryonic development
- Cysts are later formed by hormones and growth factors released by the ovarian stroma (Am J Surg Pathol 1999;23:410)
Etiology
- No known etiology
Clinical features
- Usually a single lesion (Gut Liver 2015;9:571)
- May present as abdominal pain or acute pancreatitis (Ann Surg 2008;247:571)
- Majority are slow growing and asymptomatic (Gastroenterology Res 2014;7:44)
Diagnosis
- Cytology and lab analysis of pancreatic cyst fluid from endoscopic ultrasound guided FNA
- Histology of pancreatic resection
Laboratory
- Elevated carcinoembryonic antigen (CEA) and presence of KRAS mutation in cyst fluid supports a mucinous cyst (includes MCN and intraductal papillary mucinous neoplasm) (Ann Gastroenterol;26:122)
Radiology description
- Thick walled, single, septated cyst in the body or tail of the pancreas (Gut Liver 2015;9:571)
- May have nodules or calcifications
Prognostic factors
- Prognosis is excellent unless there is invasive carcinoma with extracapsular or diffuse intracapsular infiltration (Am J Surg Pathol 2015;39:179, Ann Surg 2008;247:571)
- Features associated with invasive carcinoma include increased cyst size (> 5 cm), intracystic papillary nodules > 1 cm in size and elevated serum CA19-9 (Am J Surg Pathol 2015;39:179)
- Less than 20% of cases have invasive carcinoma (Gut Liver 2015;9:571, Ann Surg 2008;247:571)
Case reports
- 38 year old woman with anaplastic carcinoma and mucinous cystic neoplasm of the pancreas during pregnancy (World J Gastroenterol 2008;14:132)
- 46 year old man with pancreatic mucinous cystic neoplasm with sarcomatous stroma metastasizing to liver (World J Surg Oncol 2013;11:100)
- 52 year old Japanese woman with anaplastic carcinoma combined with mucinous cystadenocarcinoma of the pancreas (Arch Pathol Lab Med 1997;121:1104)
- 65 year old man (JOP 2012;13:687)
Treatment
- Surgical resection is indicated for all MCNs (Gut Liver 2015;9:571, Gastroenterology Res 2014;7:44)
Gross description
- Large (mean 10 cm)
- Typically unilocular megacysts that do not communicate with ductal system, though up to 15% communicate with main pancreatic duct (Gut Liver 2015;9:571)
- Cyst wall is papillary, trabecular or thickened
- Has mucoid / watery cyst contents
- Must sample solid areas within the cyst
Gross images
Contributed by Diana Agostini-Vulaj, D.O., Wei Chen, M.D., Ph.D., Nakul Anush Ravish, M.B.B.S. and AFIP

MCN with no connection to main duct
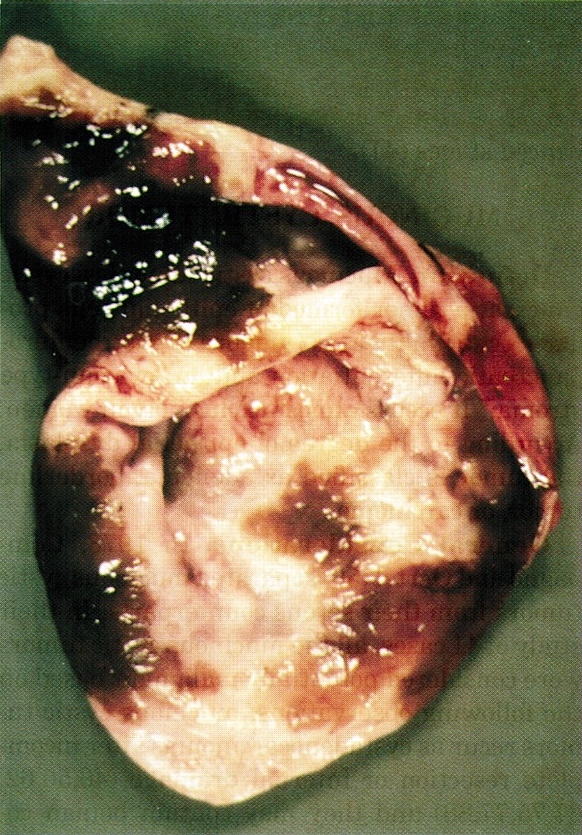
Unilocular cyst
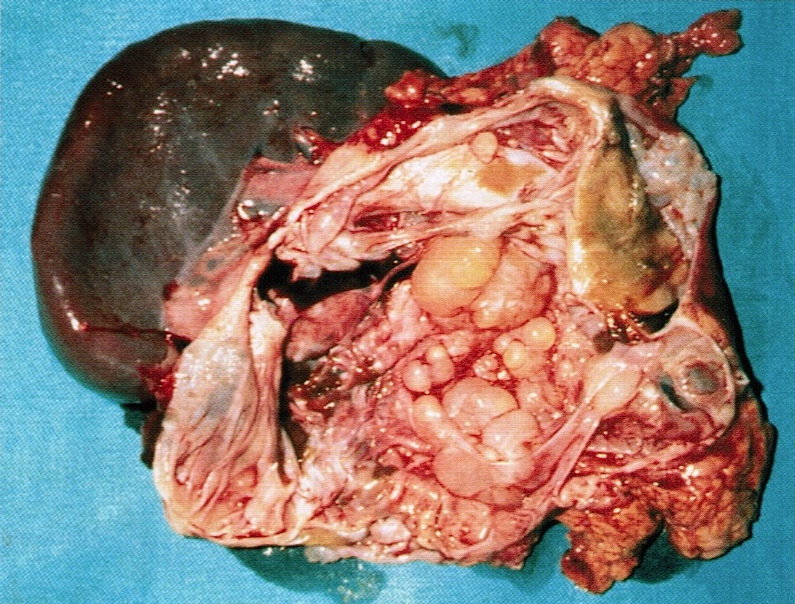
Conspicuous, irregular, solid protuberances

Multiloculated cystic lesion

36 year old
woman: large
cyst with
solid tumor

Mucinous cystic neoplasm
Images hosted on other servers:

39 year old man with multilocular cyst with thick mucin
Microscopic (histologic) description
- Large cyst lined by intestinal, pseudopyloric or gastric foveolar type epithelium that often form papillae, surrounded by characteristic dense ovarian type stroma (Gut Liver 2015;9:571)
- Epithelial lining has variable atypia (none, low grade, high grade); scattered neuroendocrine cells may be present
- Invasive adenocarcinoma may or may not be present; must sample extensively to rule out an invasive component (Gut Liver 2015;9:571, Am J Surg Pathol 1999;23:1320)
- Calcifications are common
- May have mural nodules with features of giant cell tumor, malignant fibrous histiocytoma or anaplastic carcinoma
Microscopic (histologic) images
Contributed by Raul S. Gonzalez, M.D. and Matthew W. Rosenbaum, M.D.
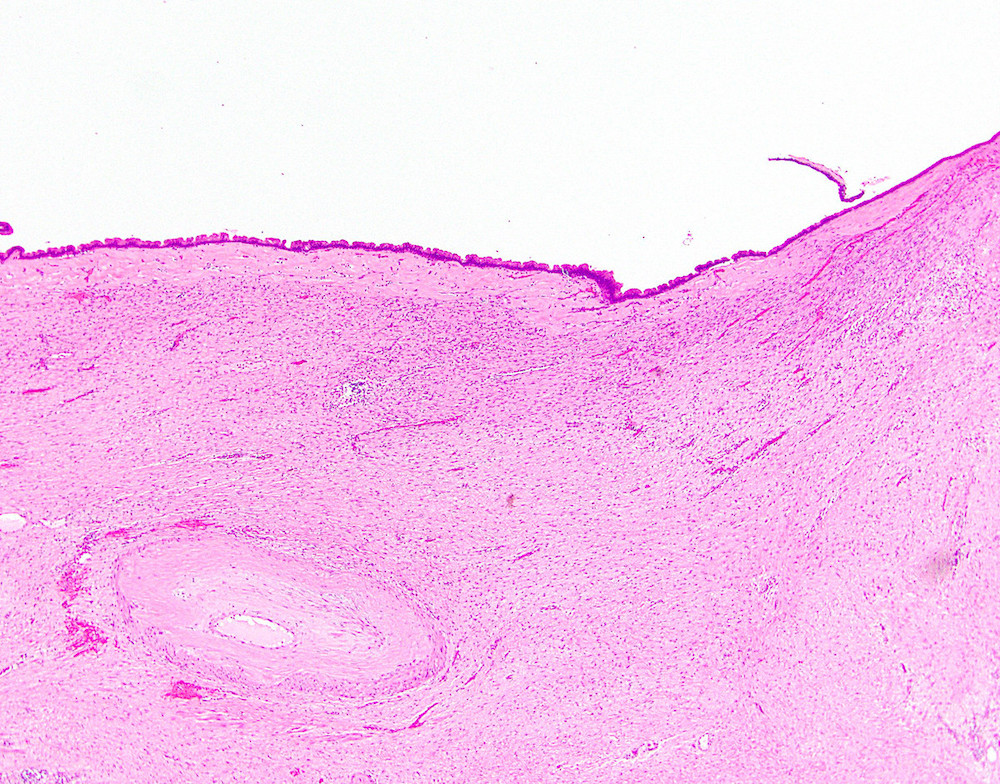
Spindled ovarian type stroma

Focal minute papillation
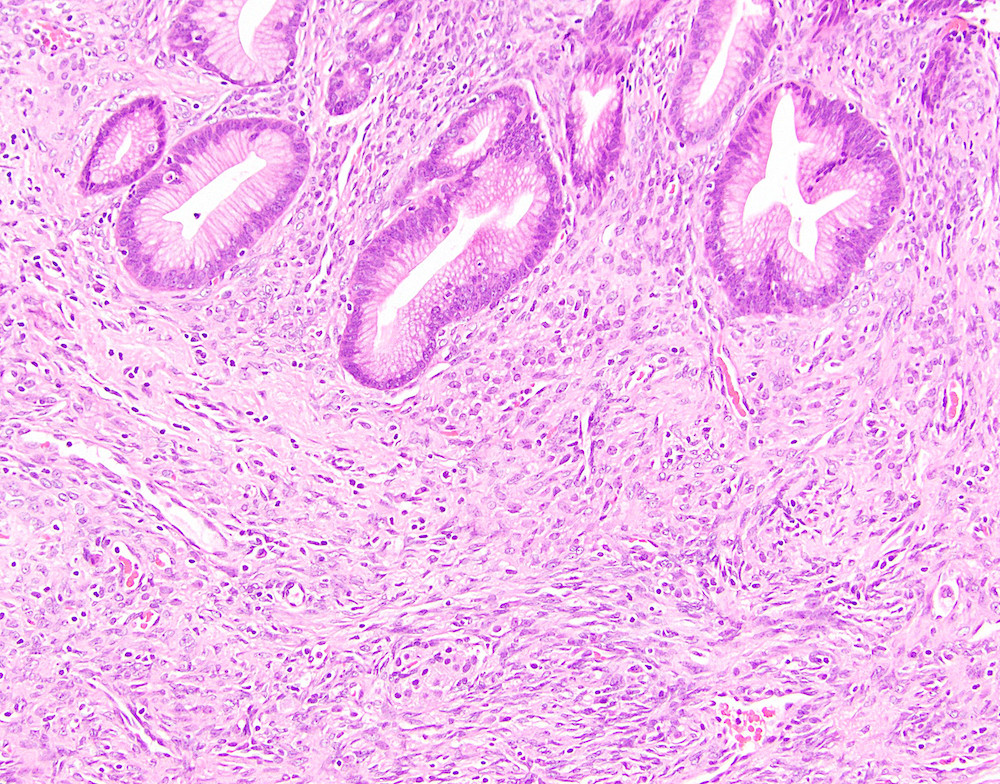
Foveolar mucinous epithelium
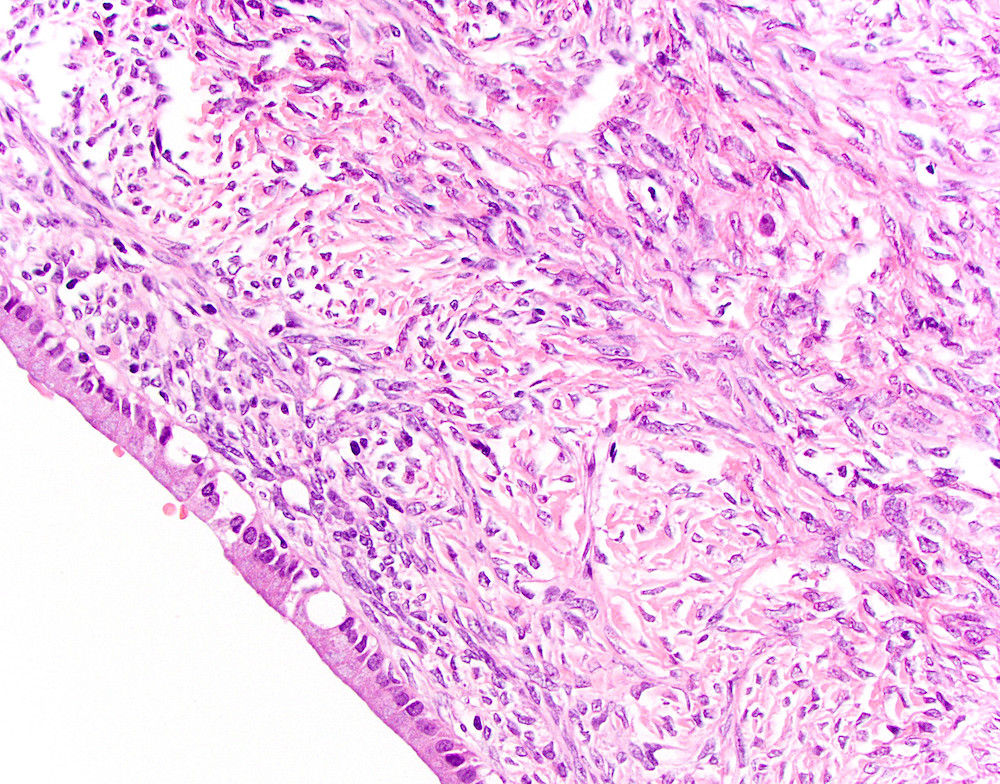
Classic ovarian type stroma

MCN with invasion
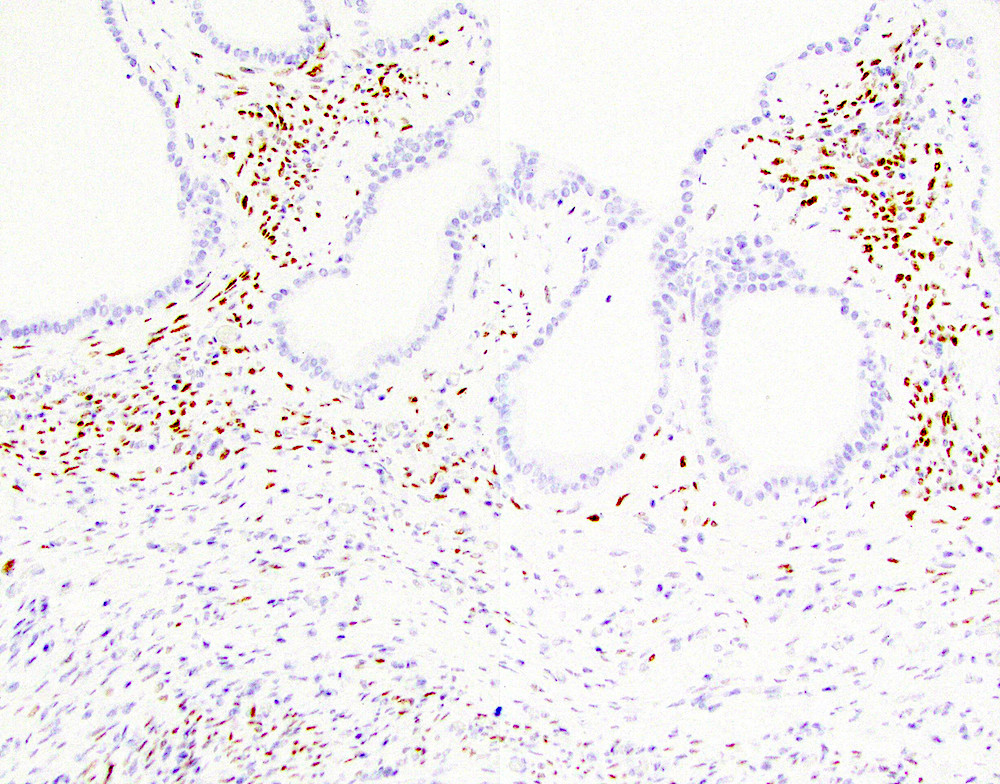
Estrogen receptor
Cytology description
- Cyst aspirates are usually acellular with thick, gelatinous mucus
- Clusters of 3 dimensional atypical glandular cells with hyperchromasia predict at least moderate dysplasia (Arch Pathol Lab Med 2009;133:388)
Cytology images
Contributed by Matthew W. Rosenbaum, M.D.
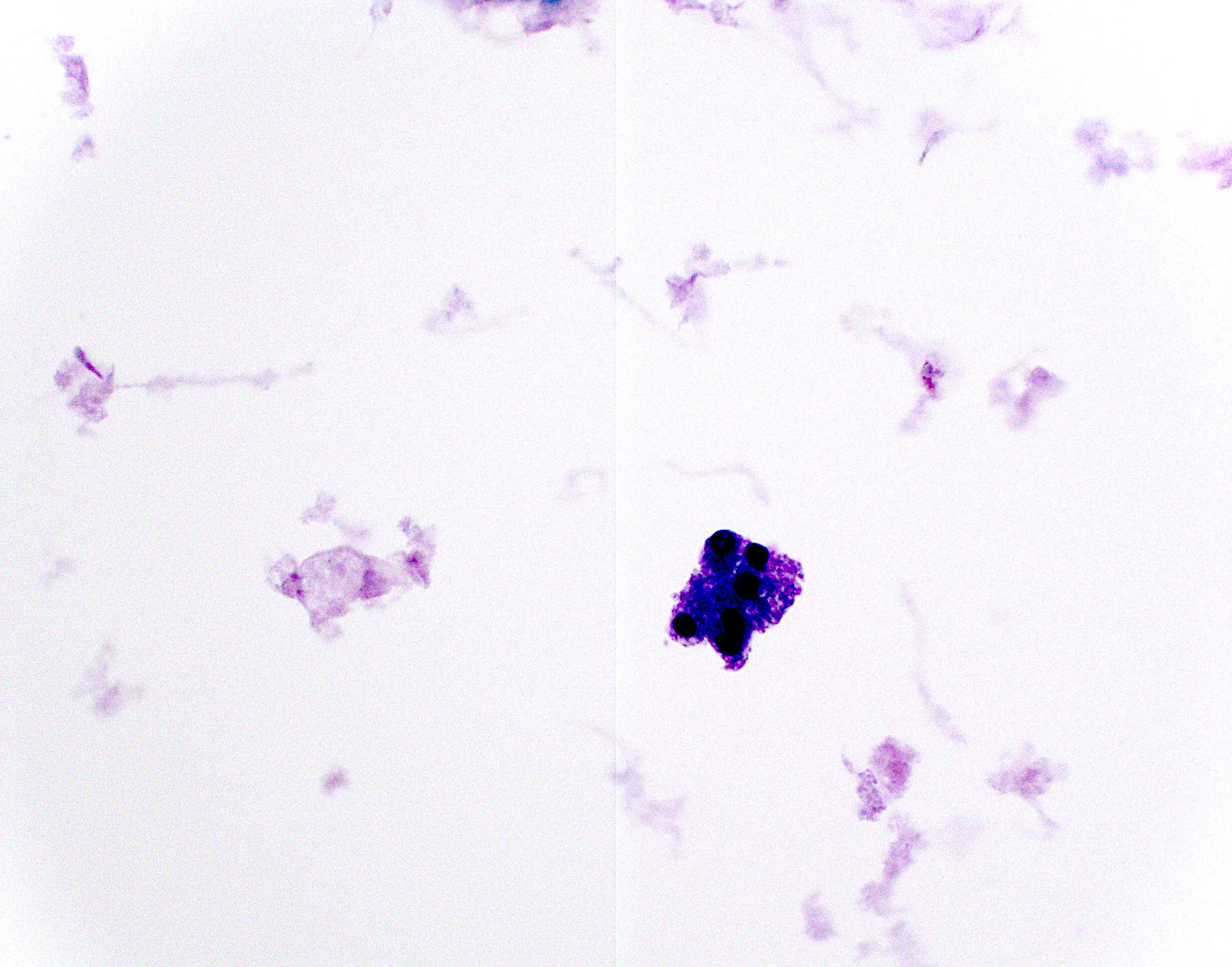
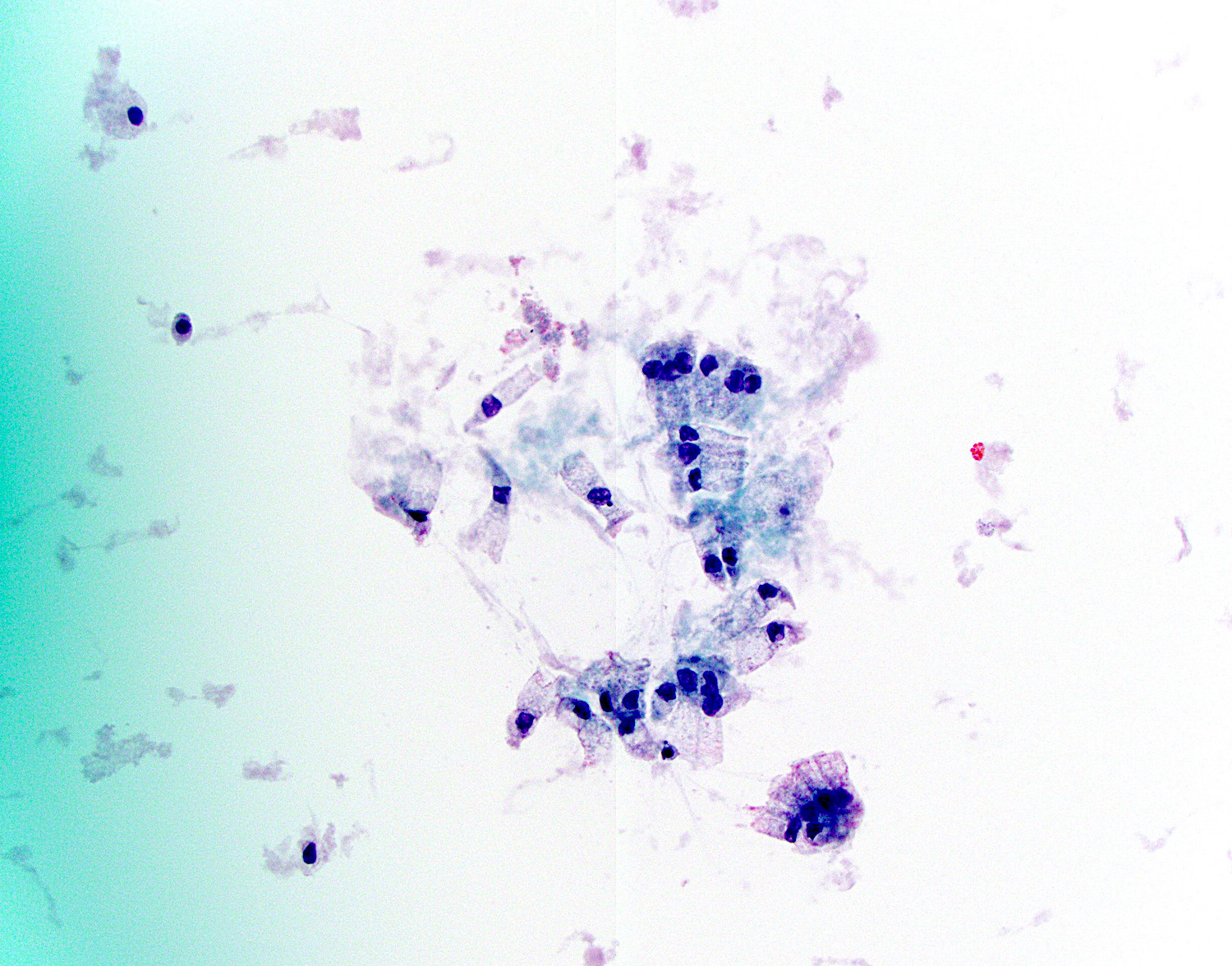

Cytology of mucinous cystic neoplasm
Positive stains
- Ovarian type stroma: CD10, ER, inhibin, PR, smooth muscle actin (SMA) and vimentin (Gut Liver 2015;9:571)
- Epithelium stains carcinoembryonic antigen (CEA), CK7, CK8, CK18 and CK19 (Gut Liver 2015;9:571)
- Gastric type epithelium stains MUC5AC (Gut Liver 2015;9:571)
- DPC4 (MADH4, SMAD4), MUC5AC present in situ areas (usually lost in invasive disease) (Am J Surg Pathol 2000;24:1544, Gut Liver 2015;9:571, Arch Pathol Lab Med 2015;139:24)
- Invasive component stains MUC1
- Cyst fluid may stain positive for Alcian blue and mucicarmine
- S100P in epithelium (Arch Pathol Lab Med 2015;139:24)
- SF1 in stroma (Pathol Int 2016;66:281)
Negative stains
- MUC1 (except in invasive components) (Am J Surg Pathol 2002;26:466, Gut Liver 2015;9:571)
- MUC2 (except for faint staining of goblet cells)
- DPC4 (MADH4, SMAD4) staining is lost in invasive MCNs (Gut Liver 2015;9:571)
- pVHL (Arch Pathol Lab Med 2015;139:24)
Molecular / cytogenetics description
- KRAS mutations noted in in situ or invasive areas, inactivating SMAD4 and TP53 mutations in more advanced MCNs (Gut Liver 2015;9:571)
- Negative for GNAS mutations
Sample pathology report
- Pancreas and duodenum, Whipple resection:
- Mucinous cystic neoplasm with low grade intraepithelial neoplasia (8.3 cm) (see comment)
- Negative for high grade intraepithelial neoplasia or malignancy.
- Focal background chronic pancreatitis
- Margins of resection unremarkable.
- Seven benign lymph nodes.
- Comment: The gross cystic lesion was entirely submitted for microscopic analysis.
- Pancreas and duodenum, Whipple resection:
- Focal adenocarcinoma arising from a mucinous cystic neoplasm (see synoptic report)
Differential diagnosis
- Intraductal papillary mucinous neoplasm:
- Usually at the head of pancreas and communicates with the duct system (MCNs usually do not communicate with the main pancreatic duct)
- IPMNs may be positive for GNAS mutations while MCNs will be negative (Gut Liver 2015;9:571)
- Both have elevated CEA and KRAS mutation in cyst fluid
- Ovarian mucinous tumors:
- Similar clinical and histologic appearance
- Pancreatic ductal adenocarcinoma, large duct variant:
- Will have smaller cysts, clustering of ducts and myxoid stroma (Arch Pathol Lab Med 2009;133:423)
- Pancreatic ductal adenocarcinoma:
- Usually not cystic, shows irregular infiltrative glands with nuclear atypia, no ovarian type stroma
- Pancreatic pseudocyst:
- Mimics MCN when MCN has denuded cyst lining
- MCN cystic fluid has high CEA content and viscosity, high expression of microRNAs, lower amylase (< 250 U/L) and elastase I than pseudocyst, although values may vary within different loculi of same neoplasm (Am J Clin Pathol 1993;100:425, Ann Gastroenterol 2013;26:122, Gastroenterology Res 2014;7:44)
- Serous cystadenoma:
- Has low levels of CEA
Practice question #1
Which of the following findings on fine needle aspiration of a pancreatic cyst are most consistent with a mucinous cystic neoplasm?
- Decreased CEA, decreased amylase, no KRAS mutation, no GNAS mutation
- Elevated CEA, elevated amylase, KRAS mutation, GNAS mutated
- Elevated CEA, highly elevated amylase, no KRAS mutation, no GNAS mutation
- Elevated CEA, variable amylase, KRAS mutation, no GNAS mutation
Practice answer #1
D. Mucinous cystic neoplasms have elevated CEA, variable amylase, KRAS mutation and no GNAS mutation. If a GNAS mutation is present, then the findings will favor an IPMN (answer B). Decreased CEA and amylase with no KRAS or GNAS mutations favor a serous cystadenoma (answer A). An elevated CEA and amylase without KRAS or GNAS mutations will favor a pancreatic pseudocyst (answer C).
Comment Here
Reference: Mucinous cystic neoplasm (MCN)
Comment Here
Reference: Mucinous cystic neoplasm (MCN)
