Placenta
Gestational trophoblastic disease
Molar pregnancies
Hydatidiform mole
Editorial Board Member: Ricardo R. Lastra, M.D.
Deputy Editor-in-Chief: Gulisa Turashvili, M.D., Ph.D.


Last author update: 2 March 2023
Last staff update: 27 March 2025
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Placenta hydatidiform mole
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Sheikh FN, Gupta R, Lanjewar S. Hydatidiform mole. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/placentahydatgeneral.html. Accessed August 27th, 2025.
Definition / general
- Abnormal placentas with variable trophoblastic proliferation and villous hydrops
Essential features
- Proliferative disorder of the placenta resulting in villous hydrops and trophoblastic hyperplasia with or without embryonic development
- Subdivided into complete and partial hydatidiform mole based on morphologic, cytogenetic and clinicopathological features
- Maternal age and history of hydatidiform mole are the most important risk factors
- Pelvic ultrasound shows characteristic snowstorm appearance
- Combination of genotyping and p57 immunostaining is used for diagnosis
Terminology
- Molar pregnancy
Epidemiology
- Incidence of hydatidiform moles has been found to be highest in southeastern Asia, the Middle East and South America while being the lowest in North America and Europe (Acta Oncol 2018;57:1094)
- Incidence in developed countries (Cell Adh Migr 2016;10:226):
- Partial hydatidiform mole: ~3 per 1,000 pregnancies
- Complete hydatidiform mole: ~1 - 3 per 1,000 pregnancies
- Risk factors:
- Maternal age (< 20 and > 40): stronger evidence for complete than partial hydatidiform mole (J Obstet Gynaecol 2013;33:406, Mod Pathol 2020;33:880, Gynecol Oncol 2016;140:470)
- History of miscarriages (Mod Pathol 2020;33:880)
- Asian race (Lancet Oncol 2003;4:670)
- Genetic: familial biparental complete hydatidiform mole (Mod Pathol 2018;31:1116)
- Dietary / lifestyle factors, oral contraceptive pills, history of abortions, parity, etc. have been suggested as risk factors but conclusive evidence is lacking
Sites
- Uterus
- Fallopian tube (ectopic)
Pathophysiology
- Subdivided into complete and partial hydatidiform mole based on morphologic, cytogenetic and clinicopathological features
- Complete hydatidiform mole:
- Monospermic, homozygous complete hydatidiform mole (80 - 90%) results from 1 sperm fertilizing an empty oocyte with reduplication of its genome, leading to a diploid paternal only genome (Surg Pathol Clin 2022;15:197)
- Dispermic, heterozygous complete hydatidiform mole (10 - 20%) results from 2 sperms fertilizing the same empty oocyte (Surg Pathol Clin 2022;15:197)
- Tetraploid complete hydatidiform mole (rare) contains 4 haploid paternal chromosome sets (Am J Surg Pathol 2008;32:445)
- An exceedingly small subset of complete hydatidiform moles (0.6 - 2.6% of all hydatidiform moles) are familial biparental complete moles that result from abnormal genomic imprinting of maternal effect genes (NALP7 / NLRP7 on chromosome 19q13.4, KHDC3L on chromosome 6q1) (Surg Pathol Clin 2022;15:197)
- Partial hydatidiform mole:
- These are diandric monogynic triploid gestations
- Dispermic, heterozygous partial hydatidiform mole (> 95%) results from 2 sperms fertilizing an oocyte (Surg Pathol Clin 2022;15:197)
- Monospermic, homozygous partial hydatidiform mole (less common) results from reduplication of a sperm's genome when it fertilizes an oocyte (Am J Surg Pathol 2008;32:445)
- Rare cases of tetraploid partial hydatidiform moles have been reported (Surg Pathol Clin 2022;15:197)
Etiology
- Presence of excess paternal genome
Clinical features
- Patients typically present with symptoms consistent with early pregnancy or its complications
- Common features: vaginal bleeding, pelvic pressure / pain, enlarged uterus, hyperemesis gravidarum
- Less common or late features: anemia, vaginal passage of hydropic vessels; in complete hydatidiform mole, complications due to high human chorionic gonadotropin (hCG) levels include hyperthyroidism, theca lutein cysts, pulmonary embolization of trophoblast and early onset of preeclampsia
- References: Int J Gynaecol Obstet 2015;131:S123, Kurman: Blaustein's Pathology of the Female Genital Tract, 7th Edition, 2019
Diagnosis
- Pelvic ultrasound
- Dilation and curettage / uterine evacuation
Laboratory
- High hCG levels (complete hydatidiform mole > partial hydatidiform mole)
Radiology description
- Pelvic ultrasound:
- Complete hydatidiform mole (Ultrasound Obstet Gynecol 2006;27:56):
- Absent embryo
- Absent amniotic fluid
- Central heterogeneous mass with numerous anechoic spaces (also called snowstorm pattern)
- Ovarian theca lutein cysts
- Partial hydatidiform mole (Obstet Gynecol 1989;73:414):
- Fetus may be identified but is often growth restricted
- Amniotic fluid is present, typically low in volume
- Placenta shows ≥ 1 abnormal finding(s) (snowstorm appearance, increased echogenicity of chorionic villi)
- Increased transverse diameter of the gestational sac
- Theca lutein cysts are usually absent
- Complete hydatidiform mole (Ultrasound Obstet Gynecol 2006;27:56):
Radiology images
Images hosted on other servers:

Complete hydatidiform mole with cystic areas

Partial hydatidiform mole
Prognostic factors
- Increased risk of persistent gestational trophoblastic disease (0.5 - 5% in partial hydatidiform mole, 15 - 20% in complete hydatidiform mole) (Lancet 2010;376:717)
- Risk of persistent gestational trophoblastic disease is higher with heterozygous complete hydatidiform mole than with homozygous complete hydatidiform mole (Int J Gynecol Pathol 2016;35:134)
- Risk of gestational choriocarcinoma is < 0.5% in partial hydatidiform mole and 2 - 3% in complete hydatidiform mole
Case reports
- 21 year old woman with history of severe preeclampsia at 28 weeks gestation with ultrasound scans showing molar changes in the placenta with a viable fetus (J Med Case Rep 2018;12:140)
- 24 year old gravida 2 para 1 woman who presented at 28 weeks gestation with severe preeclampsia and vulvar edema and ultrasound scan showing a live intrauterine pregnancy in addition to a large hydatidiform mole (Gynecol Oncol Rep 2019;31:100519)
- 33 year old woman with a history of sudden onset of right iliac fossa pain and mild vaginal bleeding following 8 weeks of amenorrhea and a positive pregnancy test (BMJ Case Rep 2018;2018:bcr2018225545)
Treatment
- Surgical removal of the molar pregnancy followed by surveillance of hCG levels to confirm disease resolution or to identify the development of gestational trophoblastic neoplasia
Gross description
- Complete hydatidiform mole:
- Well developed complete hydatidiform mole shows large specimen with villous hydrops (bunch of grapes)
- Swollen villi may range from a few millimeters to as large as 3.0 cm in diameter (average: ~1.5 cm)
- Very early complete hydatidiform mole may not show gross abnormalities
- Fetal parts are absent, regardless of gestational age
- Partial hydatidiform mole:
- First trimester: unremarkable
- Second trimester: focal fetal hydrops
- Fetus may be present with developmental anomalies
- Reference: Surg Pathol Clin 2022;15:197
Gross images
Images hosted on other servers:

Hydatidiform mole (left) and normal placenta (right)
Microscopic (histologic) description
- Complete hydatidiform mole (well developed):
- Diffuse villous enlargement and marked villous hydrops with cistern formation
- Circumferential trophoblastic hyperplasia
- Cytologic atypia of intermediate trophoblasts at the implantation site
- Smooth villous contours but surface invaginations with trophoblastic pseudoinclusions may also occur
- Absence of fetal vessels and fetal red blood cells
- Complete hydatidiform mole (early):
- No significant villous enlargement or hydrops
- Polypoid, irregular villous shape
- Hypercellular, myxoid villous stroma with apoptosis of primitive stellate cells
- Labyrinthine network of villous stromal canaliculi
- Focal hyperplasia of cytotrophoblasts and syncytiotrophoblasts on both villi and the undersurface of the chorionic plate
- Atypical trophoblasts lining the villi and at the implantation site
- Rare primitive fetal vessels and fetal red blood cells
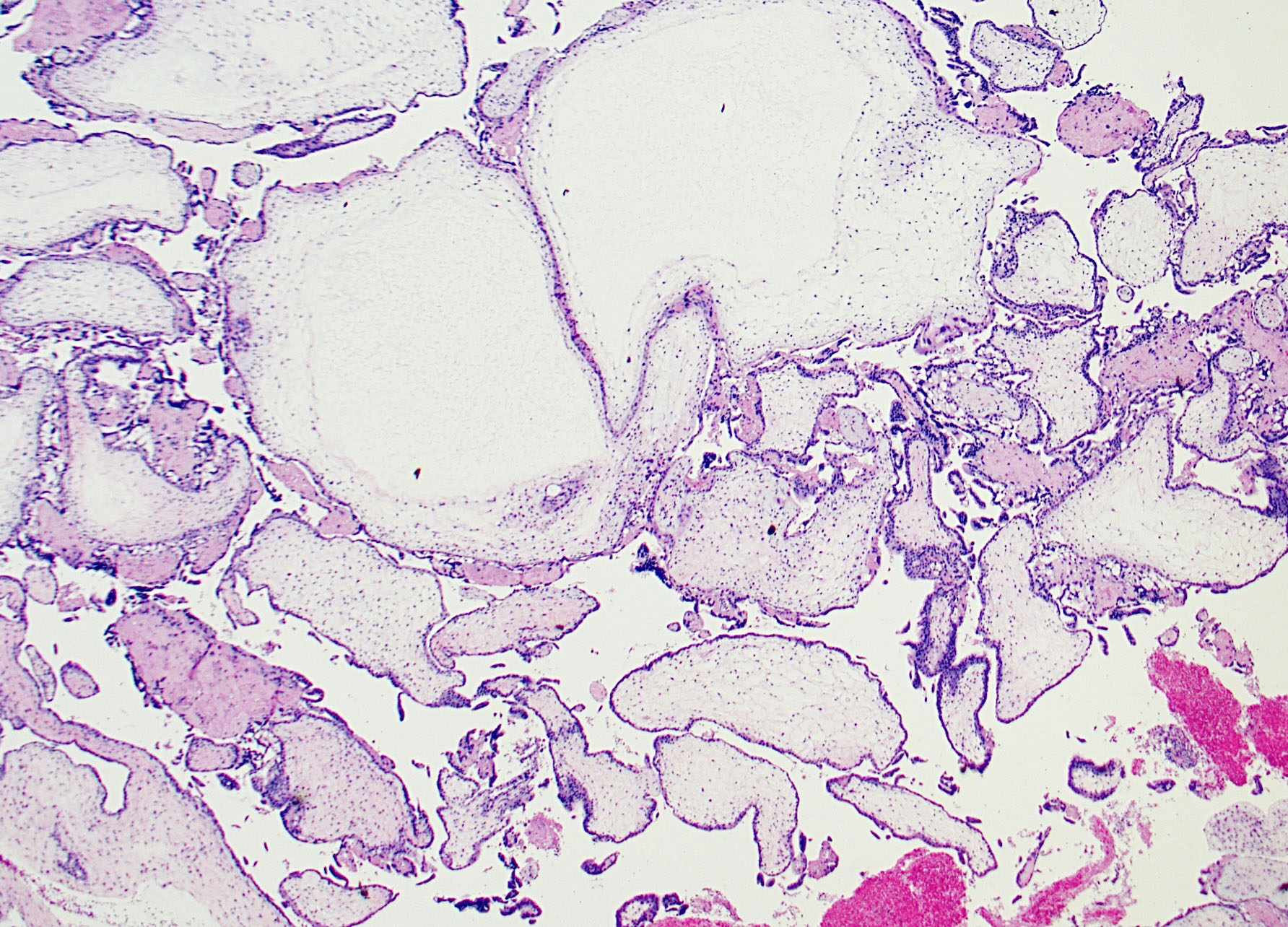
- Partial hydatidiform mole:
- 2 villous populations seen: large hydropic and small fibrotic villi
- Villous enlargement and hydrops with cistern formation
- Scalloped villi with surface invaginations and trophoblastic pseudoinclusions
- Prominent syncytiotrophoblastic knuckles
- Minimal trophoblastic hyperplasia
- Fetal vessels with nucleated red cells are usually present
- Cytologic atypia is not significant
- Reference: Surg Pathol Clin 2022;15:197
Microscopic (histologic) images
Contributed by Fahad N. Sheikh, M.D.
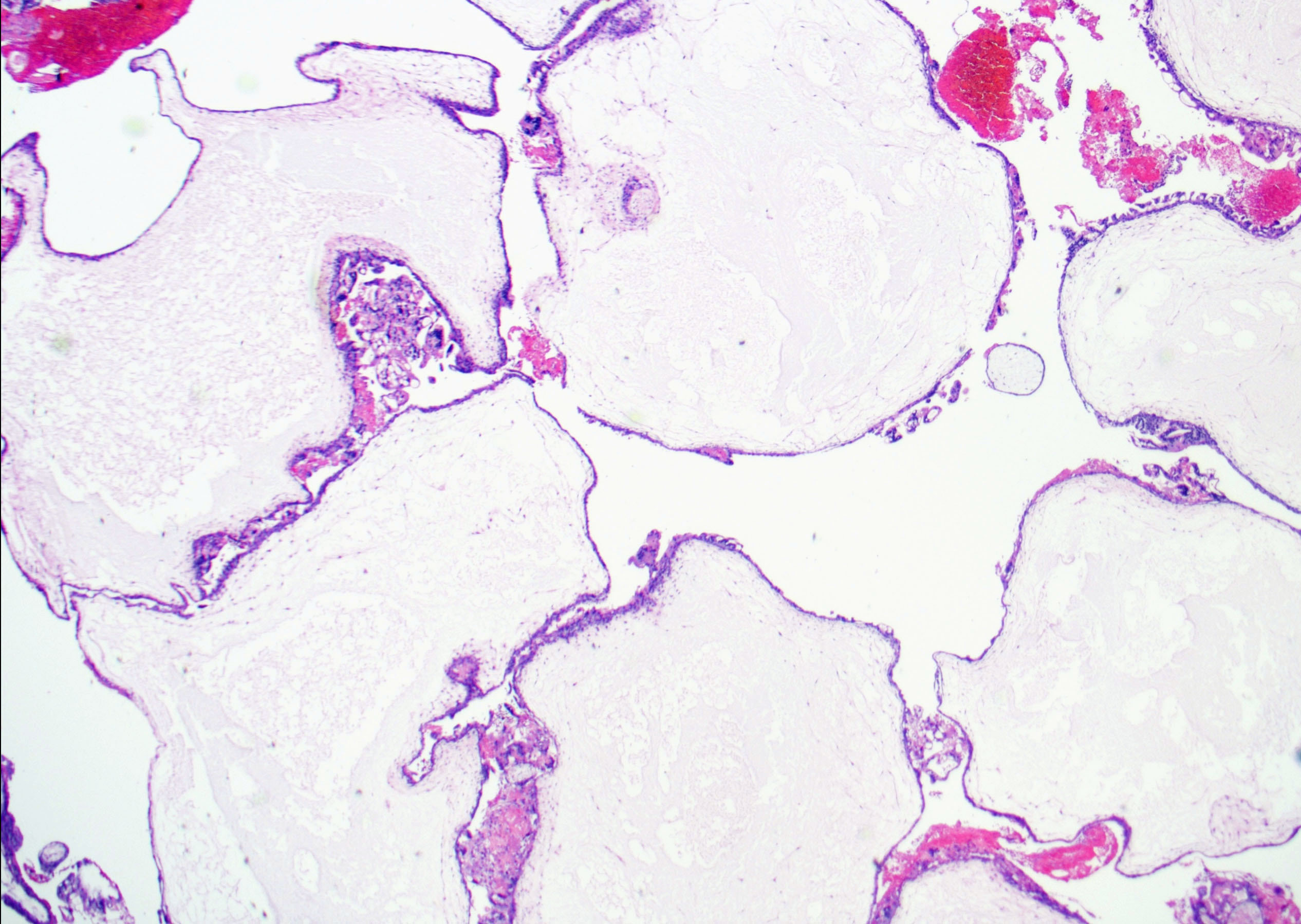
Hydropic villi
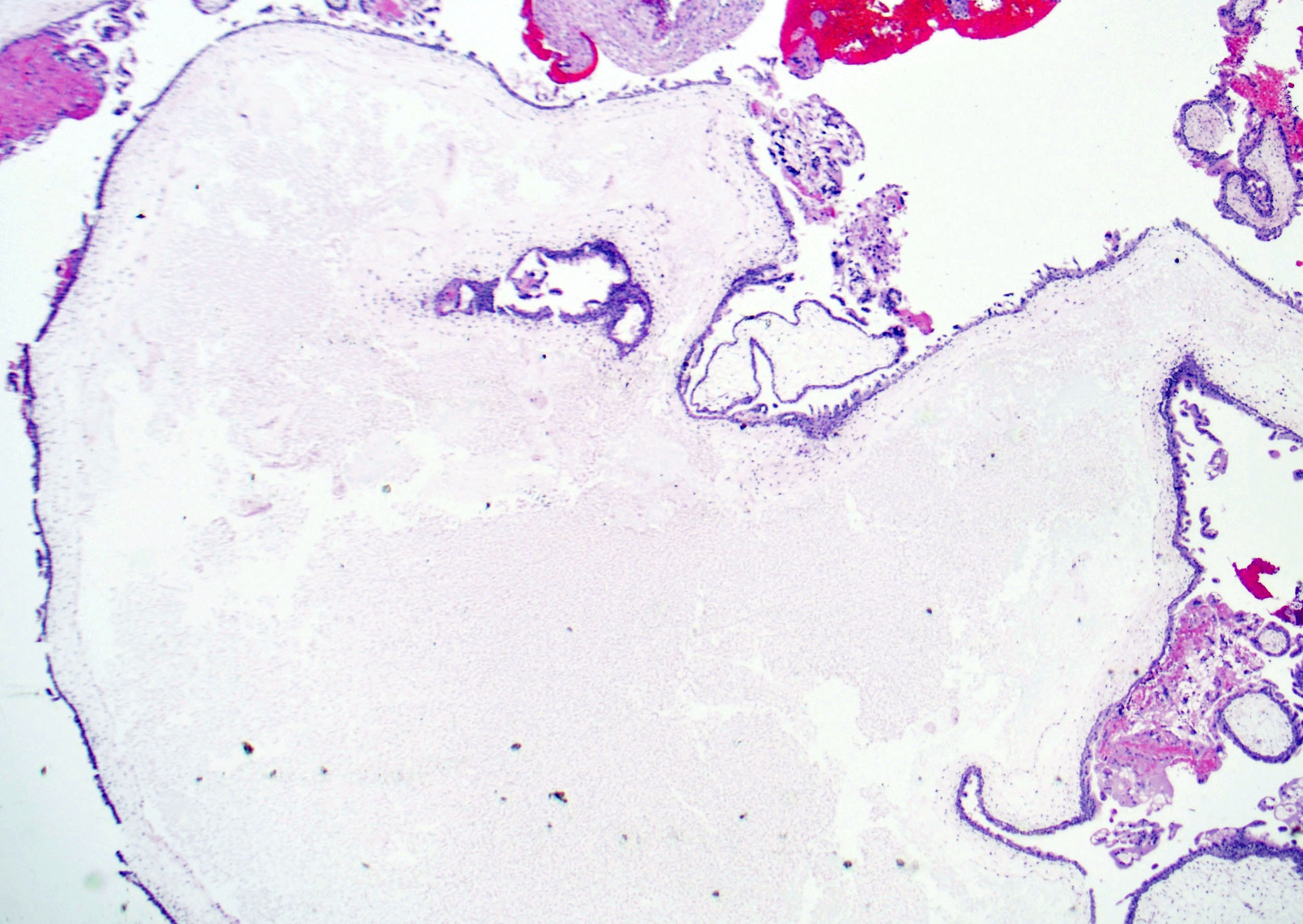
Cistern formation
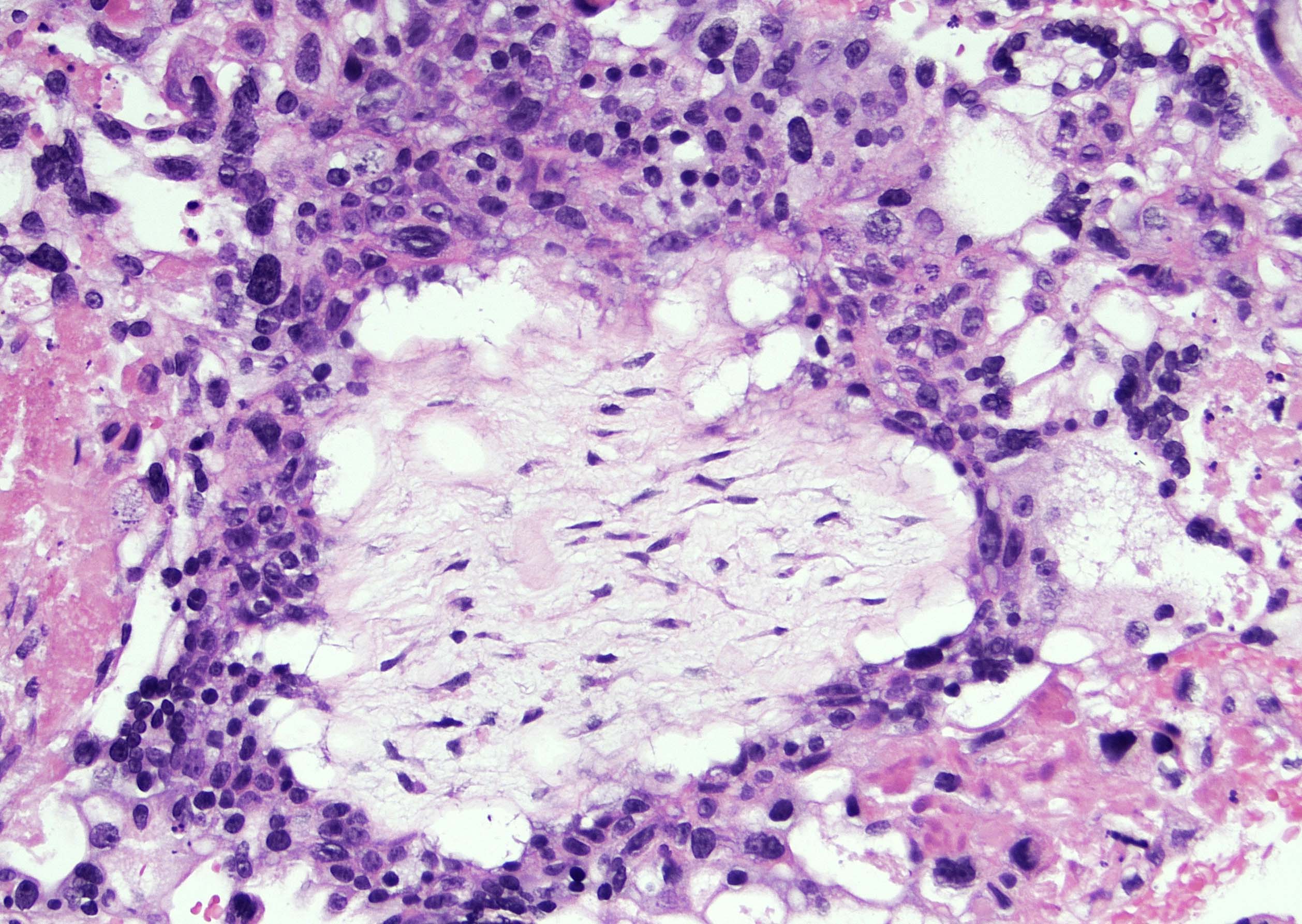
Circumferential trophoblastic proliferation
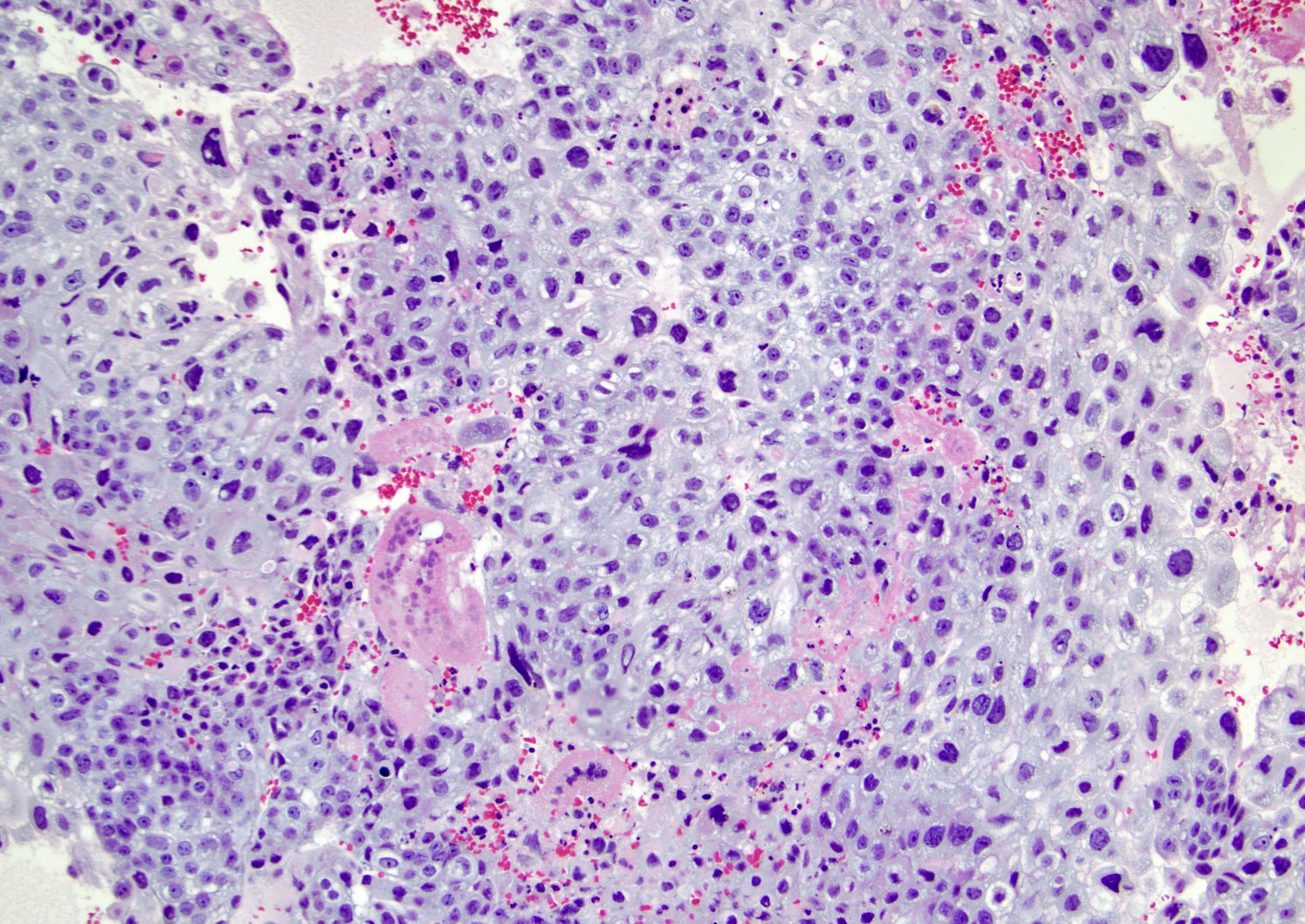
Trophoblastic proliferation and atypia
Partial mole with 2 populations of villi
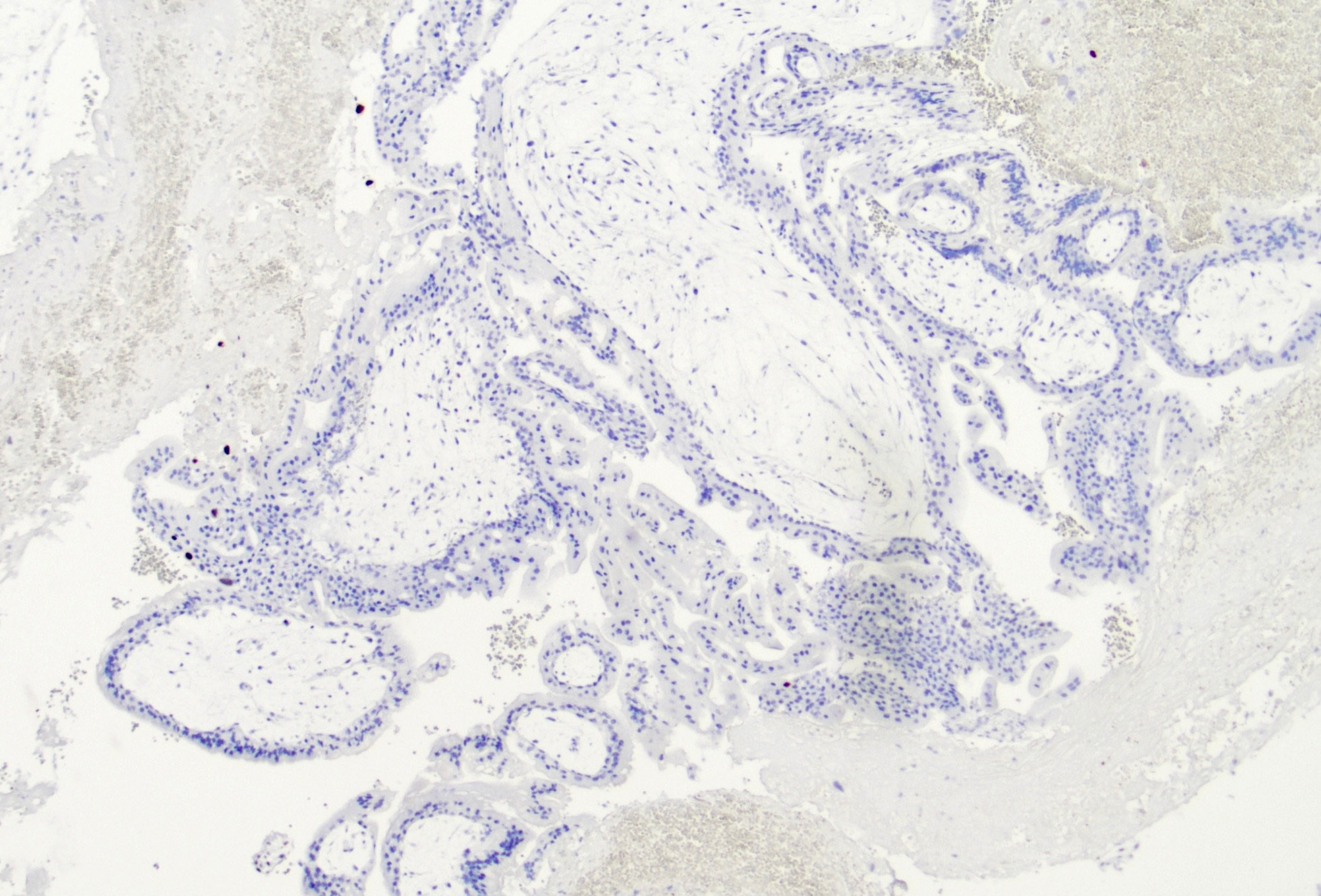
p57 immunostain
Virtual slides
Images hosted on other servers:

Partial hydatidiform mole

Complete hydatidiform more
Positive stains
- Intact nuclear expression of p57 in the villous cytotrophoblast and villous stromal cells in partial hydatidiform mole (Semin Diagn Pathol 2014;31:223)
- hCG, HPL, PLAP (Acta Pathol Jpn 1993;43:683)
Negative stains
- Loss of nuclear p57 expression in the villous cytotrophoblast and villous stromal cells in complete hydatidiform mole (Semin Diagn Pathol 2014;31:223)
Molecular / cytogenetics description
- Short tandem repeat (STR) DNA genotyping
- Complete mole shows absence of maternal genetic contribution
- Partial mole shows diandric triploidy
Sample pathology report
- Uterine contents, removal:
- Complete hydatidiform mole (see comment)
- Comment: Immunohistochemical stain for p57 is negative in cytotrophoblasts and villous stromal cells. DNA ploidy shows a diploid content. The results support the diagnosis above.
Differential diagnosis
- Nonmolar hydropic abortus:
- Enlarged edematous villi with rare cistern formation
- Polar trophoblastic proliferation is an important clue
- No cytologic atypia
- p57 positive in cytotrophoblasts and villous stromal cells
- Molecular tests: biparental diploidy
- Placental mesenchymal dysplasia:
- Placentomegaly and grape-like vesicles
- Usually associated with a normal fetus
- Absence of trophoblastic proliferation
- Association with Beckwith-Wiedemann syndrome (Histopathology 2001;39:447)
- Increased AFP but normal hCG (Nihon Sanka Fujinka Gakkai Zasshi 1994;46:562)
- Normal karyotype
- Chromosomal trisomy syndromes:
- Can display a range of morphologic features, which include dysmorphic villi, trophoblastic pseudoinclusions or cistern formation
- Genetic testing is required to determine the abnormality
- Choriocarcinoma:
- Sheets of highly atypical biphasic population of trophoblastic cells with hemorrhage and necrosis
- Invasion of surrounding tissue and vasculature
- Typically, absence of villi is the rule, except in cases of choriocarcinomas arising in the setting of complete mole or in case of intraplacental choriocarcinoma
Additional references
Practice question #1
Which of the following is true regarding hydatidiform moles?
- Both partial and complete moles are most commonly monospermic and homozygous
- Heterozygous complete mole has a higher risk of postmolar gestational trophoblastic disease / neoplasia than homozygous complete mole
- Immunohistochemical staining for p57 is negative in partial and complete hydatidiform moles
- The typical genetic profile of a partial mole is digynic triploidy
Practice answer #1
B. Heterozygous complete mole has a higher risk of postmolar gestational trophoblastic disease / neoplasia than homozygous complete mole. Immunostaining for p57 is positive in partial and negative in complete hydatidiform mole (C). Although complete moles are most commonly monospermic and homozygous, partial moles are more frequently dispermic and heterozygous (A) with diandric monogynic triploidy (D).
Comment Here
Reference: Hydatidiform mole
Comment Here
Reference: Hydatidiform mole
Practice question #2
The image above shows products of conception in a 34 year old patient. Which of the following is true regarding this entity?
- Amniotic fluid is absent
- Can be associated with ovarian theca lutein cysts
- Can result from abnormal genomic imprinting of maternal KHDC3L gene
- Risk of choriocarcinoma is < 0.5%
Practice answer #2
D. Risk of choriocarcinoma is < 0.5%. The image shows features of partial hydatidiform mole. Partial moles have a much lower risk of choriocarcinoma (< 0.5%) than complete moles (2 - 3%). Amniotic fluid is typically present in partial moles (A). Ovarian theca lutein cysts (B) and genomic imprinting of maternal KHDC3L gene (C) are commonly associated with complete moles, not partial moles.
Comment Here
Reference: Hydatidiform mole
Comment Here
Reference: Hydatidiform mole
