Skin nontumor
Vesiculobullous and acantholytic reaction patterns
Bullous pemphigoid
Editorial Board Member: Kiran Motaparthi, M.D.


Last author update: 22 June 2021
Last staff update: 22 June 2021
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: skin bullous pemphigoid [title] pathology review[ptyp]
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Immunofluorescence description | Immunofluorescence images | Videos | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Occidental M, Kim RH. Bullous pemphigoid. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorbullouspemphigoid.html. Accessed September 13th, 2025.
Definition / general
- Most common autoimmune blistering skin disorder
- Characterized by autoantibodies against hemidesmosomal antigens, bullous pemphigoid antigens 1 and 2
- Patients present with tense bullae on an erythematous base and pruritus
Essential features
- Subepidermal blister with eosinophils, often accompanied by eosinophilic spongiosis
- Early lesions can appear urticarial or eczematous
- Direct immunofluorescence (DIF): linear C3 > IgG along the basement membrane zone, n-serrated pattern
- DIF on salt split skin: immunoreactants deposited on the blister roof (40%) or on both roof and floor (60%)
- Indirect immunofluoresence: can be performed on human skin or monkey esophagus; immunoreactants localize to blister roof (95%) on salt split analysis
- Treatment: corticosteroids, tetracyclines, cytotoxic steroid sparing agents and rituximab, IVIG infusions
ICD coding
- ICD-10: L12.0 - bullous pemphigoid
Epidemiology
- Incidence rate: 7.63 per 100,000 person years (Br J Dermatol 2021;184:68)
- Increases with age
- 80% of subepidermal immunobullous dermatoses
- M = F
- Elderly > children and infants
Sites
- Inner and anterior thighs, groin, flexor surfaces of upper extremities, lower abdomen
- Childhood bullous pemphigoid: vulvar localization is most common
Pathophysiology
- Development of IgG autoantibodies against hemidesmosomal proteins BPAG1 and BPAG2
Etiology
- Autoimmune disease associated with bullous pemphigoid antigen 180 (BP180, BPAG2) and bullous pemphigoid antigen 230 (BP230, BPAG1, BPAG1e) (Am J Clin Dermatol 2017;18:513)
- Associated with medication use:
- Anti-PD1 immunotherapy
- Diuretics, ACE inhibitors, antibiotics, D penicillamine
- Pediatric cases associated with viral illness and immunization (BMC Pediatr 2017;17:60)
Clinical features
- Prodrome phase: mild to severe pruritus and eczematous, papular or urticarial lesions
- Bullous stage: tense bullae containing serous fluid or hemorrhage
- Unusual to have mucosal involvement (seen in oral cavity in 10 - 30% of cases) (Lancet 2013;381:320)
Diagnosis
- Requires histological evaluation in addition to confirmation by direct immunofluorescence studies or detection of circulating autoantibodies
Laboratory
- Enzyme linked immunosorbent assay (ELISA):
- NC16A domain of BPAG2: sensitivity = 84%, specificity = 98% (J Dermatol Sci 2002;30:224)
- BPAG1: sensitivity = 48%, specificity = 94% (Arch Dermatol Res 2016;308:269)
Prognostic factors
- 30% relapse during first year of treatment (N Engl J Med 2002;346:321)
- Risk factors: disease severity, neurological conditions, positive anti-BP180 antibody titers (Ann Med 2018;50:234)
Case reports
- 61 year old man with tender blisters on his feet, upper legs and central upper back, diagnosed with dyshidrosiform bullous pemphigoid (Cureus 2020;12:e6630)
- 72 year old woman with metastatic non small cell lung cancer develops nivolumab induced bullous pemphigoid (Oncologist 2018;23:1119)
- 84 year old woman with clear cell renal cell carcinoma and widespread paraneoplastic bullous pemphigoid (Urol Case Rep 2020;30:101119)
- 88 year old woman with newly diagnosed melanoma and associated bullous pemphigoid (Melanoma Res 2017;27:65)
Treatment
- First line: topical or systemic corticosteroids
- Systemic corticosteroid therapy should be accompanied by steroid sparing agents whenever possible (Am J Clin Dermatol 2017;18:513)
- Steroid sparing agents (mycophenolate mofetil, methotrexate)
- Tetracycline
- IVIG in steroid resistant disease
- Rituximab or IVIG for refractory disease (not resistant)
Clinical images
Images hosted on other servers:

Tense bullae

Ruptured bullae
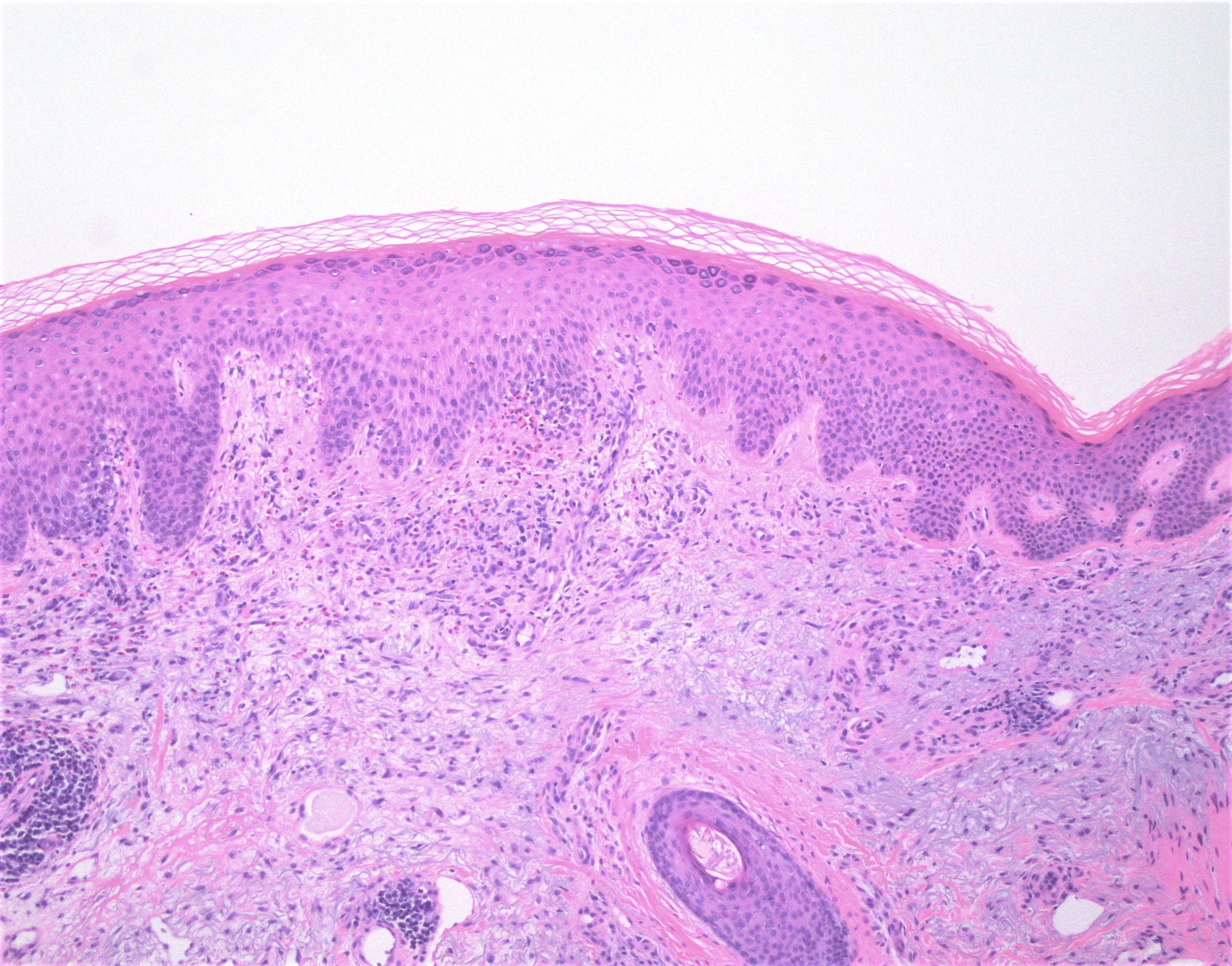
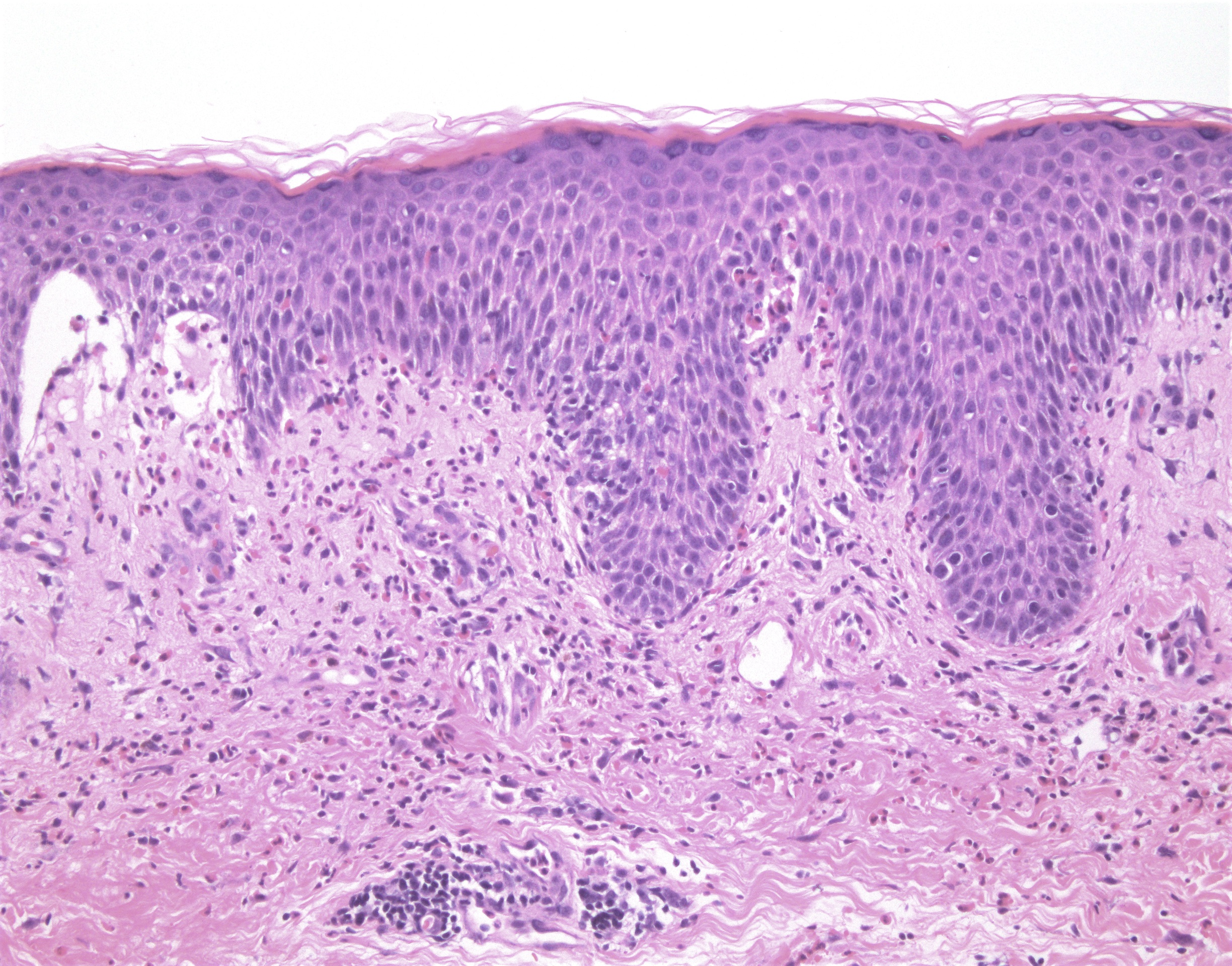
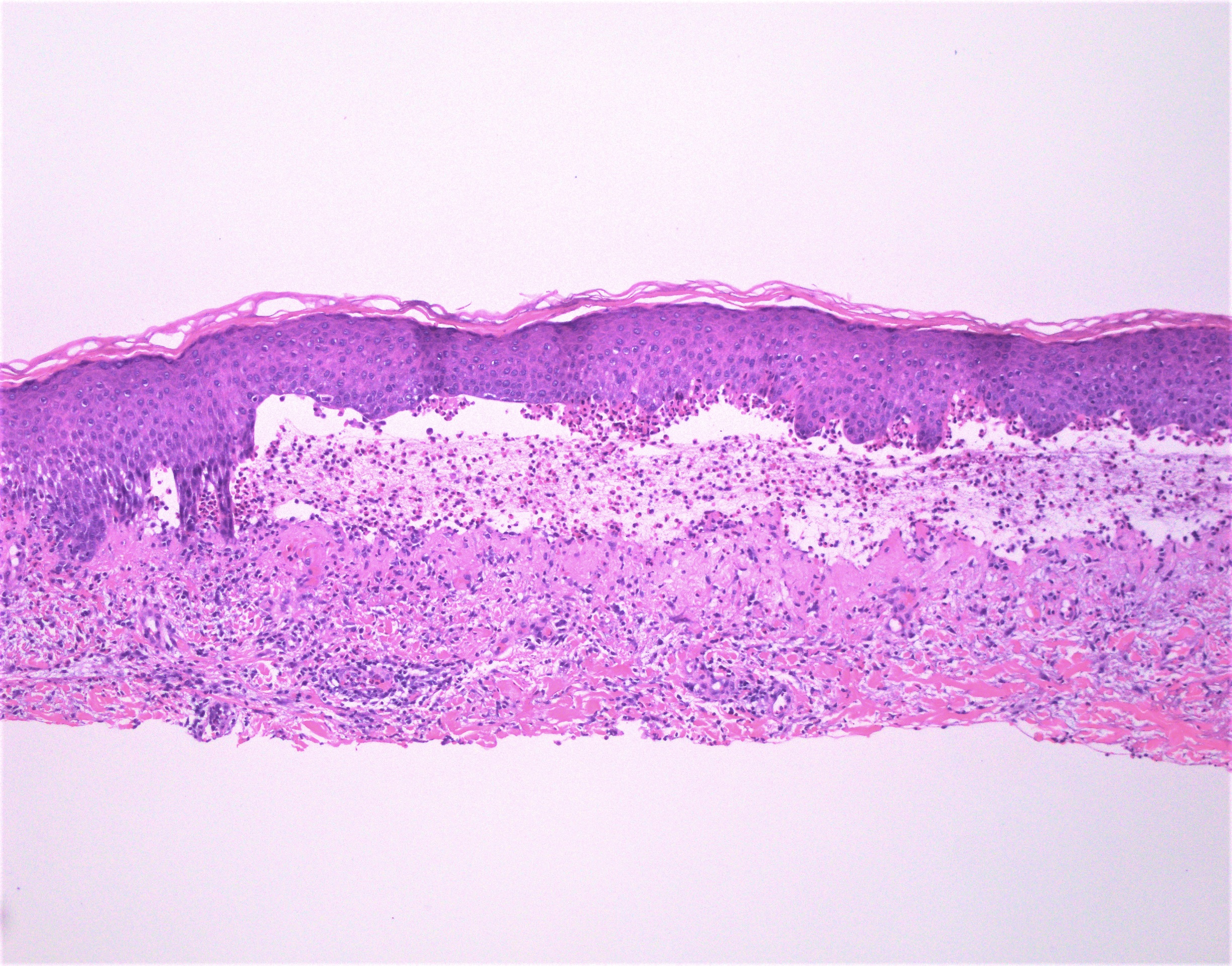
Microscopic (histologic) description
- Subepidermal blister
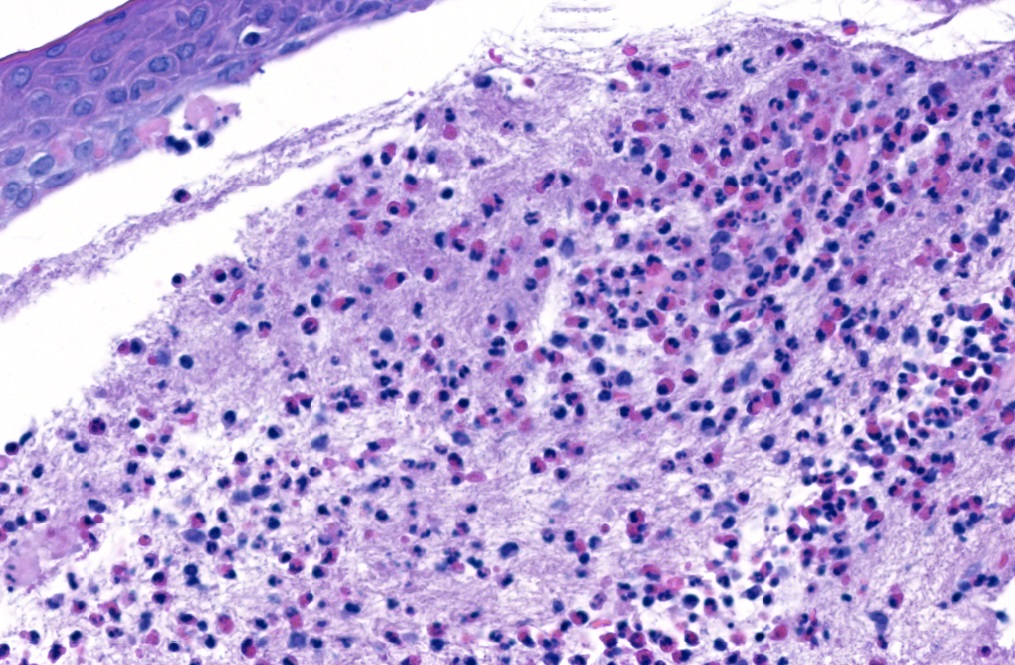
- Superficial perivascular mixed inflammatory infiltrate with eosinophils in the dermis and blister cavity
- Eosinophils may line up along the dermal epidermal junction and extend into the epidermis (eosinophilic spongiosis) (Am J Clin Dermatol 2017;18:513)
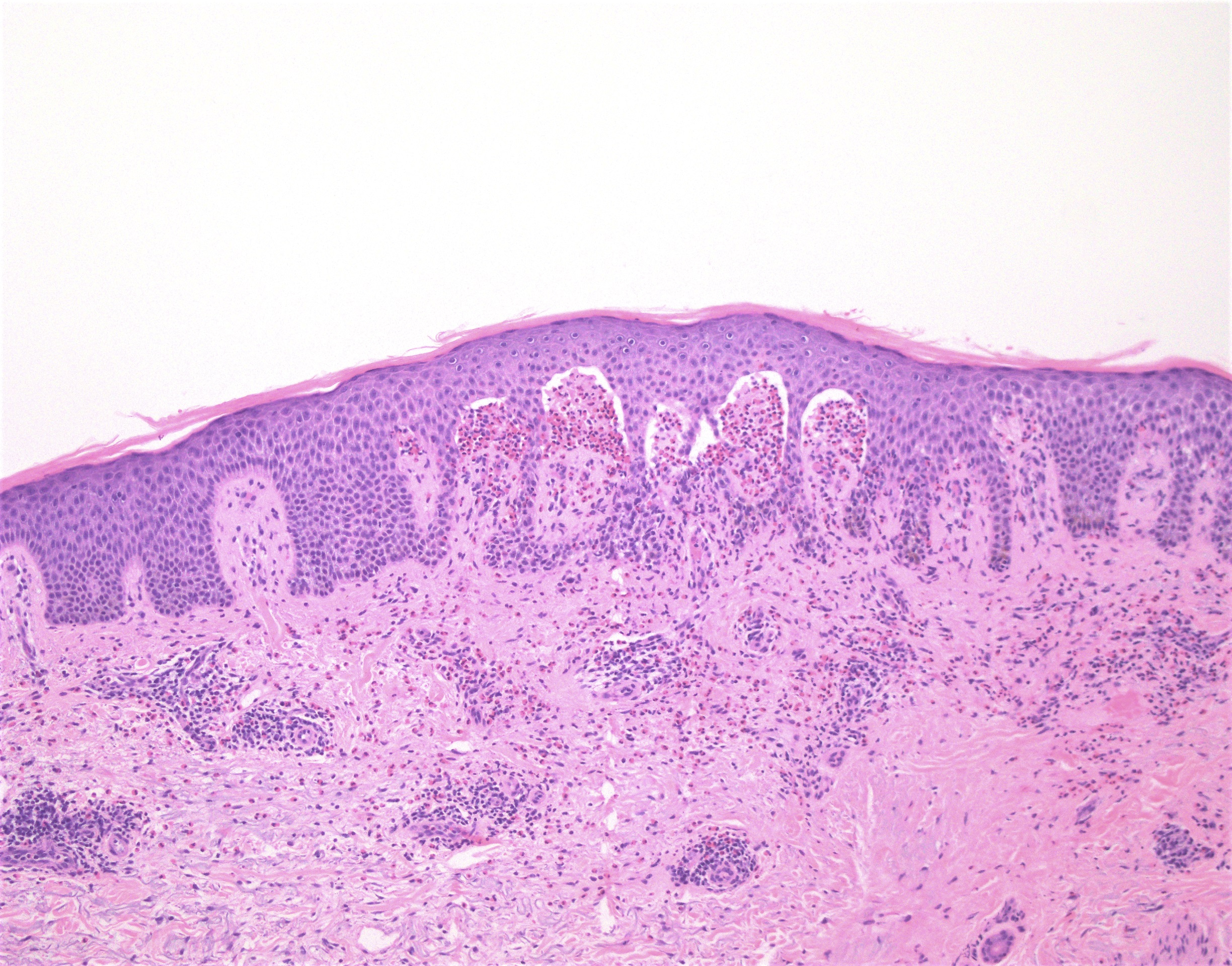
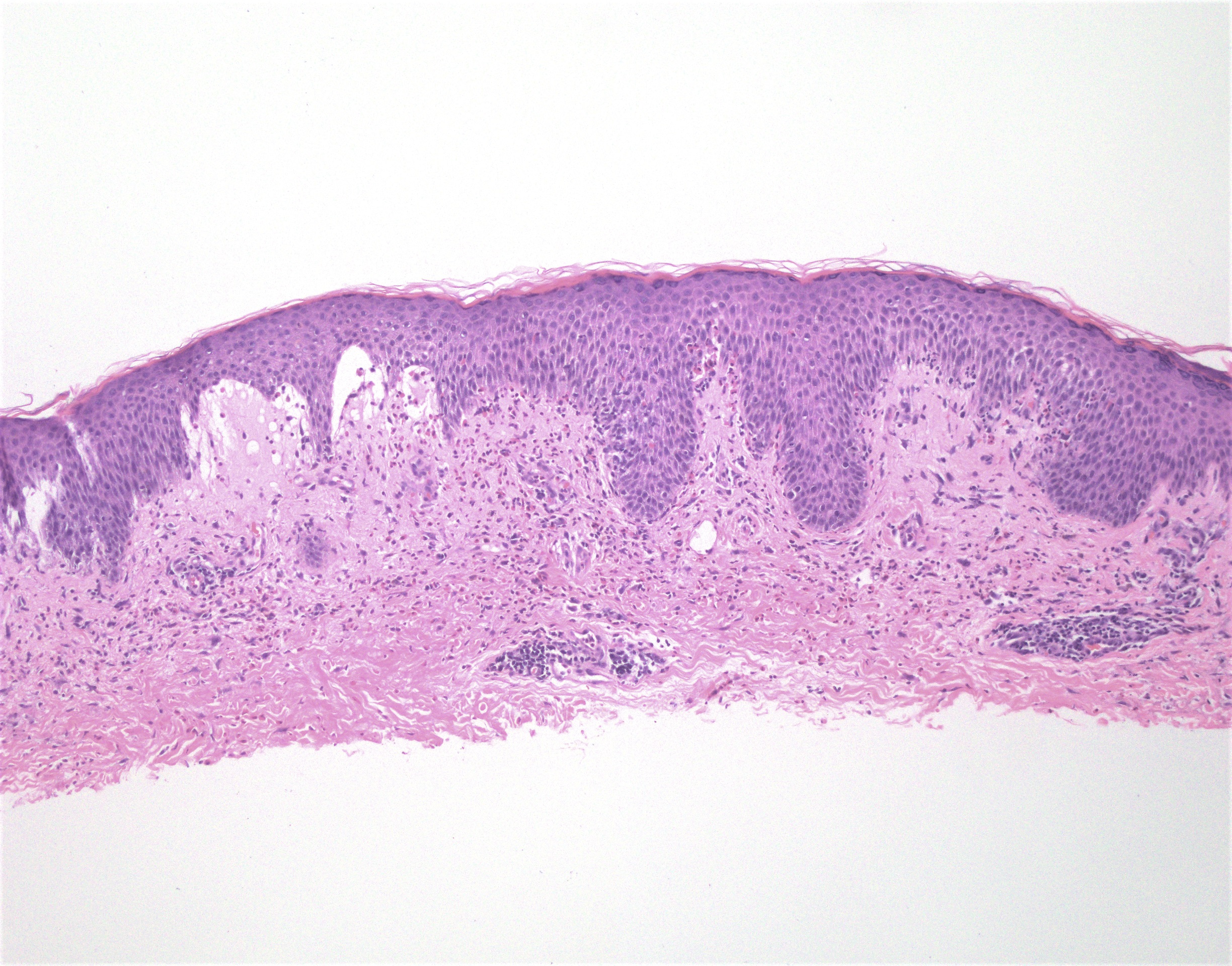
- Urticarial stage:
- Eosinophil rich perivascular and interstitial infiltrate in the papillary dermis
- Eosinophilic spongiosis with pseudovacuolar interface change
- Rare eosinophilic flame figures
- Uncommon presentations include neutrophil rich and cell poor infiltrates
Microscopic (histologic) images
Contributed by Michael Occidental, M.D. and Randie H. Kim, M.D., Ph.D.
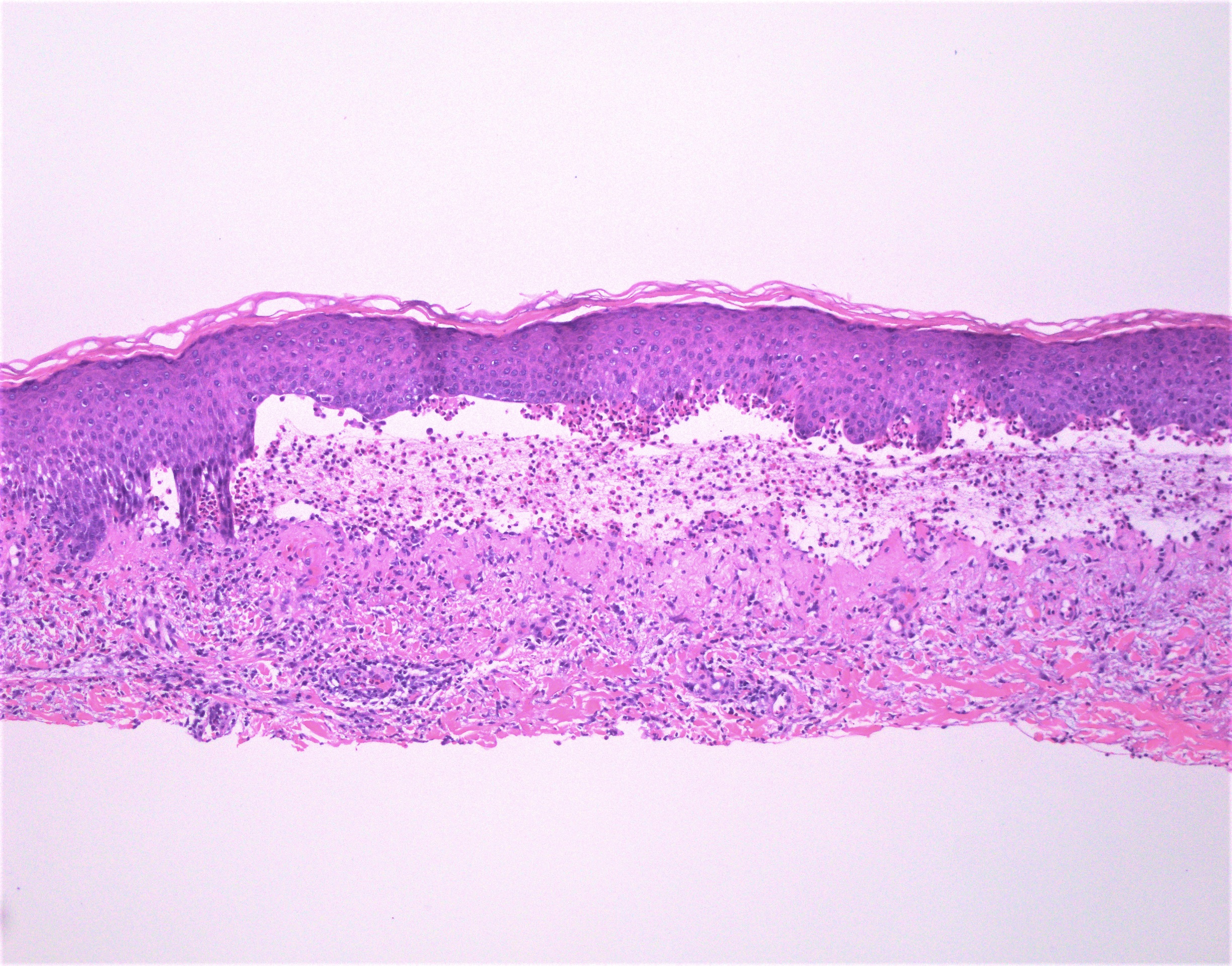
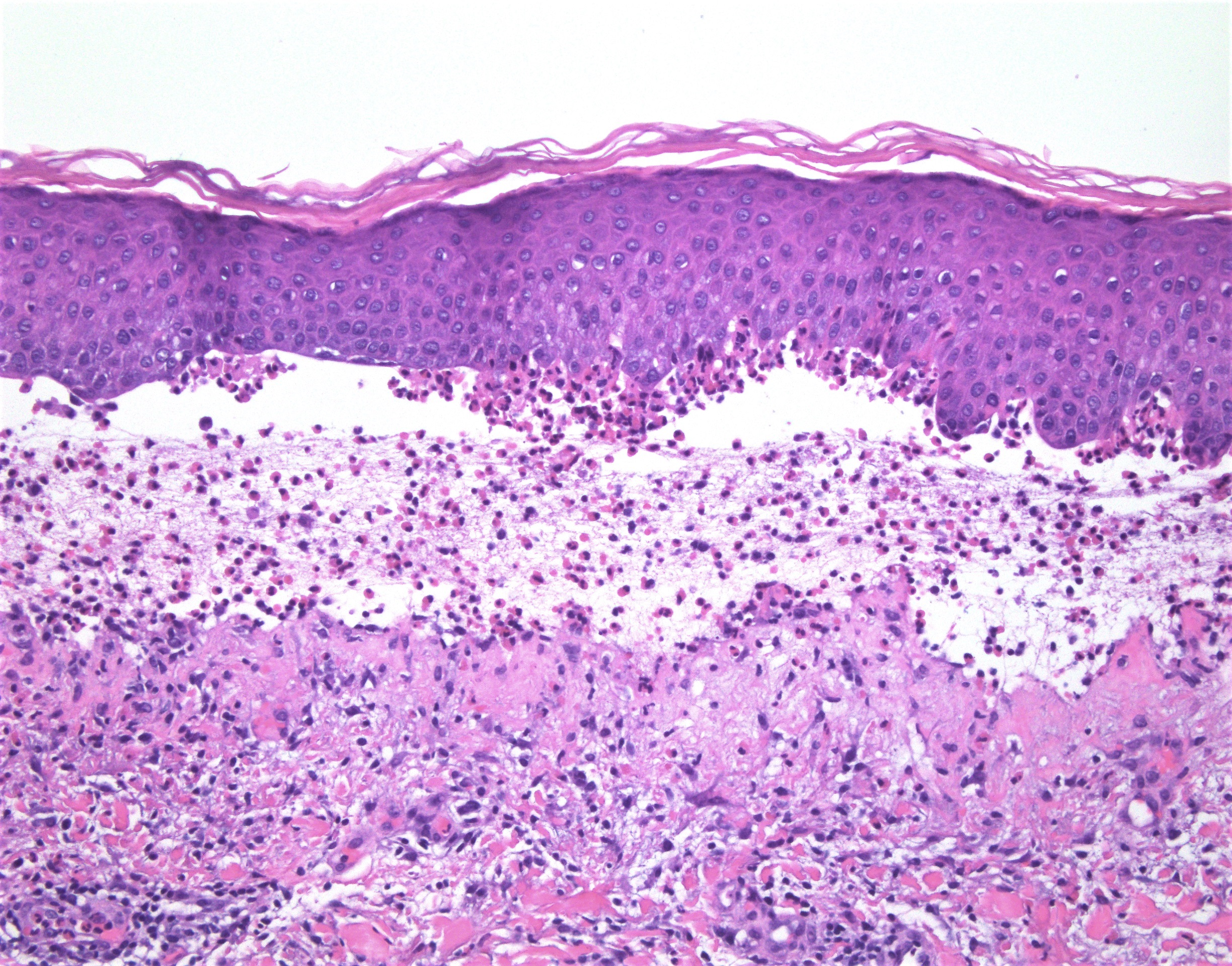
Subepidermal blister with eosinophils
Eosinophil microabscesses in papillary dermis
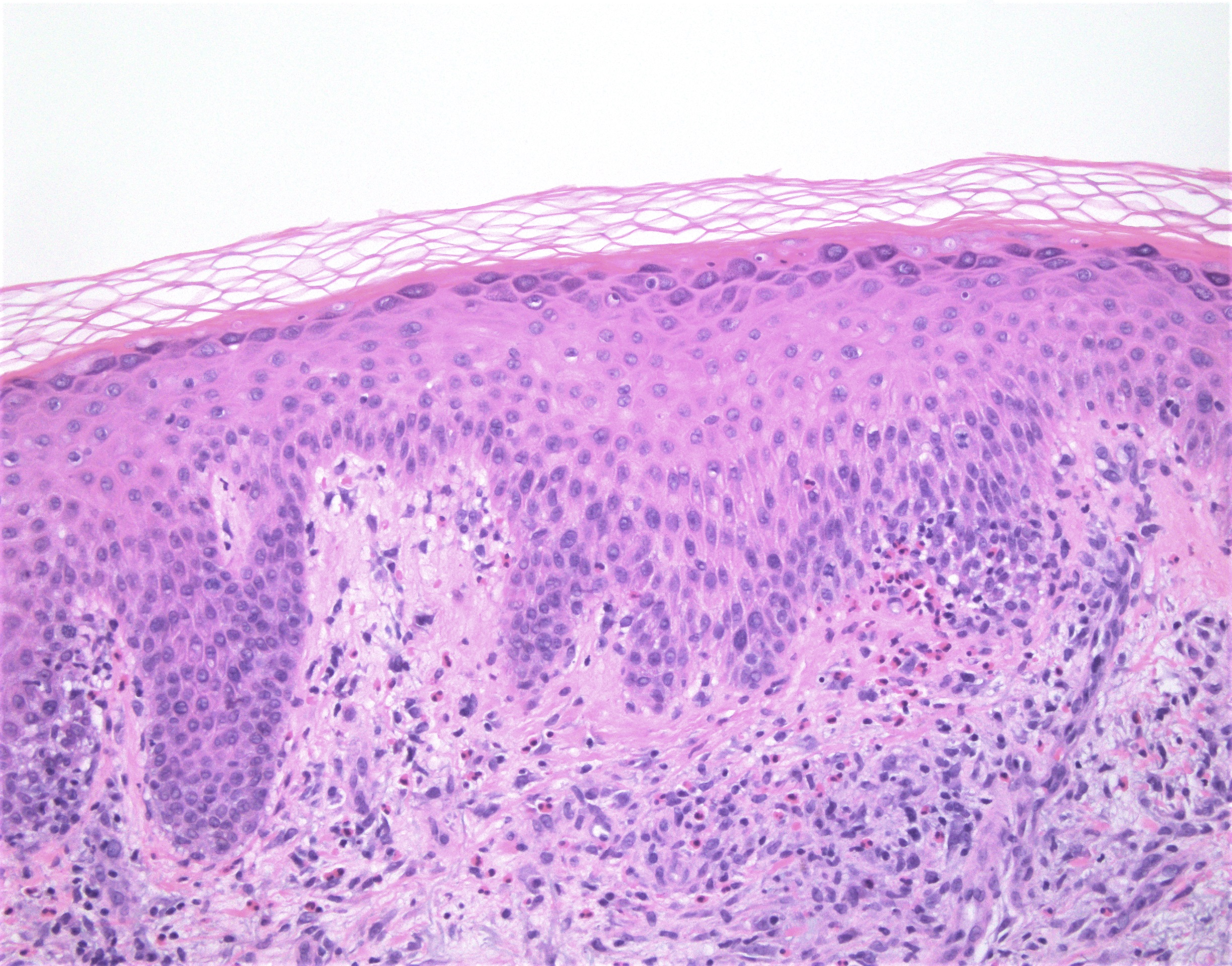
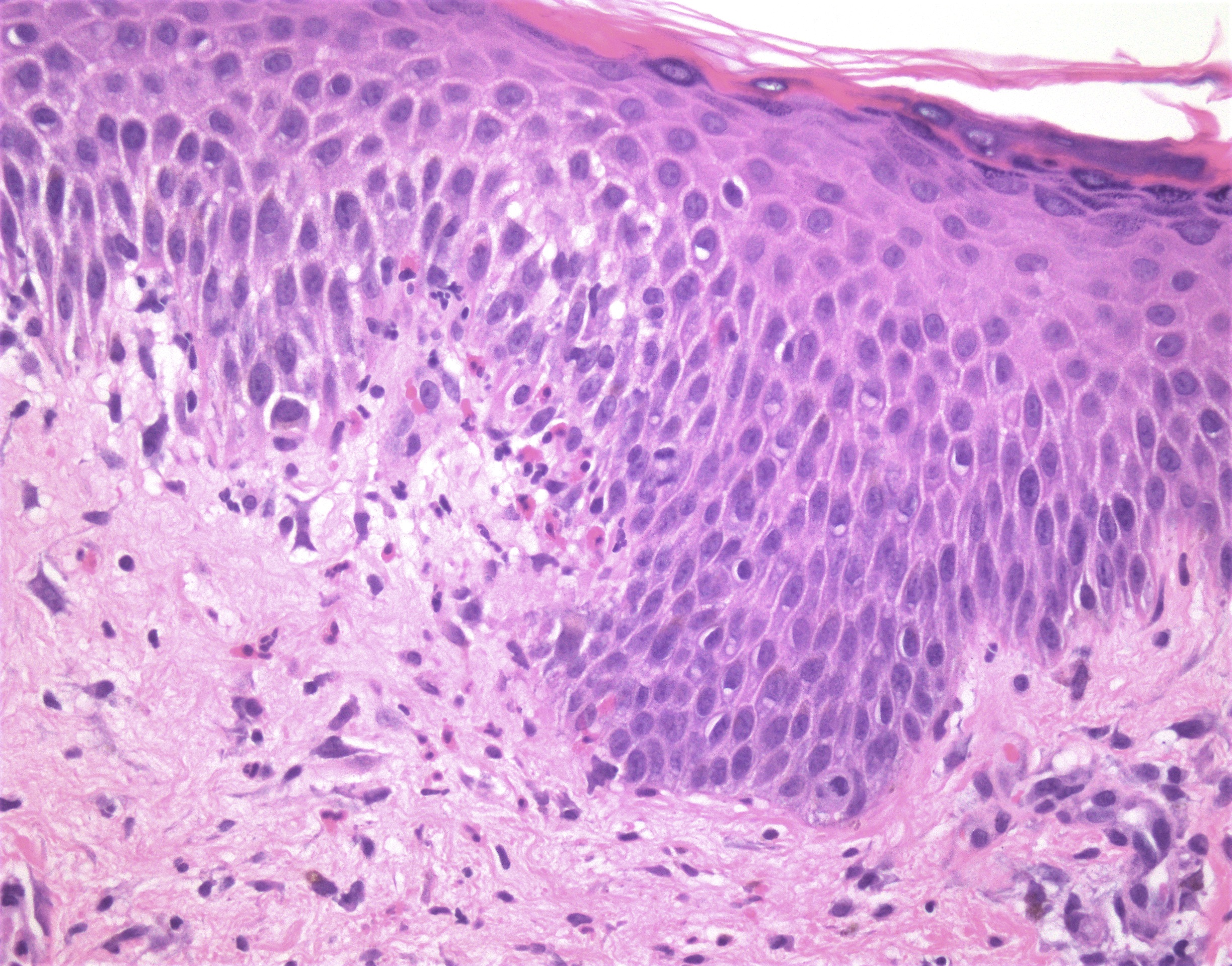
Eosinophilic spongiosis
Eosinophilic spongiosis with adjacent subepidermal blister
Virtual slides
Images hosted on other servers:

Eosinophil poor BP

Clinical images, virtual slide, direct immunofluorescence
Positive stains
- Collagen IV immunohistochemistry:
- Can be helpful in differentiating subepidermal blistering disorders with level of split below lamina densa (EBA, antilaminin gamma1/p200 pemphigoid, p105 pemphigoid) from BP and other disorders with split within lamina lucida or above lamina densa
- If split above lamina densa - dermal staining pattern
- If split below lamina densa - epidermal staining pattern
Immunofluorescence description
- Linear C3 > IgG and C3 deposition along the basement membrane zone of epithelium, hair follicles and eccrine glands, n-serrated pattern (Br J Dermatol 2013;169:100)
- Only C3 may be present in early stage lesions
- Salt split skin analysis:
- Direct immunofluoresence: localization of immunoreactants to either roof only (40%) or roof and blister (60%)
- Indirect immunofluorescence: localization of immunoreactants to the roof of the blister (95%)
Immunofluorescence images
Contributed by Randie H. Kim, M.D., Ph.D.
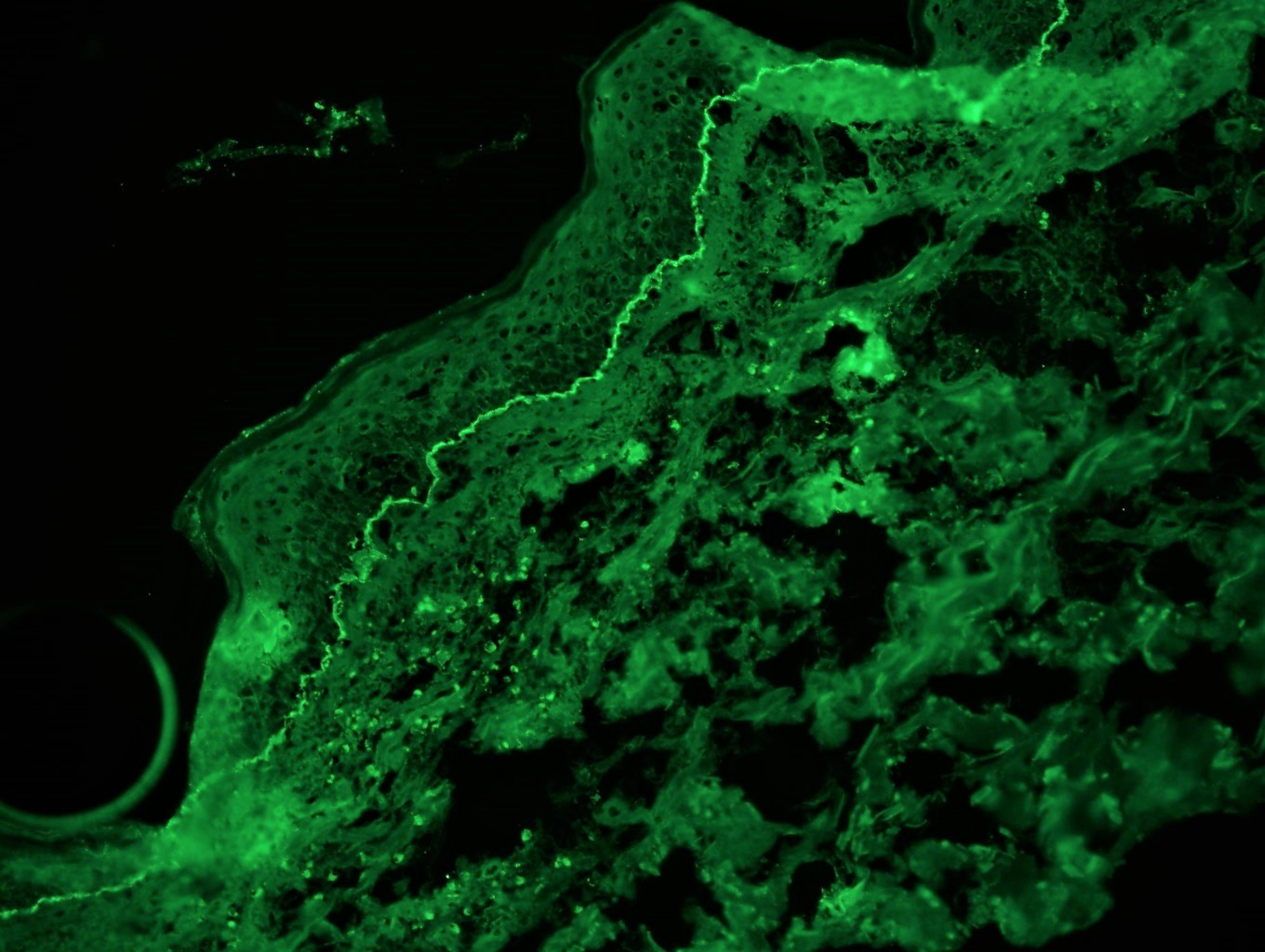
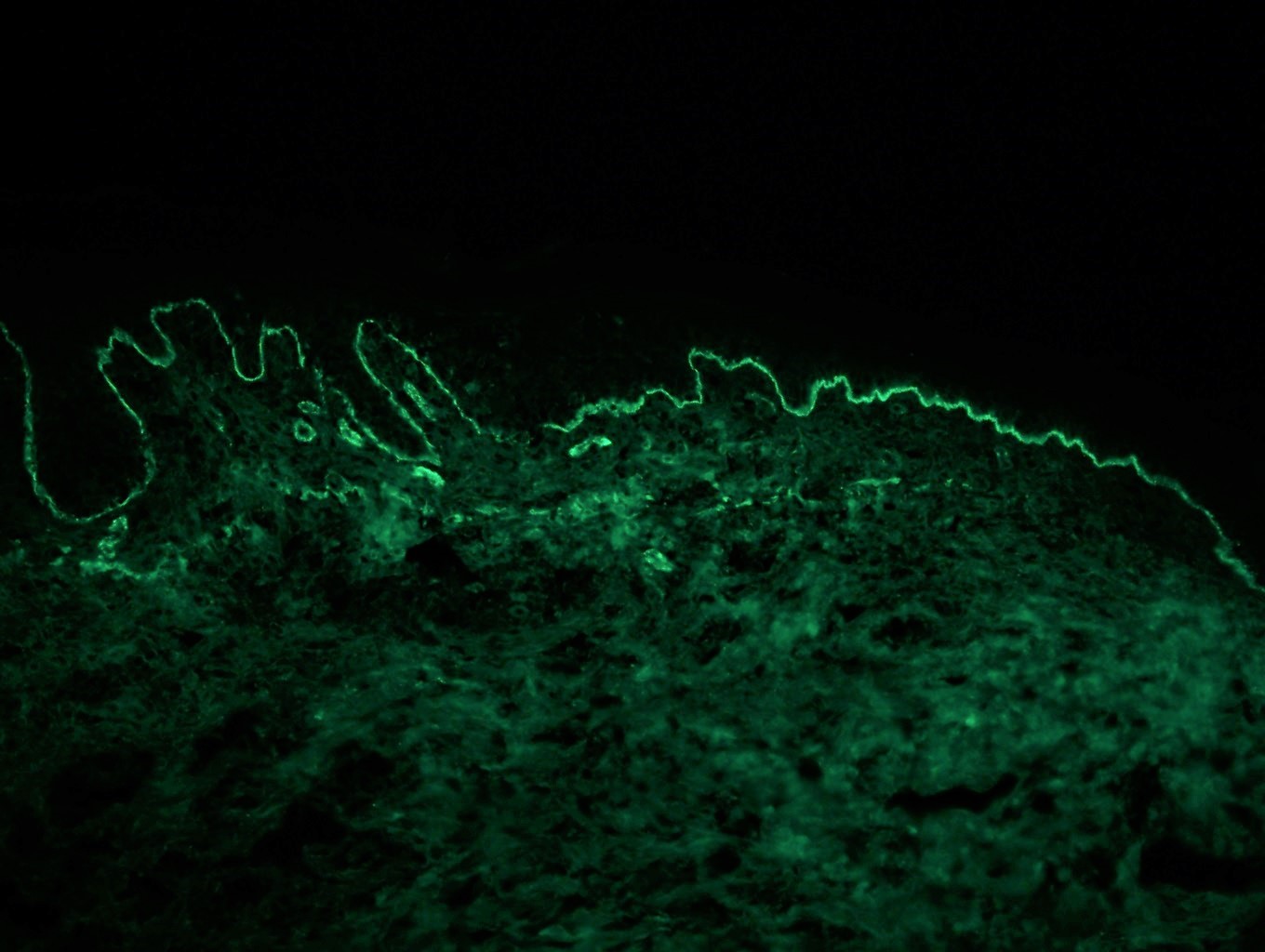
Linear C3 deposition along the basement membrane
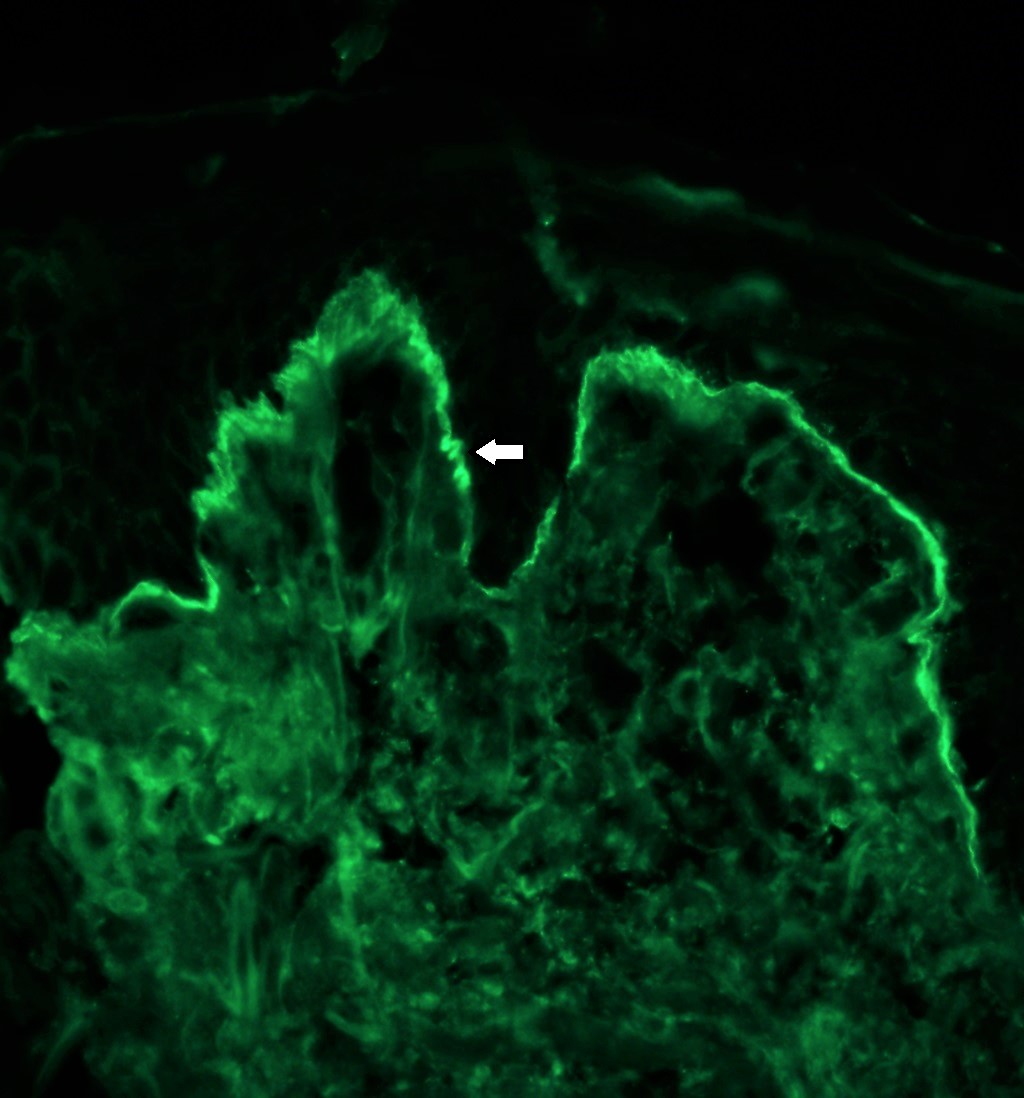
Positive IgG with n-serrated pattern (arrow)

Epidermal reactivity for IgG on roof of blister cavity (star)
Videos
Bullous pemphigoid
Dr. Phillip McKee
Bullous pemphigoid
Dr. Christine Ko
Sample pathology report
- Skin, left medial thigh, shave biopsy:
- Bullous pemphigoid (see comment)
- Comment: There is a subepidermal vesicle beneath which there is a mixed cell infiltrate including eosinophils. The associated specimen submitted for immunofluoresence studies shows linear C3 and IgG in an n-serrated pattern along the basement membrane.
- Skin, left abdomen, shave biopsy:
- Subepidermal blister with eosinophils (see comment)
- Comment: There is a subepidermal vesicle beneath which there is a mixed cell infiltrate including eosinophils. The periphery of the lesion shows areas of eosinophilic spongiosis. The differential diagnosis includes bullous pemphigoid, cicatricial pemphigoid, linear IgA disease, a bullous drug eruption and a severe arthropod bite reaction. Additional material for immunofluorescence studies is recommended.
Differential diagnosis
- Epidermolysis bullosa acquisita:
- Immunofluorescence positive on dermal side of salt split skin (u-serrated pattern) (Br J Dermatol 2004;151:112)
- IgG > C3
- Bullous lupus erythematosus:
- Neutrophil rich infiltrate, variable interface changes
- Dermal mucin deposition
- Eosinophils not present
- DIF: immunoreactive on dermal side of salt split skin (multiple reactants or IgG and C3), u-serrated pattern
- Positive lupus serology
- Positive epidermal nuclear Ig deposition(in vivo ANA) (J Rheumatol 1983;10:733)
- IgG1 is the predominant subclass found (J Dermatol Sci 1990;1:207)
- Dermatitis herpetiformis:
- Papillary neutrophilic microabscesses
- Immunofluorescence = granular IgA in dermal papillae
- May also have fibrillary IgA deposits in the dermal papillae or microgranular deposits along the dermo-epidermal junction (Postepy Dermatol Alergol 2019;36:655)
- Linear IgA bullous disease:
- Neutrophil rich infiltrate
- Immunofluorescence = linear IgA along the basement membrane zone
- Porphyria cutanea tarda:
- Pauci-inflammatory
- Festooning dermal papillae
- Hyalinized superficial blood vessels (positive PAS deposits)
- Caterpillar bodies (positive for PAS and collagen IV)
- Direct immunofluoresence: multiple immunoreactants at the dermo-epidermal junction and within superficial vessels (granular deposition)
Practice question #1
An 87 year old man presents with erythema and blistering of his chest and upper extremities. Examination shows tense bullae on an erythematous base. A skin biopsy is obtained which reveals subepidermal blister with a mixed inflammatory infiltrate with numerous eosinophils. Which of the following is true for the direct immunofluorescence findings regarding the diagnosis?
- Direct immunofluorescence would show granular IgA deposition at the tips of the dermal papillae
- Direct immunofluorescence would show IgG and C3 reactivity in the epidermis in a fishnet-like pattern in the intercellular squamous region
- Direct immunofluorescence would show linear IgA reactivity along the basement membrane
- Direct immunofluorescence would show linear IgG and C3 reactivity at the basement membrane
Practice answer #1
D. Direct immunofluorescence would show linear IgG and C3 reactivity at the basement membrane
Comment Here
Reference: Bullous pemphigoid
Comment Here
Reference: Bullous pemphigoid
Practice question #2
What is / are the antigen(s) targeted in bullous pemphigoid?
- BPAG1 and BPAG2
- Collagen VII
- Desmoglein 1 and Desmoglein 3
- Envoplakin and periplakin
Practice answer #2
