Skin nontumor
Dermal granulomatous and necrobiotic reaction patterns
Lupus miliaris disseminatus faciei (acne agminata)
Board of reviewers: Carina Dehner, M.D., Ph.D.


Last author update: 4 December 2024
Last staff update: 4 December 2024
Copyright: 2024, PathologyOutlines.com, Inc.
PubMed Search: Lupus miliaris disseminatus faciei / acne agminata
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Christie-Nguyen PT, Phung TL. Lupus miliaris disseminatus faciei (acne agminata). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorlupusmiliarisdiss.html. Accessed September 29th, 2025.
Definition / general
- Uncommon idiopathic inflammatory skin condition characterized by asymptomatic, monomorphic smooth papules on the central face, particularly affecting the eyelids, especially the lower eyelid
Essential features
- Histologic hallmarks of lupus miliaris disseminatus faciei (LMDF) include
- Perivascular and periadnexal lymphohistiocytic infiltrates in the early stages
- Perifollicular epithelioid cell granulomas with or without caseation in mature lesions
- Often associated with distorted, ruptured or hyperplastic hair follicles
- Etiology is unknown; however, it has been proven to not be associated with tuberculosis (TB) or other infections
- Although LMDF can resolve spontaneously over 12 - 24 months, untreated lesions may result in significant scarring
Terminology
- Acne agminata is a preferred term for similar lesions in the axilla (J Dtsch Dermatol Ges 2006;4:858)
- Facial idiopathic granulomas with regressive evolution (FIGURE) was suggested but has not been widely accepted (Dermatology 2000;201:287)
ICD coding
- ICD-10: L71.8 - other rosacea
Epidemiology
- Uncommon with unknown incidence (StatPearls: Lupus Miliaris Disseminatus Faciei [Accessed 11 November 2024])
- Adults (mean age of 38.2), M = F (J Dermatol 2011;38:864, Front Med (Lausanne) 2024;11:1382526)
- Cases in children are also reported (J Cosmet Dermatol 2022;21:6484)
Sites
- Central face, typically on and around the eyelids (An Bras Dermatol 2017;92:851)
Pathophysiology
- In LMDF, ruptured follicular infundibular cysts are commonly observed
- These ruptures may release follicular contents, such as keratin and sebum
- These foreign materials are key drivers of an allergic granulomatous reaction, leading to granuloma formation in LMDF (J Dermatol 2011;38:864)
Etiology
- Precise etiology is not known
- Early reports suggested an association with TB due to its histologic morphology of epithelioid cell granulomas with caseating necrosis but there is evidence disproving this link (Br J Dermatol 1997;137:614)
- Demodex species were once considered a possible factor but the evidence does not support this (J Dermatol 2011;38:864)
- A proposed hypothesis is that an immune reaction targeting the pilosebaceous units plays a significant role in the development of granulomas in LMDF (J Dermatol 2011;38:864)
- Recent detection of Propionibacterium acnes in granulomatous lesions of LMDF suggests a potential role in its pathogenesis (J Dermatol 2015;42:418)
Clinical features
- Monomorphous, yellow-brown to red, dome shaped papules typically appear on the central face, often in periocular areas; these papules may extend to the neck and chin and in rare cases, can also be found on extrafacial sites, such as the arms and axillae (Dermatology 2003;206:120)
- Typically asymptomatic, though some patients have reported mild itchiness (Front Med (Lausanne) 2024;11:1382526)
Diagnosis
- Diagnosis is usually based on histologic morphology, which shows epithelioid cell granulomas with caseating necrosis, accompanied by distorted, ruptured or hyperplastic hair follicles
- No evidence of TB or fungal infections
Laboratory
- Serum levels of calcium and angiotensin converting enzyme within normal limits, ruling out sarcoidosis (An Bras Dermatol 2017;92:851)
Prognostic factors
- Frequently regress on their own over 12 - 24 months without treatment but they often result in significant scarring (An Bras Dermatol 2017;92:851)
- Early treatment shows reduced scarring (J Dermatol 2011;38:864)
Case reports
- 6 year old Japanese girl with a 5 month history of pruritic papular eruptions on the face and scattered reddish papules on the labia majora (An Bras Dermatol 2024;99:618)
- 60 year old Korean woman with multiple erythematous and yellowish papules across her face (JAAD Case Rep 2022;27:16)
- 62 year old man with asymptomatic papules on his face (Case Rep Dermatol 2021;13:321)
- 70 year old woman with a history of Demodex blepharitis presented with a 1 year history of red-yellow nodules in the tarsal region of her eyelids (Ophthalmic Plast Reconstr Surg 2020;36:e90)
- 70 year old woman with a long history of systemic lupus erythematosus (SLE) and Stevens-Johnson syndrome (SJS) presented with skin lesions extending from the neck to the lower chin (J Dermatol 2021;48:110)
Treatment
- Tetracycline was initially recommended but many treatment failures have been reported (Clin Exp Dermatol 2003;28:677)
- Response to oral isotretinoin and topical steroids is variable (J Dermatol 2011;38:864)
- Systemic dapsone and topical tacrolimus have shown effectiveness (Sisli Etfal Hastan Tip Bul 2018;52:142)
- Topical JAK inhibition (ruxolitinib) may be particularly effective in treating certain cases of LMDF (JAMA Dermatol 2023;159:790)
- Recalcitrant LMDF has shown a response to cyclosporin monotherapy (JAAD Case Rep 2022;27:16)
Clinical images
Contributed by Yu-Hung Wu, M.D.

Erythematous, dome shaped papules
Microscopic (histologic) description
- Characteristics vary depending on the stage of development
- In the early stages, there are nonspecific changes, such as perivascular and periadnexal lymphohistiocytic infiltrates and scattered neutrophils in the superficial dermis without granuloma formation
- As lesions mature, they may present various patterns, including perifollicular epithelioid cell granulomas with or without central necrosis (central necrosis being a diagnostic feature of LMDF) or granulomas with abscesses often related to ruptured hair follicles
- Commonly associated with distorted, ruptured or hyperplastic hair follicles
- Lymphoid tissue accumulation may be observed surrounding the giant cells contained in the granulomas (J Dtsch Dermatol Ges 2006;4:858)
Microscopic (histologic) images
Contributed by Yu-Hung Wu, M.D.

Shave biopsy



Caseating granulomatous inflammation
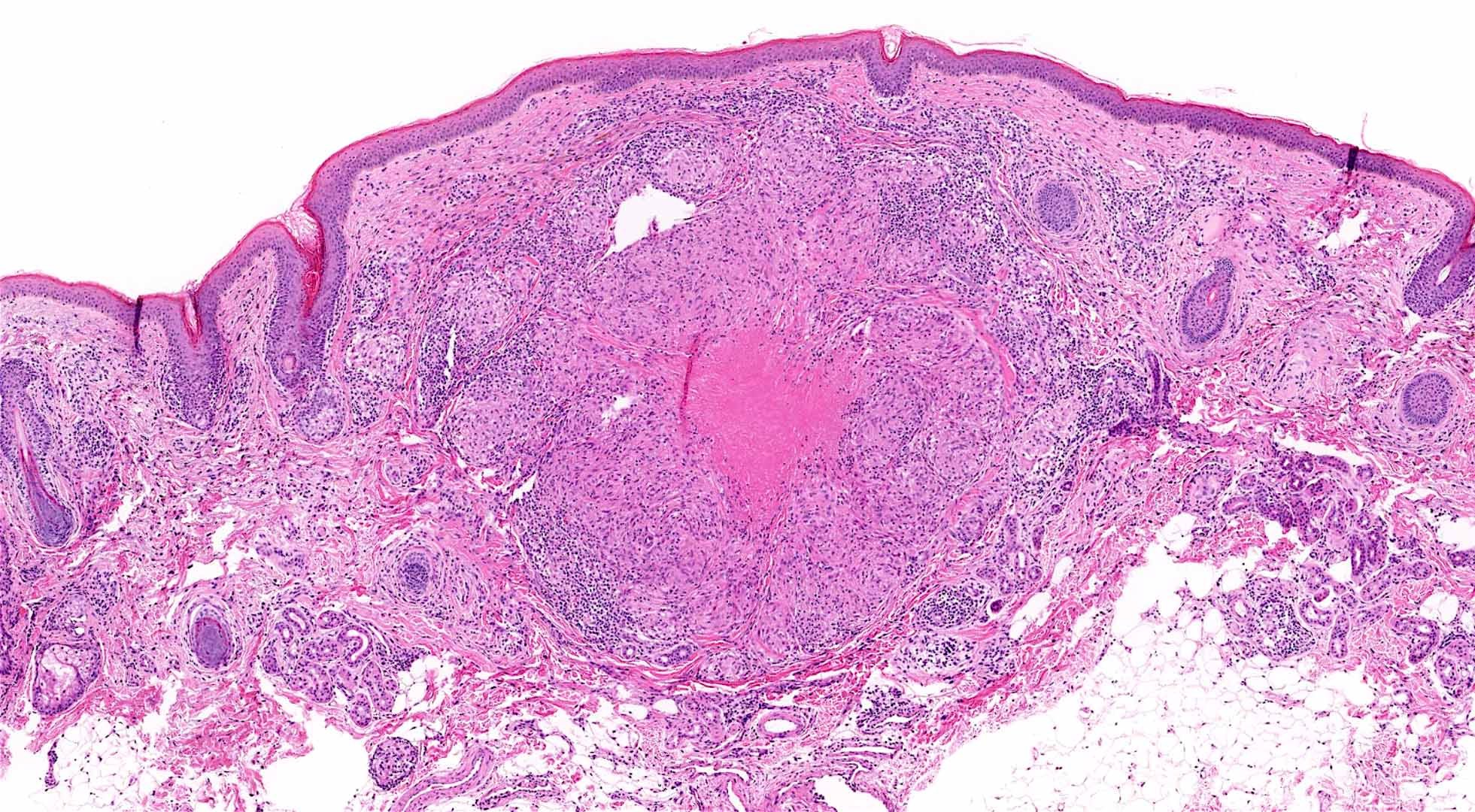

Caseating granulomatous inflammation
Positive stains
- Uncommon, typically diagnosed by H&E stain
Negative stains
Sample pathology report
- Skin, upper eyelid, punch biopsy:
- Lupus miliaris disseminatus faciei (see comment)
- Comment: Epithelioid cell granuloma with caseating necrosis and ruptured hair follicles, consistent with lupus miliaris disseminatus faciei in the appropriate clinical setting.
Differential diagnosis
- Granulomatous rosacea:
- Unlike LMDF, these granulomas are typically associated with Demodex folliculorum and do not show features of caseating necrosis
- Lymphoid infiltrate and capillary dilation are more prominent; symptoms can include flushing, which may worsen with alcohol, spicy food or sun exposure (Case Rep Dermatol 2021;13:321)
- Might respond to tetracycline and typically does not leave scars (Case Rep Dermatol 2021;13:321)
- Sarcoidosis:
- LMDF with noncaseating granulomas can look similar to sarcoidosis
- Some distinct features of sarcoidosis include annular, flesh colored deep nodules that may present as solitary lesions and involve only 1 side of the face (Int J Dermatol 2005;44:606)
- Can be ruled out by clinical assessment and laboratory tests, including chest Xray and measurement of angiotensin converting enzyme levels
- Nontuberculous / tuberculous mycobacterial infections:
- Deep fungal infections:
- Can be ruled out by PAS stain
Practice question #1
Where are lesions of lupus miliaris disseminatus faciei usually found?
- Central face
- Scalp
- Trunk
- Upper extremities
Practice answer #1
A. Central face. Lupus miliaris disseminatus faciei typically presents as monomorphic, smooth papules on the central face, with a predilection for the eyelids. Answers B, C and D are incorrect because it is rarely observed on the scalp, trunk or extremities.
Comment Here
Reference: Lupus miliaris disseminatus faciei (acne agminata)
Comment Here
Reference: Lupus miliaris disseminatus faciei (acne agminata)
Practice question #2
Which of the following is the best description for the histologic appearance of lupus miliaris disseminatus faciei?
- Epithelioid cell granulomas with caseating necrosis and ruptured hair follicles
- Marked papillary dermal edema with superficial and deep perivascular lymphocytic infiltrate
- Prominent keratinocyte necrosis in the basal layer of the epidermis and follicular epithelium
- Superficial and deep perivascular and periadnexal lymphocytic infiltrate with plasma cells
Practice answer #2
A. Epithelioid cell granulomas with caseating necrosis and ruptured hair follicles are characteristic histological features of lupus miliaris disseminatus faciei. Answer C is incorrect because prominent keratinocyte necrosis in the basal layer of the epidermis and follicular epithelium describes interface dermatitis, which can result from various conditions, such as drug reactions, lupus erythematosus or graft versus host disease. Answer D is incorrect because superficial and deep perivascular and periadnexal lymphocytic infiltrate with plasma cells are histologic hallmarks of cutaneous lupus erythematosus. Answer B is incorrect because marked papillary dermal edema with superficial and deep perivascular lymphocytic infiltrate is typically seen in polymorphous light eruption.
Comment Here
Reference: Lupus miliaris disseminatus faciei (acne agminata)
Comment Here
Reference: Lupus miliaris disseminatus faciei (acne agminata)
