Skin nontumor
Neutrophilic and eosinophilic dermatoses
Eosinophilic cellulitis (Wells syndrome)
Last author update: 1 July 2017
Last staff update: 25 August 2025 (update in progress)
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Wells Syndrome [title]


Table of Contents
Definition / general | Essential features | Epidemiology | Etiology | Clinical features | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Differential diagnosis | Practice question #1 | Practice answer #1Cite this page: Dubyk F, Elwood HR. Eosinophilic cellulitis (Wells syndrome). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorwellssyndrome.html. Accessed September 22nd, 2025.
Definition / general
- Idiopathic inflammatory dermatitis with eosinophilic infiltration
- Also known as eosinophilic cellulitis
Essential features
- Idiopathic condition typically characterized by recurrent pruritic to painful plaques that often clinically resemble cellulitis
- Histopathology characterized by a prominent eosinophilic infiltrate with "flame figures"
Epidemiology
- Equal prevalence in men and women
- Most cases sporadic
- Higher prevalence in adults than children
Etiology
- Unknown
- Some cases may be secondary to hypersensitivity reaction to insect bites, medications, infections, vaccinations, malignant tumors or myeloproliferative disorders (J Clin Aesthet Dermatol 2011;4:55)
Clinical features
- Clinical picture is variable but most often recurrent bouts of edematous nodules and plaques, often preceded by prodromal itching or pain
- Usually a limited course over weeks to month but often recur
- May resemble cellulitis clinically but not warm or tender (Postepy Dermatol Alergol 2014;31:322) and does not improve with antibiotics (J Clin Aesthet Dermatol 2011;4:55)
- Erythematous papules, plaques or nodules that may be painful or pruritic (Postepy Dermatol Alergol 2014;31:322)
- Sometimes annular configuration, can blister
- May be single or multiple
- Peripheral blood eosinophilia common (found in 67% of cases) (Can J Plast Surg 2012;20:91)
- Leukocytosis (found in 41% of cases)
Treatment
- Oral or topical corticosteroids most commonly, often with dramatic improvement
- Antihistamines and immunomodulatory agents also used for refractory or unresponsive cases
Clinical images
Images hosted on other servers:

Swollen plaques on right forearm

Diffuse erythematous plaque

Resembling bacterial cellulitis
Microscopic (histologic) description
- Diffuse dermal infiltrate of perivascular and interstitial eosinophils throughout superficial and deep dermis, often with extension into subcutis
- Admixed histiocytes and lymphocytes
- Old lesions may show granulomas
- Flame figures often present (deposition of eosinophil basic protein on collagen bundles)
- Can have subepidermal edema, sometimes with blister formation
- May have eosinophilic spongiosis
- No vasculitis
Microscopic (histologic) images
Contributed by Favia Dubyk, M.S., M.D.
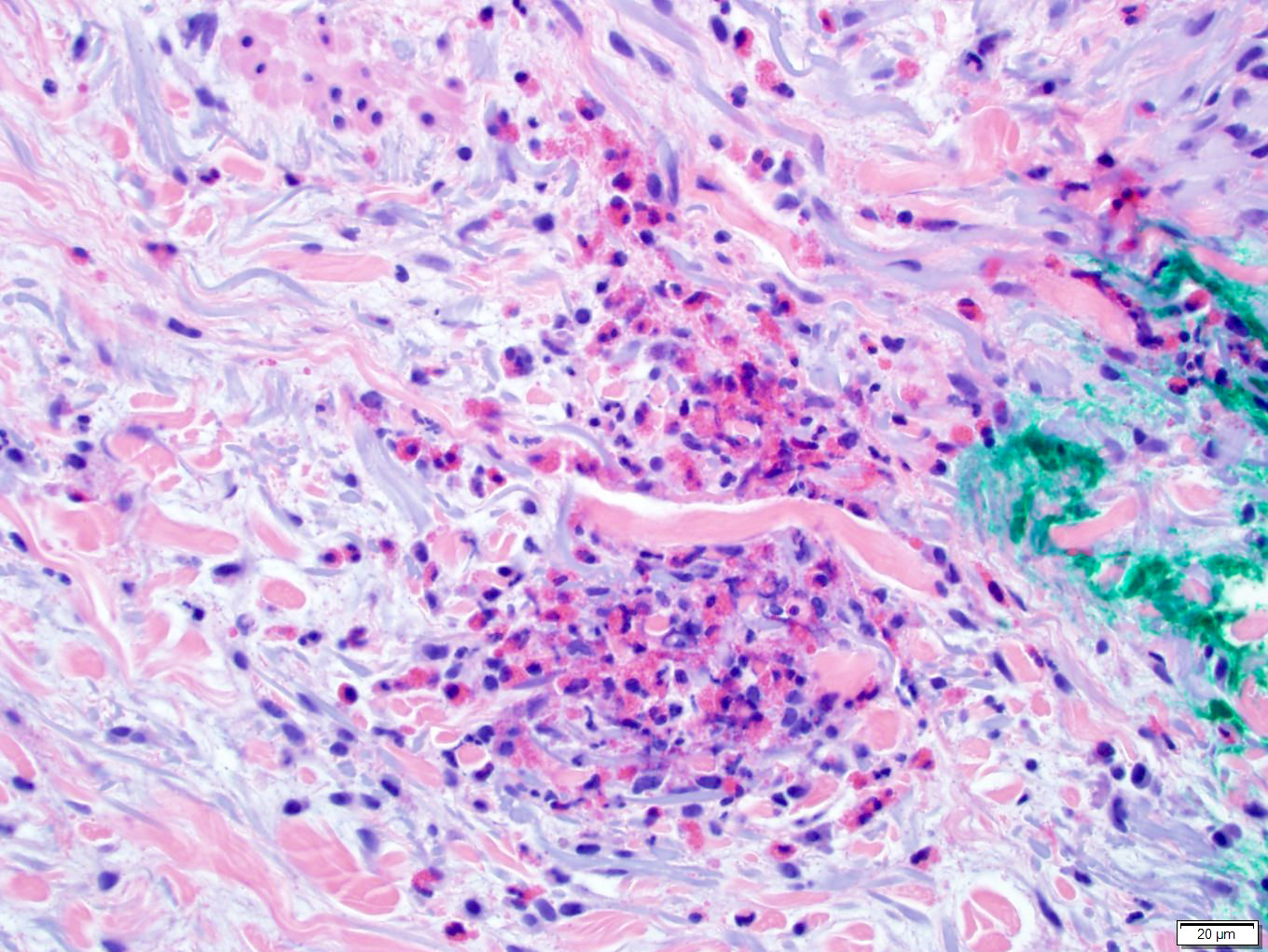
Nodular collections of eosinophils
Images hosted on other servers:

Diffuse dermal eosinophilic infiltrate

High power view of eosinophils and flame figures

Multiple flame figures

Interstitial infiltrate
with eosinophils
magnification 100x

Numerous eosinophils magnification 200x
Differential diagnosis
- Bacterial cellulitis: dermal to subcutaneous infiltrate of neutrophils, often with superficial dermal edema; typically lacks flame figures and neutrophils predominate over eosinophils
- Churg-Strauss syndrome: may have similar eosinophilic granulomas, vasculitis not always present in skin biopsy, clinical correlation helpful
Practice question #1
Which of the following statements is true of Wells syndrome?
- Flame figures are pathognomonic
- Granulomatous inflammation always absent
- Lesions can clinically resemble cellulitis
- Peripheral blood eosinophilia is required for diagnosis
- Vasculitis usually present
Practice answer #1
C. Often clinically resembles cellulitis, hence it's other name eosinophilic cellulitis. Answer A is incorrect because while flame figures are a hallmark of the disease, these can sometimes be seen in a number of other settings such parasite infestation, arthropod bite, drug reaction, allergic contact dermatitis and bullous pemphigoid. Answer B is incorrect because older lesions can have a granulomatous component, sometimes with prominent giant cells. Answer D is incorrect because this is seen in up to 67% of patients but not required for diagnosis. Answer E is inocrrect because vasculitis is typically absent although there may be extravasated erythrocytes.
Comment Here
Reference: Wells syndrome
Comment Here
Reference: Wells syndrome
