

Kidney tumor
Adult renal cell carcinoma - rare
Succinate dehydrogenase deficient
Last author update: 1 May 2016
Last staff update: 29 February 2024 (update in progress)
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: SDH [title] kidney


Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Pathophysiology | Diagrams / tables | Clinical features | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | IHC panels | Molecular / cytogenetics description | Differential diagnosis | Additional referencesCite this page: Andeen NK, Tretiakova M. Succinate dehydrogenase deficient. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumorSDH.html. Accessed April 26th, 2024.
Definition / general
- Succinate dehydrogenase (SDH) deficient renal cell carcinoma is defined by the WHO as a malignant epithelial tumor composed of vacuolated eosinophilic to clear cells with loss of immunohistochemical expression of SDHB, a marker of dysfunction of mitochondrial complex II (WHO 2016)
Essential features
- Characteristic flocculent cytoplasmic vacuoles with a pale eosinophilic, wispy or bubbly appearance and low grade nuclei (at least focally)
- May have high grade areas
- Oncogenesis is driven by metabolic derangements due to double hit inactivation of SDH genes, leading to dysfunction of mitochondrial complex II
- Most patients have a germline mutation in an SDH gene, usually SDHB
Terminology
- Terminology which is sometimes used but not recommended is SDHB negative renal carcinoma or SDH deficient renal oncocytoma
Epidemiology
- Rare
- Represents 0.05% to 0.2% of all renal cell carcinomas (WHO 2016)
- Median age 35 years (range 14 to 76); M:F ratio = 1:8:1
- Bilateral in 26% (Am J Surg Pathol 2014;38:1588)
Sites
- Kidney
Pathophysiology
- Most cases occur in setting of germline mutation of an SDH gene; neoplasia occurs with double hit inactivation, leading to dysfunction of mitochondrial complex II, increased reactive oxygen species, DNA damage and HIF1α stabilization (Int Journal of Cell Biology 2012:2012)
- SDHB is most commonly affected in SDH deficient RCC, then SDHC
- Rarely SDHA or SDHD (different for other SDH deficient tumors)
Diagrams / tables
Images hosted on other servers:

Redox alterations
Clinical features
- Often confined to the kidney at presentation
- Presents with flank pain or as incidental finding
- Personal or family history of paragangliomas or SDH deficient gastrointestinal stromal tumor may be present (WHO 2016) (GeneReviews 2008;NBK1548)
Prognostic factors
- Overall metastasis rate of ~ 33% (based on 27 cases) but metastasis uncommon if only low grade features (Am J Surg Pathol 2014;38:1588)
- Higher metastasis rate if high grade nuclei (70% metastasize) or coagulative necrosis present (4/4 cases metastasized, Am J Surg Pathol 2014;38:1588)
Case reports
- Loss of SDHB by immunohistochemistry in 3 patients with known SDHB mutations (N Engl J Med 2011;364:885)
- With SDHA mutation (Hum Pathol 2015;46:1951)
Treatment
- Resection; further treatment is dependent on grade / stage, may include targeted therapy (J Clin Oncol 2014;32;e10)
- All patients with a diagnosis of SDH deficient RCC should be offered genetic testing (WHO 2016)
Gross description
- Well circumscribed, solid with red / brown cut surface, variable multicystic change, generally no necrosis
- Usually confined to kidney with no involvement of renal sinus, vein or fat
Gross images
Images hosted on other servers:

Cystic change;
solid neoplasms
Microscopic (histologic) description
- Well circumscribed or pushing border, commonly entraps tubules
- Solid, nested or tubular growth pattern with scattered cysts containing eosinophilic material
- Neoplastic cells have smooth nuclear contours and fine chromatin with no nucleoli
- Characteristic finding is flocculent cytoplasmic vacuoles with a pale eosinophilic, wispy or bubbly appearance with low grade nuclei
- This morphology is commonly diffuse and should be at least focal (WHO 2016)
- May have areas of higher grade nuclei, necrosis, sarcomatoid change
- Variant morphologies have been reported but are rare in absence of more characteristic low grade regions (WHO 2016)
Microscopic (histologic) images
Images hosted on other servers:






Various images


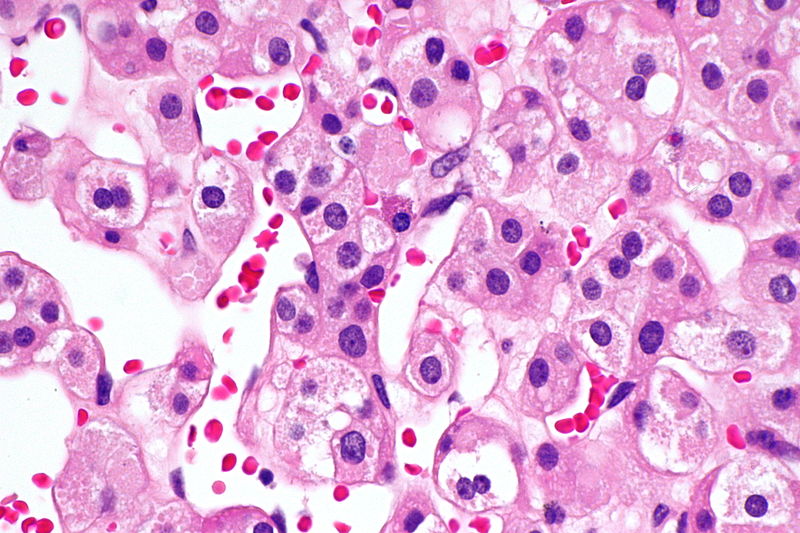
SDH deficient RCC
Positive stains
Negative stains
- Loss of SDHB immunohistochemical staining (be cautious on overinterpretation of negativity in tumors with very clear cytoplasm)
- Loss of SDHB immunohistochemical staining indicates disruption of the mitochondrial complex 2 for any reason, not just SDHB gene mutation (Am J Surg Pathol 2014;38:1588)
- CK7, CAIX, RCC, c-kit (mast cells only), vimentin (Mod Pathol 2015;28:80), neuroendocrine markers
- Minimal AMACR staining
IHC panels
| Hale | KIT | CK7 | S100A1 | VIM | CAIX | AMACR | SDH | TFE3 | |
| Chromophobe RCC | +++ | +++ | +++ | - | - | - | - | +++ | - |
| Clear cell RCC | - | - | - | - | +++ | +++ | - | +++ | - |
| Oncocytoma | - | +++ | rare | +++ | - | - | - | +++ | - |
| Papillary RCC | - | - | +++ | - | +++ | - | +++ | +++ | - |
| Translocation RCC | - | - | - | - | - | - | ++ | +++ | +++ |
| SDH deficient RCC | - | - | - | - | - | - | - | - | - |
References: Pathol Res Pract 2015;211:303, Ann Diagn Pathol 2020;44:151448, Am J Surg Pathol 2014;38:e6, Arch Pathol Lab Med 2019;143:1455, Transl Androl Urol 2019;8:S123, Hum Pathol 2020 Jul 13 [Epub ahead of print]
Molecular / cytogenetics description
- No mutations in VHL, PIK3CA, AKT, mTOR, MET or TP53 genes (WHO 2016)
- Genes for succinate dehydrogenase subunits (SDHA, SDHB, SDHC, SDHD) encode proteins which are part of mitochondrial complex II, which links the Krebs cycle and electron transport chain (N Engl J Med 2011;364:885)
Differential diagnosis
- Eosinophilic variant of chromophobe RCC:
- Prominent cell borders and crinkled / raisinoid nuclei with binucleation
- Also CK7+ with no loss of SDHB expression
- Eosinophilic variant of clear cell RCC: CAIX+, vimentin+
- Oncocytoma: often has myxohyaline stroma; CKIT+ with no loss of SDHB expression (Mod Pathol 2015;28:80)
- Papillary renal cell carcinoma (type 2):
- Cytoplasm is eosinophilic but not as pale wispy/bubbly
- Nuclei often pseudostratified
- Loss of SDHB immunohistochemical expression is rare in other carcinomas (Appl Immunohistochem Mol Morphol 2014;22:31)
Additional references
