

Mediastinum
Thymic carcinoma
Thymic squamous cell carcinoma
Author: Hanni Gulwani, M.B.B.S.

Last author update: 1 December 2012
Last staff update: 19 February 2024 (update in progress)
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Thymic carcinoma general

Table of Contents
Definition / general | Epidemiology | Diagrams / tables | Clinical features | Radiology images | Prognostic factors | Case reports | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy description | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Gulwani H. Thymic squamous cell carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mediastinumthymiccarcinoma.html. Accessed May 13th, 2024.
Definition / general
- By definition, has overt cellular anaplasia
Epidemiology
- Ages ≥ 50 years; occasionally children
Diagrams / tables
Images hosted on other servers:

Proposed stage T1, tumor limited to thymic gland

Proposed stage T2, tumor invades nearby structures

Proposed stage T3, direct (continuous) extrathoracic tumor extension beyond thoracic inlet or below diaphragm
Clinical features
- Associated with hypercalcemia, elevated parathyroid hormone levels, pulmonary sarcoidosis
- Not associated with paraneoplastic syndromes such as myasthenia gravis or pure red cell aplasia
- Patients usually present with mass related symptoms
- Aggressive clinical course
- Must exclude other primaries, which are much more common (lung, trachea, bronchi, esophagus)
- Usually squamous cell carcinoma and variants (lymphoepithelioma-like, basaloid)
- Proposed staging system (Am J Clin Pathol 2012;138:115)
Radiology images

Prognostic factors
- May be less aggressive than commonly believed; important prognostic factors are lymph node status and tumor size (Am J Clin Pathol 2012;138:103)
- Keratinizing: good prognosis with few fatalities if well differentiated
Case reports
- 42 year old man with multiple lung, bone and brain metastases (Acta Neurol Taiwan 2010;19:41)
- 47 year old Asian woman with malaise, weight loss, chest pain and shortness of breath (Case of the Month #479)
- 52 year old man with complaints of left anterior chest pain (Kyobu Geka 2003;56:509)
Gross description
- Unencapsulated, no internal fibrous septation, firm / hard / gritty with gray-white cut surface, necrosis and hemorrhage
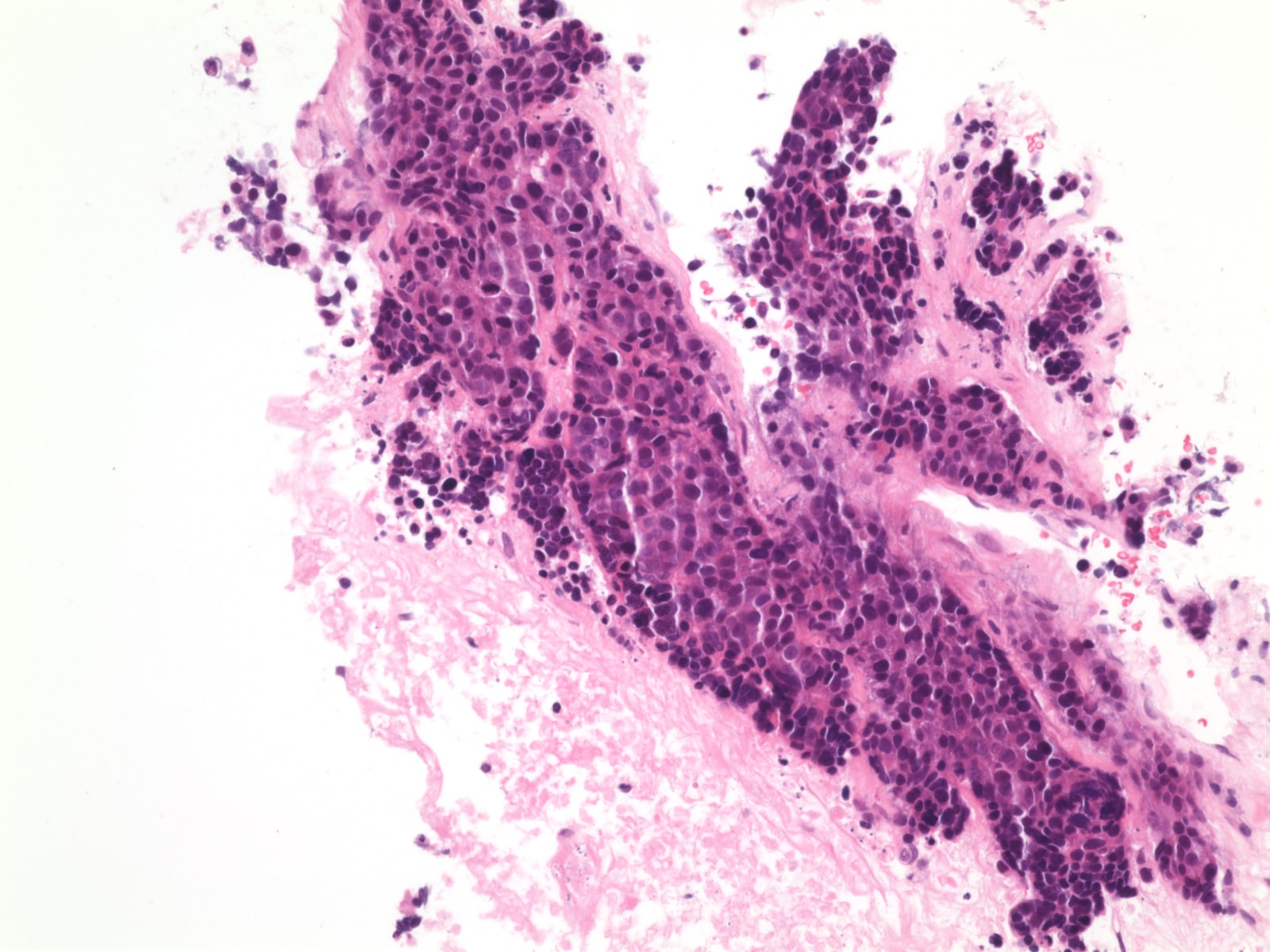
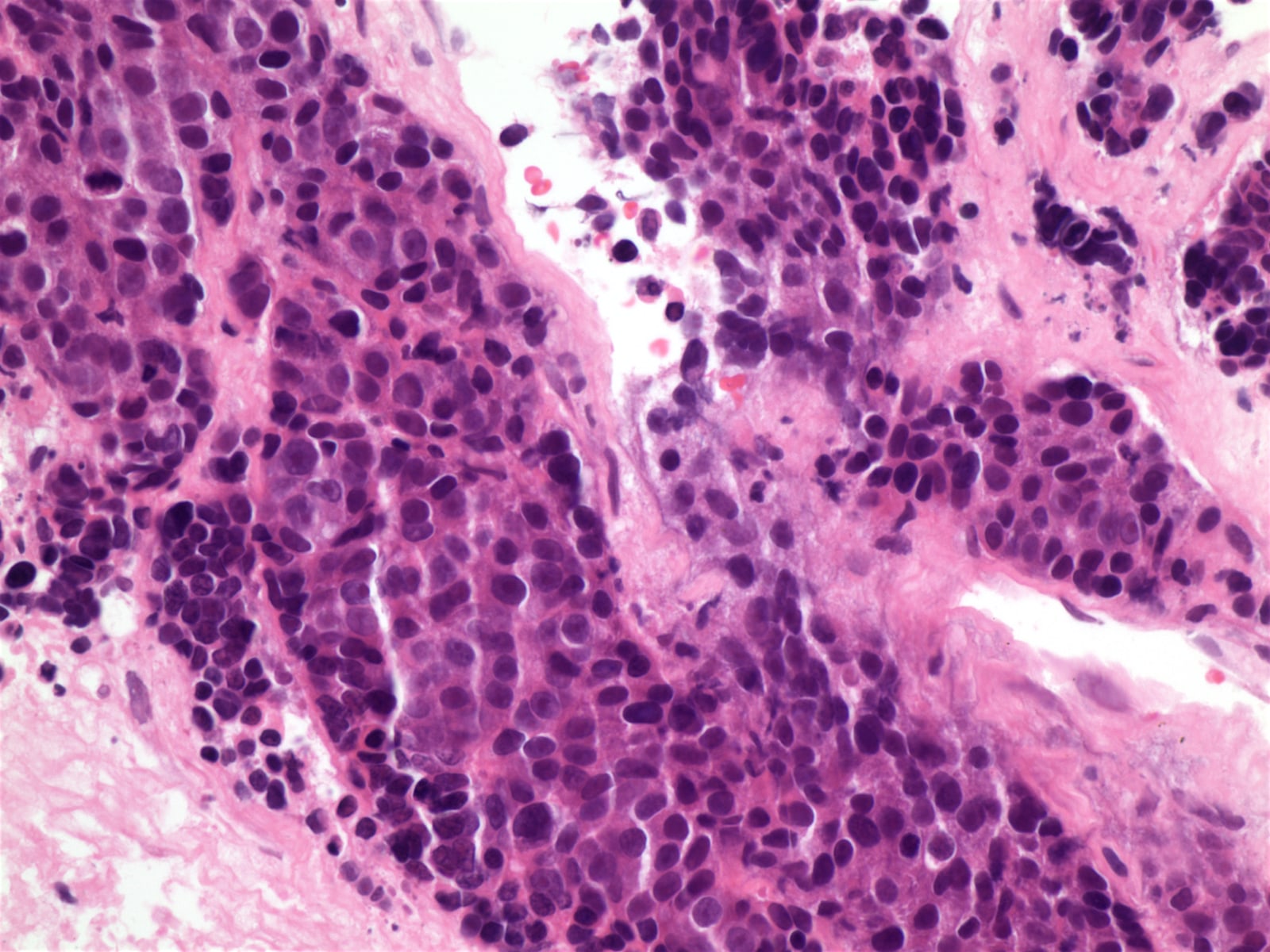
Microscopic (histologic) description
- Usually cohesive cellular growth, regularly round / oval nuclear outlines, eosinophilic nucleoli, geographic necrosis
- Usually foci of medullary differentiation, abortive Hassall corpuscles, rosettes, gland-like spaces, T lymphocytes; no perivascular spaces
- Keratinizing:
- Similar to tumor in skin, lung, other sites
- Lobular growth with fibrous bands
- Nests and cords of large polyhedral cells with intercellular bridges
- Vesicular or hyperchromatic nuclei, prominent nucleoli, eosinophilic or glassy cytoplasm, keratin pearls
- Also angiolymphatic invasion, necrosis
- Rarely coexists with thymoma
- Non-keratinizing
- Angular nests of malignant squamous cells in desmoplastic stroma
- No intercellular bridges, no eosinophilic cytoplasm, no keratin pearls
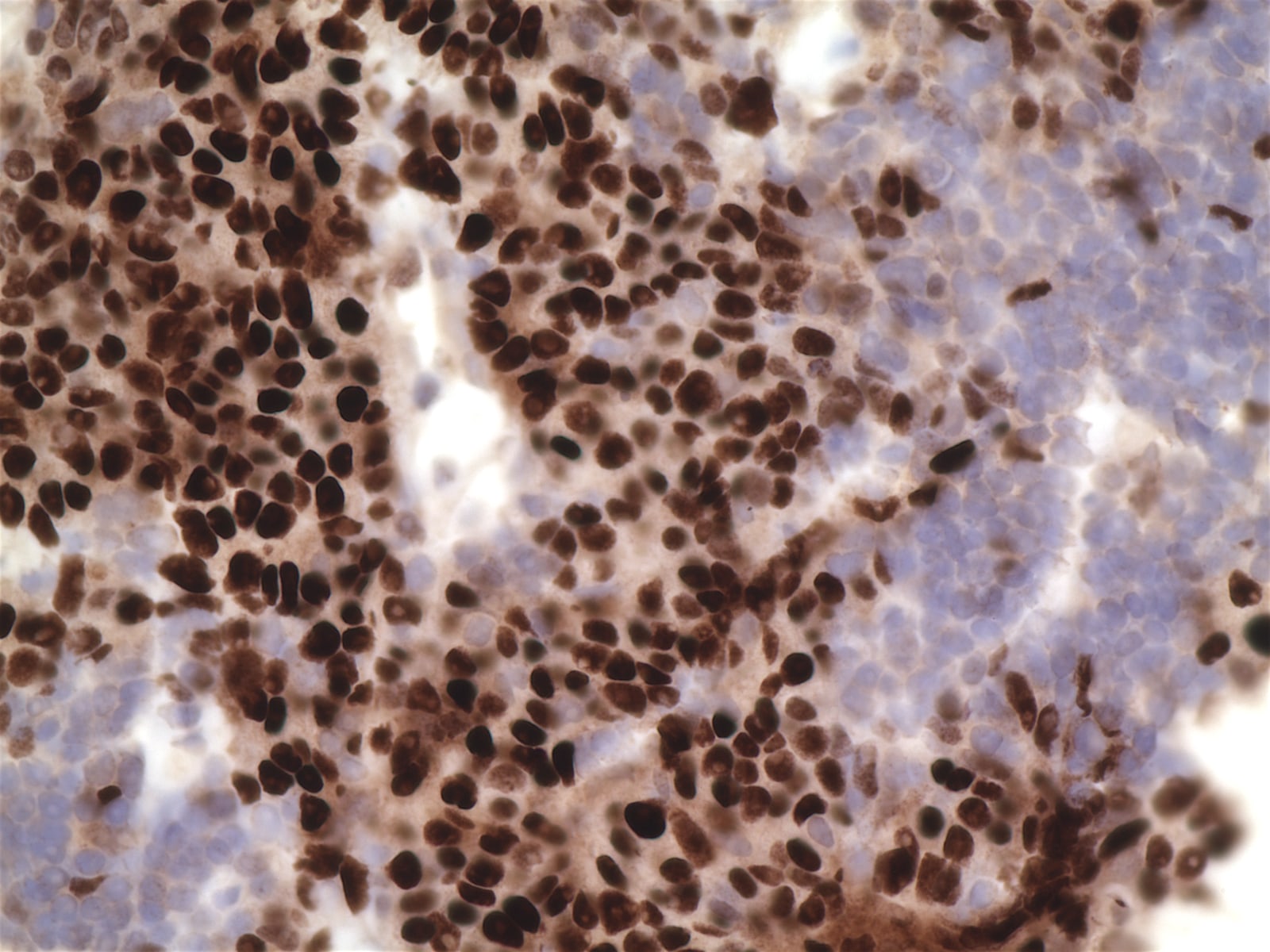
Microscopic (histologic) images
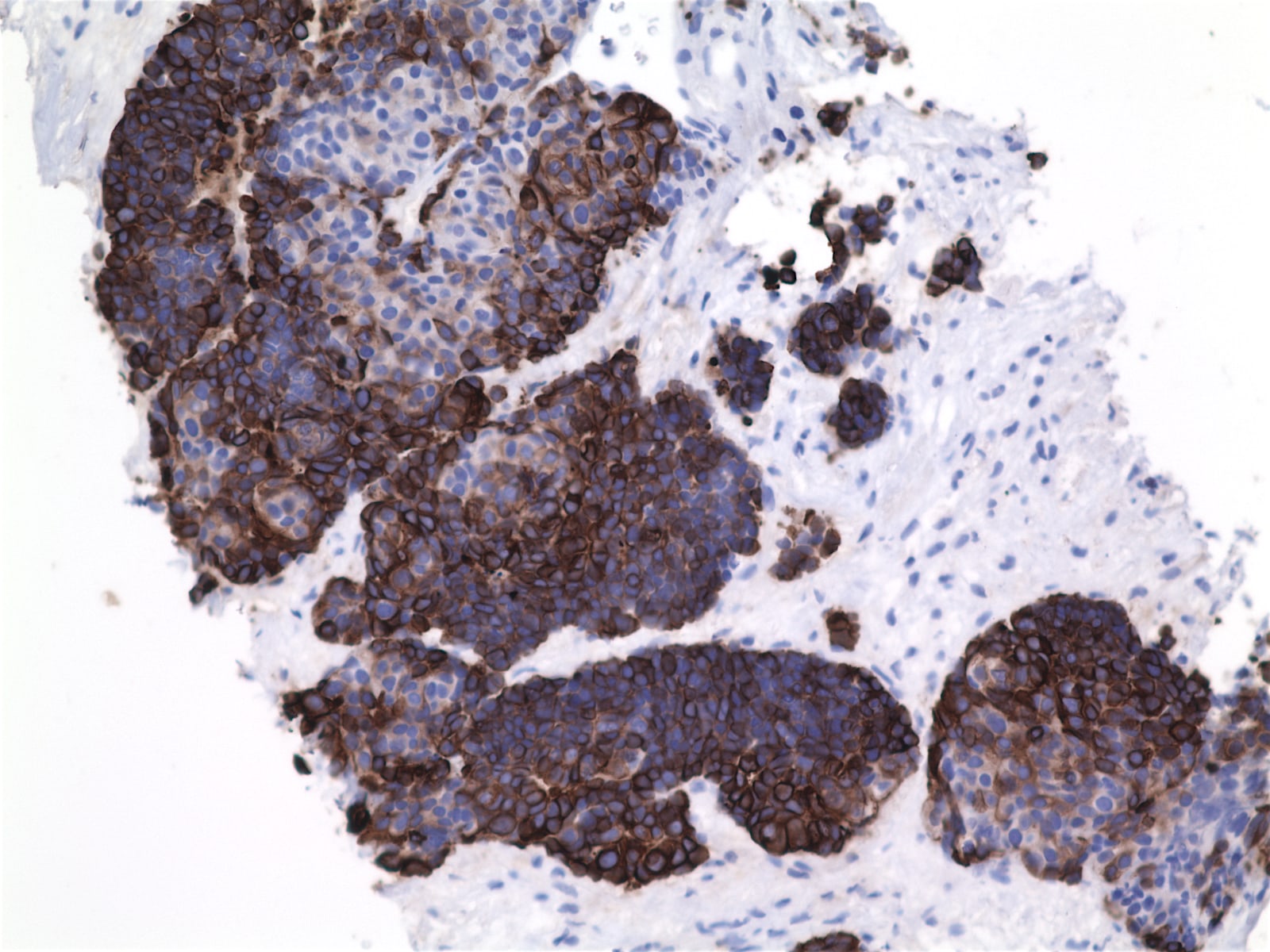
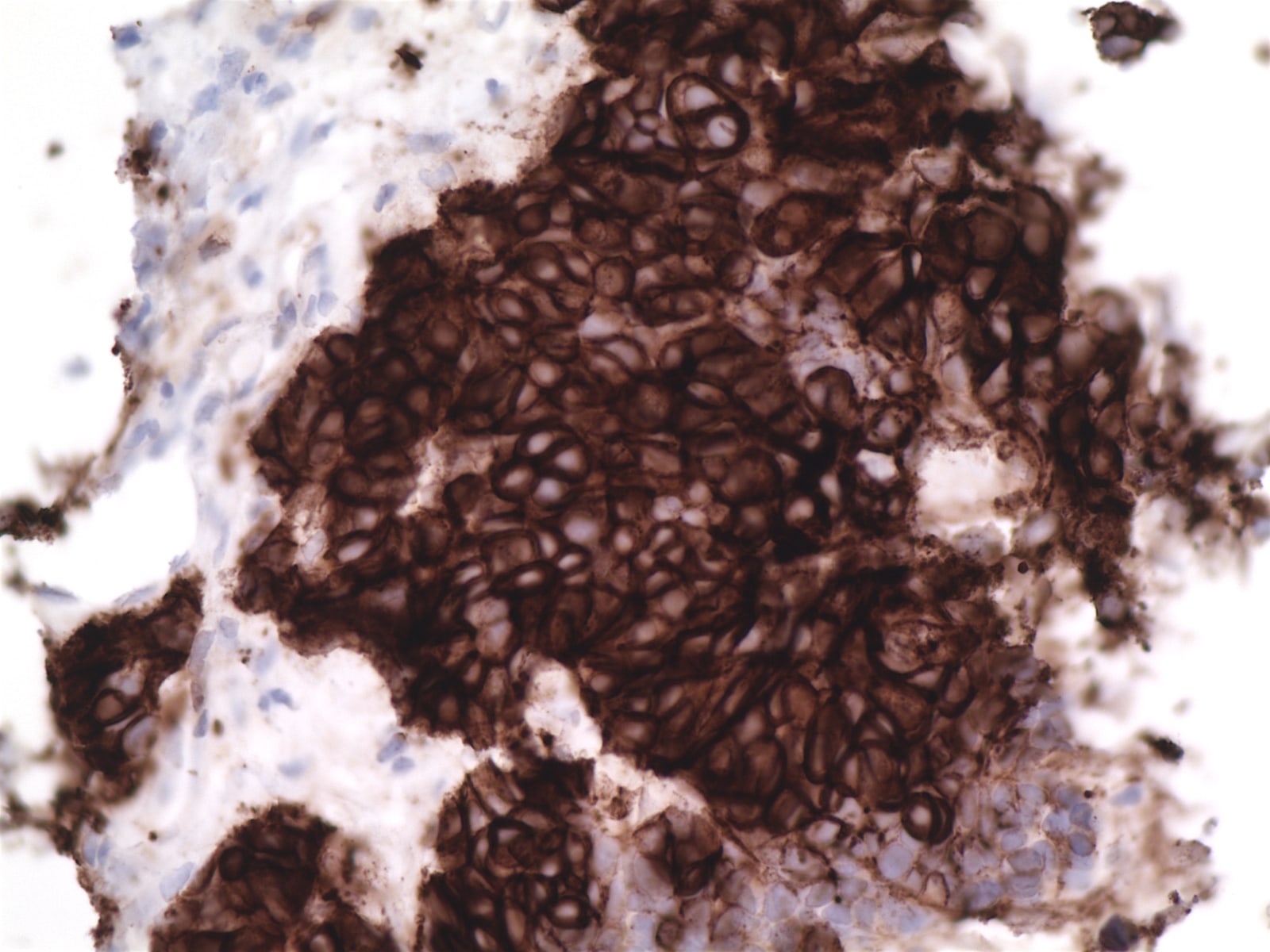
Positive stains
- Keratin, CD5, CD70, often EMA, variable CEA (if overt glandular differentiation), c-kit, GLUT1 (Am J Surg Pathol 2000;24:742, Am J Surg Pathol 2011;35:1296, Virchows Arch 2011;458:615)
Negative stains
- Vimentin, proteasome beta subunit (Am J Surg Pathol 2011;35:1296)
Electron microscopy description
- Well formed desmosome-like intercellular junctions, cytoplasmic tonofilaments that may insert into junctional complexes
Differential diagnosis
- Metastatic carcinoma
- Thymoma type B3:
- GLUT1 usually negative (Mod Pathol 2009;22:1341)
Board review style question #1
Which 2 antibodies are most helpful in diagnosing thymic carcinoma?
A. CK5/6, 34bE12
B. CD5, p63
C. CEA, synaptophysin
D. p63, p40
E. KIT / CD117, INSM1
A. CK5/6, 34bE12
B. CD5, p63
C. CEA, synaptophysin
D. p63, p40
E. KIT / CD117, INSM1
Board review style answer #1
B. CD5 combined with p63 are helpful thymic markers.
Comment Here
Reference: Thymic squamous cell carcinoma
Comment Here
Reference: Thymic squamous cell carcinoma
