

Skin nontumor
Dermal perivascular and vasculopathic reaction patterns
Dermal hypersensitivity reaction
Authors: Jiejun Wu, M.D., Ph.D., Maxwell A. Fung, M.D.
Editorial Board Member: Viktoryia Kozlouskaya, M.D., Ph.D.


Last author update: 30 September 2021
Last staff update: 23 January 2023
Copyright: 2021-2024, PathologyOutlines.com, Inc.
PubMed Search: Dermal hypersensitivity reaction pathology review [PT]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Wu J, Fung MA. Dermal hypersensitivity reaction. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumordermalhypersensitivity.html. Accessed April 26th, 2024.
Definition / general
- Nonspecific histologic reaction pattern that may be seen in multiple clinical conditions
- Superficial and mid dermal perivascular lymphocytic infiltrate with eosinophils and minimal, if any, epidermal alteration (J Am Acad Dermatol 2002;47:898, Am J Dermatopathol 2004;26:516, Patterson: Weedon's Skin Pathology, 5th Edition, 2020)
- Clinically confirmed disorders include spongiotic / eczematous dermatitis, arthropod bite reaction, urticaria, drug eruption or idiopathic (see Terminology)
Essential features
- Sparse to moderately dense superficial and mid perivascular and interstitial lymphocytic infiltrate with eosinophils
- Epidermal changes may be absent, minimal (spongiotic or vacuolar interface) or secondary (excoriation)
Terminology
- Comparable or equivalent histologic terms: cutaneous hypersensitivity reaction / response, dermal hypersensitivity response, urticarial hypersensitivity reaction
- For idiopathic pruritic skin conditions, some clinicians include dermal hypersensitivity reaction in their clinical differential diagnosis
- Similar or equivalent terms: itchy red bump disease, papular dermatitis, subacute prurigo and urticarial dermatitis
- Note: papular urticaria is a synonym for arthropod bite reactions; drug induced hypersensitivity syndrome (DIHS) is a specific type of drug reaction
Epidemiology
- Most reported patients are adults but may occur at any age
- Urticarial dermatitis was reported mostly in adults in multiple series (J Am Acad Dermatol 2002;47:898, Arch Dermatol 2006;142:29, J Am Acad Dermatol 2014;70:263)
Sites
- Idiopathic cases tend to involve the trunk, upper extremities or lower extremities, often symmetrically
- In cases with an identified disorder, involved sites should be compatible with the specific disorder (J Am Acad Dermatol 2002;47:898, Arch Dermatol 2006;142:29, J Am Acad Dermatol 2014;70:263)
Pathophysiology
- For idiopathic cases, T cell hypersensitivity with overexpression of Th2 cytokines may be involved (Arch Dermatol 2006;142:932, Actas Dermosifiliogr (Engl Ed) 2018;109:929)
Etiology
- Idiopathic until or unless confirmed to be other entities based on clinical correlation (see Differential diagnosis)
Clinical features
- Pruritus, may be intense (J Am Acad Dermatol 2002;47:898, Arch Dermatol 2006;142:29)
- Idiopathic cases typically present with urticarial or eczematous papules or plaques
- Lesions are typically multiple and symmetrical and may be numerous; excoriation may be present
Diagnosis
- Histologic reaction pattern that must be confirmed microscopically but the final diagnosis requires clinical correlation
- Deeper tissue sections to rule out other diagnoses may be needed; e.g., folliculitis, spongiotic dermatitis, scabies may become apparent only in deeper sections
- Exceptionally, may be a paraneoplastic hypersensitivity reaction (J Am Acad Dermatol 2010;63:e13, Clin Exp Dermatol 2016;41:322)
Laboratory
- No laboratory requests are mandated but screening for evidence of specific causes may be prudent (see Differential diagnosis)
- Ancillary testing may include a second biopsy for direct immunofluorescence (DIF) testing, scabies prep, complete blood count (CBC) or other serologic studies (J Am Acad Dermatol 2014;70:263)
Prognostic factors
- Idiopathic cases have chronic course with potentially unsatisfactory responses to treatment (see Treatment)
- No reported impact on life expectancy in idiopathic cases
Case reports
- 53 year old woman with rituximab induced urticarial dermatitis (Saudi J Kidney Dis Transpl 2017;28:657)
- 66 year old man with severe, refractory pruritus on his back and occult pancreatic cancer (Clin Exp Dermatol 2016;41:322)
- 69 year old man with long term control of dermal hypersensitivity reaction with mycophenolate mofetil (Arch Dermatol 2006;142:1512)
Treatment
- In cases with a clinically confirmed disorder, management is dictated by standard management for that disorder
- In idiopathic cases, treatment is symptomatic and management tends to be challenging and unsatisfactory
- Phototherapy, systemic steroids and immunosuppressants, such as methotrexate and mycophenolate mofetil have been reported (J Am Acad Dermatol 1998;38:929, J Dermatolog Treat 2015;26:431, Arch Dermatol 2006;142:1512, Ann Dermatol 2017;29:143)
Clinical images
Contributed by Maxwell A. Fung, M.D.

Crusted papules coalescing into plaques

Papules and lichenified plaques

Multiple papules on the leg

Urticarial papules and plaques
Microscopic (histologic) description
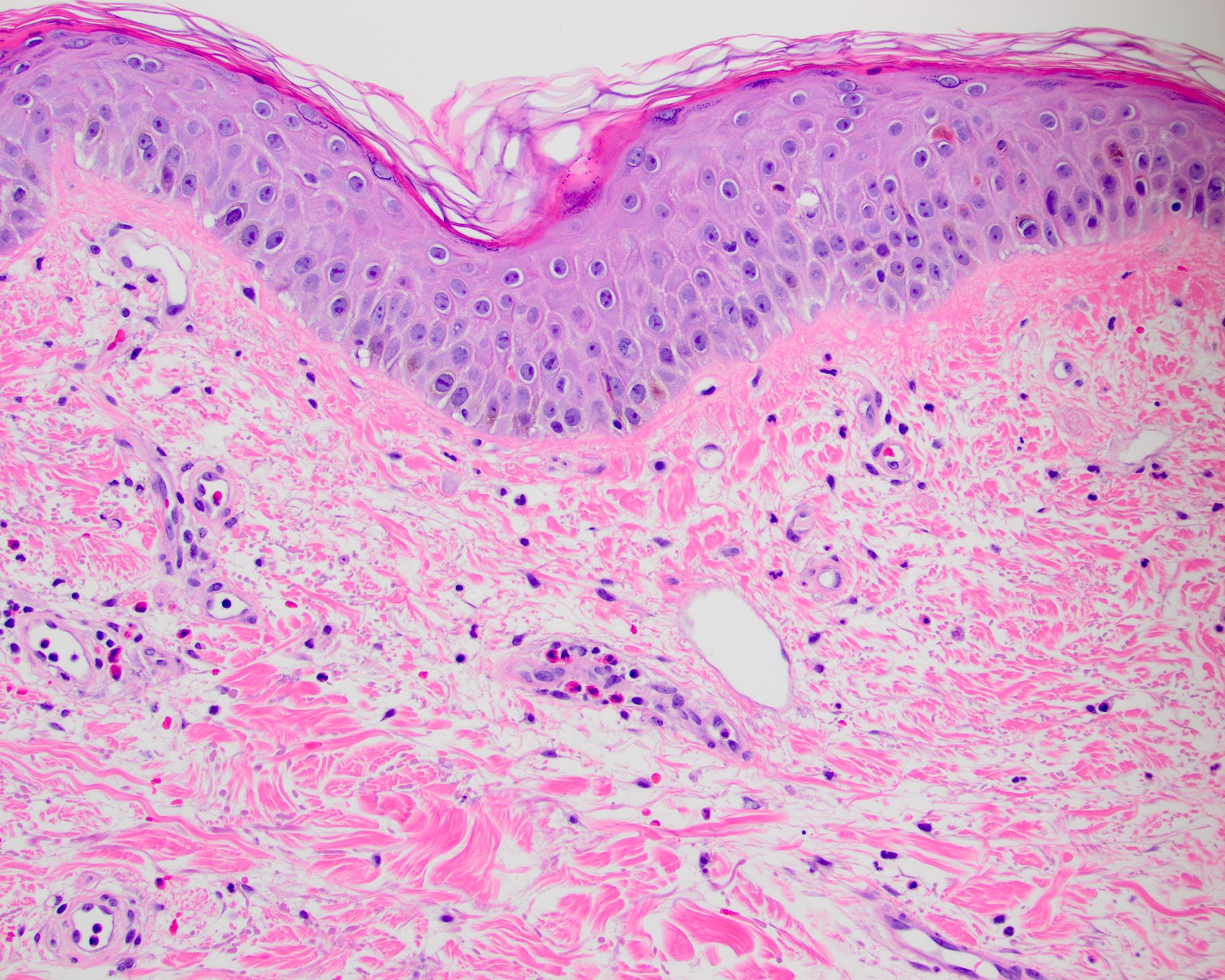
- Superficial and mid dermal perivascular and interstitial infiltrate involving the superficial (papillary) and mid (upper reticular) dermis; may extend to deep reticular dermis
- Predominantly lymphocytic infiltrate with eosinophils; with or without neutrophils
- Varying intensity of infiltrate, typically sparse to moderately dense
- Epidermal alteration, if present, may consist of minimal parakeratosis, spongiosis, vacuolar interface changes or secondary crust / excoriation
- References: J Am Acad Dermatol 2002;47:898, Arch Dermatol 2006;142:29, J Am Acad Dermatol 2014;70:263
Microscopic (histologic) images
Contributed by Maxwell A. Fung, M.D.
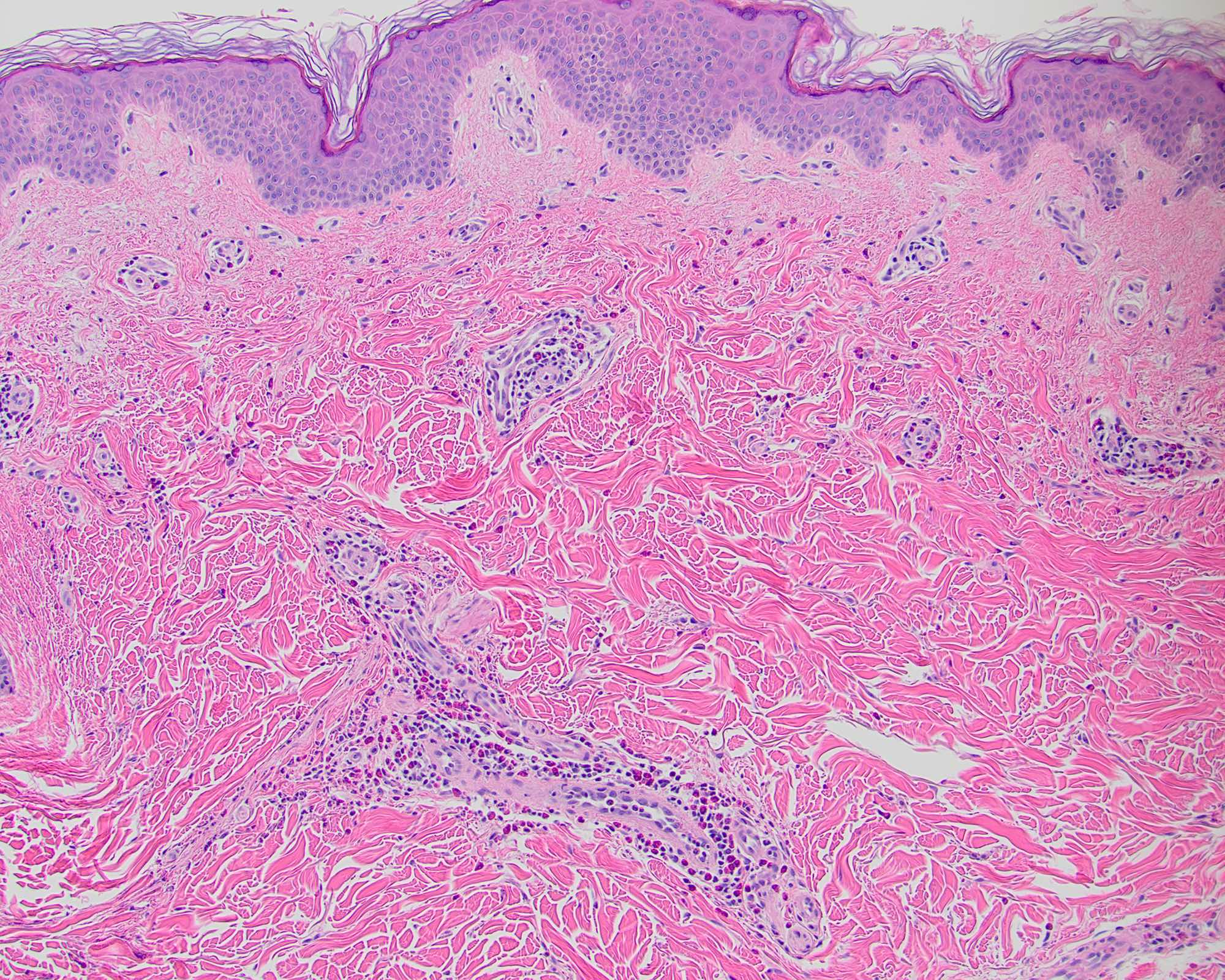
Itchy red bump disease
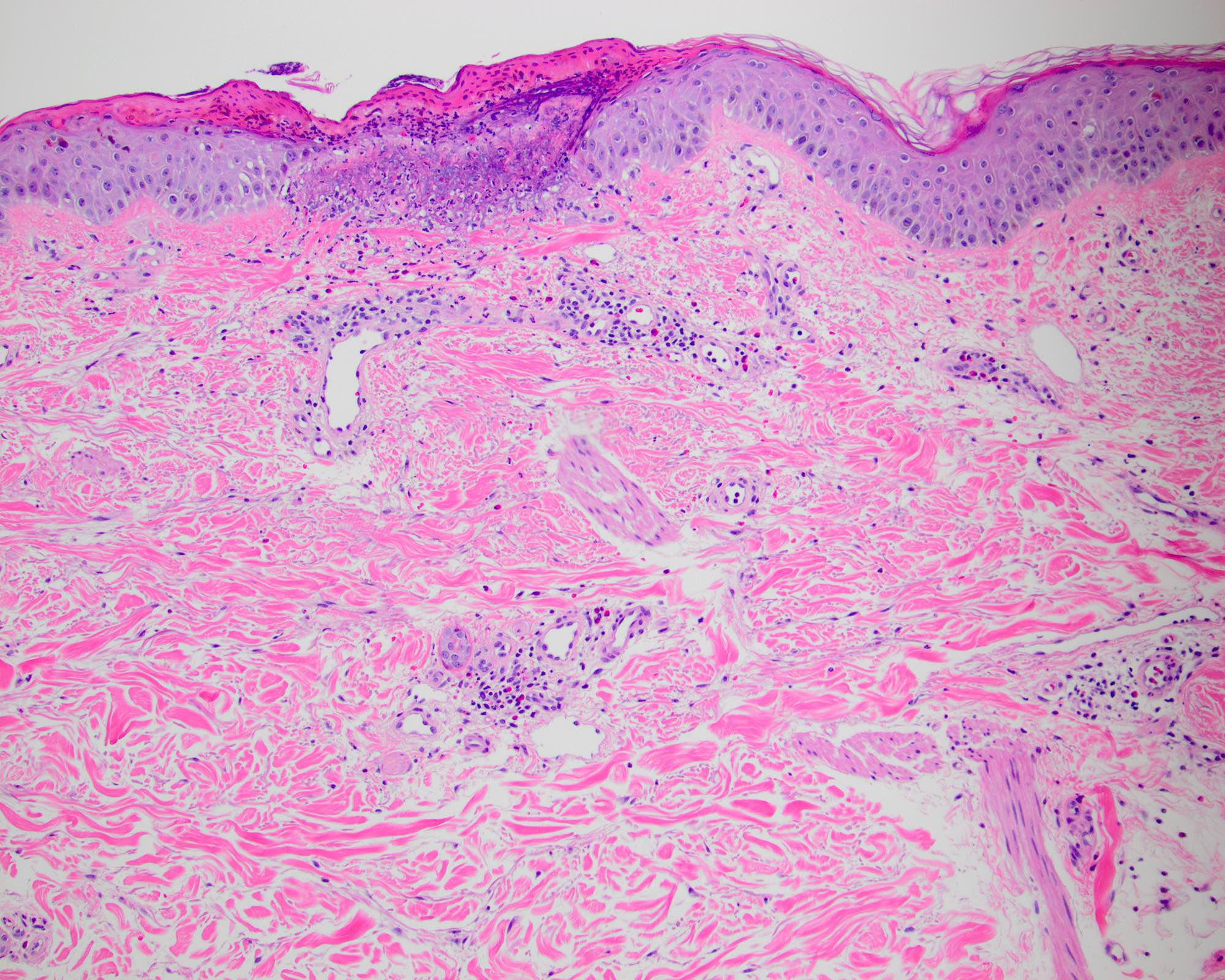
Atopic dermatitis
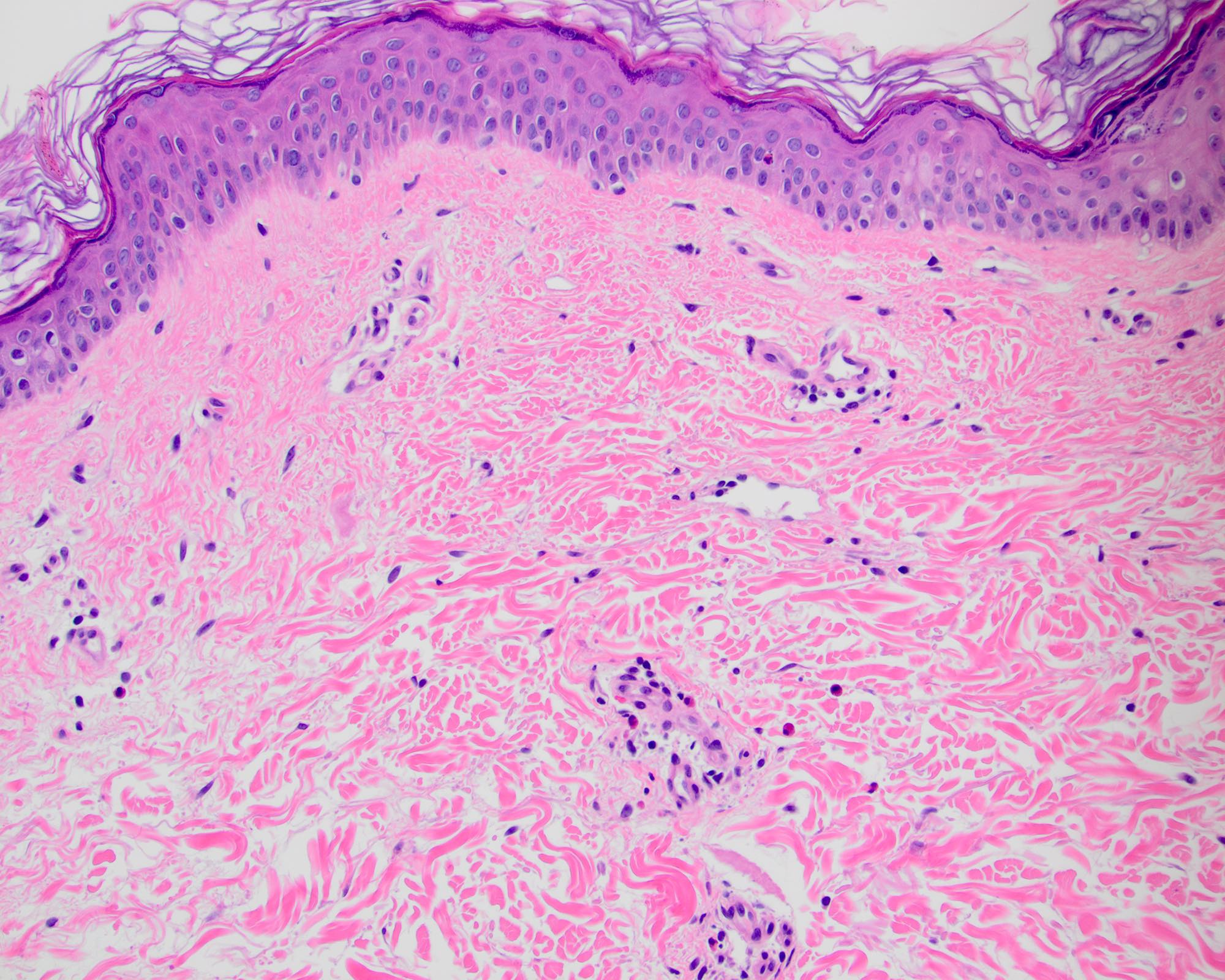
Urticarial dermatitis
Videos
Perivascular dermatitis, invisible dermatoses and sclerosing disorders
Sample pathology report
- Example #1 (circa 2001, University of Connecticut)
- Clinical information: rule out hypersensitivity reaction
- Specimen / site: left upper arm
- Diagnosis: dermal hypersensitivity reaction (see comment)
- Comment: Deeper sections have been performed. The histological differential diagnosis includes a lesion of urticaria. There is a sparse superficial and mid dermal perivascular infiltrate composed of lymphocytes, histiocytes, neutrophils and eosinophils.
- Example #2 (circa 1998, Cornell University Medical Center)
- Superficial and deep perivascular dermatitis, consistent with a dermal hypersensitivity reaction, biopsy:
- T-01000; T-02471; M-40006
- ICD-9: V72.6 and 693.89
- Comment: A reaction to an internal antigen source seems likely because of the deep inflammation; however, slight spongiosis is noted and chronic allergic contact dermatitis cannot be completely ruled out histologically.
- Superficial and deep perivascular dermatitis, consistent with a dermal hypersensitivity reaction, biopsy:
- Example #3 (circa 2020, University of California Davis)
- Skin, right posterior forearm, punch biopsy:
- Sparse dermatitis with eosinophils and mild spongiosis (see comment)
- Comment: The histologic differential diagnosis includes a drug reaction or spongiotic / eczematous dermatitis, as well as a sparse arthropod bite or other hypersensitivity reaction. There is focal epidermal necrosis consistent with external trauma. Overt fungi on H&E is not visible; a fungal stain may be obtained upon request if necessary.
- Skin, right posterior forearm, punch biopsy:
- Example #4 (circa 2020, University of California Davis)
- Skin, mid back, punch biopsy:
- Sparse perivascular and interstitial dermatitis with eosinophils (see comment)
- Comment: The histologic differential diagnosis includes a drug or other hypersensitivity reaction, nondiagnostic spongiotic / eczematous dermatitis or as a diagnosis of exclusion, an idiopathic eruption (e.g., itchy red bump disease, urticarial dermatitis). Some eosinophils are present near the dermal epidermal junction, so urticarial pemphigoid could also be considered (but not specifically favored). Deeper sections fail to reveal additional findings.
- Skin, mid back, punch biopsy:
Differential diagnosis
- Differential diagnosis of dermal hypersensitivity reaction is broad; clinical correlation is required in all instances
- Drug eruption:
- Subtle vacuolar interface changes or spongiosis are often present
- Arthropod bite reaction (papular urticaria):
- Infiltrates tend to be deeper and denser with abundant eosinophils; may involve subcutis; may show centrally positioned intraepidermal vesicle or crusted erosion / ulcer (punctum)
- Clinically, the lesions should be exclusively papules, erythematous and usually edematous / urticarial and tend to occur either as a single or localized cluster of papules on the extremities, ideally with a patient confirmed mosquito, flea, mite or other arthropod exposure
- Atopic dermatitis:
- Biopsies of atopic dermatitis usually present as spongiotic dermatitis so more prominent spongiosis, such as spongiotic vesicles and confluent or diffuse parakeratosis, would support this possibility
- Clinically, patients present with eczematous skin plaques or papules and a personal or history of atopy; diagnostic criteria (Hanifin-Rajka) for atopic dermatitis may be applied by the clinician
- Contact dermatitis:
- Biopsies of contact dermatitis usually present as spongiotic dermatitis, so more prominent spongiosis, such as spongiotic vesicles and confluent or diffuse parakeratosis, would support this possibility
- Clinically, allergens or irritants may be confirmed by clinical history or patch testing
- Spongiotic / eczematous dermatitis, NOS:
- Dermal hypersensitivity reaction with more prominent spongiosis, such as spongiotic vesicles and confluent or diffuse parakeratosis, would support this possibility
- Clinical correlation is required to confirm a specific type of spongiotic / eczematous dermatitis (e.g., atopic, contact, nummular)
- Urticaria:
- Dermal hypersensitivity reaction with no epidermal changes at all; dermal edema and neutrophils typically present in addition to the lymphocytes and eosinophils
- Pruritic urticarial papules and plaques of pregnancy (PUPPP):
- Dermal hypersensitivity reaction, sometimes with more prominent spongiosis and marked papillary dermal edema
- Associated with malignancy or other systemic conditions:
- Dense, eosinophil predominant infiltrates have been reported; reported associations include Hodgkin lymphoma, large B cell lymphoma, leukemia, myelodysplastic syndrome, prostate cancer, colon cancer, vulvar cancer, breast cancer, autoimmune diseases, herpes virus and H. pylori infection (Clin Exp Dermatol 2016;41:322, J Am Acad Dermatol 2010;63:e13, J Cutan Pathol 2012;39:929, JAAD Case Rep 2020;6:156)
- Urticarial vasculitis:
- In addition to clinical correlation, evidence of vasculitis from another biopsy or a positive direct immunofluorescence (DIF) result would typically be required
- Bullous pemphigoid:
- Infiltrate of eosinophils centered upon the dermoepidermal junction and within the epidermis (eosinophilic spongiosis) would be typical of the urticarial or prebullous phase of pemphigoid
- Positive DIF result from perilesional skin would be required
- Scabies:
- Crust and prominent eosinophils are typical
- Deeper sections, multiple biopsies or scabies prep may be required to identify diagnostic findings (mite, eggs, feces [scybala])
- Wells syndrome (eosinophilic cellulitis) and other eosinophil predominant infiltrates:
- Dermal hypersensitivity reaction must contain eosinophils but the infiltrate is predominately lymphocytic (Dermatol Clin 2012;30:667)
- Flame figures typify Wells syndrome but may be present occasionally in any eosinophil rich dermal infiltrate
- Viral exanthem:
- Vacuolar interface dermatitis, often with extravasated erythrocytes and exocytosis of lymphocytes, often accompanies sparse dermal infiltrates
- Eosinophils are not specifically characteristic of a viral exanthem but would not exclude this possibility
Additional references
- Fung: Inflammatory Diseases of the Dermis and Epidermis, 2010, Billings: Inflammatory Dermatopathology: A Pathologist's Survival Guide, 2nd Edition, 2016, UpToDate: Uritcarial Dermatitis [Accessed 22 September 2021], Curr Allergy Asthma Rep 2015;15:62, Int J Dermatol 2019;58:e196, J Cutan Pathol 2021;48:592, Australas J Dermatol 2014;55:137, J Am Acad Dermatol 2010;62:541
Board review style question #1
Which of the following histologic findings is required for the diagnosis of dermal hypersensitivity reaction?
- Eosinophils
- Granulomas
- Neutrophils
- Plasma cells
- Spongiosis
Board review style answer #1
A. Eosinophils. Required histologic features of dermal hypersensitivity reaction include a perivascular and interstitial lymphocytic infiltrate with eosinophils. Neutrophils and spongiosis are variable but not required findings. Granulomas and plasma cells are not features of dermal hypersensitivity reaction.
Comment Here
Reference: Dermal hypersensitivity reaction
Comment Here
Reference: Dermal hypersensitivity reaction
Board review style question #2
A punch biopsy of a pruritic eruption of 5 years duration involving the trunk of a 64 year old man is reported as a dermal hypersensitivity reaction. The pathologist commented that deeper sections were negative. The microscopic description documents scant parakeratosis and spongiosis. Which of the following may be considered in the differential diagnosis?
- Folliculitis
- Sarcoid
- Syphilis
- Urticaria
- Urticarial dermatitis
Board review style answer #2
E. Urticarial dermatitis. The negative deeper sections are against folliculitis. Sarcoid would require granulomas which are not a feature of dermal hypersensitivity reaction. Syphilis typically shows a psoriasiform lichenoid pattern with plasma cells. The parakeratosis and spongiosis excludes urticaria.
Comment Here
Reference: Dermal hypersensitivity reaction
Comment Here
Reference: Dermal hypersensitivity reaction
