

Kidney nontumor / medical renal
Developmental & cystic diseases
Benign renal cysts
Authors: Rana Chakrabarti, M.D., M.P.H., Ian W. Gibson, M.B.Ch.B., M.D., Miao (Vivian) Lu, M.D., Deepak K. Pruthi, M.D., M.Sci.-T.S.
Editorial Board Members: Bonnie Choy, M.D., Jonathan E. Zuckerman, M.D., Ph.D.


Last author update: 23 March 2023
Last staff update: 23 March 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Benign renal cysts
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Radiology images | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Chakrabarti R, Gibson IW, Lu M, Pruthi DK. Benign renal cysts. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumorsimplecyst.html. Accessed May 14th, 2024.
Definition / general
- Discrete fluid filled cystic lesions within the kidney parenchyma or at the capsular surface
Essential features
- Common benign lesion usually seen incidentally in adults
- Fluid filled cortical or medullary cystic lesions lined by flattened epithelial cells but may have papillary excrescences or clear cell change
- Generally asymptomatic and do not require intervention
Epidemiology
- Prevalence in adults: 12 - 25%
- Present in up to 40% of patients undergoing abdominal imaging
- Rare in pediatric populations (< 1%) (J Urol 2002;167:21)
- Male predominance
Sites
- Renal cortex and medulla
Pathophysiology
- Diverticula of the distal collecting duct (DCT) or collecting tubules increase in number with age, probably as a result of weakening of the tubular basement membranes (Urol Res 1977;5:103)
Clinical features
- Predominantly asymptomatic and incidental
- Cyst hemorrhage may present with acute pain or asymptomatic microscopic hematuria
- Solitary or multiple renal cysts
- Unilateral or bilateral
- Risk factors: age, male, hypertension, renal dysfunction (BJU Int 2004;93:1300)
- Complications: hypertension
- Size and quantity increase with age, with more rapid growth under 50 years of age (J Urol 2002;167:21)
- 5.1% in fourth decade
- 36.1% in eighth decade
- Average increase in size and rate of enlargement is 2.82 cm and 6.3% yearly, respectively
Diagnosis
- Incidentally found on abdominal CT or at autopsy
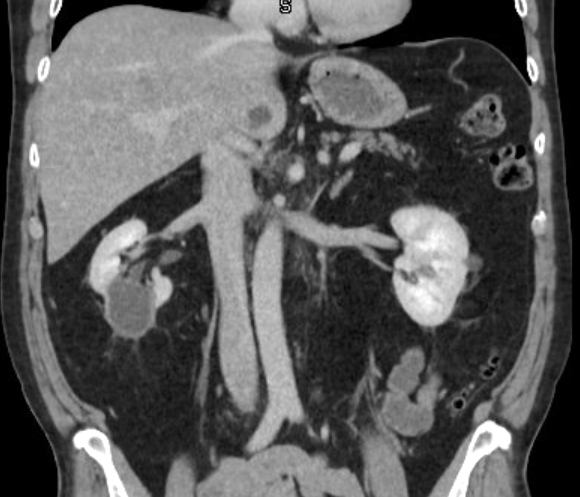
Radiology description
- Hairline thin wall with water attenuation (Radiology 2005;236:441)
- Absence of septations or calcifications
- No nodular enhancement
| Proposed Bosniak classification, version 2019* | ||
| Class | CT | MRI |
| I | Well defined, thin (≤ 2 mm) smooth wall; homogeneous simple fluid (29 to 20 Hounsfield units [HU]); no septa or calcifications; the wall may enhance | Well defined, thin (≤ 2 mm) smooth wall; homogeneous simple fluid (signal intensity similar to CSF); no septa or calcifications; the wall may enhance |
| II | 6 types, all well defined with thin (≤ 2 mm) smooth walls | 3 types, all well defined with thin (≤ 2 mm) smooth walls |
| IIF | Cystic masses with a smooth, minimally thickened (3 mm) enhancing wall or smooth minimal thickening (3 mm) of 1 or more enhancing septa or many (≥ 4) smooth thin (≤ 2 mm) enhancing septa | 2 types:
|
| III | 1 or more enhancing thick (≥ 4 mm width) or enhancing irregular (displaying ≤ 3 mm obtusely margined convex protrusion[s]) walls or septa | 1 or more enhancing thick (≥ 4 mm width) or enhancing irregular (displaying ≤ 3 mm obtusely margined convex protrusion[s]) walls or septa |
| IV | 1 or more enhancing nodule(s) (≥ 4 mm convex protrusion with obtuse margins or a convex protrusion of any size that has acute margins) | 1 or more enhancing nodule(s) (≥ 4 mm convex protrusion with obtuse margins or a convex protrusion of any size that has acute margins) |
Radiology images
Contributed by Deepak K. Pruthi, M.D., M.Sci.-T.S.

CT abdomen

Contrast enhanced

Axial CT
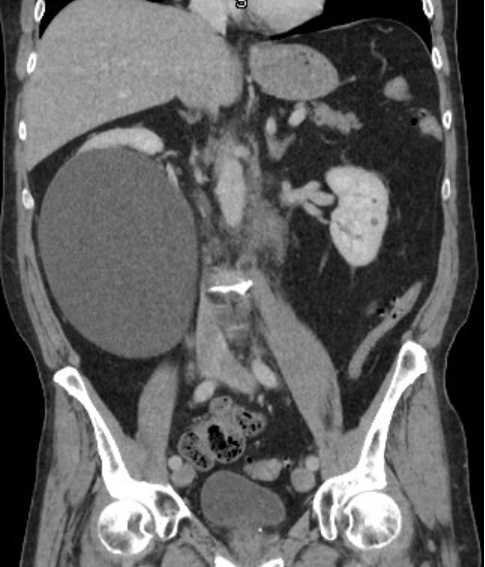
Coronal CT
Postsclerotherapy
Case reports
- 4 year old girl with infected right simple renal cyst (BMC Pediatr 2021;21:265)
- 21 year old man with hypertensive retinopathy and irregular shaped kidney (Balkan J Med Genet 2022;24:83)
- 30 year old woman with back pain (Int J Surg Case Rep 2022;98:107614)
- 75 year old man and woman with asymptomatic renal cystic mass (Medicine (Baltimore) 2019;98:e15249)
Treatment
- Generally, not indicated
- Percutaneous cyst aspiration if (Int J Urol 2003;10:63):
- Mass effect
- Pelvicalyceal obstruction
- Hypertension secondary to renal segmental ischemia
- Pain
- Hematuria
- Aspiration and sclerotherapy (AJR Am J Roentgenol 2008;190:1193, Abdom Radiol (NY) 2021;46:2875)
- Very rare: partial nephrectomy
Gross description
- Thin walled round cysts in renal cortex
- Up to 10 cm maximum diameter
- Unilocular or rarely multilocular
- Smooth contour
- Filled with clear or yellow fluid
- References: StatPearls: Simple Renal Cyst [Accessed 6 February 2023], Nephrol Dial Transplant 2014;29:iv106
Gross images
Images hosted on other servers:

Simple cyst of upper pole

Large cyst

Multiple, smooth renal cysts filled with serous fluid

Solitary, smooth
kidney cyst
(lower pole) filled
with serous fluid

Large cortical cysts with dark red blood
Microscopic (histologic) description
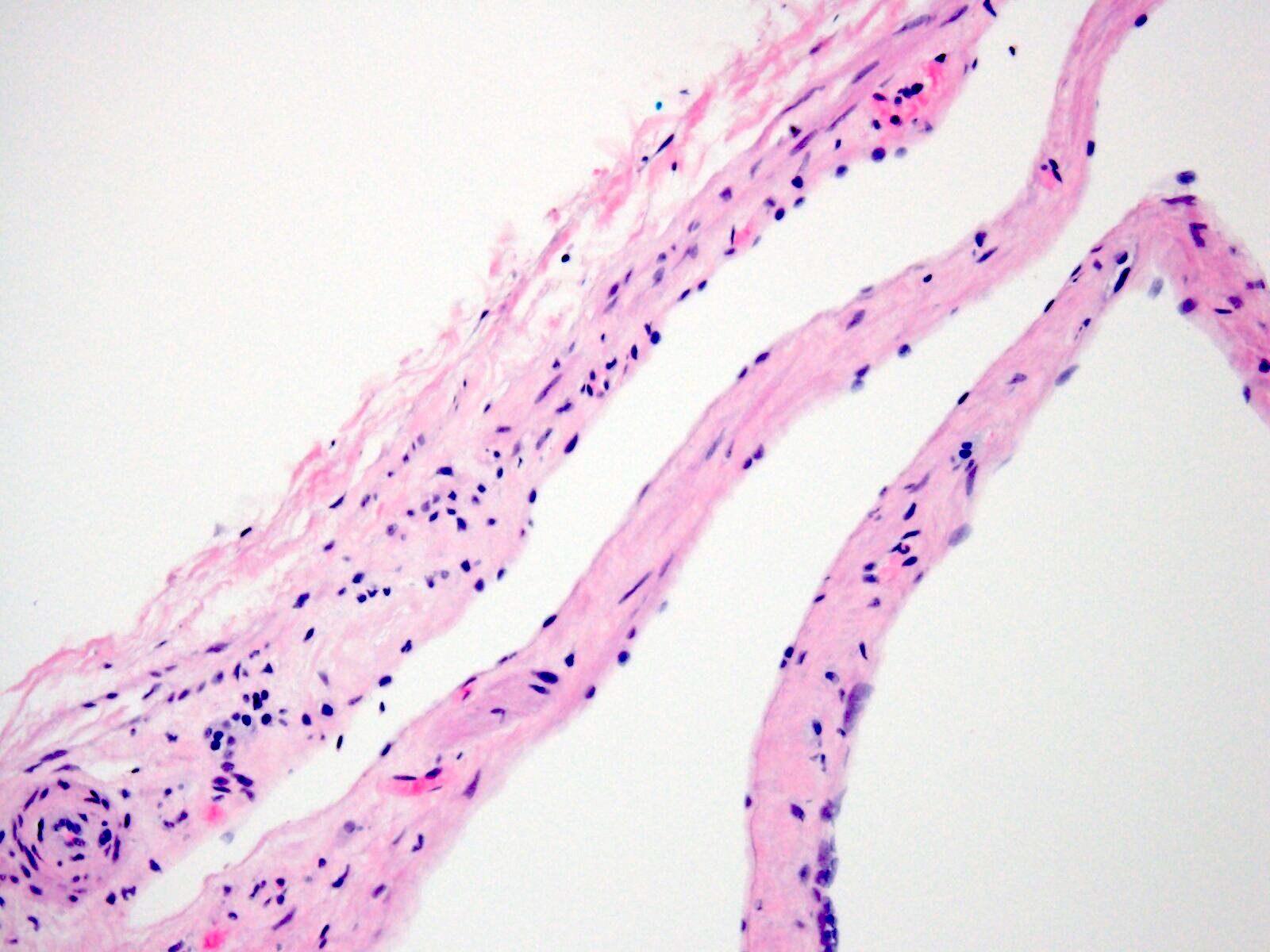
- Cyst wall is lined by single layer of cuboidal or attenuated epithelium
- Lining epithelium may be absent focally or entirely
- Atypical renal cysts have small papillary infoldings and a lining epithelium composed of cells with clear cytoplasm
- Negative for nests or expansile nodules of clear cells
- Cysts complicated by hemorrhage or infection may have hemosiderin laden macrophages and thicker fibrotic walls with focal calcifications
- Surrounding renal cortex shows effects of compression with chronic tubulointerstitial damage
- References: StatPearls: Simple Renal Cyst [Accessed 6 February 2023], Kidney Int 2006;70:1468, Postgrad Med J 1969;45:767
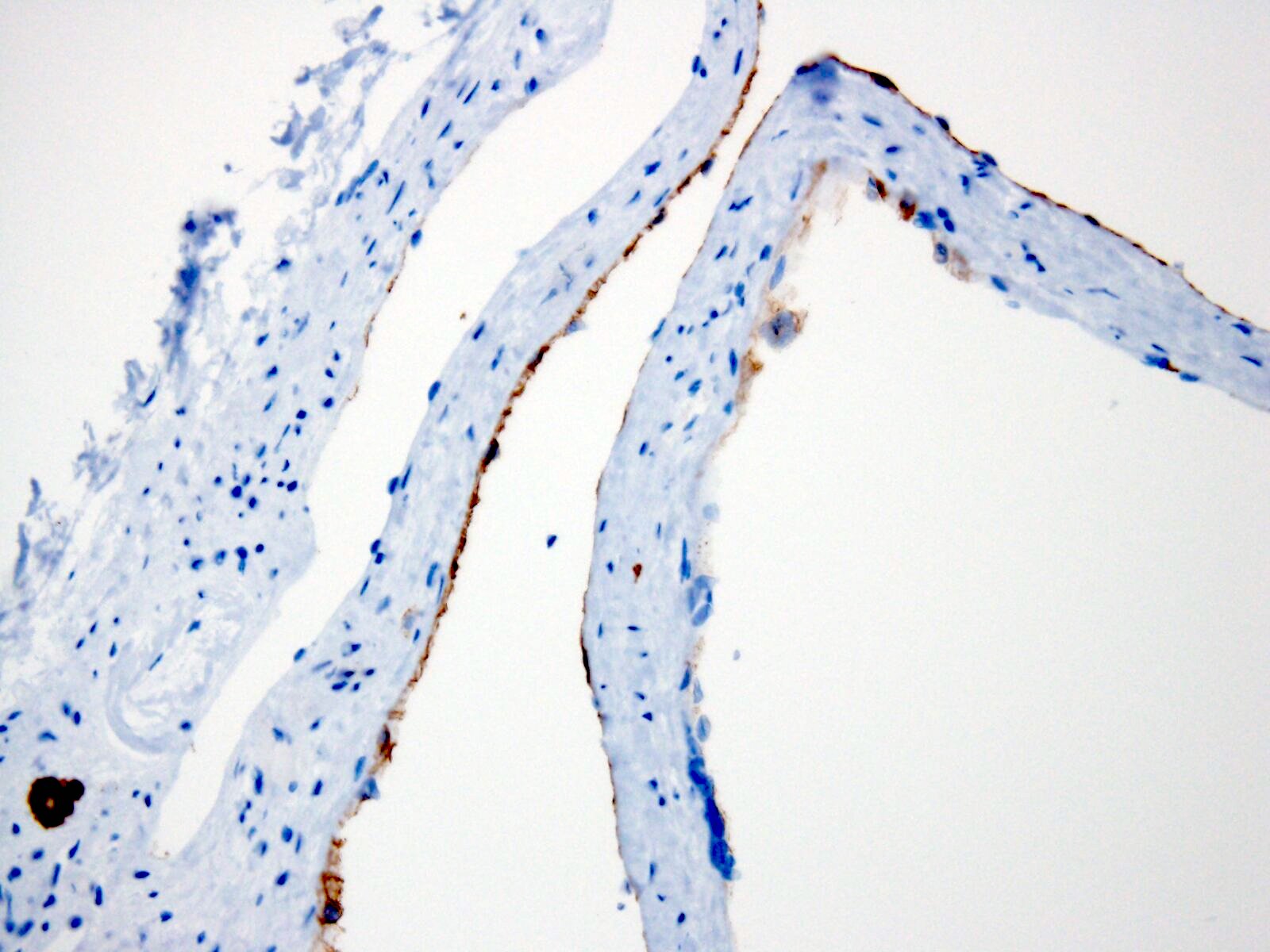
Microscopic (histologic) images
Contributed by Rana Chakrabarti, M.D., M.P.H.

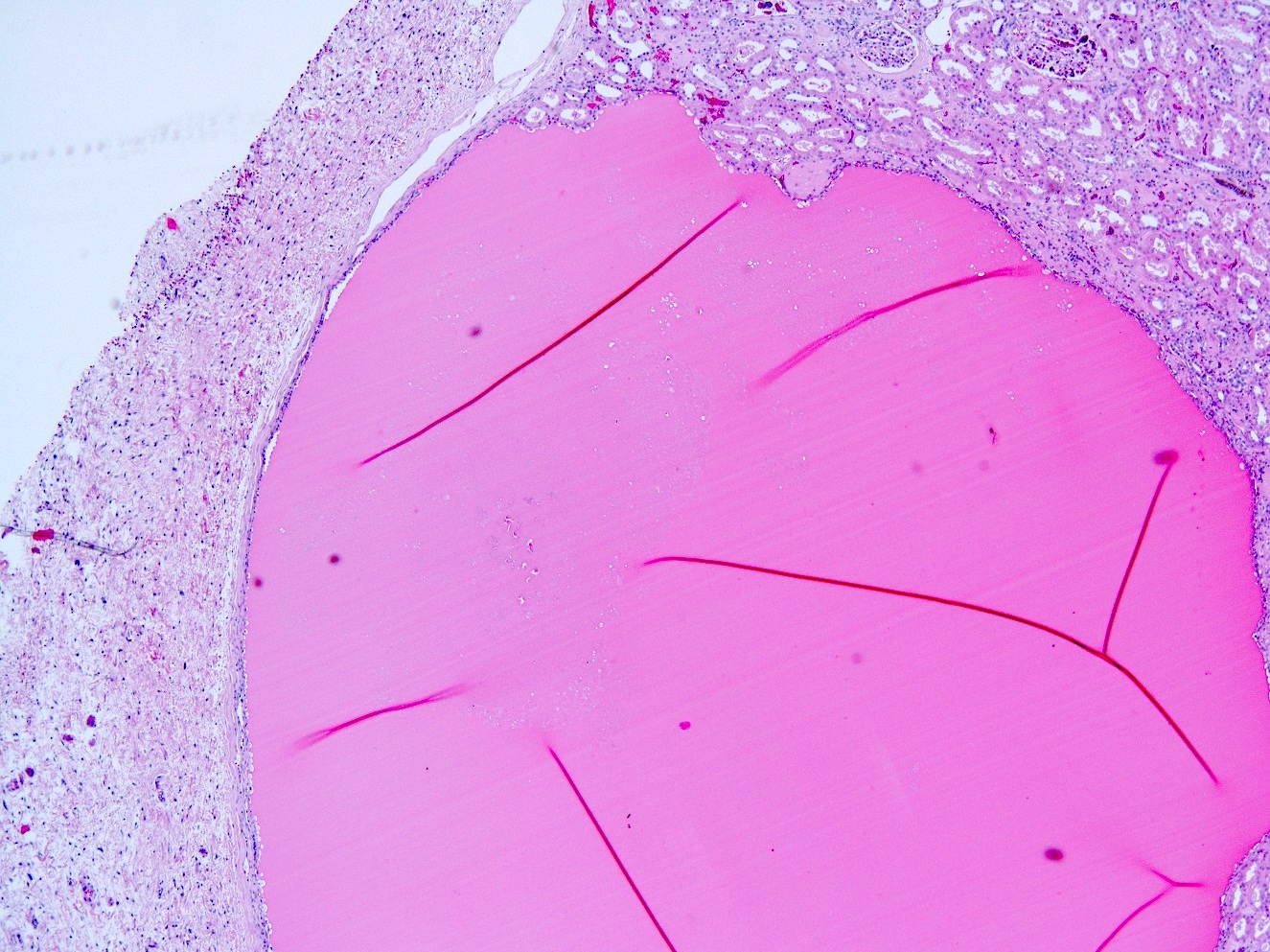
Subcapsular cortical cyst
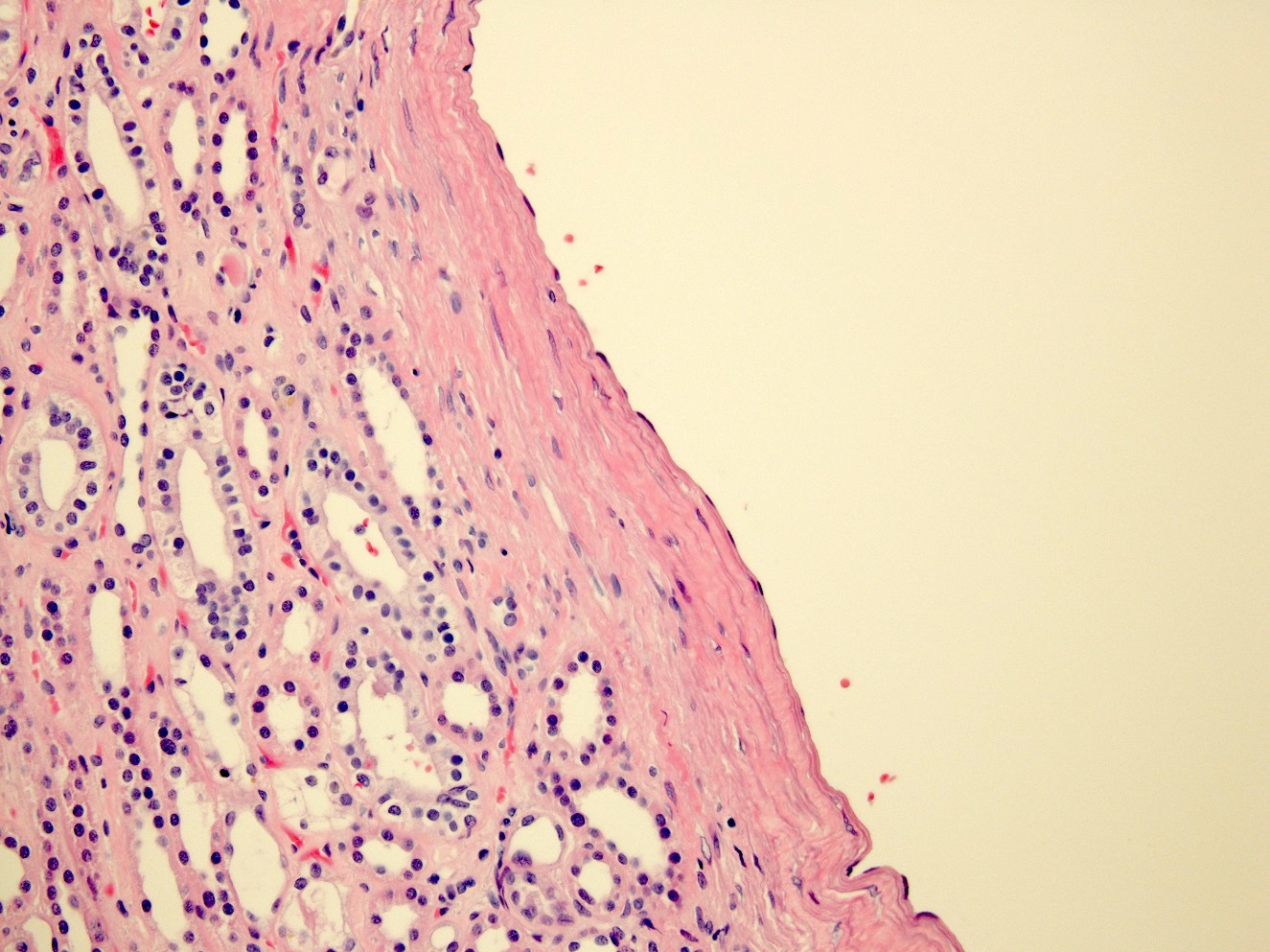
Flattened cyst wall epithelium
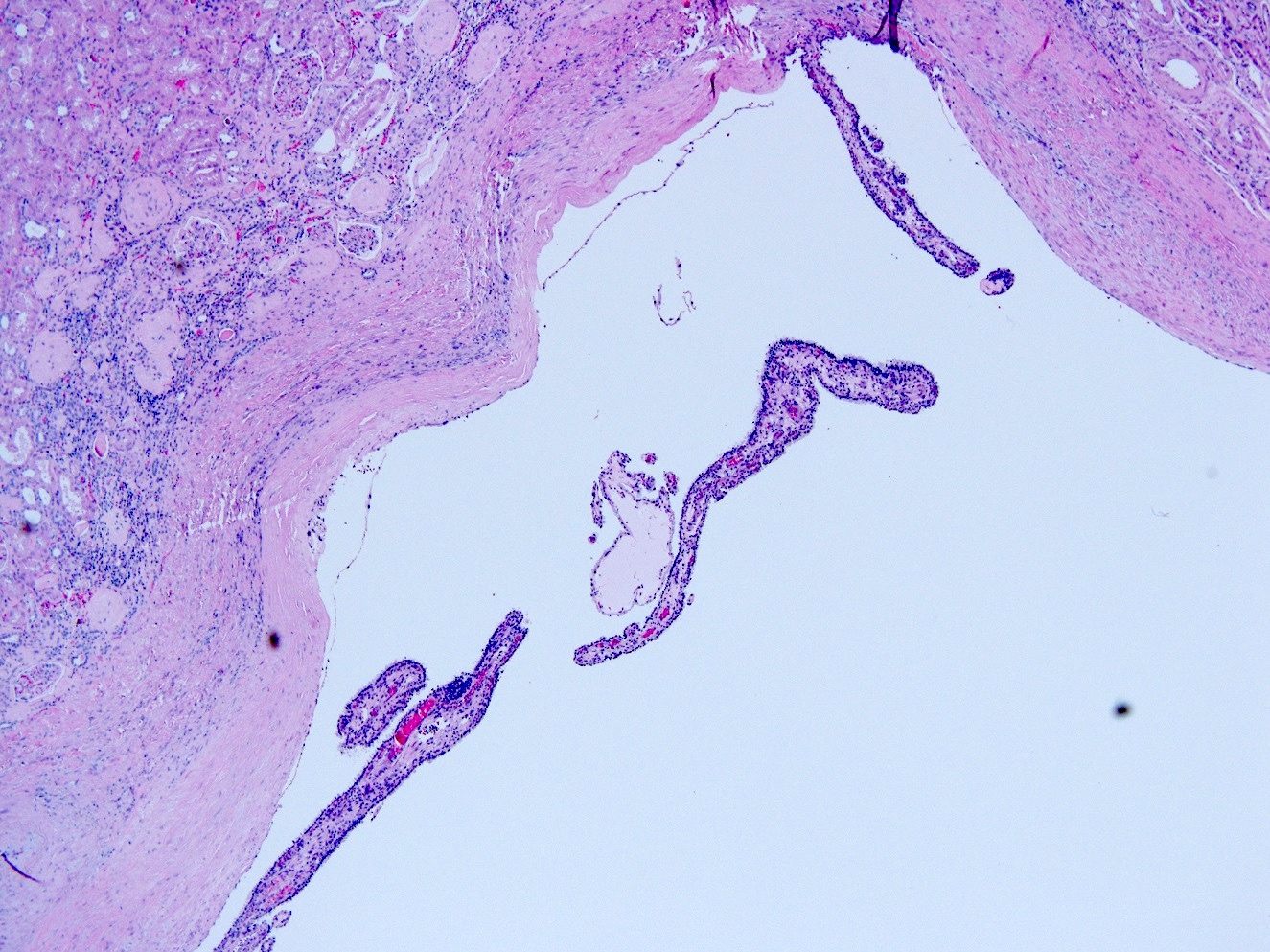
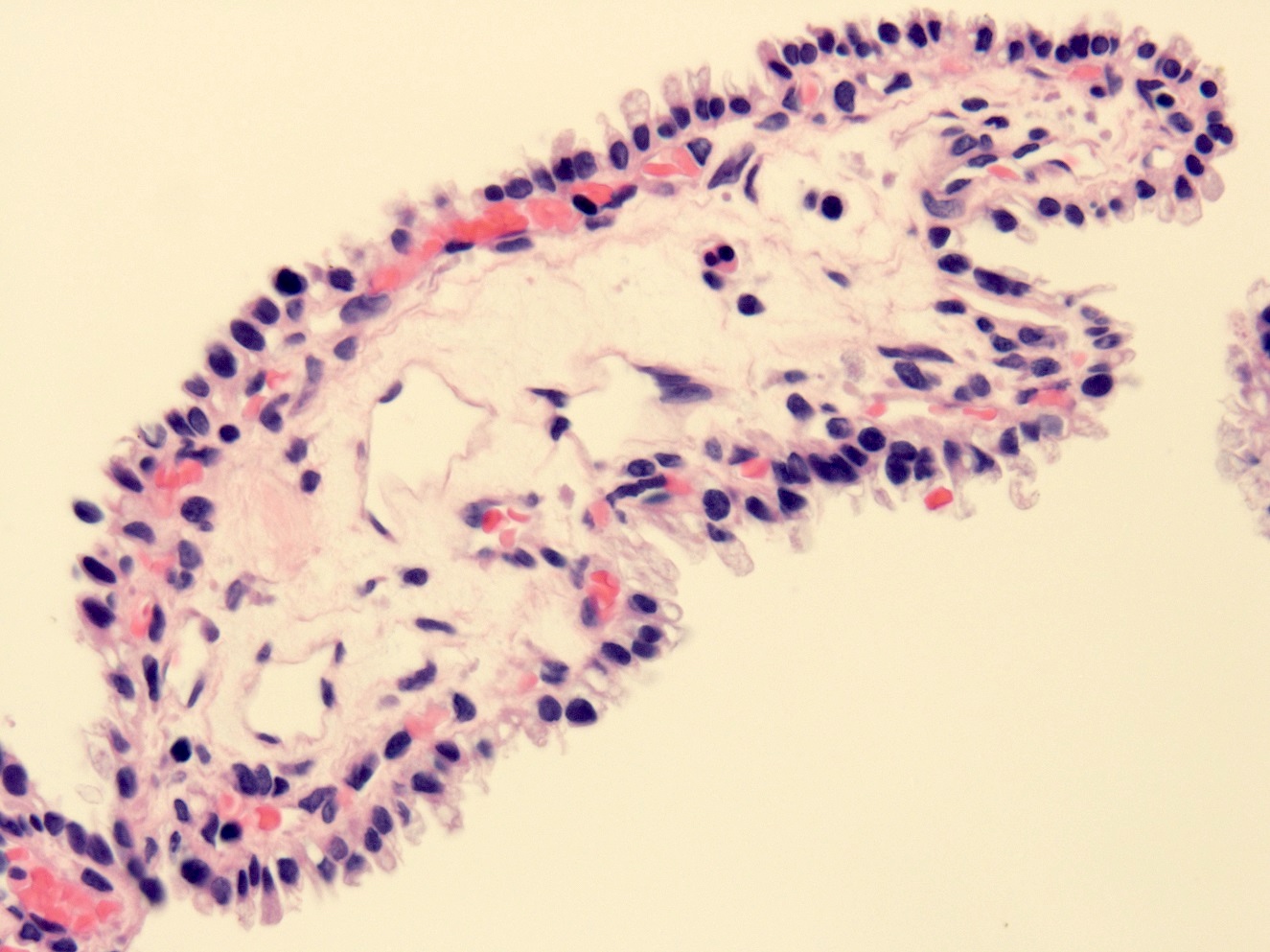
Papillary excrescence
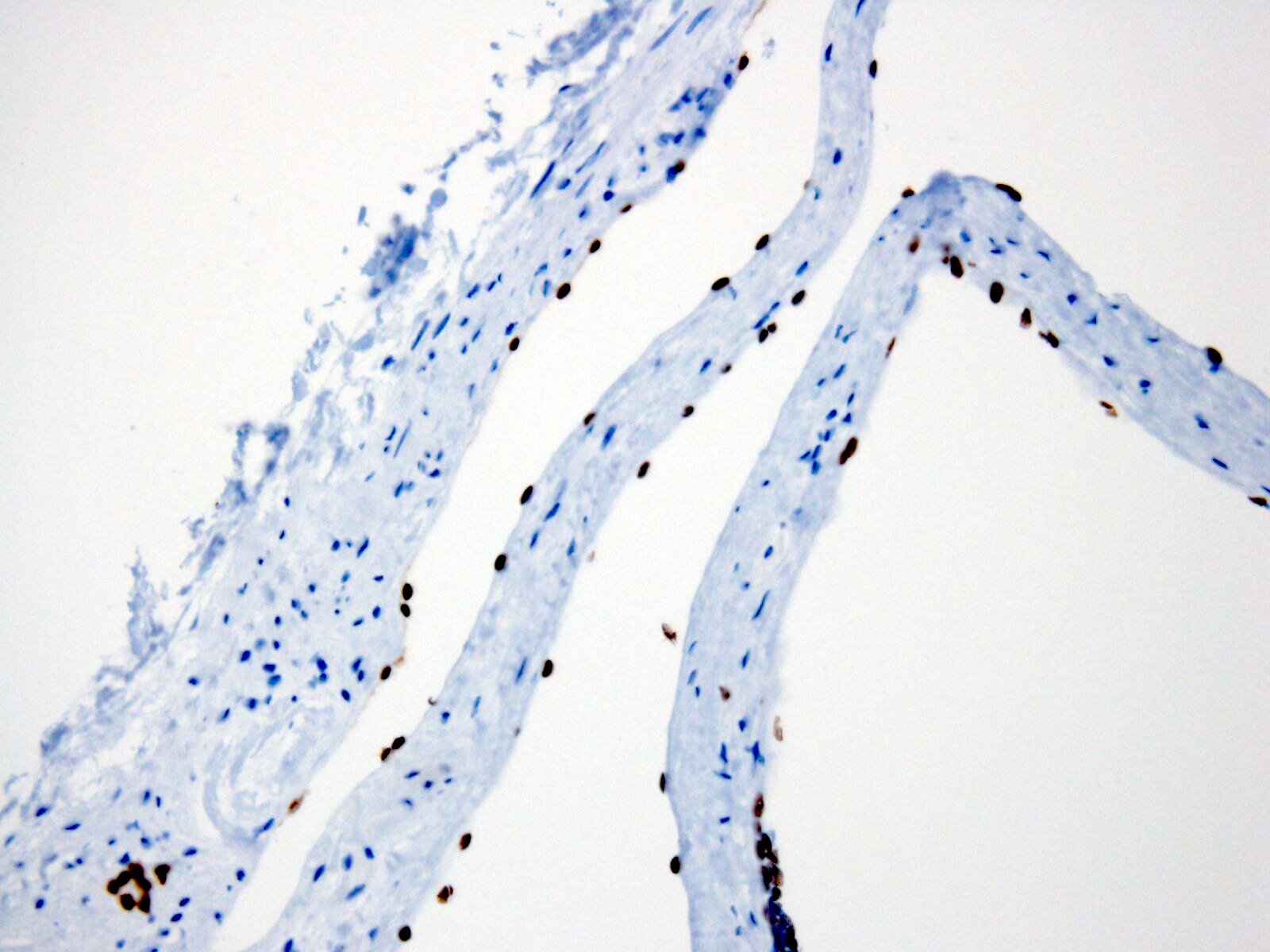
Positive stains
- CK7 membrane staining of lining epithelial cells
- PAX8 nuclear staining of lining epithelial cells
- Reference: Am J Surg Pathol 2016;40:202
Sample pathology report
- Right kidney, resection:
- Simple renal cyst
Differential diagnosis
- Multilocular cystic renal neoplasm of low malignant potential:
- Cysts lined by cuboidal clear cells
- Fibrous septa contain small nests of clear cells
- Cystic renal cell carcinoma:
- Extensively cystic neoplasm with solid areas or expansile nodules of renal cell carcinoma
- Most commonly clear cell renal cell carcinoma
- Autosomal dominant polycystic kidney disease:
- Multiple cortical cysts on bilateral kidneys
- Decreased renal function
- Family history
- Genetic predisposition
- Acquired cystic disease:
- Patients undergoing long term renal replacement therapy
- Multiple cortical and medullary cysts in end stage chronic kidney damage
- Adult cystic nephroma / mixed epithelial stromal tumor:
- Female predominance
- Age: 40 - 50s
- Variable sized cysts lined by benign renal tubular epithelium
- Ovarian type stromal component; often estrogen and progesterone receptor positive
Additional references
Board review style question #1
Which one of the following statements is true about renal cysts?
- Acquired sporadic simple renal cysts require no further investigation
- Large renal cysts are typically managed with laparoscopic cyst decortication
- Renal cell carcinoma is a common complication of simple renal cysts
- Simple renal cysts frequently result in obstruction of the of the segmental calyces
- The prevalence of sporadic renal cysts remains fairly constant beyond age 40
Board review style answer #1
A. Acquired sporadic simple renal cysts require no further investigation. Answer B is incorrect because even large cysts are left untreated unless there are other symptoms, including pain, hematuria, mass effect or obstruction. Answers C and D are incorrect because while it may occur, this is exceedingly rare. Answer E is incorrect because the size and quantity of cysts increases with age; however, the most rapid proliferation occurs under 40.
Comment Here
Reference: Benign renal cysts
Comment Here
Reference: Benign renal cysts
Board review style question #2
Epithelial cells of a simple renal cyst stain positively with which of the following immunohistochemical stains?
- CAIX (membranous) and CD10 (membranous)
- CD117 (cytoplasmic) and PAX8 (nuclear)
- PAX8 (nuclear) and CK7 (membranous)
- PAX8 (nuclear) and CK20 (membranous)
- Vimentin (nuclear and membranous)
Board review style answer #2
C. PAX8 (nuclear) and CK7 (membranous). No other combination correctly identifies the stain and pattern.
Comment Here
Reference: Benign renal cysts
Comment Here
Reference: Benign renal cysts
