Penis & scrotum
Squamous cell carcinoma and variants
Squamous cell carcinoma-general

Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Squamous cell carcinoma[TI] penis[TI] free full text[sb]
See also: Specific variants described separately
- Malignant epithelial tumor composed of squamous cells; diagnosis often delayed (eMedicine: Urogenital Squamous Cell Carcinoma [Accessed 4 April 2018])
- Squamous cell carcinoma, NOS: not otherwise specified (i.e., usual histologic pattern); represents 48 - 65% of all penile squamous cell carcinomas (Anal Quant Cytol Histol 2007;29:185)
- Pseudoglandular growth: unusual and aggressive variant of penile carcinoma with pseudoglands, often filled with amorphous material
- Squamous cell carcinoma, NOS is also called usual, typical, conventional, classical or epidermoid squamous cell carcinoma
- Pseudoglandular growth: also called adenoid or acantholytic carcinoma
- Most penile neoplasms are squamous cell carcinoma
- Rare in U.S.; < 1% of carcinomas in men versus 10 - 20% in Asia (excluding Japan), Africa and South America (Cancer 2008;113:2883)
- Usually age 40 - 70 years, median age 58 years
- Incidence is 0.29 per 100,000 in U.S. whites versus 4.2 per 100,000 in Paraguay versus 4.4 per 100,000 in Uganda
- Rare if circumcision at birth, more common if late circumcision (after age 10)
- More prevalent in populations with lower education and higher poverty (Cancer 2008;113:2910)
- More common in Hispanic and black men
- Familial cases have occasionally been reported
- Patients from high risk areas tend to be younger and present with a higher stage disease
- Rarely associated with genital piercing (J Sex Med 2010;7:2280)
- In squamous cell carcinoma, NOS, mean age is 58 years
- In pseudoglandular growth, average age is 54 years
- Phimosis and long foreskin, paraphimosis (Am J Surg Pathol 2003;27:994)
- Genital warts (6 times increased risk) (J Natl Cancer Inst 1993;85:19)
- Also HPV infection in general, particularly HPV 16 and related risk factors (Cancer Epidemiol Biomarkers Prev 2008;17:2683)
- ~33% of non-HPV cases are associated with lichen sclerosus (balanitis xerotica obliterans) (Am J Surg Pathol 2003;27:1448)
- Penile injury, tears and chronic balanitis
- Smoking, psoriasis patients treated with UVB radiation, penile rash > 1 month, immunosuppression and radiation therapy
- Most tumors arise from glans or inner foreskin near coronal sulcus as a slow growing, irregular mass
- In high incidence areas, tumors involve multiple anatomical compartments in up to 50% of cases
- In squamous cell carcinoma, NOS, glans is the preferred site but extension to coronal sulcus and inner foreskin is common
- In pseudoglandular growth, glans, coronal sulcus and inner foreskin are usually involved
- In squamous cell carcinoma, NOS, 25% of cases are HPV+ (Am J Surg Pathol 2010;34:104)
AFIP images

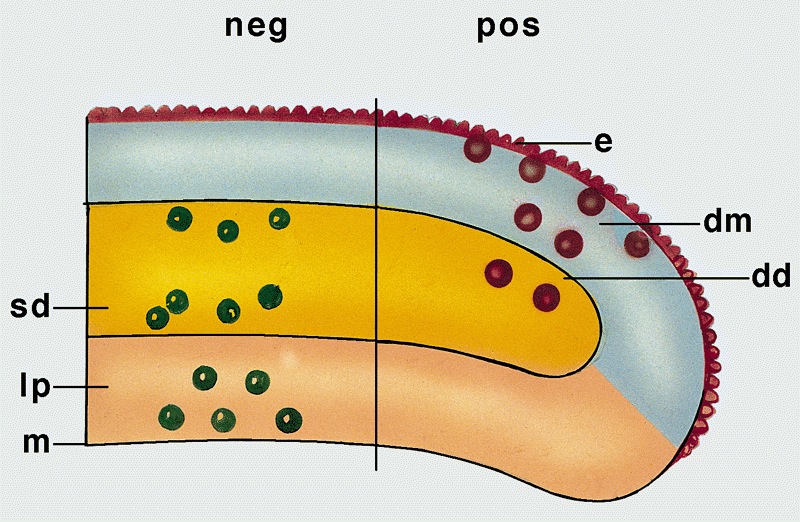
Schematic representation of effect of anatomic depth of invasion on risk of lymph node metastasis in carcinoma

Possible sites of
resection margin
involvement at time
of frozen section
Verruciform lesions
Frozen section evaluation of surgical margins
- Patients occasionally present with inguinal nodal metastases with occult penile cancer due to severe phimosis or very small primary tumor
- Local recurrence in 33% is due to insufficient surgery or positive margins, which also increases risk of regional inguinal and pelvic nodal metastases
- 10 year survival rate of 82% (J Urol 2009;182:528)
- Histologic subtypes have similar frequency in Paraguay and U.S. (Int J Surg Pathol 2010;18:268)
- Metastases:
- 5% have metastases at diagnosis
- Common sites are inguinal and pelvic lymph nodes, liver, lung, heart or bone (Int J Surg Pathol 2011;19:164)
- Nodes are often enlarged at clinical presentation due to infection, not metastases
- 5 year survival is related to nodal involvement: 66% (not involved) versus 27% (involved)
- Low grade:
- Usually no regional metastases if only superficial invasion of ≤ 6 mm (Mod Pathol 2001;14:963)
- High grade:
- Deep invasion (8 - 10 mm) into corpus spongiosum, dartos or corpora cavernosa is associated with 80% rate of metastases
- Intermediate / high grade with invasion of 5 - 10 mm have 15% risk of metastases
- Squamous cell carcinoma, NOS:
- Inguinal nodal metastases in 28 - 39% and recurrences in 28% of all cases
- Intermediate mortality rate (20 - 38%)
- Pseudoglandular growth has a higher metastatic rate and cancer related deaths when compared with usual SCC
- Poor prognostic factors:
- High stage
- High histologic grade (Am J Surg Pathol 2008;32:974, J Surg Oncol 2008;97:487)
- Deeper invasion (anatomic levels are epithelium, lamina propria, corpus spongiosum and corpus cavernosum) but anatomic variations exist (corpus cavernosum may not be located in glans in 25% of cases) (Am J Surg Pathol 2001;25:1091)
- Angiolymphatic invasion (J Urol 2008;180:1354)
- Perineural invasion (World J Urol 2009;27:169)
- Anaplastic, basaloid, pseudoglandular, sarcomatoid or solid subtypes
- Lymph node density in one study (J Urol 2009;182:2721)
- Prognostic index score:
- Combines histologic grade, anatomical level of tumor infiltration and perineural invasion to predict the likelihood of inguinal nodal involvement (Am J Surg Pathol 2009;33:1049)
- Useful for risk group stratification and clinical management
- Appropriate for surgical specimens, not for biopsies
- Score is sum of points for histologic grade (grade 1: 1, grade 2: 2, grade 3: 3), anatomical level of maximum tumor infiltration (lamina propria: 1, corpus spongiosum / dartos: 2, corpus cavernosum / preputial skin: 3) and perineural invasion (absent: 0, present: 1)
- Low risk: score of 2 - 3, intermediate risk: score of 4, high risk: score of 5 - 7
- 66 year old man with metastatic disease in pleural effusion (Arch Pathol Lab Med 1992;116:198)
- Series of 7 cases where patients presented with predominant pseudoglandular or adenoid features (Am J Surg Pathol 2009;33:551)
- Local resection, partial / total penectomy (NIH: Skin Cancer Treatment [Accessed 4 April 2018])
- Local excision and partial penectomy are inadequate for sarcomatoid and basaloid carcinomas (Am J Surg Pathol 2009;33:1299); poor outcomes with metastatic disease (Ann Surg Oncol 2007;14:3614)
- Higher risk for recurrence if node positive or partial penectomy (Eur Urol 2008;54:161)
- Possibly brachytherapy for tumors confined to glans (Int J Radiat Oncol Biol Phys 2009;74:1150)
- Criteria for inguinal lymphadenopathy are controversial, as palpable nodes may be reactive (Can Urol Assoc J 2008;2:525)
- Patients with prognostic index scores of 2 - 3 may not need inguinal nodal dissection
- Patients with prognostic index scores of 5 - 7 may benefit from prophylactic groin dissection
Contributed by Stewart F. Cramer, M.D. and AFIP images

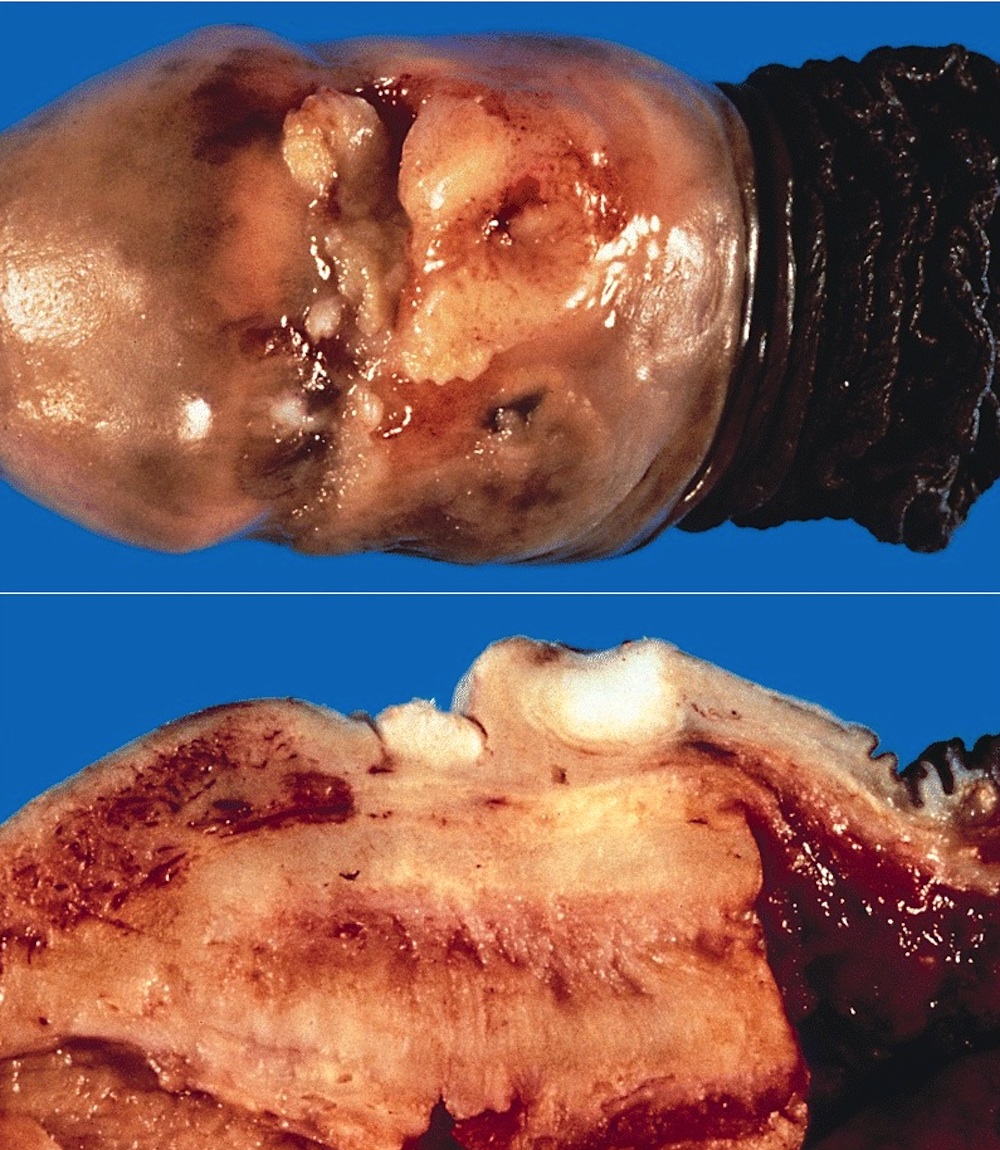
Large bosselated mass
Tumor at junction of scrotum and penis
Images hosted on other servers:

Arising on genital lichen sclerosus

Papillary SCC

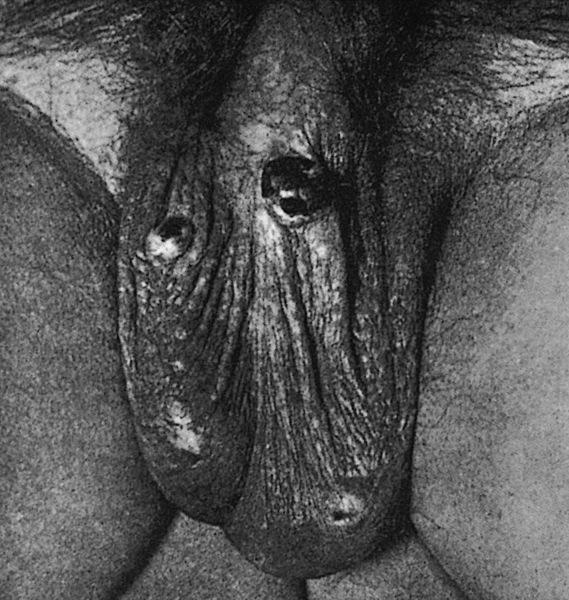
Ulcerated SCC on glans



Verrucous carcinoma
- Grossly noted growth patterns may have prognostic implications (Am J Surg Pathol 1993;17:753, World J Urol 2009;27:169)
- Superficial spreading: tumors are limited to lamina propria or superficial corpus spongiosum and usually extend horizontally through multiple anatomical compartments
- Vertical growth: tumors invade deep anatomical levels, surface is nonverruciform and frequently ulcerated
- Verruciform: tumors are exophytic and papillomatous with a cauliflower-like aspect, may be limited to surface (verrucous) or invade deep anatomical levels (cuniculatum)
- Mixed patterns: observed in 10 - 15% of all cases
- In some cases, multicentric tumors (2 or more independent foci of carcinomas) are identified
- Squamous cell carcinoma, NOS:
- Predominant growth patterns are vertical and superficial spreading
- Gross aspect is nondistinctive and variable
- Mean tumor size varies from 2 cm in low incidence areas to 4 - 5 cm in high incidence areas
- Cut surface shows tan-white solid irregular tumor with superficial or deep penetration
- Pseudoglandular growth:
- Large, irregular white-gray ulcerative or exophytic masses
- Frequent invasion of deep erectile tissues
- Average size is 4.6 cm
AFIP images
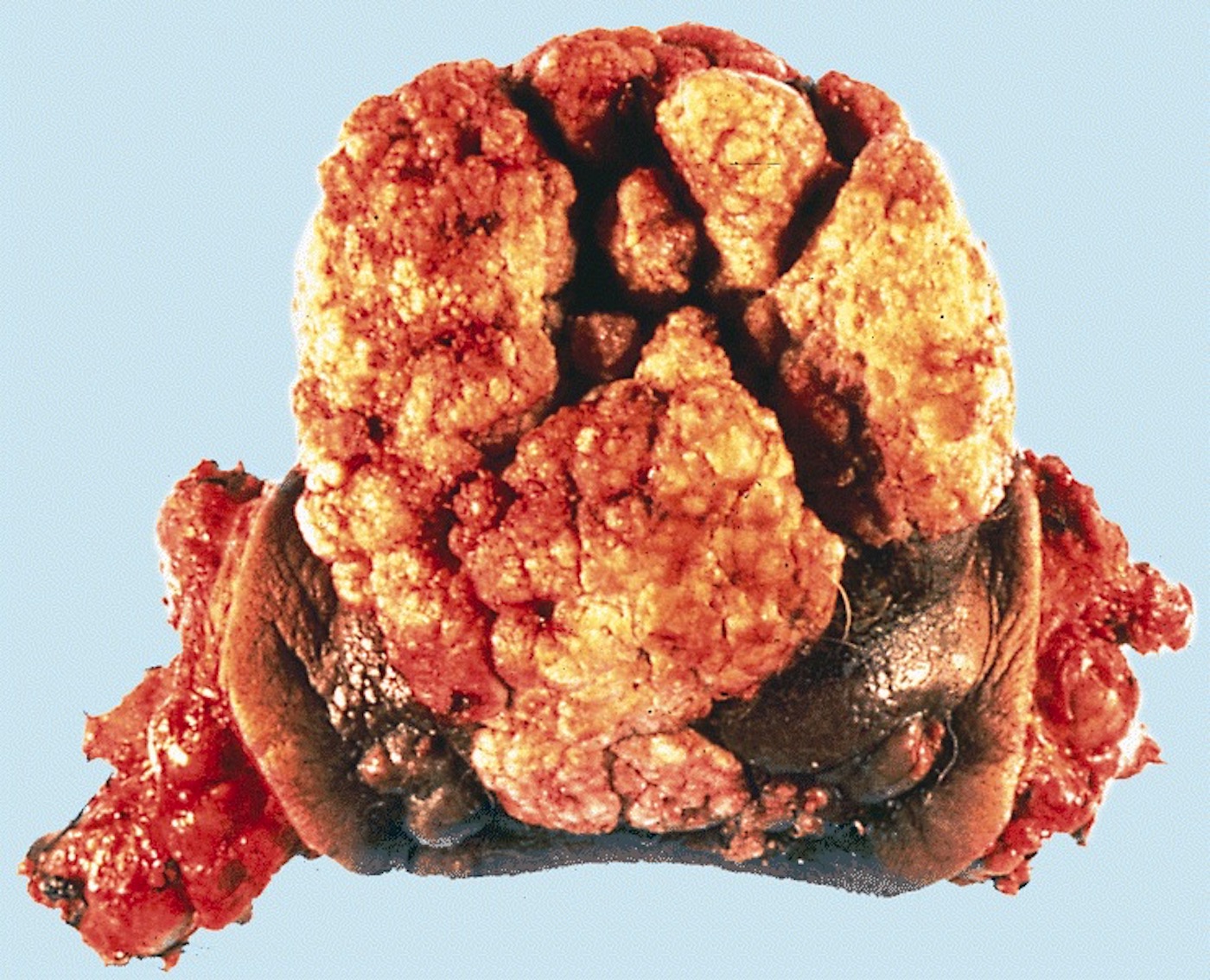
Glans:

Exophytic cauliflower-like mass

Glans extensively
involved by a
multinodular mass
with focal ulceration
Foreskin:

Circumcision
specimen shows a
flat, granular and
beige neoplasm

Massive involvement
has caused multiple
foci of ulceration
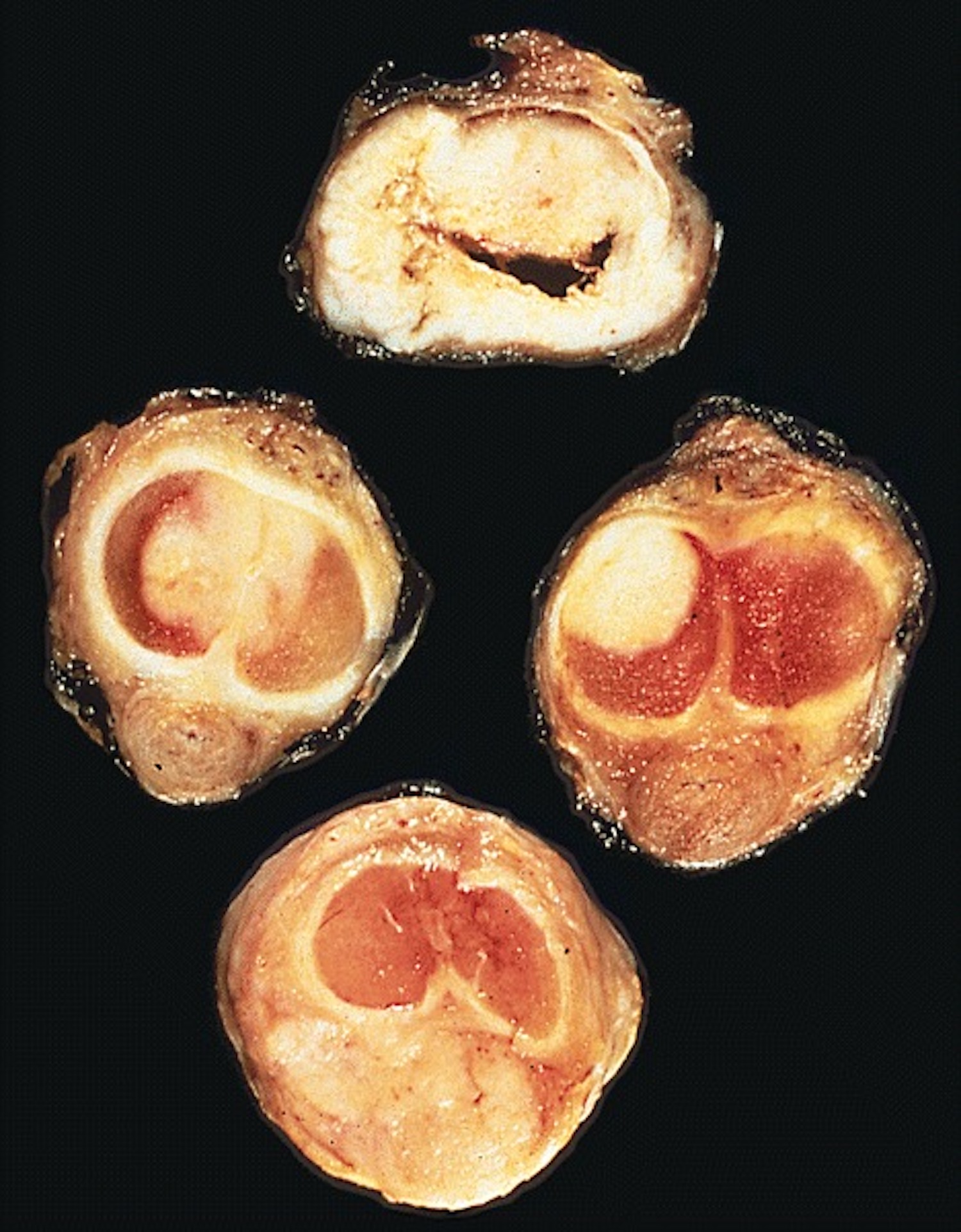
Coronal sulcus:
Nodular white
tumor extensively
involves the sulcus
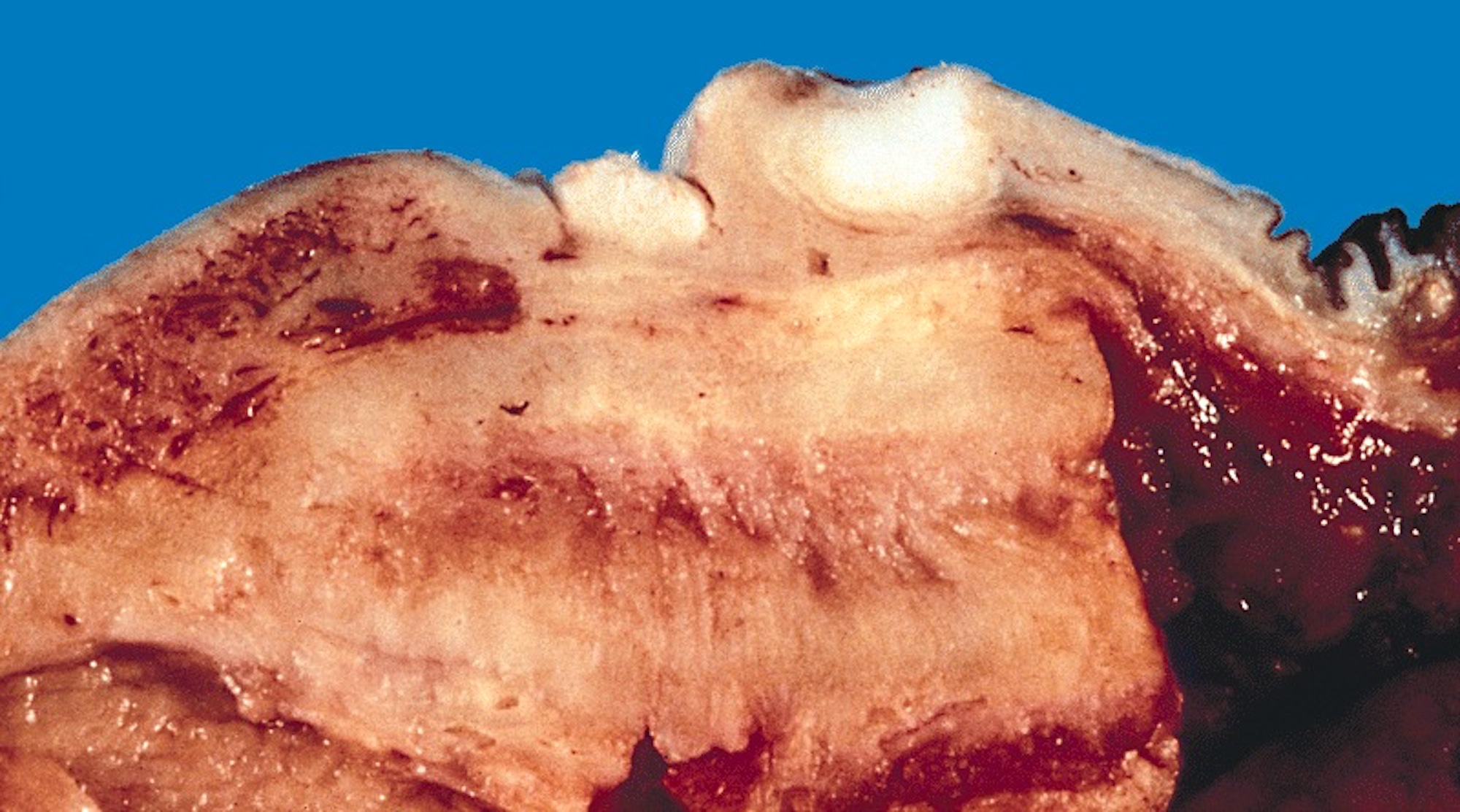
Cut section
shows 2
discrete nodules
of tumor
Verruciform lesions:
Verrucous
carcinoma
Cobblestone:

Cobblestone appearance representing condyloma
Multiple compartments:
Massive involvement
of glans, coronal
sulcus and foreskin

Massive involvement
has resulted in
autoamputation

4 separate
foci of
carcinoma
are present
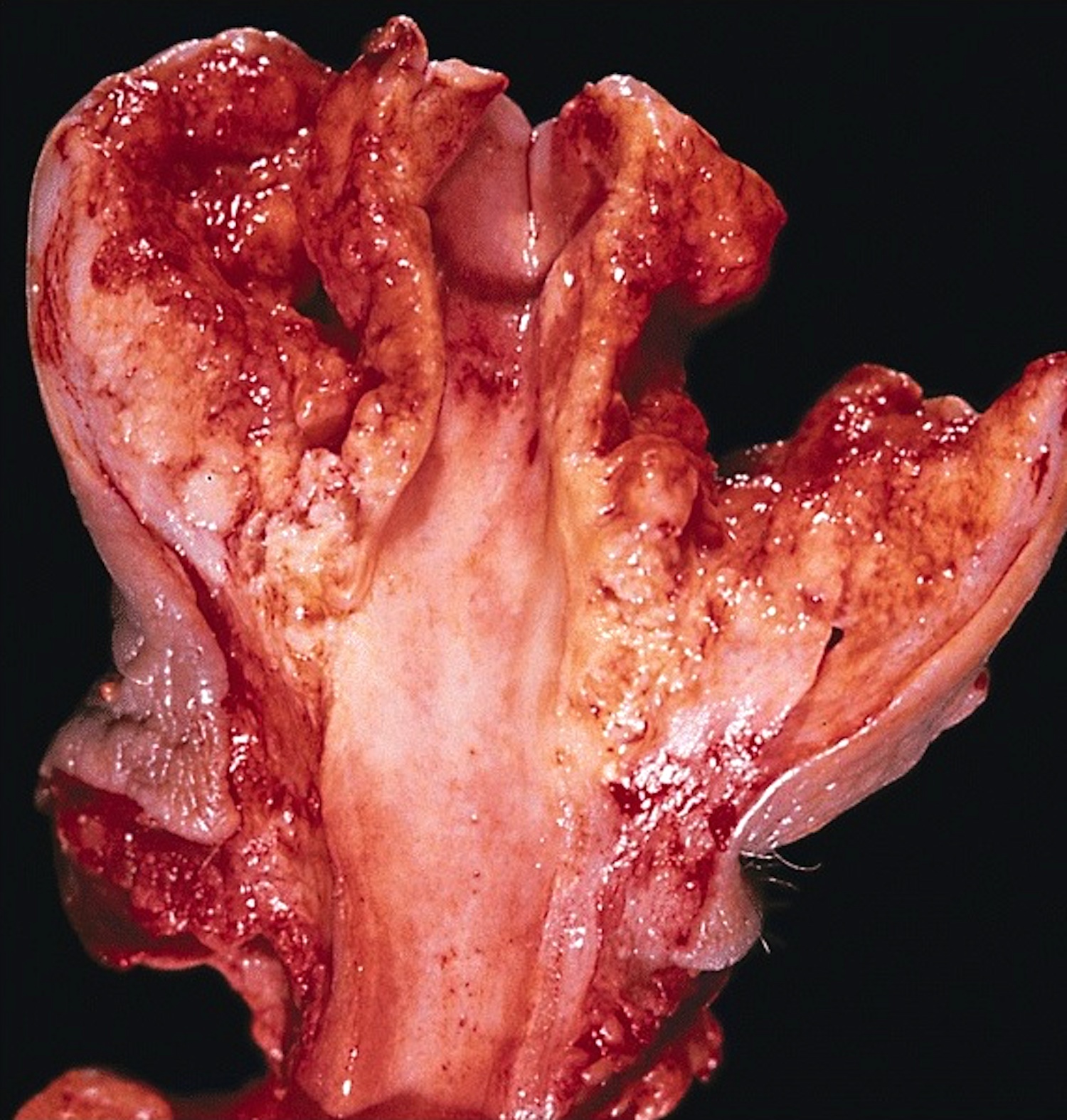
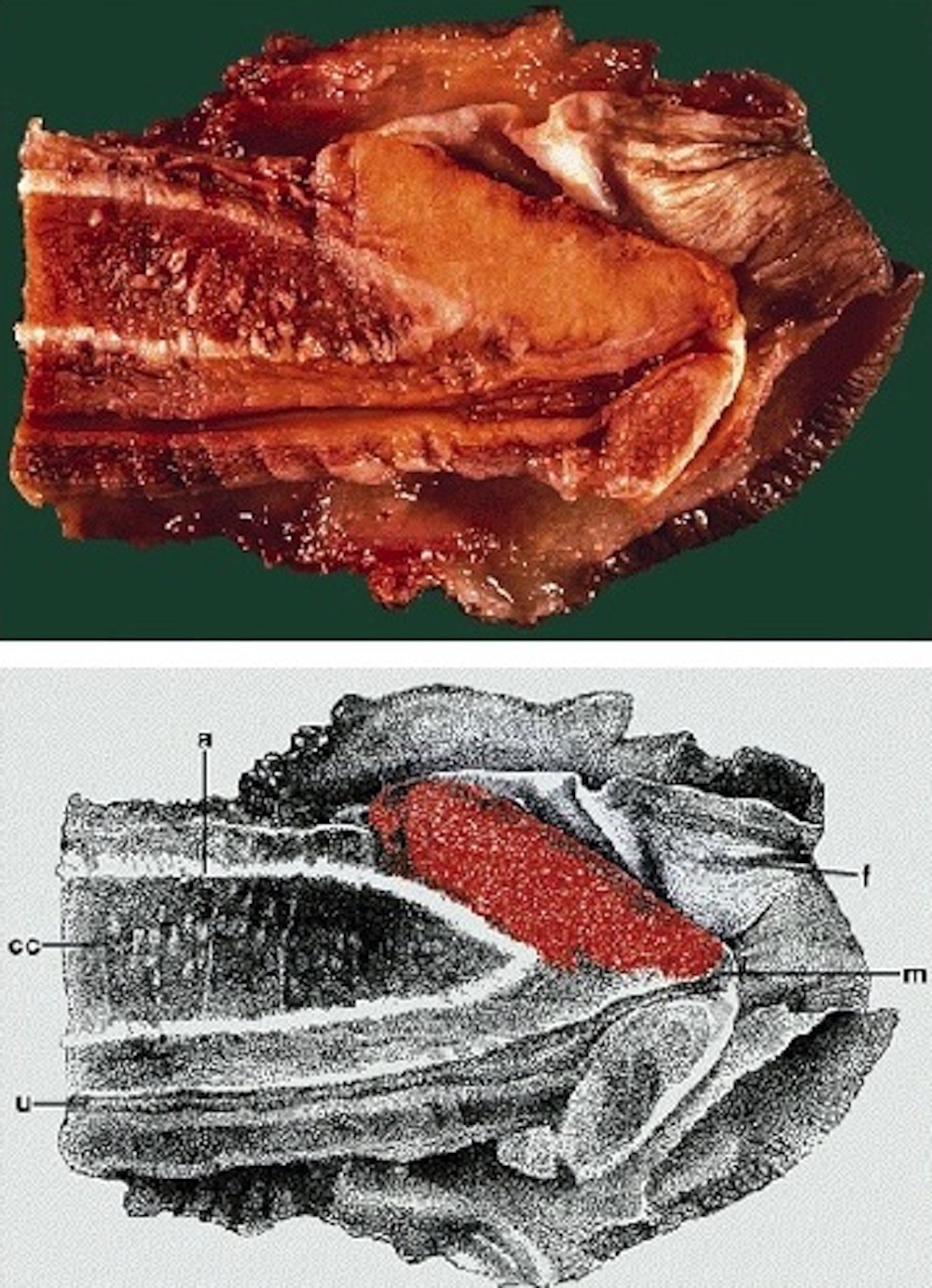
Superficial spreading (SCC):

Tumor involves
the glans with
extension to
coronal sulcus
Tumor is white,
involves the mucosa
of the foreskin
and coronal sulcus
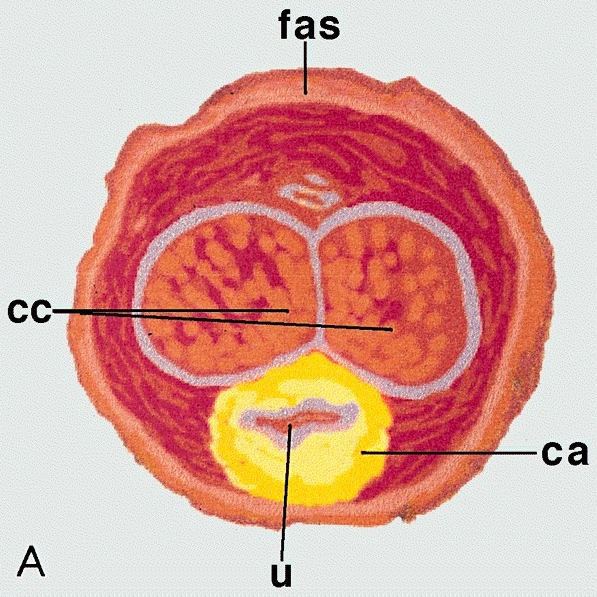
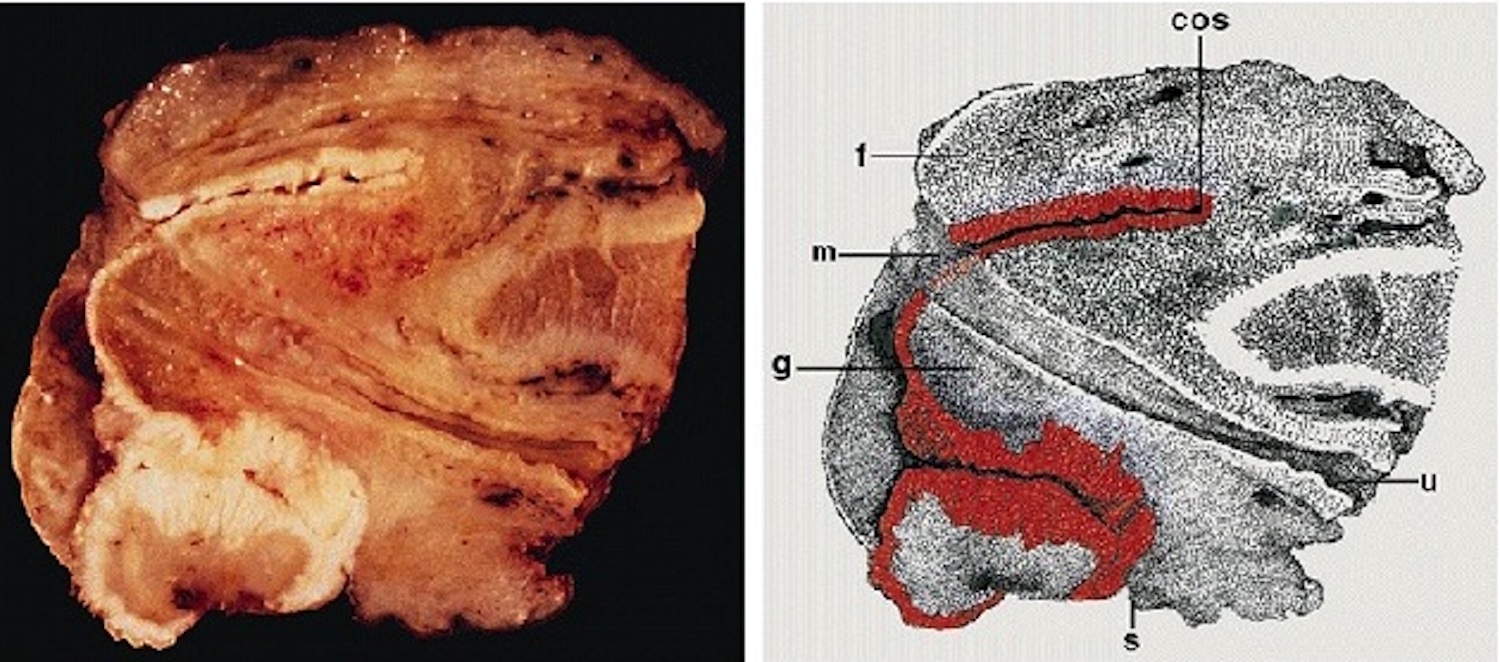
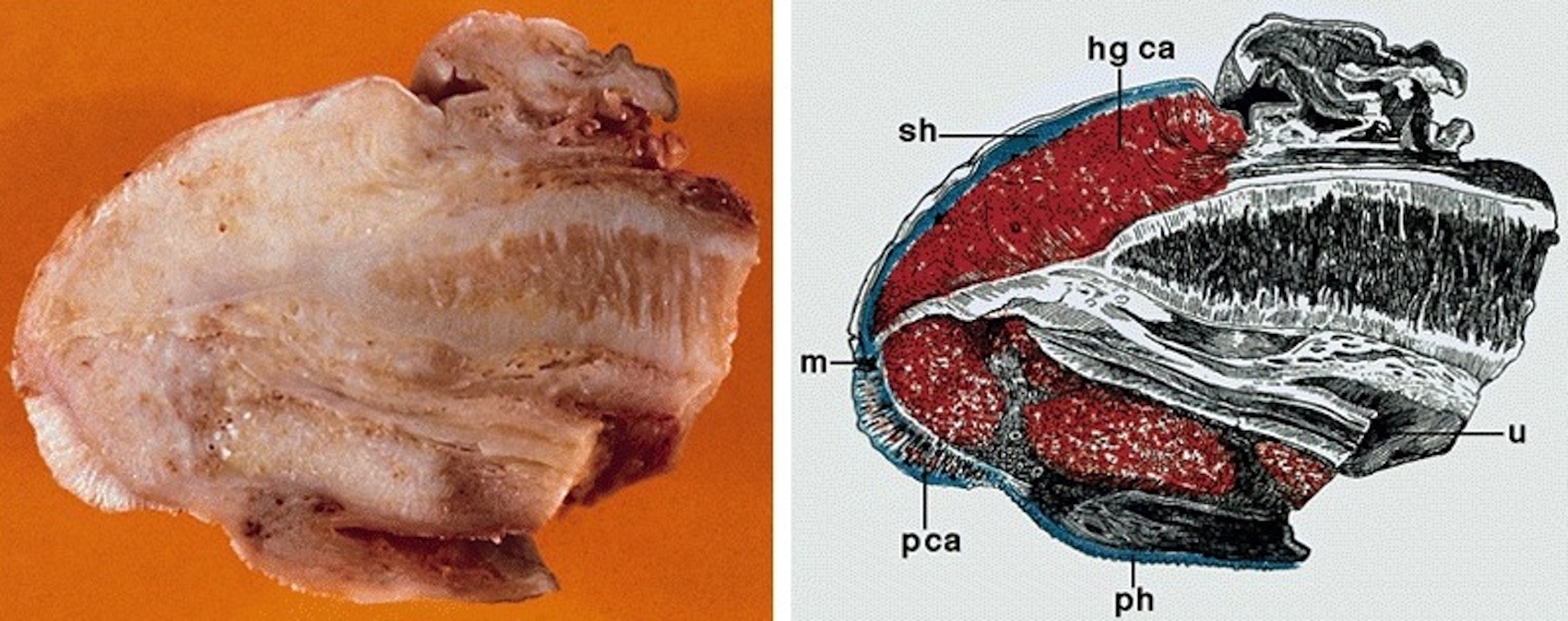
Assessment of depth of invasion:
Penile carcinoma has
been transversely
sectioned
Assessment of
depth of invasion
of tumor in
resected specimen
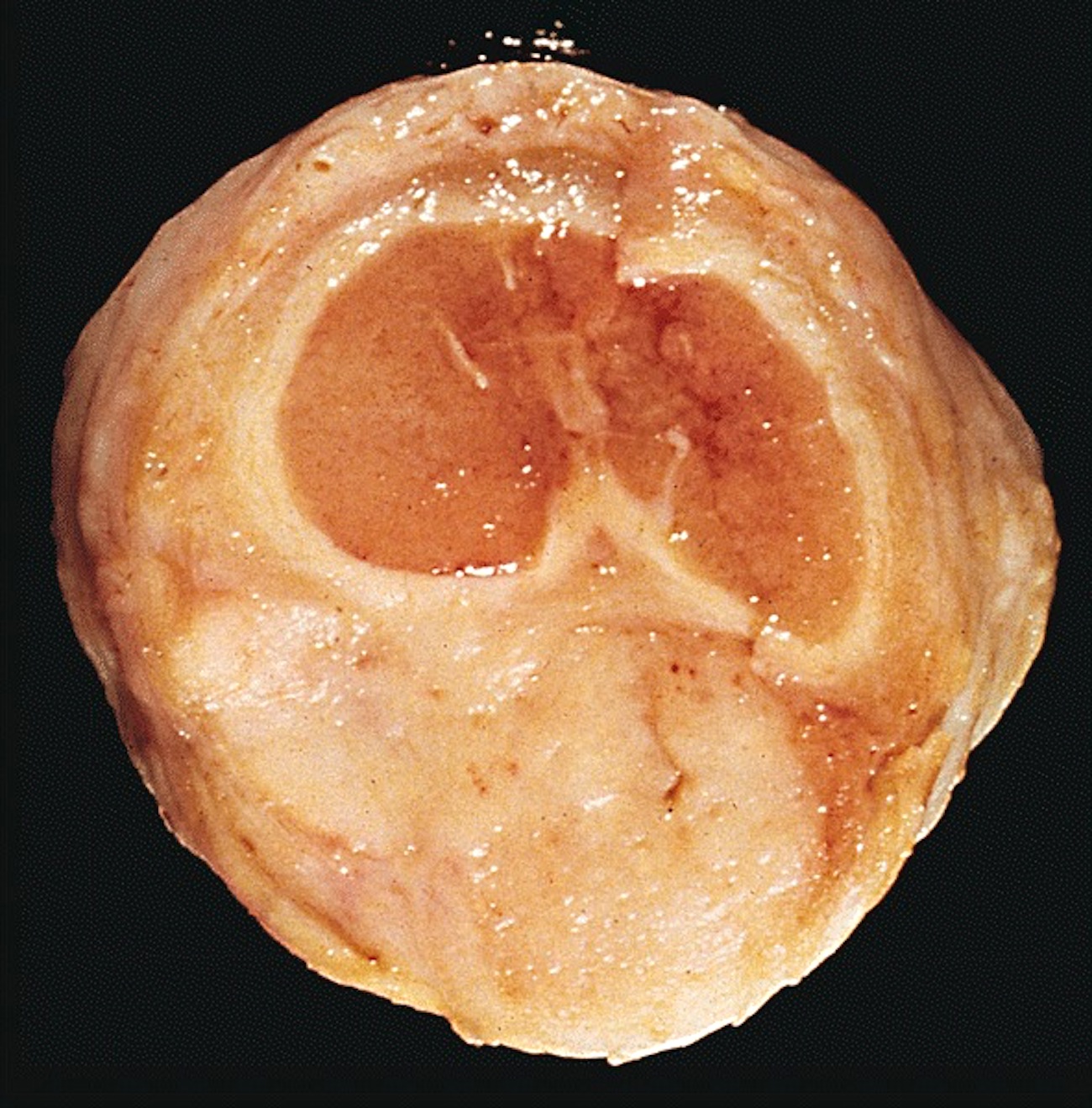
Vertical growth (SCC):
Solid yellow-tan
neoplasm in
the dorsal half
of the glans
Mixed low and high grade (SCC):
Neoplasm shows
superficial, white,
serrated papillary
Margin involvement:

Frozen section evaluation of surgical margins
Images hosted on other servers:

Red-tan ulcerated tumor

Fungating mass
- Most histologic subtypes resemble those in vulva, anus or buccal mucosa
- 48 - 65% are usual squamous cell carcinoma
- Verruciform tumors are verrucous, warty, papillary or cuniculatum carcinomas
- Basaloid and sarcomatoid carcinomas usually have a vertical growth pattern
- Often undifferentiated (bowenoid) penile intraepithelial neoplasia and lichen sclerosis (J Am Acad Dermatol 2010;62:284)
- Features to report: depth of invasion measured from deepest malignant cells to highest overlying dermal papilla; resection margins
- Grading:
- Grade 1: well differentiated cells, almost undistinguishable from normal squamous cells except for the presence of minimal basal / parabasal cell atypia
- Grade 2: all tumors not fitting into criteria for grade 1 or 3 (Am J Surg Pathol 2009;33:1042)
- Grade 3: any anaplastic cells
- Squamous cell carcinoma, NOS:
- Usually keratinized with moderate differentiation
- Up to 50% of cases are heterogeneous (> 1 histological grade)
- Most cases have differentiated penile intraepithelial neoplasia and squamous hyperplasia
- Tumors composed exclusively of extremely well differentiated or poorly differentiated areas are uncommon
- In some cases, clear glycogenated cells may predominate (but must differentiate from koilocytes)
- Stroma has variable lymphoplasmacytic infiltrate
- Foreign body type giant cells are often seen in highly keratinized tumors
- Pseudoglandular growth:
- Hallmark is the pseudogland: open space lined by atypical, cubical or cylindrical uni or multistratified cells
- Pseudoglands frequently filled with amorphous material containing debris, keratin and desquamated cells
- Intraluminal neutrophilic microabscesses are not uncommon
- Frequent presence of intracytoplasmic clear vacuoles, sometimes with a collaret arrangement
- Variegated tumor aspect showing solid areas intermingled with pseudoglandular spaces
- Frequent vascular and perineural invasion
Contributed by Antonio L. Cubilla, M.D., Alcides Chaux, M.D. and AFIP images

Scrotum: well, moderately and poorly differentiated tumors
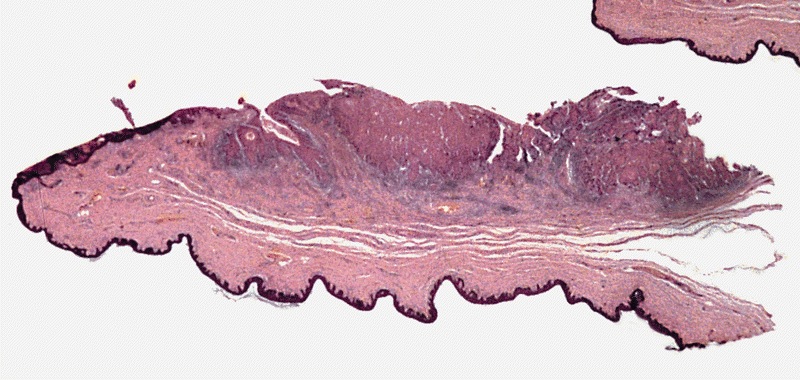
Mucosa is involved by carcinoma
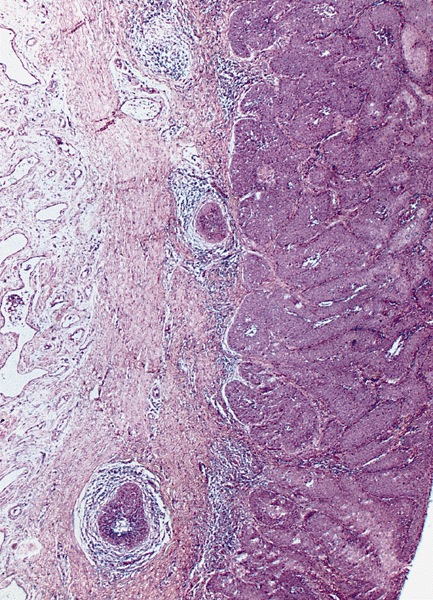
Invasion of the lamina propria
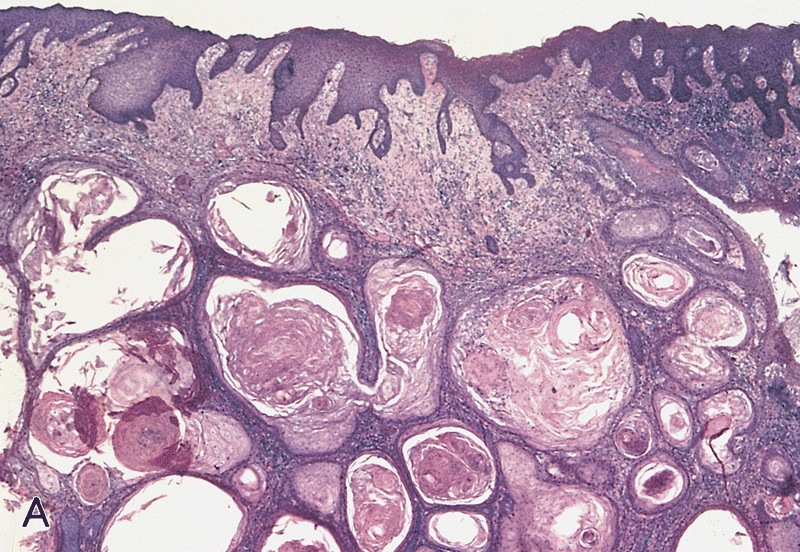
Mixed (hybrid) usual: verrucous carcinoma
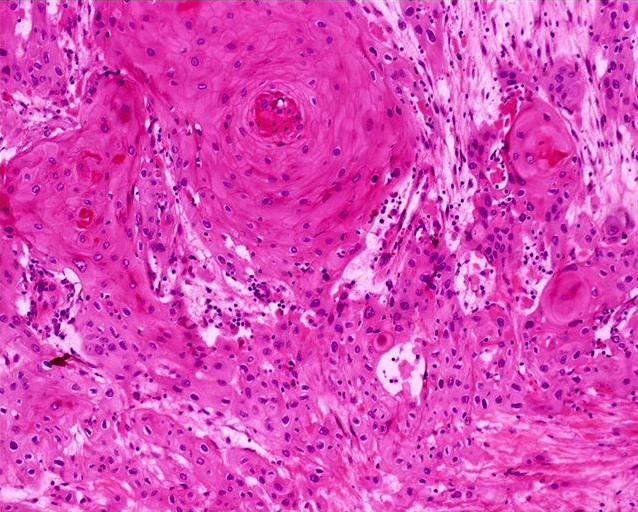
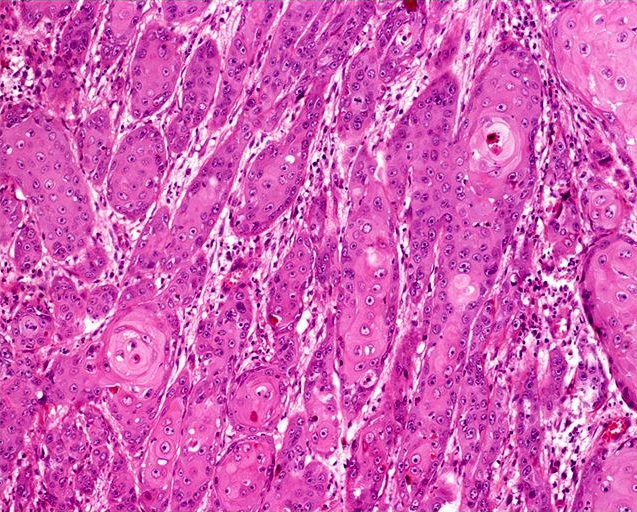
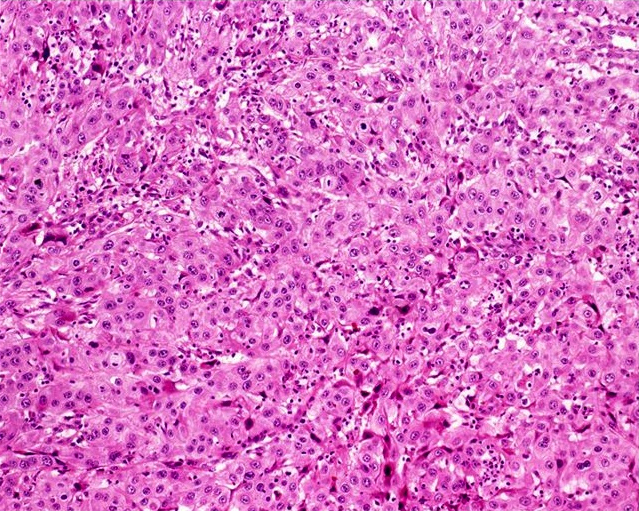
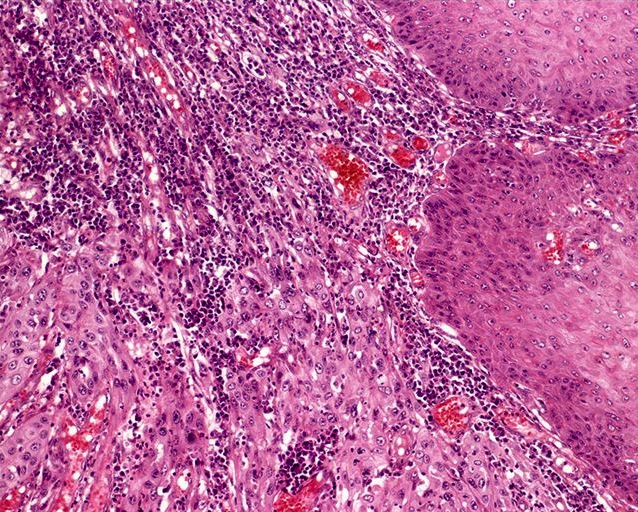
Usual type: well differentiated (left, grade 1); moderately differentiated (middle, grade 2); poorly differentiated (right, grade 3)
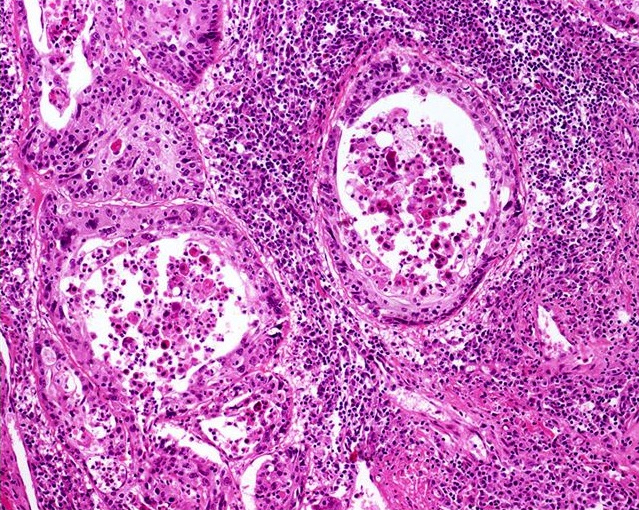
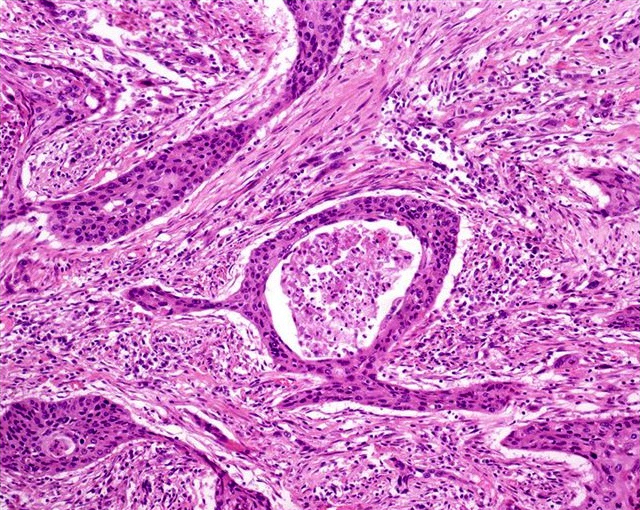
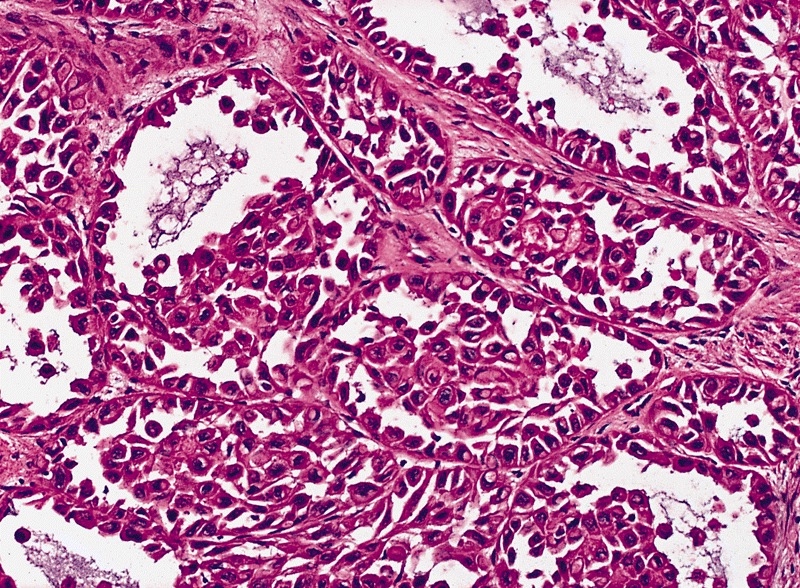
Pseudoglandular growth
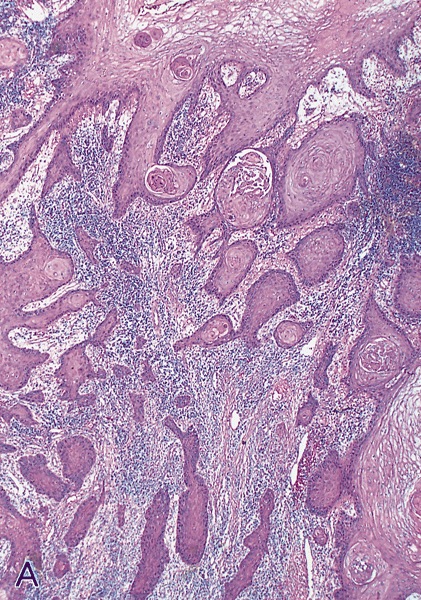
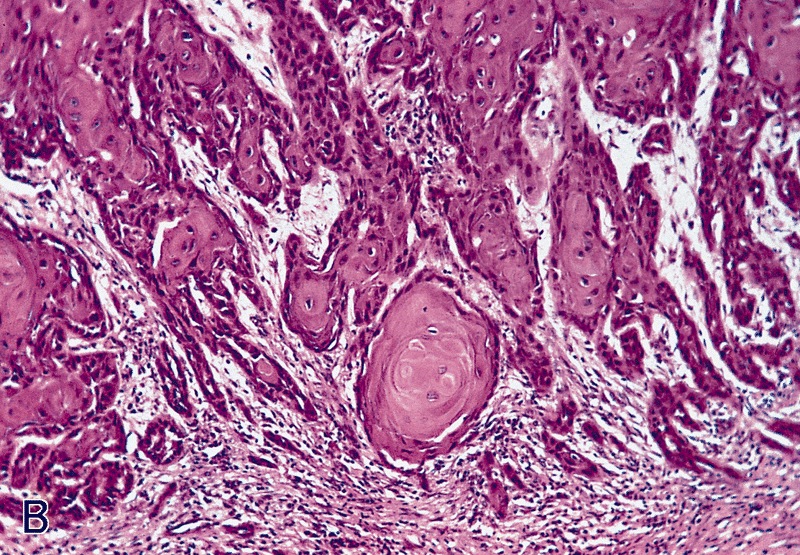
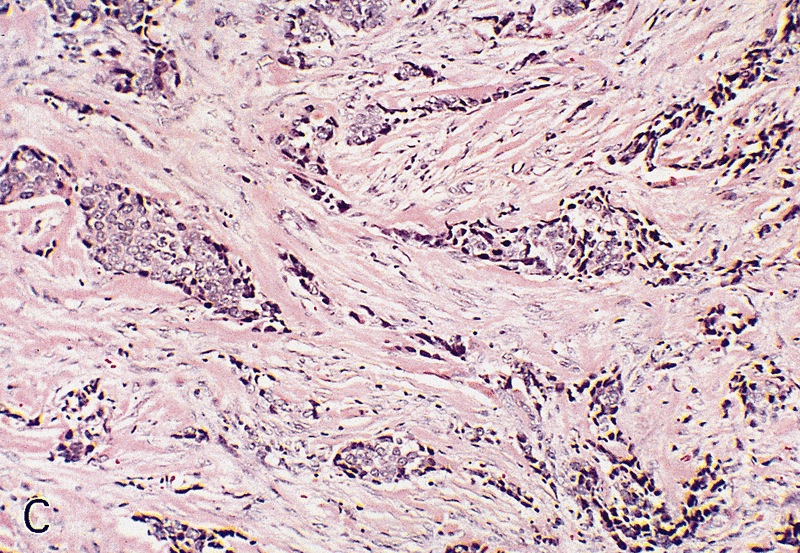
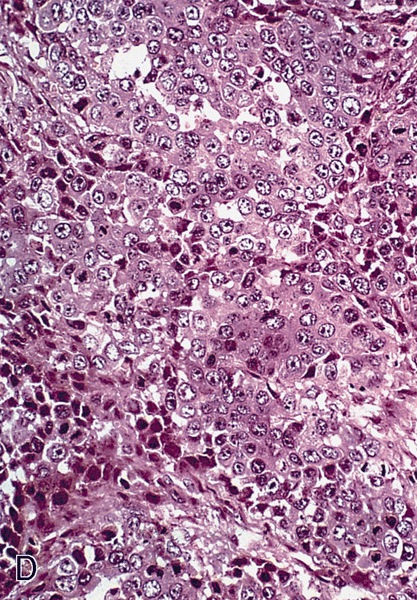
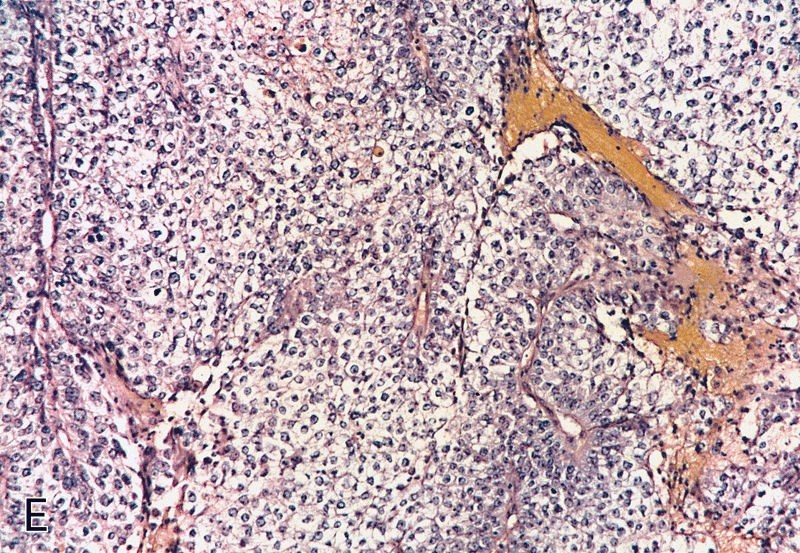
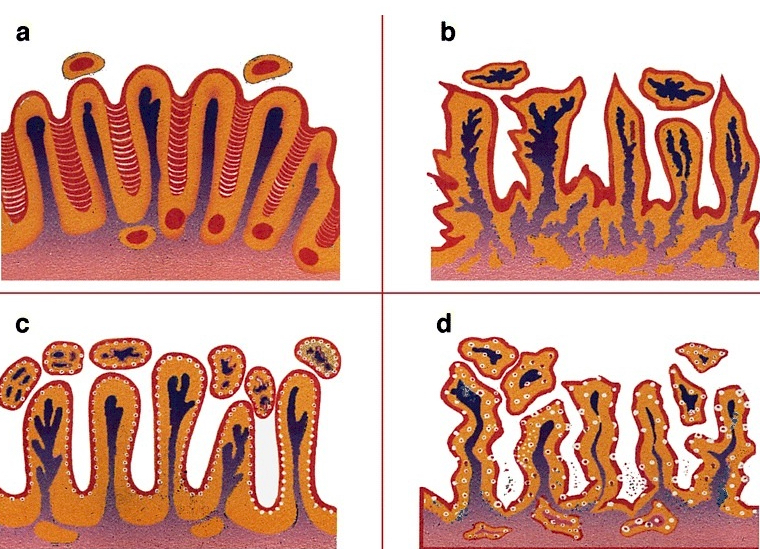
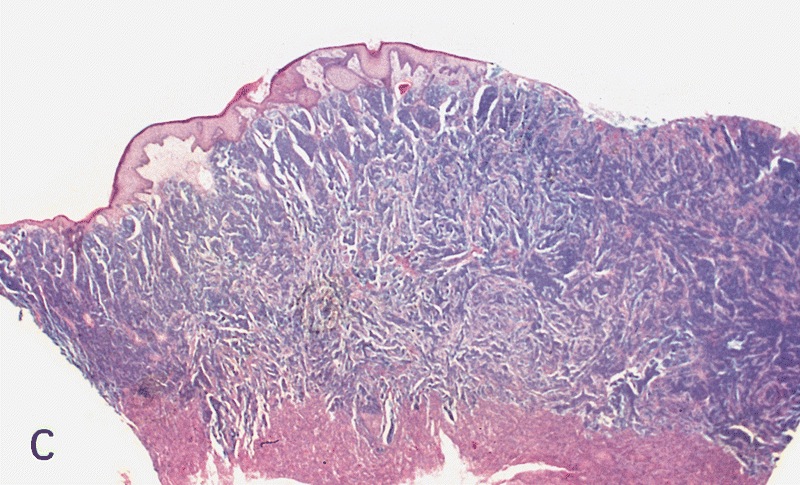
Low grade keratinizing (A, B); moderate to high grade nonkeratinizing (C); high grade nonkeratinizing tumor (D); and carcinoma with prominent glycogenated clear cells (E)
Images hosted on other servers:
Pseudoglandular growth:

Conjunctiva: acantholysis of neoplastic squamous cells


Head and neck: pseudolumina are present but no true glands
- Negative staining in pseudoglandular variant for factor VIII, PAS and Alcian blue
- Mutations in PIK3CA, HRAS or KRAS genes in 39% (J Urol 2008;179:2030)
- Epigenetic silencing (by methylation) of FHIT gene in 92% (Virchows Arch 2008;452:377)
- Squamous cell carcinoma, NOS:
- Basaloid carcinoma:
- Basophilic cytoplasm, indistinctive cellular borders and mostly HPV+
- Clear cell carcinoma:
- Pseudoepitheliomatous hyperplasia:
- Elongated rete ridges, no nuclear atypia, regular epithelial nests with evident peripheral palisading and no stromal reaction
- Urothelial carcinoma:
- Ventral surface of penis, absence of squamous metaplasia, microglandular hyperplasia, lichen sclerosus or penile intraepithelial neoplasia, presence of urothelial carcinoma in situ or history of urothelial CIS or bladder tumor
- Basaloid carcinoma:
- Pseudoglandular growth:
- Adenocarcinoma of Littré glands:
- True glandular differentiation, ventrally located with secondary extension to perimeatal area
- Adenosquamous carcinoma:
- Pseudoangiosarcomatoid variant of sarcomatoid carcinoma:
- Urothelial carcinoma of distal urethra with glandular features:
- Previous / concurrent history of urothelial carcinoma elsewhere and presence of urothelial carcinoma in situ
- Positive for urothelial markers (uroplakin III, thrombomodulin)
- Adenocarcinoma of Littré glands:
