Skin nontumor
Infectious disorders
Tinea versicolor
Deputy Editor-in-Chief: Jonathan D. Ho, M.B.B.S., D.Sc.

Last author update: 27 September 2024
Last staff update: 4 December 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Tinea versicolor
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Videos | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2 | Practice question #3 | Practice answer #3Cite this page: Pybus A, Logemann NF. Tinea versicolor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorfungitineaversicolor.html. Accessed August 25th, 2025.
Definition / general
- Superficial skin infection with commensal Malassezia species, a dimorphic fungus
Essential features
- Common superficial infection of the stratum corneum in sebaceous areas of skin with Malassezia species
- Budding yeast and hyphae (spaghetti and meatballs appearance) are seen on potassium hydroxide (KOH) preparation as well as on skin biopsy
- Topical imidazole antifungals are first line treatment and periodic maintenance therapy is recommended to prevent recurrence
Terminology
- Pityriasis versicolor
Epidemiology
- Seen commonly worldwide, with increased prevalence in tropical regions (Lancet 2004;364:1173)
- Any age group but more frequent in young adults (Clin Dermatol 2010;28:140)
- No sex predilection (Clin Dermatol 2010;28:140)
Sites
- Favors skin with high density of sebaceous glands, such as upper back, upper chest, shoulders and arms in adults (Lancet 2004;364:1173)
- Facial involvement is less common in adults but may be seen in children (Lancet 2004;364:1173)
Pathophysiology
- Infection is noncontagious; host factors, such as presence of certain free fatty acids and triglycerides, are theorized to result in conversion of normal flora Malassezia yeast forms to pathogenic mycelial forms (Lancet 2004;364:1173)
- Azelaic acid produced by the pathogenic fungus induces tyrosinase inhibition and melanosome alterations, resulting in pigmentary changes (Lancet 2004;364:1173)
Etiology
- Malassezia species are dimorphic lipophilic fungi that normally colonize the stratum corneum and hair follicles of human skin, particularly in areas rich with sebaceous lipids (Lancet 2004;364:1173)
- Malassezia globosa, Malassezia sympodialis and Malassezia furfur are the 3 species that cause most cases (Lancet 2004;364:1173)
Clinical features
- Numerous scattered and often coalescing macules, patches and thin plaques that may be pink, hypopigmented or hyperpigmented and can be mildly pruritic
- Fine scale can often be elicited by gently scraping the surface
- Atrophying tinea versicolor, an uncommon variant, presents with depressed or atrophic hypo or hyperpigmented macules and patches (Int J Dermatol 2003;42:928)
Diagnosis
- Clinical diagnosis is often sufficient but direct microscopy of lesional scale scrapings with KOH or chlorazol black preparation may assist with diagnosis
- Skin biopsy may be performed if the diagnosis is uncertain
Laboratory
- Fungal culture for Malassezia is not routinely performed in clinical practice
Prognostic factors
- Prognosis is excellent with appropriate treatment, though it may take months for pigmentary changes to resolve following adequate therapy
- Recurrence is extremely common and maintenance therapy is recommended
Case reports
- 3 month old boy with multiple hypopigmented macules on trunk (Cureus 2023;15:e40763)
- 7, 8 and 14 year old boys with hypopigmented macules on the scalp (Front Pediatr 2024;12:1361225)
- 52 year old man with psoriasis who developed hypopigmented and hyperpigmented scaly macules on trunk, arms and legs shortly after starting ixekizumab therapy (JAAD Case Rep 2021;18:54)
Treatment
- Topical imidazole antifungals (ketoconazole, fluconazole, itraconazole, clotrimazole) are first line (Lancet 2004;364:1173)
- Oral antifungals are a second line option for difficult cases (Lancet 2004;364:1173)
- Ketoconazole shampoo maintenance therapy is recommended once every 1 - 2 weeks following resolution of active infection to reduce recurrence risk (Lancet 2004;364:1173)
Clinical images
Images hosted on other servers:

Bilateral chest tinea versicolor

Left arm tinea versicolor
Microscopic (histologic) description
- Direct microscopy of lesional scale prepared with KOH or chlorazol black shows clusters of budding ovoid yeasts (blastoconidia) and hyphae (pseudomycelium) referred to as spaghetti and meatballs (Lancet 2004;364:1173)
- H&E of skin biopsy shows ovoid budding yeasts and hyphae (spaghetti and meatballs) within the stratum corneum (Lancet 2004;364:1173)
- Fungi are accentuated with periodic acid-Schiff (PAS) or Gomori methenamine silver (GMS) stains (Lancet 2004;364:1173)
- Other histologic changes are often subtle or absent; slight hyperkeratosis or sparse superficial perivascular inflammatory infiltrate may be present (Patterson: Weedon’s Skin Pathology, 5th Edition, 2020)
- Atrophying tinea versicolor may have dermal elastolysis visible with Verhoeff van Gieson staining (Int J Dermatol 2003;42:928)
Microscopic (histologic) images
Contributed by Alexander J. Pybus, M.D. and C. Lamar Hardy, M.D.
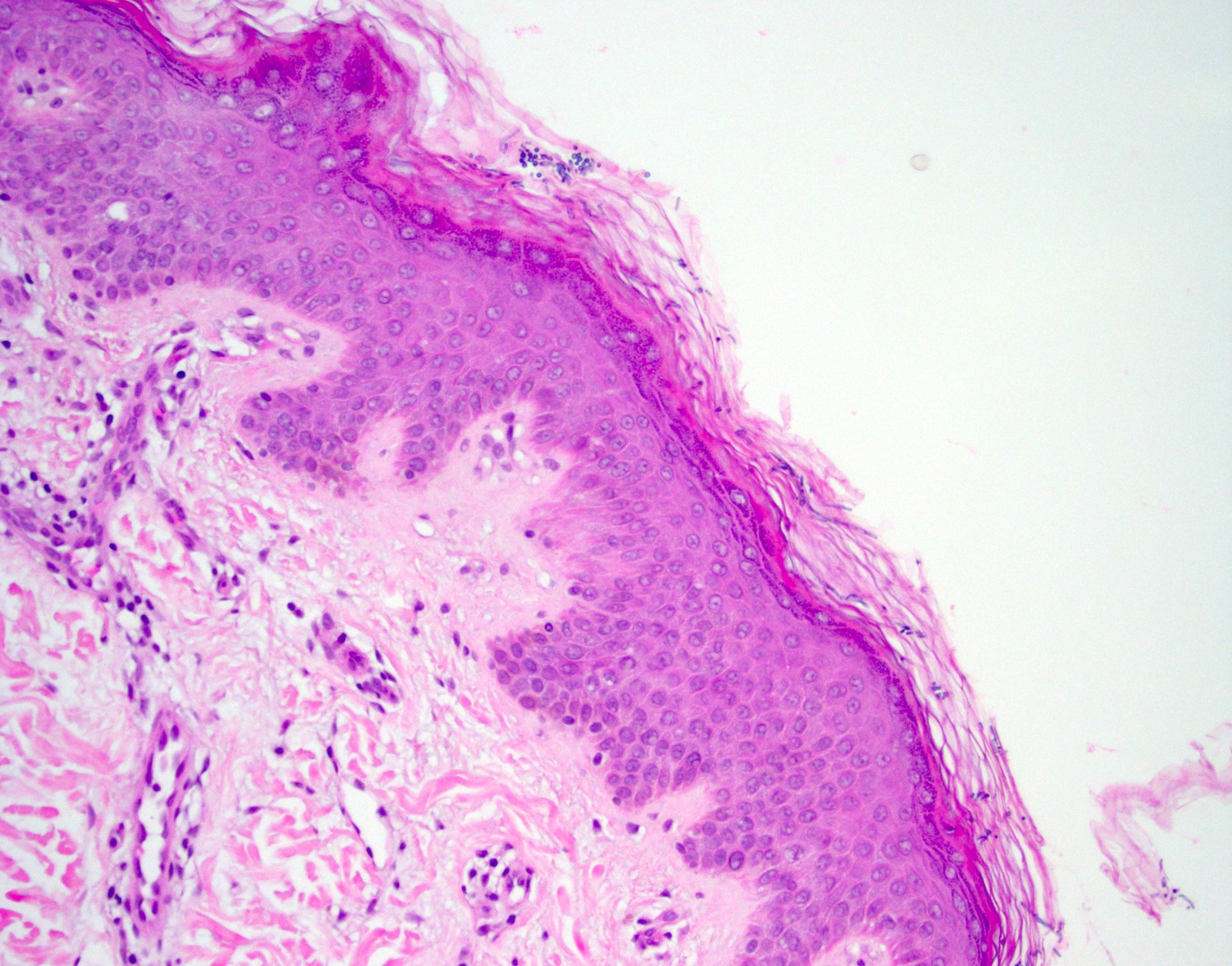


Stratum corneum fungal elements

Yeasts and hyphae


Stratum corneum fungal elements
Positive stains
- Malassezia in the stratum corneum
- Periodic acid-Schiff (PAS) (Lancet 2004;364:1173)
- Gomori methenamine silver (GMS) (Lancet 2004;364:1173)
- Alcian blue (Patterson: Weedon’s Skin Pathology, 5th Edition, 2020)
- Fontana-Masson (Patterson: Weedon’s Skin Pathology, 5th Edition, 2020)
- Congo red (Patterson: Weedon’s Skin Pathology, 5th Edition, 2020)
Videos
Tinea versicolor - Dr. Jerad Gardner
Sample pathology report
- Skin, shave biopsy:
- Tinea versicolor (see comment)
- Comment: Microscopic sections show ovoid yeasts and hyphae within the stratum corneum. These fungal organisms are accentuated with PAS and GMS staining, supporting the H&E impression. There is sparse superficial vascular inflammatory infiltrate and mild focal acanthosis of the epidermis.
Differential diagnosis
- Pityriasis rosea:
- Herald patch followed by eruption of pink, scaly patches and plaques in a Christmas tree distribution on the trunk
- Constitutional symptoms such as fever, headache, cough or arthralgia may precede the eruption
- Histologic findings include mounded parakeratosis, extravasated red blood cells and a spongiotic epidermis
- Secondary syphilis:
- Classically copper colored to dark brown scaling papules and plaques on the trunk weeks to months after an untreated syphilitic chancre (primary syphilis)
- Involvement of palms and soles can be seen along with moth eaten alopecia
- Histologic findings include long slender rete ridges as well as superficial and deep lymphoplasmacytic infiltrate
- Seborrheic dermatitis:
- Chronic recurrent pink, hypopigmented or hyperpigmented macules, patches and plaques with greasy scale
- Seborrheic areas of the scalp, face and upper chest
- Histologic changes show spongiotic dermatitis and overlying scale crust with few neutrophils
- Tinea corporis:
- Itchy annular erythematous plaques with peripheral scale
- Histology shows hyphae within the stratum corneum and may also show neutrophils in the stratum corneum
- Yeast forms would not be present on histology
- Vitiligo:
- Depigmented macules and patches without scale
- Accentuated with Wood's lamp examination but does not produce colored fluorescence
- Histology findings often resemble normal skin but reduced epidermal basilar pigmentation may be appreciated when compared to unaffected skin areas
Practice question #1

What is the correct diagnosis for the image shown above?
- Atopic dermatitis
- Seborrheic dermatitis
- Tinea versicolor
- Vitiligo
Practice answer #1
C. Tinea versicolor. The patient shown has scattered and coalescing hypopigmented macules and scaly patches on the back, clinically consistent with tinea versicolor. This is a benign superficial skin infection with Malassezia species dimorphic fungi, which normally colonize the skin and convert into pathogenic mycelial forms in the presence of certain host skin factors. Answer A is incorrect because atopic dermatitis most commonly presents as xerotic or lichenified scaly papules and plaques in flexural skin areas, such as the neck, antecubital fossae and popliteal fossae. Answer B is incorrect because seborrheic dermatitis tends to present as dandruff on the scalp or erythematous papules and plaques on the central face, brows, nose and upper chest with overlying greasy appearing scale. Answer D is incorrect because vitiligo would present as depigmented macules and patches of skin without any associated scale.
Comment Here
Reference: Tinea versicolor
Comment Here
Reference: Tinea versicolor
Practice question #2
What is the most appropriate first line treatment for the skin condition shown in the image above?
- Amphotericin B
- Clotrimazole
- Oral griseofulvin
- Oral terbinafine
Practice answer #2
B. Clotrimazole. This photomicrograph depicts ovoid budding yeasts and hyphae within the stratum corneum consistent with a diagnosis of tinea versicolor. The first line treatments for tinea versicolor are topical imidazole antifungals, such as clotrimazole or ketoconazole. Answer D is incorrect because oral terbinafine is a second line treatment to be reserved for patients who have not responded to topical therapy. Answers A and C are incorrect because amphotericin B and oral griseofulvin are not used to treat tinea versicolor.
Comment Here
Reference: Tinea versicolor
Comment Here
Reference: Tinea versicolor
Practice question #3
Practice answer #3
D. Malassezia globosa. This photomicrograph shows ovoid budding yeasts and hyphae within the stratum corneum consistent with a diagnosis of tinea versicolor. This condition is caused by dimorphic lipophilic yeasts of the genus Malassezia (formerly known as Pityrosporum), specifically M. globosa, M. furfur and M. sympodialis. Answer A is incorrect because Aspergillus fumigatus causes aspergillosis, which in the skin would present as 3 - 6 µm septate hyphae with right angle branching in the dermis or with angioinvasion of dermal blood vessels. Answer B is incorrect because Coccidioides immitis can be seen cutaneously in disseminated coccidioidomycosis as thick walled spherules (10 - 80 µm in diameter) within giant cells and granulomas in the dermis. Answer C is incorrect because Cryptococcus neoformans causes cryptococcosis, with 10 - 15% of cases presenting with cutaneous involvement, including disseminated involvement in immunocompromised patients, such as those with AIDS or organ transplant recipients. Histology of cryptococcosis would show dermal chronic inflammatory infiltrate with tuberculoid granulomas and few encapsulated yeast organisms (5 - 15 µm in diameter) or even large mucoid masses of encapsulated organisms in some cases.
Comment Here
Reference: Tinea versicolor
Comment Here
Reference: Tinea versicolor
