Soft tissue
Adipose tissue tumors
Liposarcoma
Myxoid liposarcoma


Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Myxoid liposarcoma
- Malignant tumor composed of primitive nonlipogenic mesenchymal cells, signet ring lipoblasts and prominent myxoid stroma with a highly characteristic branching vascular pattern
- Prominent myxoid stroma with branching vasculature (so called chicken wire vasculature)
- Majority of the tumor can be nonlipogenic with only scattered lipoblasts that often have a characteristic signet ring morphology
- Recurrent molecular alteration with either t(12;16)(q13;p11.2) FUS::DDIT3 or very rarely (~2%) t(12;22)(q13;q12) EWSR1::DDIT3 rearrangements
- Includes a spectrum of disease including high grade lesions, which were formerly regarded as round cell liposarcoma (see Terminology)
- Has an unusual propensity to present with a first metastasis to another soft tissue or bony site (such as from one leg to the contralateral leg or to the retroperitoneum or spine)
- Although myxoid liposarcoma and round cell liposarcoma were initially described separately, both tumors have identical molecular alterations and clear evidence of cases with transition between the 2 morphologic patterns are easily found
- Both tumors are now classified as myxoid liposarcoma with a secondary designation of high or low grade
- Percent of round cell component needed for this distinction is debated in the literature with most pathologists using either > 25% or > 5% indicating a high grade lesion
- WHO currently lists 5%
- Cases with borderline round cell component (< 5%) are regarded as having areas of transition, a designation of unclear diagnostic significance
- ICD-O: 8852/3 - myxoid liposarcoma
- ICD-11: 2B59.Y & XH3EL0 - liposarcoma, other specified primary site & myxoid liposarcoma
- Peaks in the fourth and fifth decades and represents ~5% of adult sarcomas (Int J Surg Oncol 2018;2018:8928706)
- M = F
- May occur in children or very rarely in the elderly
- Usually in the extremities, proximal thigh is quite common
- Primary retroperitoneal involvement is rare, although metastasis to the retroperitoneal soft tissue is not uncommon
- Propensity to present with multifocal disease, seemingly from hematogenous spread that has spared the lungs (J Surg Oncol 2002;80:89)
- Primary subcutaneous tumors have been reported (J Cutan Pathol 2014;41:907)
- Core needle biopsy is minimally invasive and can provide sufficient tissue sampling for definitive diagnosis, although it may not allow for accurate tumor grading due to sampling bias
- Surgical resection is the gold standard procedure for ensuring accurate diagnosis and prognostication
- Vague foci of fat in a lacy or linear pattern on MRI (Radiographics 2000;20:1007)
- May appear cystic on nonenhanced MRI, although they enhance like other solid masses, often as T1 hyperintense fatty septa (Radiographics 2000;20:1007, Radiol Case Rep 2017;12:811)
- Other features include encapsulation, lobulated fat and diffuse, globular or nodular intense enhancement (Radiol Case Rep 2017;12:811)
Images hosted on other servers:

Well circumscribed
intermuscular
mass within left
thigh on MRI

MRI of myxoid liposarcoma postradiotherapy
- Predilection for metastasis, especially when there is a significant round cell component
- Metastases can occur decades later, necessitating continued long term follow up (World J Surg Oncol 2008;6:62)
- Pure low grade tumors have less aggressive behavior but still share a propensity for recurrence and can metastasize in 5 - 10% of cases
- Unfavorable outcome has been associated with TP53 and CDKN2A gene mutations, although this seems rare (Tumori 1998;84:571)
- Some evidence suggests that high grade components can be identified via MRI and that metastases can be identified very early with imaging studies (Acta Radiol 2014;55:952, Skeletal Radiol 2018;47:369)
- 35 and 44 year old men with multicentric tumors (World J Surg Oncol 2007;5:139)
- 51 year old man with thyroidal metastases from a right thigh myxoid liposarcoma (J Laryngol Otol 2006;120:511)
- 66 year old woman with solitary breast metastasis from a right thigh myxoid liposarcoma (BMC Cancer 2014;14:482)
- 71 year old man with supraclavicular fossa mass (Chest 2000;117:1518)
- Review of patients with skeletal metastases (Ann Surg Oncol 2007;14:1507)
- Surgical resection with negative margins is the treatment of choice
- Trabectedin may be useful in nonresectable tumors
- Neoadjuvant or adjuvant radiation therapy may be considered since myxoid liposarcoma has been found to be more radiosensitive than many other soft tissue tumor types (Cancer 2009;115:3254)
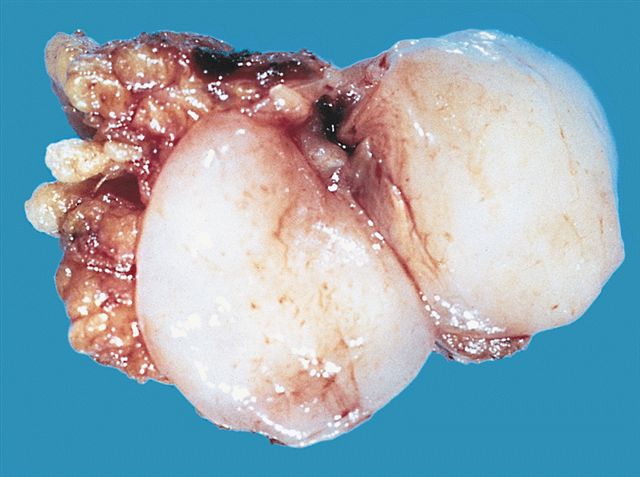
- Typically these lesions are well circumscribed and multinodular
- Low grade tumors will have a gelatinous cut surface, with higher grade tumors showing a more solid fleshy appearance
AFIP images
Well differentiated myxoid liposarcoma

Thigh tumor postchemotherapy
Images hosted on other servers:

Recurrence of adipose mass with kidney involvement

Well circumscribed white tumor

Lobulated gray white tumor within skeletal muscle
- Low grade
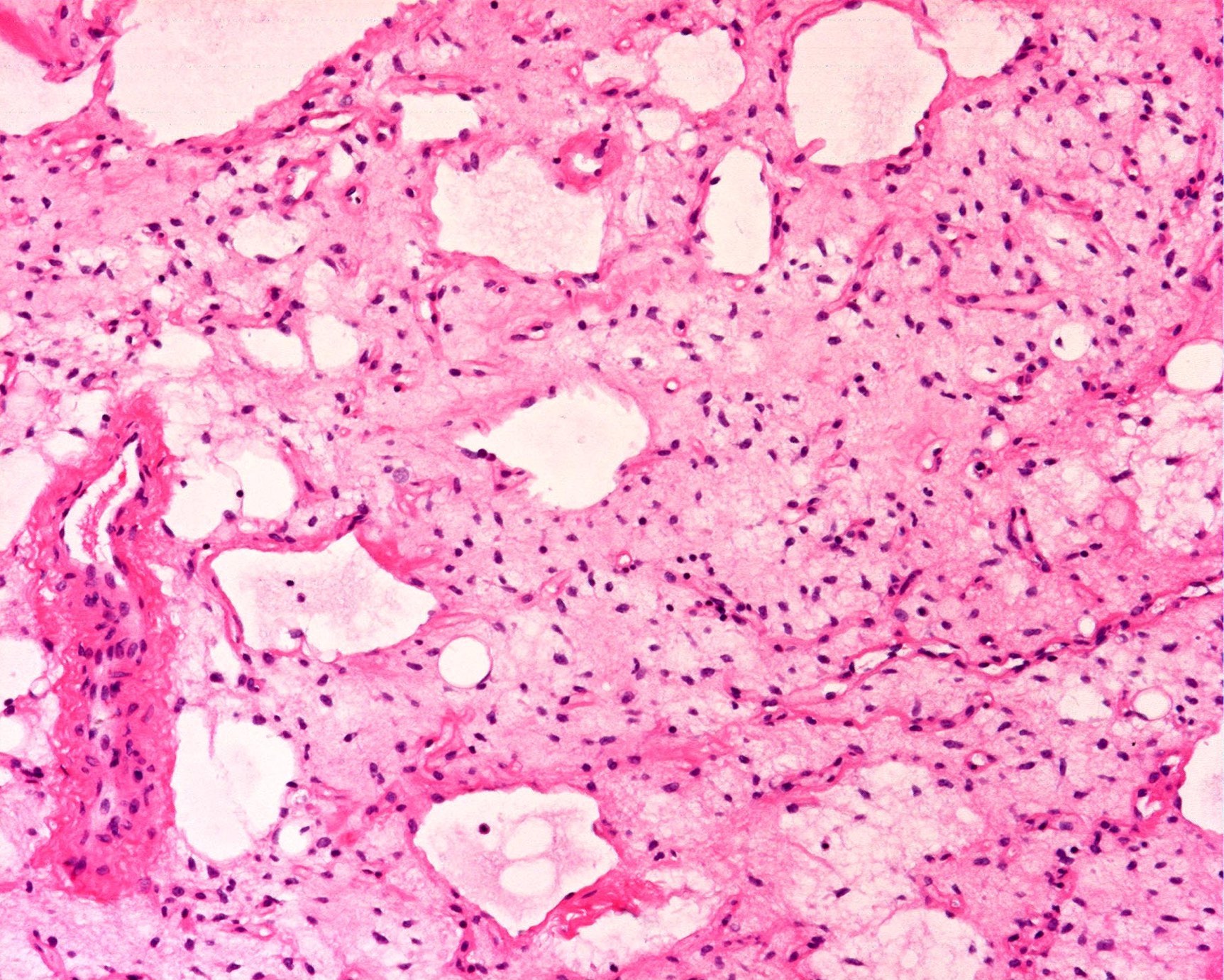
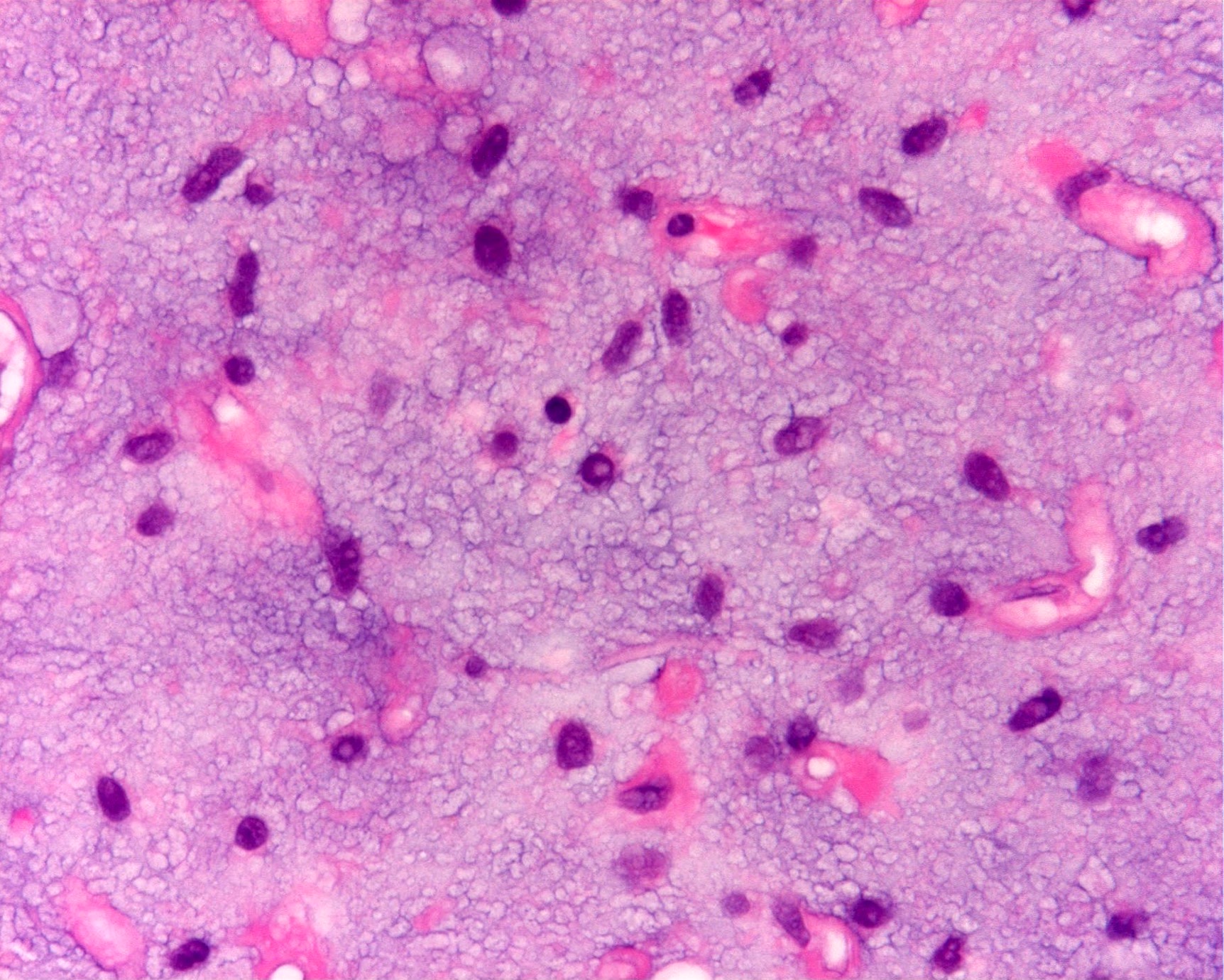
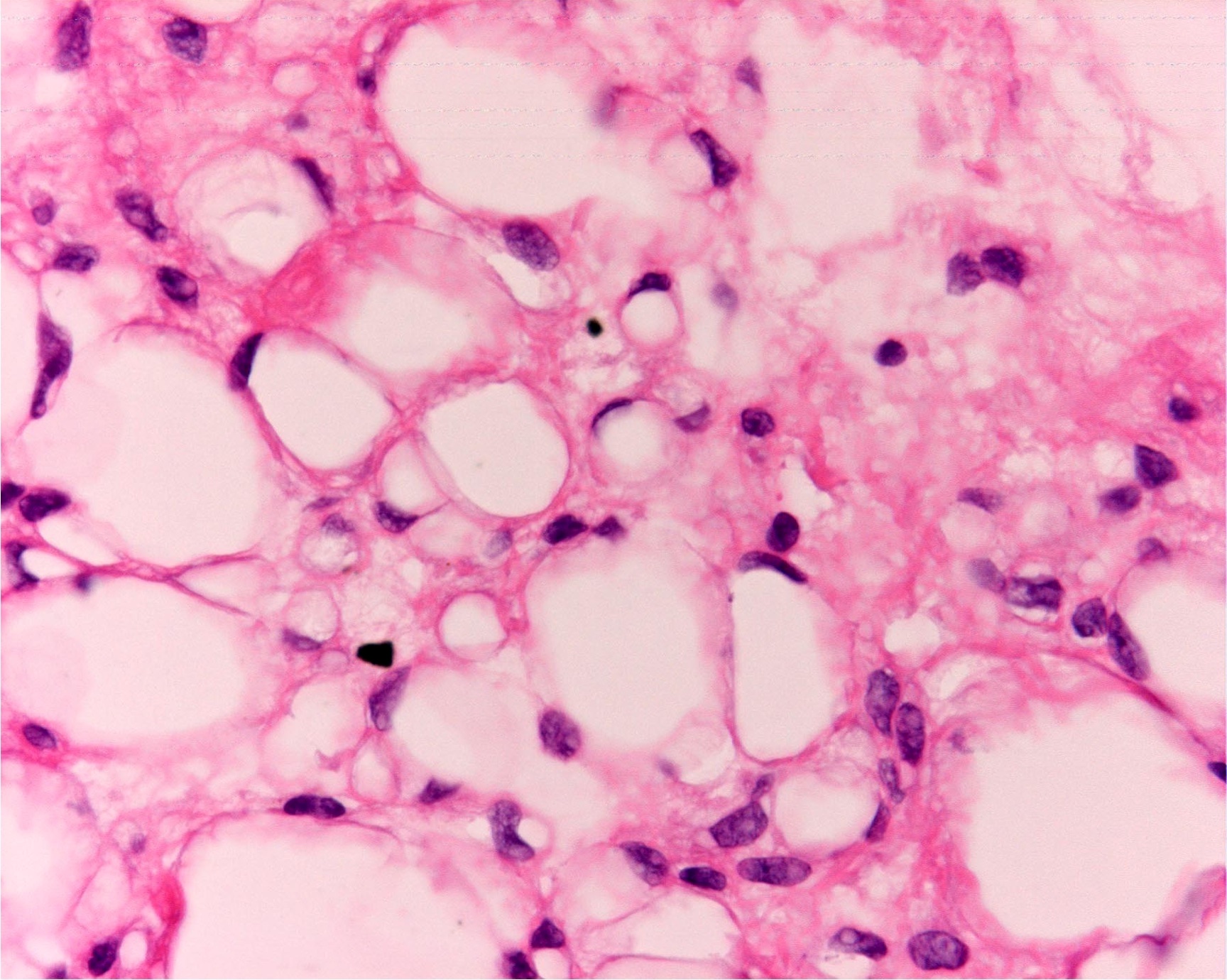
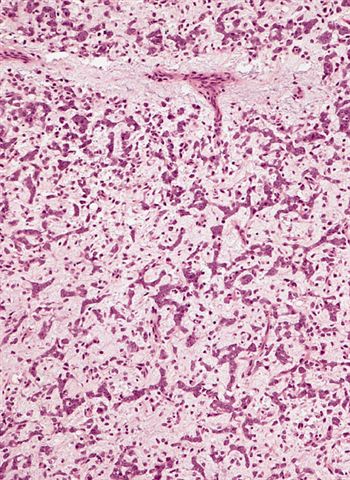
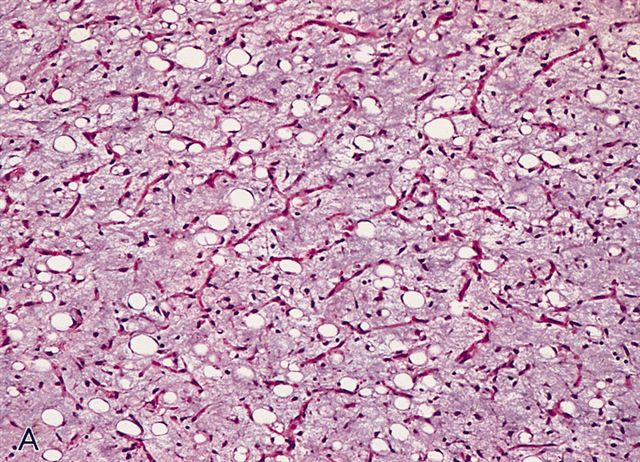
- Paucicellular with monomorphic, stellate or fusiform shaped cells without atypia; striking in their blandness, so much so that any significant pleomorphism should cause one to pause
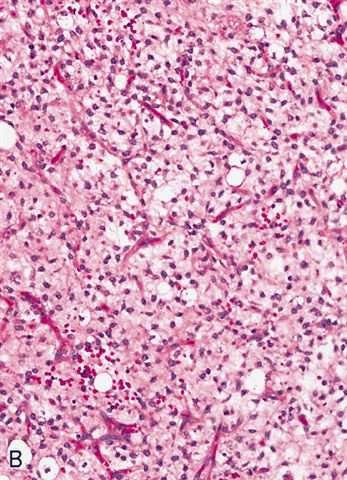
- Prominent plexiform vasculature (delicate thin walled arborizing and curving capillaries that form a network reminiscent of chicken wire fencing)
- These are striking because of the overall background paucicellularity and are still present in high grade tumors but are much less obvious
- Numerous signet ring lipoblasts, particularly at periphery of lobules
- This imparts a lipoblastoma-like appearance (see Differential diagnosis)
- Mucoid matrix is rich in hyaluronic acid that may form large mucoid pools (so called pulmonary edema pattern)
- Will be positive for stromal mucin stains such as Alcian blue (see Microscopic (histologic) images)
- Metaplastic cartilage or bone can rarely be seen
- Metaplastic components retain the same molecular alteration without progressive molecular change (no support that these foci represent dedifferentiation) (J Clin Oncol 2018;36:151, Appl Immunohistochem Mol Morphol 2007;15:477)
- Typically there is no significant mitotic activity
- There are many rare morphologic variants (Am J Clin Pathol 2012;137:229)
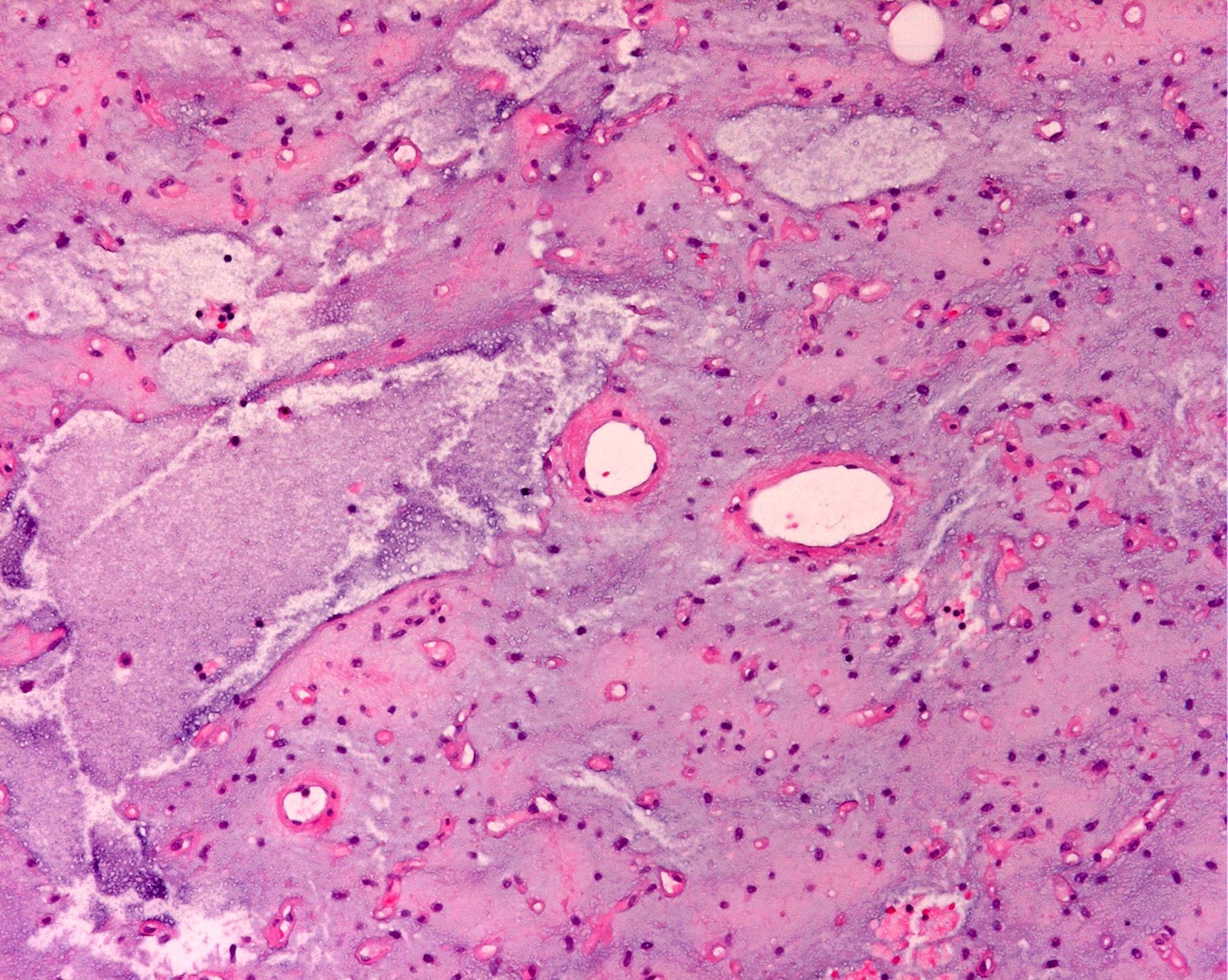
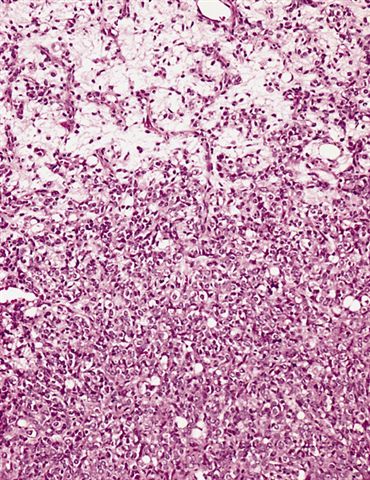
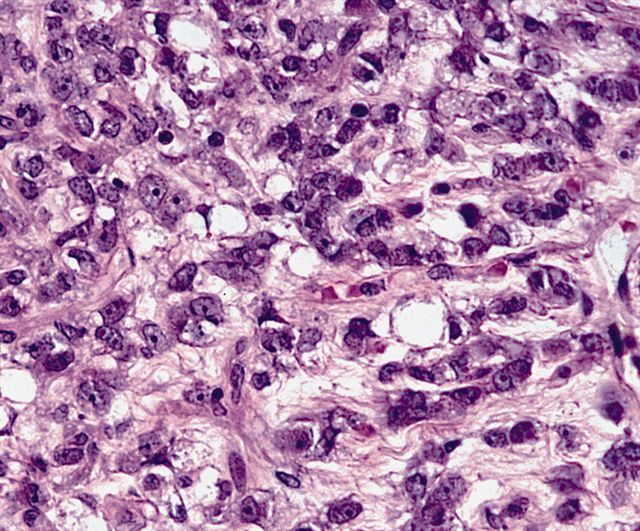
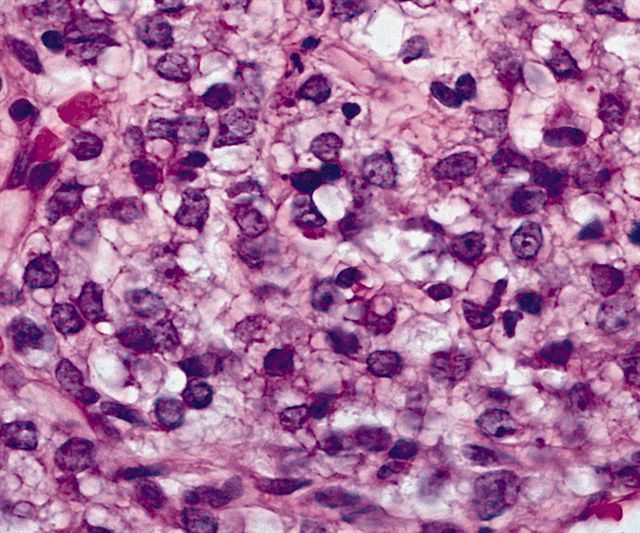
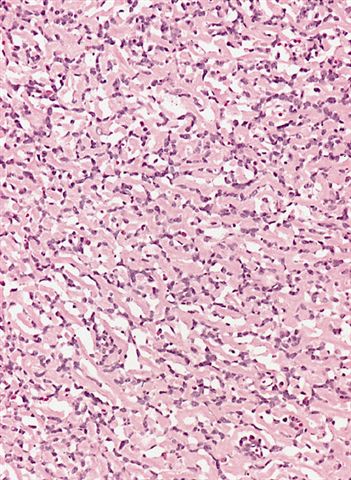
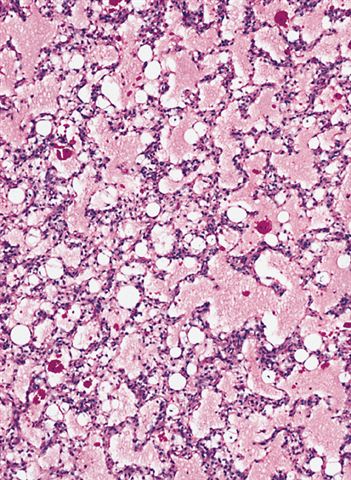
- High grade
- Hypercellular solid sheets of back to back cells with round cell or primitive cytomorphology in > 5% of the sampled tumor
- Cells can have a small amount of hypereosinophilic cytoplasm, a finding of no clinical significance but of significant diagnostic confusion, especially in a limited sample
- Pitfalls and tips
- High grade tumors are so cellular that you can typically walk across nuclei in a high power field without stepping in matrix
- When in doubt, especially in a small sample, pursue molecular testing (typically fluorescent in situ hybridization) for FUS gene rearrangement
- If no FUS gene rearrangement is detected and your suspicion is high that the lesion represents myxoid liposarcoma, proceed to EWSR1 fusion testing, as EWSR1::DDIT3 fusions are detected in rare cases (see Molecular / cytogenetics description)
- Sample these tumors extensively; you likely will not see small amounts of round cell progression grossly
- Can contain large areas of mature adipocytic differentiation
- If the clinical or radiologic picture is concerning, sample additional tumor or do molecular testing
- Location (e.g., extremity) and age of the patient (e.g., young adult) can be helpful clues in the differential diagnosis
- Most of the diagnostic clues are helpful in the appropriate context but individually can be seen in many other tumor types
- Plexiform vasculature and cells that look like signet rings can be found in a diverse variety of tumors
- Combination of a number of clinical, radiologic, histologic and if needed, molecular features will make the diagnosis
Contributed by Jesse J. Jenkins, M.D. and AFIP
Bland stellate shaped cells
High power
Pulmonary edema pattern
Signet ring lipoblasts


Postchemotherapy
Sheets of primitive round cells
Cords of cells resembling myxoid chondrosarcoma
Hyalinized collagenous stroma
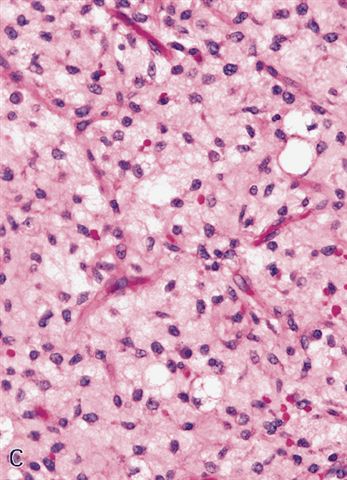
Delicate capillary network
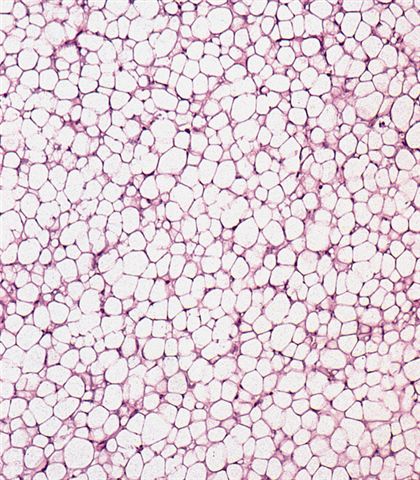

Large (mature) and small fat cells
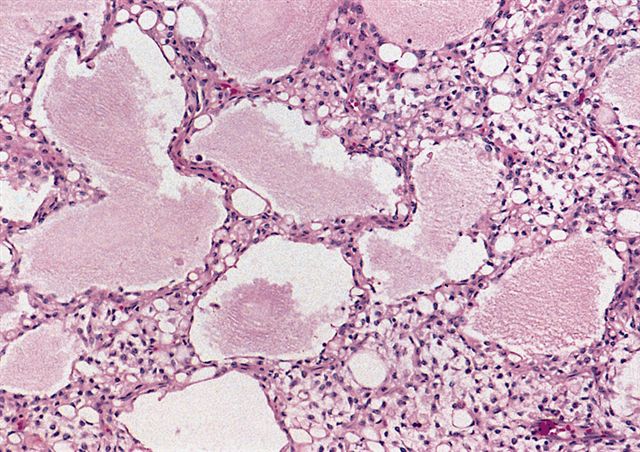

Pulmonary edema pattern

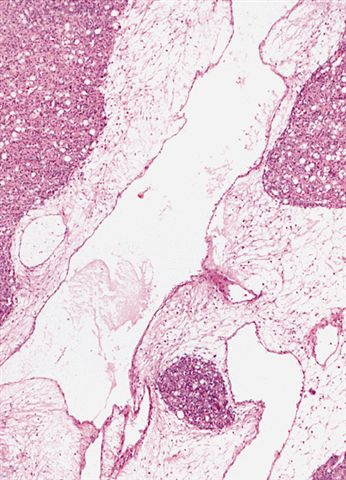
Hypocellular zones
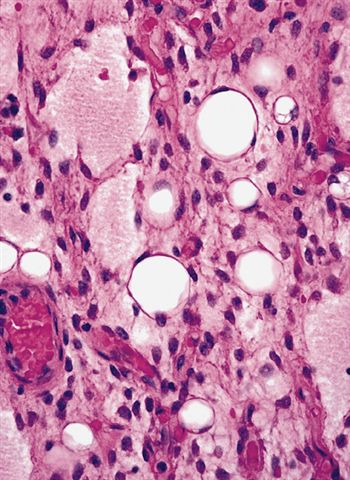

Signet ring lipoblasts

Alcian blue
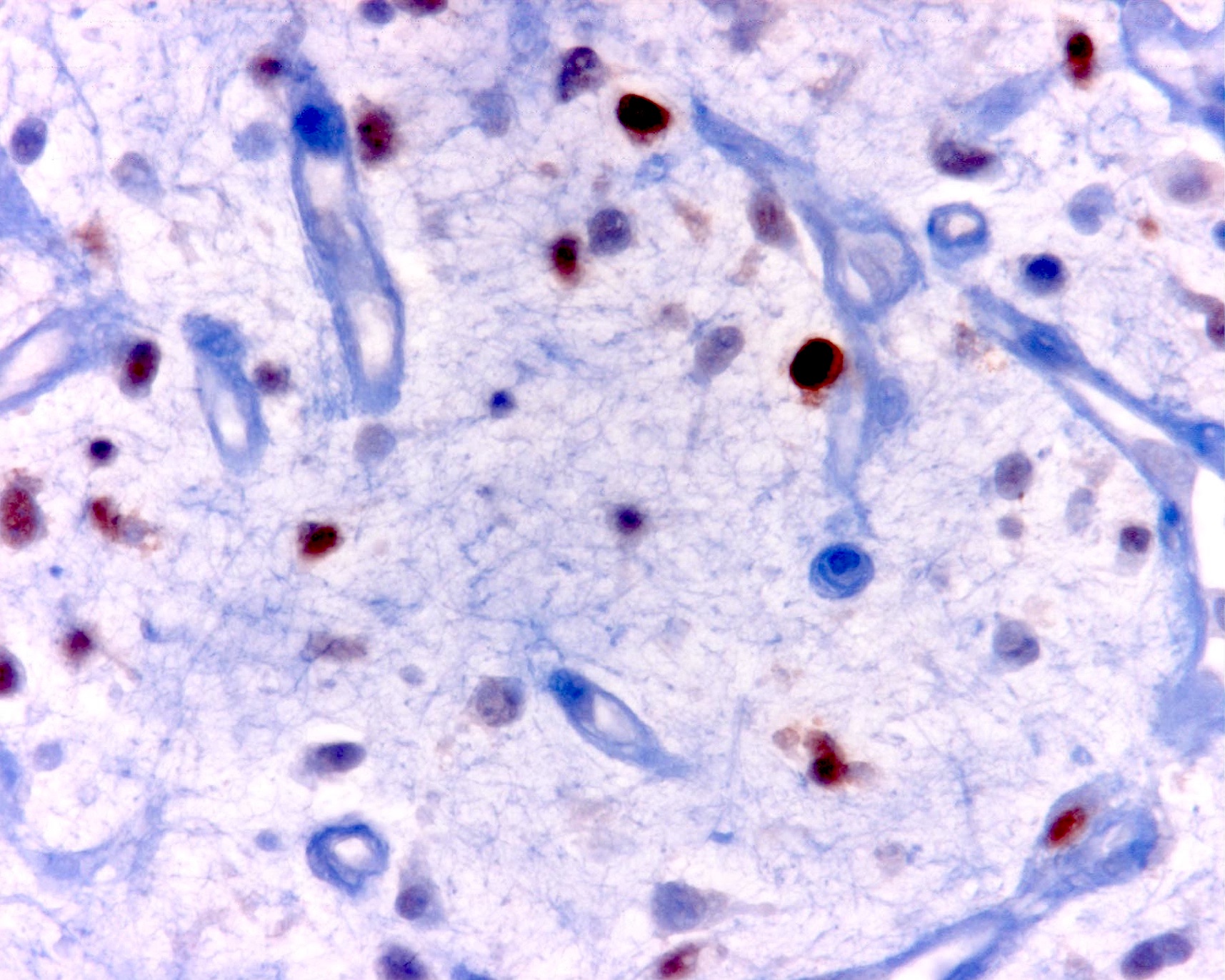
S100 protein

Vimentin
Images hosted on other servers:

MLPS: soft tissue, thigh, excision

MLPS: abdomen, excision
- Myxoid material with arborizing blood vessels and lipoblasts (Acta Cytol 2007;51:456)
- t(12;16)(q13;p11.2) FUS::DDIT3 in most cases
- t(12;22)(q13;q12) EWSR1::DDIT3 very rarely (2 - 5%)
- Rearrangements can be complex and involve other chromosomes (Am J Clin Pathol 1995;103:20)
- DDIT3 was formerly known as CHOP (early literature will use the terminology FUS::CHOP)
- Can be identified via FISH, PCR, classic cytogenetics and sequencing
Myxoid liposarcoma
High grade myxoid liposarcoma
- Soft tissue mass, left thigh, resection:
- Myxoid liposarcoma, low grade (5.5 cm) (see comment)
- Surgical resection margins are negative for tumor
- Comment: Histologic sections of this soft tissue mass demonstrate a hypocellular lesion composed of bland round to stellate cells evenly dispersed in a myxoid stroma with delicate arborizing vasculature. No areas of high grade disease are identified. FISH studies are positive for a DDIT3 gene rearrangement, supporting the diagnosis.
- Low grade:
- Atypical lipomatous tumor / well differentiated liposarcoma (ALT / WDL):
- Can be myxoid and focally indistinguishable from myxoid liposarcoma
- Usually has some degree of stromal atypia, however, and will lack the plexiform vasculature
- Has amplification of chromosome 12q14 (including the MDM2 gene) versus the FUS rearrangement seen in myxoid liposarcoma
- Myxoid liposarcomas are also more likely to show a predilection for signet ring lipoblasts
- Extraskeletal myxoid chondrosarcoma (EMC):
- Composed of cords of epithelioid malignant cells set in a similar chondromyxoid matrix
- No cytoplasmic fat vacuoles and less prominent vasculature
- Immunohistochemical staining is not helpful (both are S100 positive)
- Cytogenetics can be helpful but care must be taken
- EMC has t(9;22)(q22;q12) gene rearrangements in most cases that result in an EWSR1::NR4A3 fusion
- EWSR1 FISH will be positive but can lead to confusion with the 2 - 5% of myxoid liposarcomas that rarely have EWSR1 rearrangements
- PCR applications can be particularly helpful in this setting
- In the lung, primary pulmonary myxoid sarcoma should be considered (Pathology 2017;49:792)
- Lipoblastoma / lipoblastomatosis:
- Can show similar histology but usually are present in patients < 5 years old
- Will have PLAG1 gene rearrangements instead of FUS or EWSR1 rearrangements
- Lipoblastoma-like tumor of the vulva:
- Recently described entity that occurs in the vulva and shares remarkable histologic overlap with lipoblastoma and myxoid liposarcoma
- These lesions have been shown to have Rb loss like the spindle cell lipoma family of tumors
- Does not have PLAG1 or FUS rearrangements (Int J Gynecol Pathol 2019;38:204, Am J Surg Pathol 2015;39:1290)
- There is a significant difference in treatment and clinical outcome (only a limited ability to locally recur) and these lesions should be distinguished when possible
- Myxoid dermatofibrosarcoma protuberans (DFSP):
- Typically these are located superficially, which is uncommon in myxoid liposarcoma
- Look carefully to distinguish between entrapped fat versus true signet ring lipoblasts
- Immunohistochemical staining and molecular testing can help
- DFSP will be CD34 positive, S100 negative, with the inverse seen in myxoid liposarcoma and DFSP will harbor the t(17;22)(q22;q13) COL1A1::PDGFB gene fusion
- Some large reference labs offer PDGFB as a break apart FISH assay
- Myxoma:
- Extremely paucicellular, lacks a prominent vascular component and no lipoblasts are found
- Associated with GNAS mutations (Mod Pathol 2009;22:718)
- Atypical lipomatous tumor / well differentiated liposarcoma (ALT / WDL):
- High grade:
- Myxofibrosarcoma:
- Older adults, often superficial, infiltrative and with no true cytoplasmic fat vacuoles (although they can contain pseudolipoblasts)
- Significantly more nuclear atypia, thicker curvilinear vessels and frequent mitotic figures
- Pleomorphic liposarcoma (PLS):
- Entirely different entity that shares similarity in name only
- High grade pleomorphic sarcoma with scattered atypical lipoblasts
- Atypia far in excess of what is seen in round cell liposarcoma, which retains its monotony (a clue to a tumor driven by a translocation)
- Typically has a complex karyotype
- Round cell sarcomas (Ewing, BCOR::CCNB3, CIC::DUX4, etc.):
- Numerous round cell sarcomas that may morphologically resemble high grade myxoid liposarcoma
- Low grade areas and lipoblasts can be particularly informative
- Immunohistochemical and molecular differences can also be exploited (Ewing sarcoma has different partner genes than does myxoid liposarcoma, a feature that can be taken advantage of via sequencing or PCR)
- Myxofibrosarcoma:
The microscopic image above depicts the histologic appearance of a soft tissue mass resected from the thigh of a 37 year old man and is representative of the entire lesion. Which of the following is true regarding the diagnosis?
- Immunohistochemical studies for MDM2 will show strong diffuse positive nuclear staining in the tumor cells
- Majority of cases harbor t(7;16) FUS::CREB3L2 gene fusion
- Majority of cases harbor t(9;22) EWSR1::NR4A3 gene fusion
- Majority of cases harbor t(12;16) FUS::DDIT3 gene fusion
- The lesion is classified as high grade if hypercellular solid sheets of back to back cells with round cell cytomorphology compose > 1% of the sampled tumor
Comment Here
Reference: Myxoid liposarcoma
- Hyalinized, thick walled vessels
- Poor response to radiation therapy
- Primary tumor in the retroperitoneum
- Propensity to skip the lung and metastasize to other soft tissue sites
- Marked nuclear atypia
Comment Here
Reference: Myxoid liposarcoma
