Stomach
Polyps
Pyloric gland adenoma
Author: Supriya Srivastava, M.D., Ph.D.
Editorial Board Member: Catherine E. Hagen, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.

Last author update: 2 April 2021
Last staff update: 2 February 2022
Copyright: 2021-2025, PathologyOutlines.com, Inc.
PubMed Search: pyloric gland adenoma [TI]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Srivastava S. Pyloric gland adenoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stomachpyloricglandadenoma.html. Accessed September 3rd, 2025.
Definition / general
- Grossly visible neoplastic lesion in the stomach, wherein the native glands are replaced by closely packed pyloric glands lined by cuboidal to low columnar epithelium
- 40 - 50% associated with high grade dysplasia
Essential features
- Closely packed tubular glands lined by cuboidal to low columnar epithelium with ground glass cytoplasm, bland nuclei and no well formed apical mucin cap
- 60% observed in corpus of the stomach, followed by cardia and antrum
- Associated with autoimmune gastritis, familial adenomatosis polyposis and Lynch syndrome
- Commonly associated with dysplasia
Terminology
- Pyloric gland tubular adenoma; gastric differentiated adenoma (German); pyloric gland intracystic papillary neoplasm (J Clin Pathol 2014;67:883)
ICD coding
- ICD-O: 8210/0 - adenomatous polyp
- ICD-10: K31.7 - polyp of stomach and duodenum
- ICD-11: 2E92.1&XH3DV3 - benign neoplasm of stomach and adenoma NOS
Epidemiology
- Accounts for 3% of all gastric epithelial polyps (Virchows Archive 2003;442:317)
- Slightly more common in females as compared with males (Am J Surg Pathol 2009;33:186)
- Mean age: 70 years
- No predilection for a specific geographic location
- Strongly associated with autoimmune gastritis; some association with familial adenomatosis polyposis
Sites
- In stomach, most commonly seen in fundus / corpus, followed by cardia and antrum
- Other sites: reported frequencies are variable in different studies; however, one of the largest series of 373 cases of pyloric gland adenoma (PGA) reports the following frequencies - duodenum including duodenal bulb (11%), gallbladder (4.3%), pancreas, bile duct (1.4%), pancreatic duct (0.3%), rectum (1.1%), esophagus (2.4%), cervix (rare) (J Clin Pathol 2014;67:883)
Pathophysiology
- Pyloric gland metaplasia (in the stomach) / gastric heterotopia (elsewhere) is the precursor lesion of pyloric gland adenoma (J Clin Pathol 2014;67:883)
Etiology
- Associated with autoimmune gastritis
- It is also seen in association with familial polyposis syndrome, Lynch syndrome, juvenile polyposis syndrome, McCune-Albright syndrome (Am J Surg Pathol 2014;38:784, Am J Surg Pathol 2014;38:1618, Virchows Arch 2017;470:391)
Clinical features
- Usually asymptomatic but may present with gastric distention, epigastric pain or heartburn
- Background mucosa is that of autoimmune gastritis or Helicobacter pylori gastritis
- Its predominance in females reflects its association with autoimmune gastritis
- Sporadic PGA tends to occur in younger patients and without any inflammatory background, sometimes in association with fundic gland polyp
Diagnosis
- Diagnosis is made by endoscopy and histology
Prognostic factors
- Since it is associated with high grade dysplasia and gastric adenocarcinoma, all PGAs should be resected
- Prognosis depends on the associated dysplasia and adenocarcinoma
- The neoplastic risk increases with the associated autoimmune gastritis, larger mean polyp size and tubulovillous architecture; however, after a complete endoscopic resection, the rate of local recurrence is low (< 10%) (Histopathology 2018;72:1007)
Case reports
- 60 year old man presenting with epigastric pain and polyp in corpus of stomach (Case Rep Gastroenterol 2013;7:392)
- 69 year old man with a submucosal tumor-like lesion in stomach body (World J Clin Cases 2020;8:2380)
- 75 year old man with STK11 germline mutation and multiple gastrointestinal tumors (Case Rep Gastroenterol 2020;14:547)
- 80 year old woman with a polypoid tumor in cardia (Am J Gastroenterol 2018;113:2645)
- 81 year old man with a flat lesion 20 mm in diameter (J Gastrointestin Liver Dis 2018;27:361)
Treatment
- Endoscopic mucosal resection, surgical resection
Clinical images
Contributed by Supriya Srivastava M.D., Ph.D.
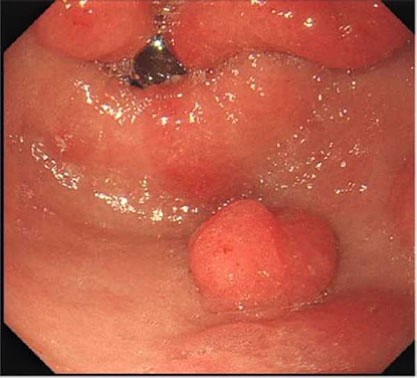
Endoscopic appearance
Images hosted on other servers:

Endoscopy
Gross description
- Polyp, sessile or pedunculated or masses ranging from 1 - 10 cm in size
- Usually single
Gross images
Images hosted on other servers:

Intraoperative image
Microscopic (histologic) description
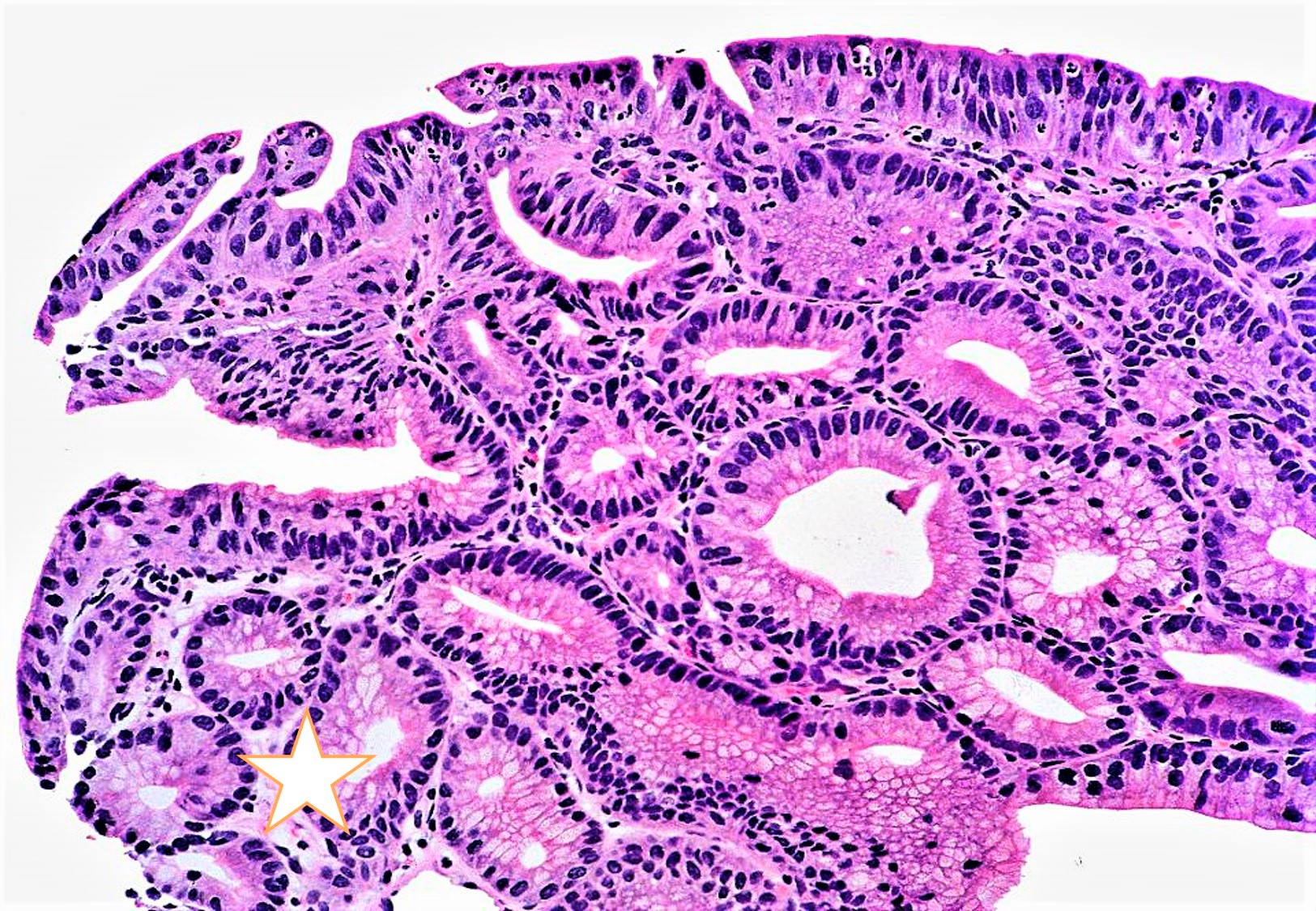
- Closely packed tubular glands (pyloric glands / pseudopyloric glands) with low cuboidal to columnar epithelium; cytoplasm is eosinophilic with ground glass appearance; round nuclei, basally located without any prominent nucleoli
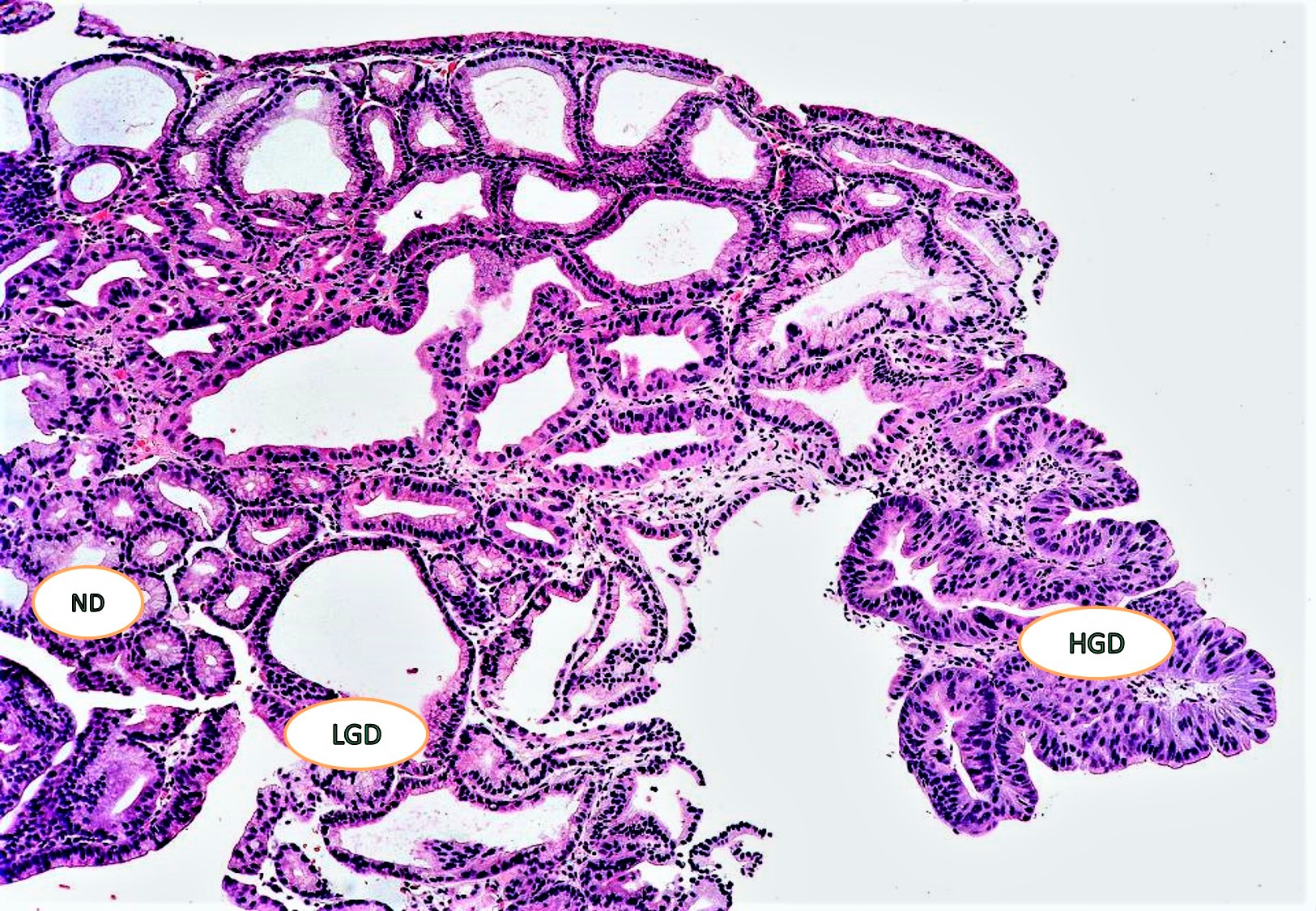
- PGA can occur without dysplasia, with low grade dysplasia and with high grade dysplasia; PGA may also be associated with adenocarcinoma (12 - 47%) but submucosal invasion is observed in fewer than 10% of cases
- PGA without dysplasia: small tubular glands, closely packed, lined by bland cuboidal to columnar epithelium with basally arranged round nuclei with inconspicuous nucleoli
- PGA with low grade dysplasia: slightly irregularly arranged tubular glands with slightly elongated nuclei with mild hyperchromasia with some stratification
- PGA with high grade dysplasia: architectural distortion such as irregularly arranged occasional cribriform glands with nuclear crowding, loss of polarity, vesicular nuclei and prominent nucleoli and few mitoses
- PGA associated with adenocarcinoma: invasive irregular complex glands, loss of nuclear polarity, high nuclear:cytoplasmic ratio, vesicular nuclei with irregular nuclear membranes and numerous mitoses
Microscopic (histologic) images
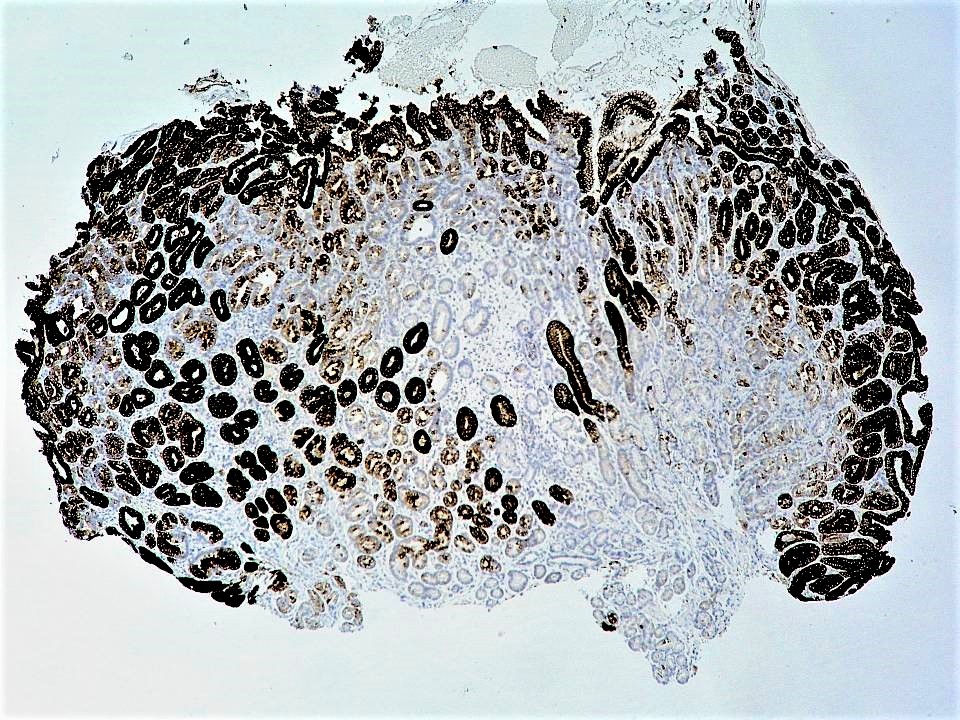
Contributed by Supriya Srivastava M.D., Ph.D.
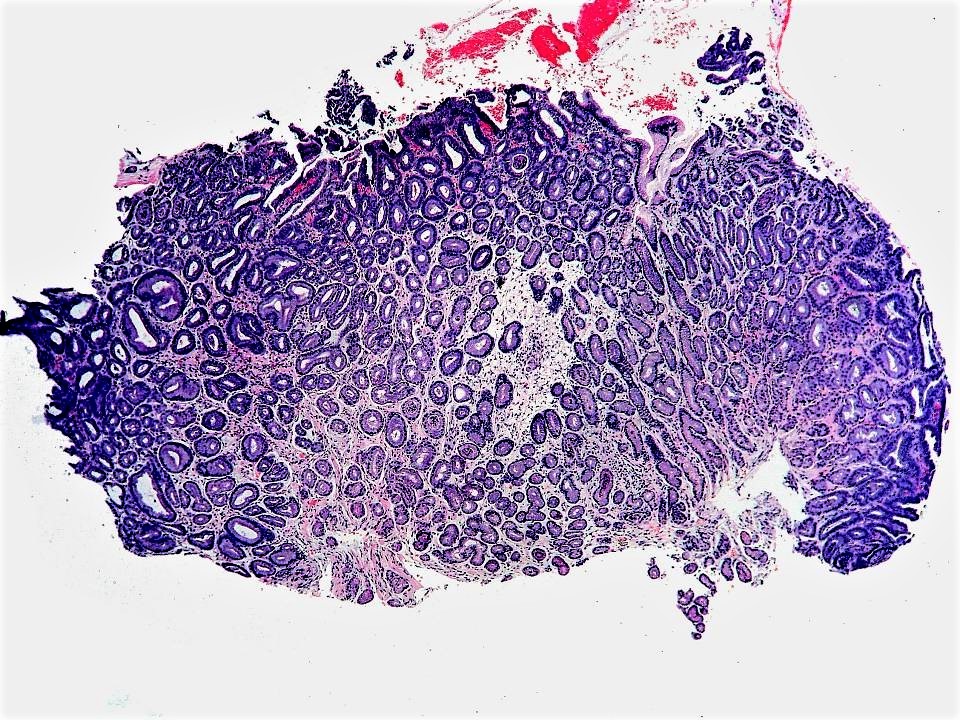
Antral polyp
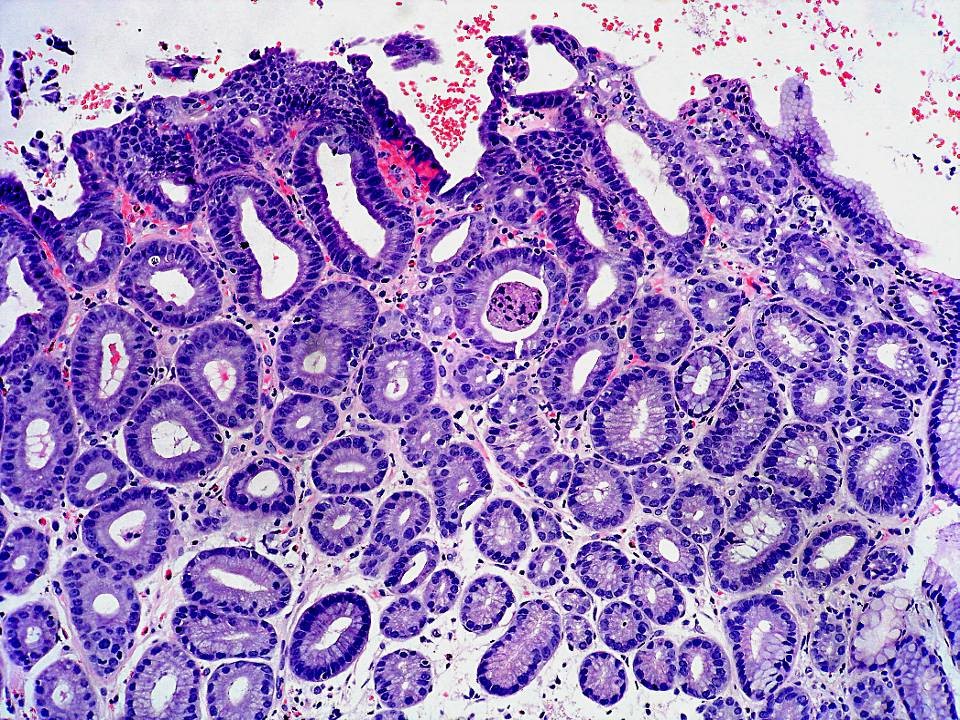
PGA without dysplasia
MUC5AC staining
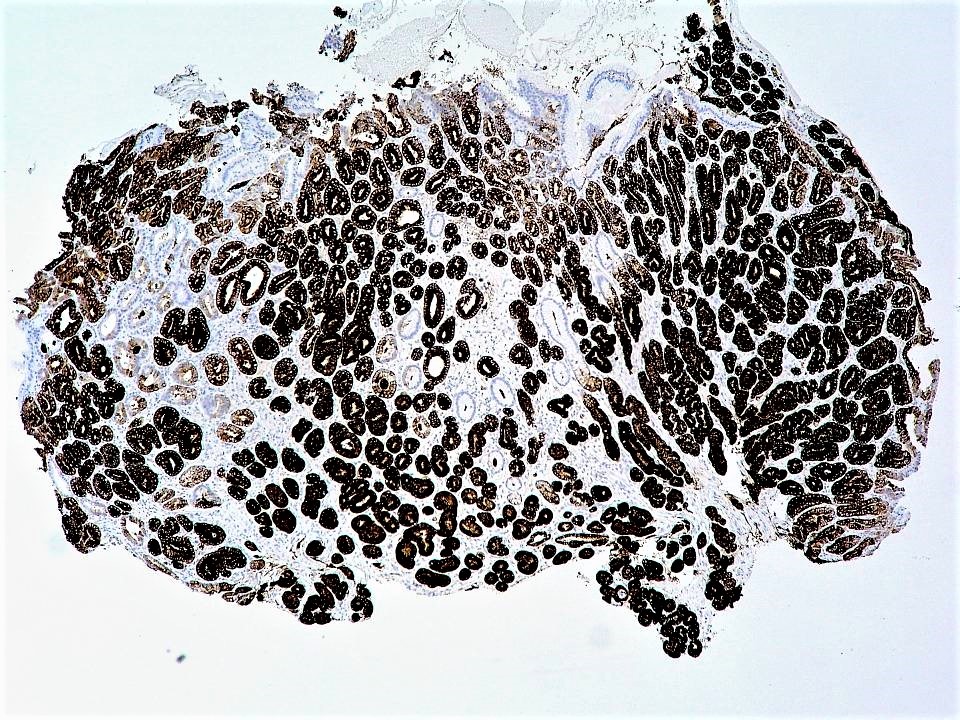
MUC6 staining
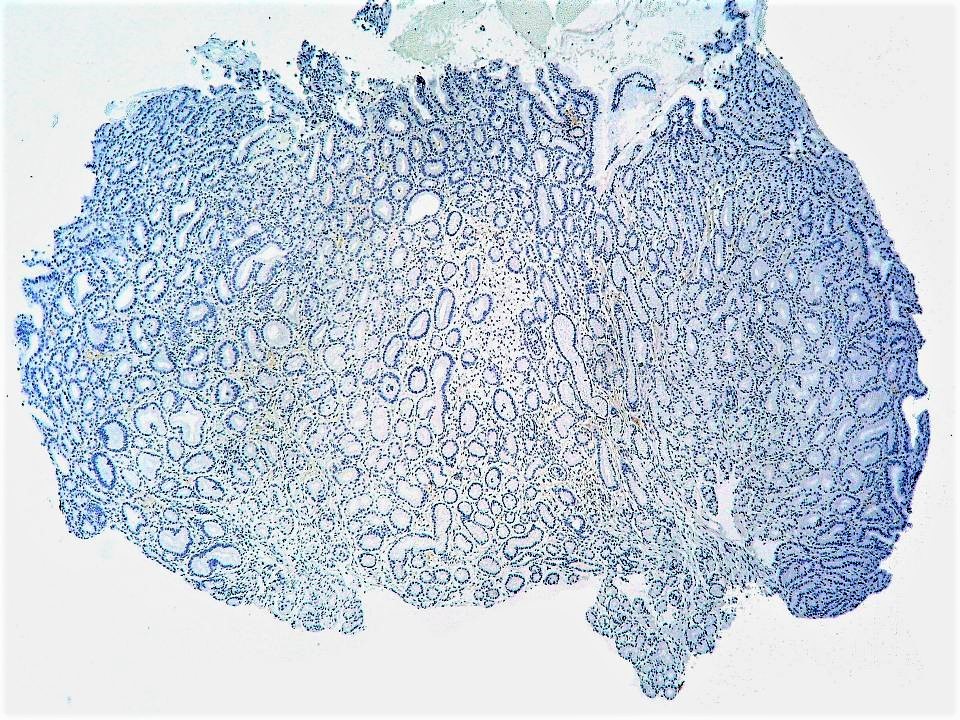
MUC2 staining
PGA with dysplasia
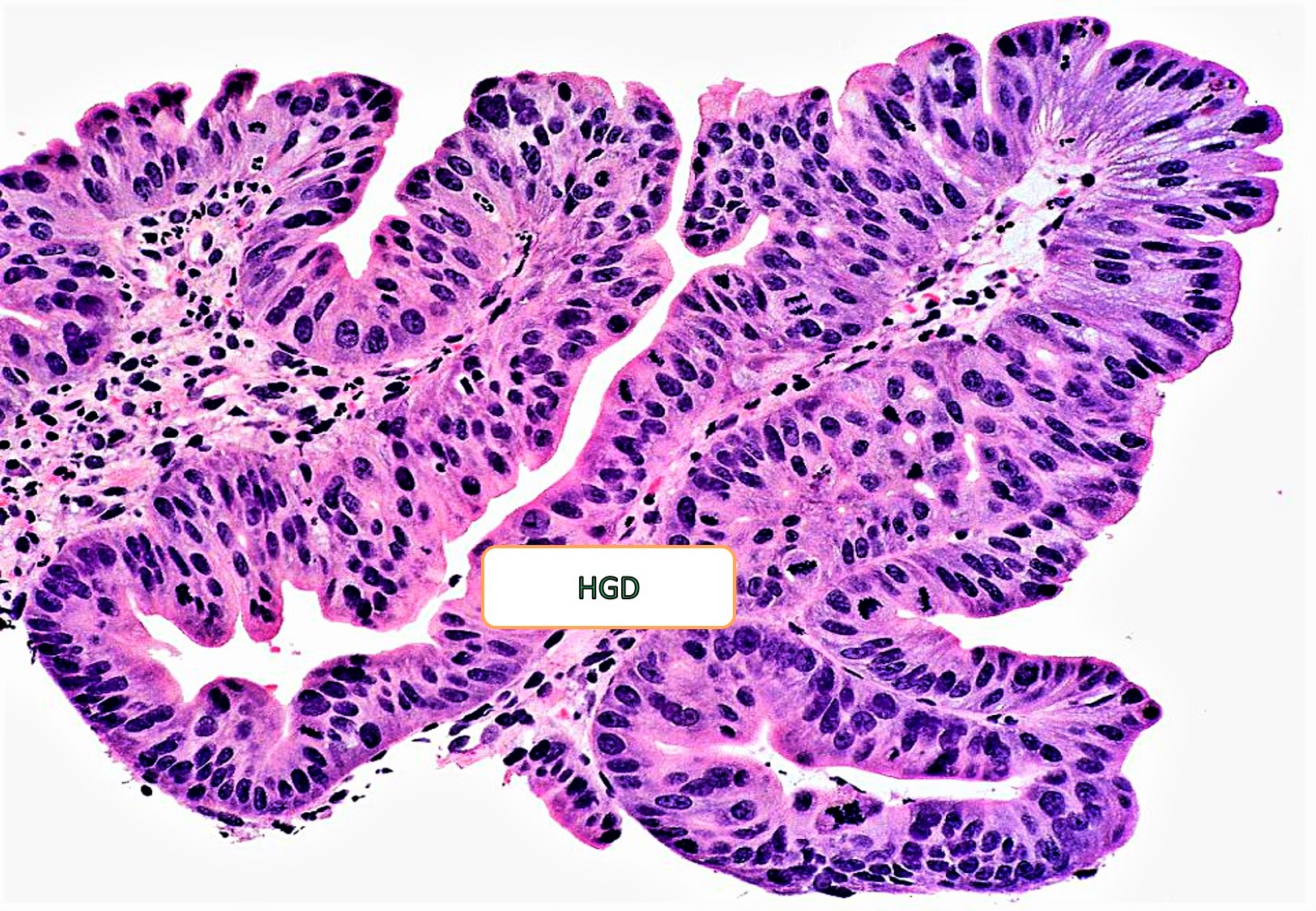
High grade dysplasia
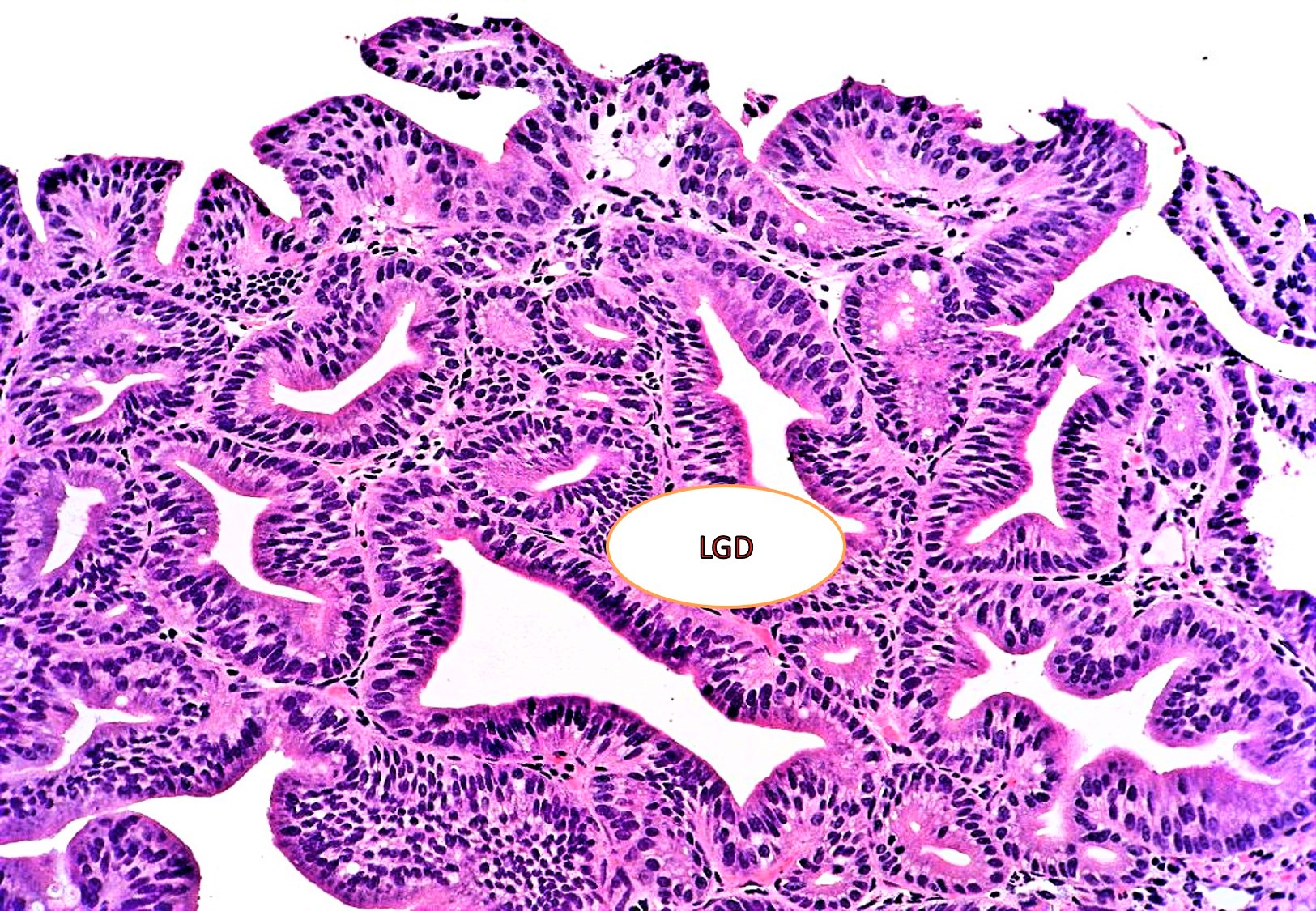
Low grade dysplasia
PGA with and without dysplasia
Positive stains
- Diffuse MUC6 in the deeper pyloric glands and MUC5AC in the superficial gastric glands (not limited to the surface foveolar epithelium generally)
- Concanavalin and MUC3 show similar expression as MUC6 (J Clin Pathol 2014;67:883)
- Nuclear beta catenin is also observed (Histopathology 2017;70:549)
Negative stains
- MUC2 and CDX2 (generally negative but could be occasionally focally positive)
- PASD and Alcian blue negative
Molecular / cytogenetics description
- GNAS and KRAS mutations often occur in PGAs of both stomach and duodenum (J Pathol 2013;229:579)
- GNAS, KRAS and APC mutations have also been reported in sporadic and familial cases of PGA (Histopathology 2015;67:689)
- KRAS, APC, TP53 and CTNNB1 mutations may also occur in PGA without or with cytological dysplasia (Mod Pathol 2020;33:2075)
Sample pathology report
- Stomach, polypectomy:
- Pyloric gland adenoma (see comment)
- Comment: Histology shows tightly packed pyloric glands lined by cuboidal or low columnar epithelium with ground glass eosinophilic cytoplasm, basally located nuclei and absent apical mucin.
Differential diagnosis
- Hyperplastic polyp:
- Tall columnar epithelium, paler cytoplasm, apical mucin seen, irregular branching pits and edematous inflamed stroma
- Reactive foveolar hyperplasia:
- Proliferation of foveolar epithelium rather than deep pyloric glands
- Gastric foveolar type adenoma:
- Oxyntic gland adenoma:
- Arising from the oxyntic mucosa; proliferating glands show chief cell differentiation
- Pepsinogen I and II positive
Additional references
Practice question #1
A polypoid lesion of the stomach was resected in a 75 year old man. Based on the histological feature provided in the photomicrograph above, which of the following statements is correct?
- Cells have an apical mucin cap
- GNAS mutation is commonly observed
- MUC2 expression is frequent in this lesion
- TP53 mutations are commonly seen
Practice answer #1
B. KRAS and GNAS mutations are commonly seen in pyloric gland adenoma
Comment Here
Reference: Pyloric gland adenoma
Comment Here
Reference: Pyloric gland adenoma
Practice question #2
Which of the following statements is true about pyloric gland adenoma?
- It is most commonly observed in antrum of the stomach
- It is commonly observed in a background of autoimmune gastritis
- It is rarely associated with dysplasia
- PASD is extensively positive in the neoplastic glands
Practice answer #2
B. Pyloric gland adenoma is commonly observed in a background of autoimmune gastritis
Comment Here
Reference: Pyloric gland adenoma
Comment Here
Reference: Pyloric gland adenoma
