
Breast
Congenital anomalies
Supernumerary / accessory tissue
Authors: Sara Salehiazar, M.D., Gary Tozbikian, M.D.
Editorial Board Members: Julie M. Jorns, M.D., Kristen E. Muller, D.O.


Last author update: 22 June 2023
Last staff update: 22 June 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Supernumerary / accessory breast tissue

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Salehiazar S, Tozbikian G. Supernumerary / accessory tissue. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastsupernumerary.html. Accessed April 27th, 2024.
Definition / general
- Persistent epidermal thickenings along milk line from axilla to perineum / vulva, due to clusters of primordial breast cells that fail to involute
- Ectopic breast tissue (nipple, areola and glandular breast tissue) may arise from anywhere along mammary ridge (midaxilla to inguinal area)
- Reference: eMedicine: Supernumerary Nipple [Accessed 5 May 2023]
Essential features
- Supernumerary or accessory breast tissue can arise anywhere along mammary ridge
- Mostly benign but reported with an increased risk of genitourinary neoplasms (renal adenocarcinoma, urinary bladder carcinoma, testicular and prostate cancers) (Dermatol Online J 2013;19:4)
- May develop breast carcinomas because it contains breast tissue
Terminology
- Polymastia classification system (Eplasty 2012;12:ic5)
- Class I: consists of a complete breast including glandular tissue, nipple and areola
- Class II: consists of only glandular tissue and nipple, without areola
- Class III: consists of only glandular tissue and areola, without nipple
- Class IV: consists of only glandular tissue
- Class V (pseudomamma): consists of only nipple and areola without glandular tissue
- Class VI (polythelia): accessory nipple (no glands or areola)
- Class VII (polythelia areolaris): accessory areola (no nipple or glands)
- Class VIII (polythelia pilosa): consists only of hair
- Polymastia: accessory breast including nipple, areola and glandular breast tissue
ICD coding
Epidemiology
- ~2 - 6% of females and 1 - 3% of males (Eplasty 2012;12:ic5)
- Occurrence rates vary widely on the basis of ethnicity and gender, ranging from 0.6% in Caucasians to 5% in Japanese females (Eplasty 2012;12:ic5)
Sites
- Found along the thoracoabdominal region of the milk line (the embryologic mammary streak)
- Accessory nipples: thorax or abdomen (65%) and axilla (20%) are most common; back, shoulder, buttock, face and neck are less common
- Accessory glandular tissue: axilla is most common (may occur bilaterally)
- Reference: S D J Med 1996;49:149
Pathophysiology
- In the human embryo, the mammary ridge first becomes apparent in the 7 - 8 mm long embryo and atrophies before birth
- Failure of normal apoptotic regression of the mammary ridges during gestation results in ectopically displaced or accessory breast tissue
- Extramammary glands can arise from anywhere along the mammary ridge (midaxilla to inguinal area) (Klimberg: Bland and Copeland's The Breast -Comprehensive Management of Benign and Malignant Diseases, 6th Edition, 2023)
Etiology
- Usually sporadic, can be familial (autosomal dominant) with incomplete expression (J Am Acad Dermatol 1994;30:667)
- Reported associations with other syndromes such as Turner syndrome, Fanconi anemia and other hematologic disorders; ectodermal dysplasia; Kaufman-McKusick syndrome; Char syndrome; Simpson-Golabi-Behmel syndrome; epibulbar lipodermoids associated with preauricular appendages syndrome (Pediatr Hematol Oncol 2004;21:461, Ophthalmic Genet 2010;31:81)
- Reported associations with renal abnormalities (J Pediatr 1979;95:274)
Diagrams / tables
Images hosted on other servers:
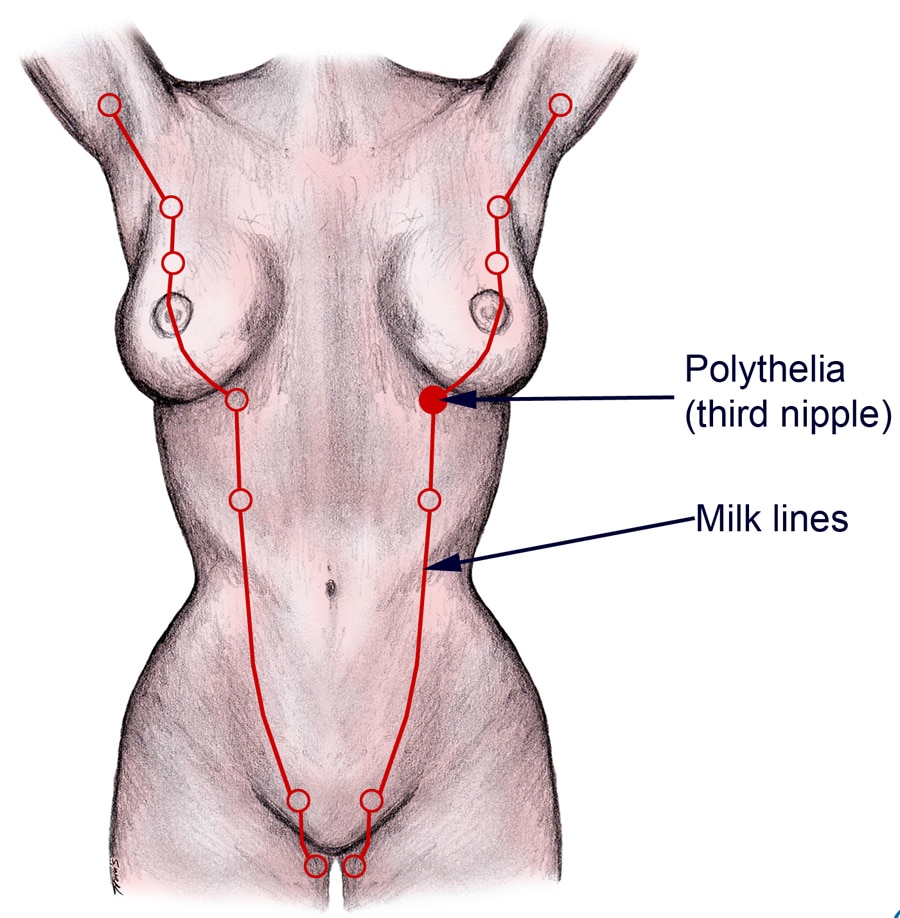
Extramammary tissue may arise anywhere along mammary ridge
Clinical features
- Higher incidence of urinary tract malformations reported in patients with supernumerary nipples; this may be explained by ethnic or geographic variations (Eur J Pediatr 1998;157:821)
- Polythelia is associated with an increased risk of genitourinary malignancies such as testicular seminoma (Dermatol Online J 2013;19:4)
- Supernumerary nipple can be considered a cutaneous marker of mitral valve prolapse with chest pain, palpitations, precordial pulsations and cardiomegaly in patients of Asian Indian ethnicity (Am J Cardiol 2000;86:695)
Diagnosis
- Usually made by self examination
- Mostly similar to brown freckle
Radiology description
- Radiographically the accessory tissue resembles normal glandular tissue as a high density lesion resembling normal breast parenchyma but is separate from normal breast tissue (Radiol Case Rep 2021;16:2804)
- The mean radiographic dimension of the accessory tissue is 3.9 cm and on mammography, clearly separated from glandular parenchyma but located in the axilla (Radiology 1987;163:709)
- Accessory tissue is best visualized on oblique and exaggerated craniocaudal views in mammography (Radiology 1987;163:709)
- Ultrasound can help to differentiate accessory breast tissue from lipoma, lymphadenopathies, sebaceous cysts and other pathologic entities in the axilla (J Ultrasound Med 2017;36:1469)
- All the benign and malignant diseases of the breast also occur in accessory breast tissue with the same imaging features as the main breast tissue; the identification of normal breast tissue adjacent to a mass strongly suggests that the lesion arose from accessory breast tissue (J Ultrasound Med 2017;36:1469)
Radiology images
Images hosted on other servers:

Proliferation of glandular tissue, without areola or nipple


Normal appearance of accessory breast tissue on mammography

Accessory breast tissue on ultrasound
Prognostic factors
- Usually benign
- If containing breast glands and stroma, breast malignancies can arise in the breast tissue underlying supernumerary nipples
Case reports
- 14 year old boy with accessory nipple over the right scapula (Int J Surg Case Rep 2019;55:35)
- 25 year old woman with cutaneous periumbilical fibroadenoma in the ectopic breast tissue (Cureus 2021;13:e17523)
- 32 year old woman with multiple supernumerary nipples (Am Fam Physician 2022;106:11A)
- 40 year old man with pleomorphic adenoma of a supernumerary male nipple (J Breast Imaging 2019;1:356)
- 44 year old woman with Paget disease of supernumerary breast (Ann Dermatol Venereol 2018;145:423)
- 61 year old woman with syringomatous tumor presenting as inversion of a supernumerary nipple (Case Rep Pathol 2019;2019:9461815)
- 70 year old woman with ductal invasive carcinoma in the anterior chest wall accessory breast tissue (Medical Research Archives 2022;10:6)
- 71 year old woman with unilateral axillary supernumerary breast, which gets larger after menopause (Radiol Case Rep 2021;16:2804)
- 78 year old woman with poorly differentiated infiltrative breast carcinoma in the accessory nipple (JAAD Case Rep 2020;6:540)
Treatment
- Usually no surgery
- Surgery performed for cosmetic reasons or if a lesion has developed in the breast tissue
Clinical images
Images hosted on other servers:
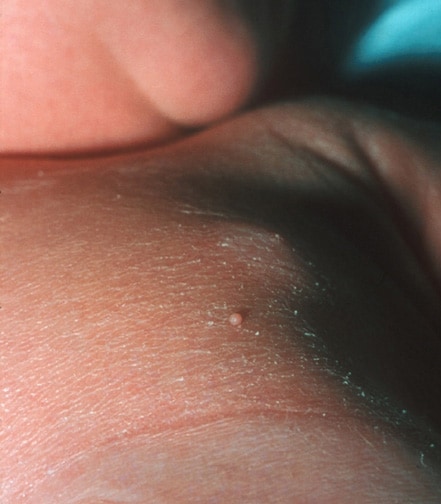
Supernumerary nipple in a neonate

Supernumerary nipple in an adolescent boy

Supernumerary nipple (bilateral) in an adolescent girl

Ectopic supernumerary nipple on the shoulder


Nipple on foot


Large axillary supernumerary breast

Hyperpigmented papule shape skin elevation

Cutaneous fibroadenoma in ectopic breast tissue

Supernumerary nipple on abdomen
Gross description
- Well demarcated, hyperpigmented or skin colored papule, with central elevation or opening
Microscopic (histologic) description
- Same histologic features as normal nipple, including hyperpigmentation, slight hyperkeratosis, pilosebaceous structure of Montgomery tubercles, smooth muscle, Toker cells and possibly breast lobules and ducts (J Cutan Pathol 2003;30:256)
Microscopic (histologic) images
Contributed by Sara Salehiazar, M.D. and Gary Tozbikian, M.D.
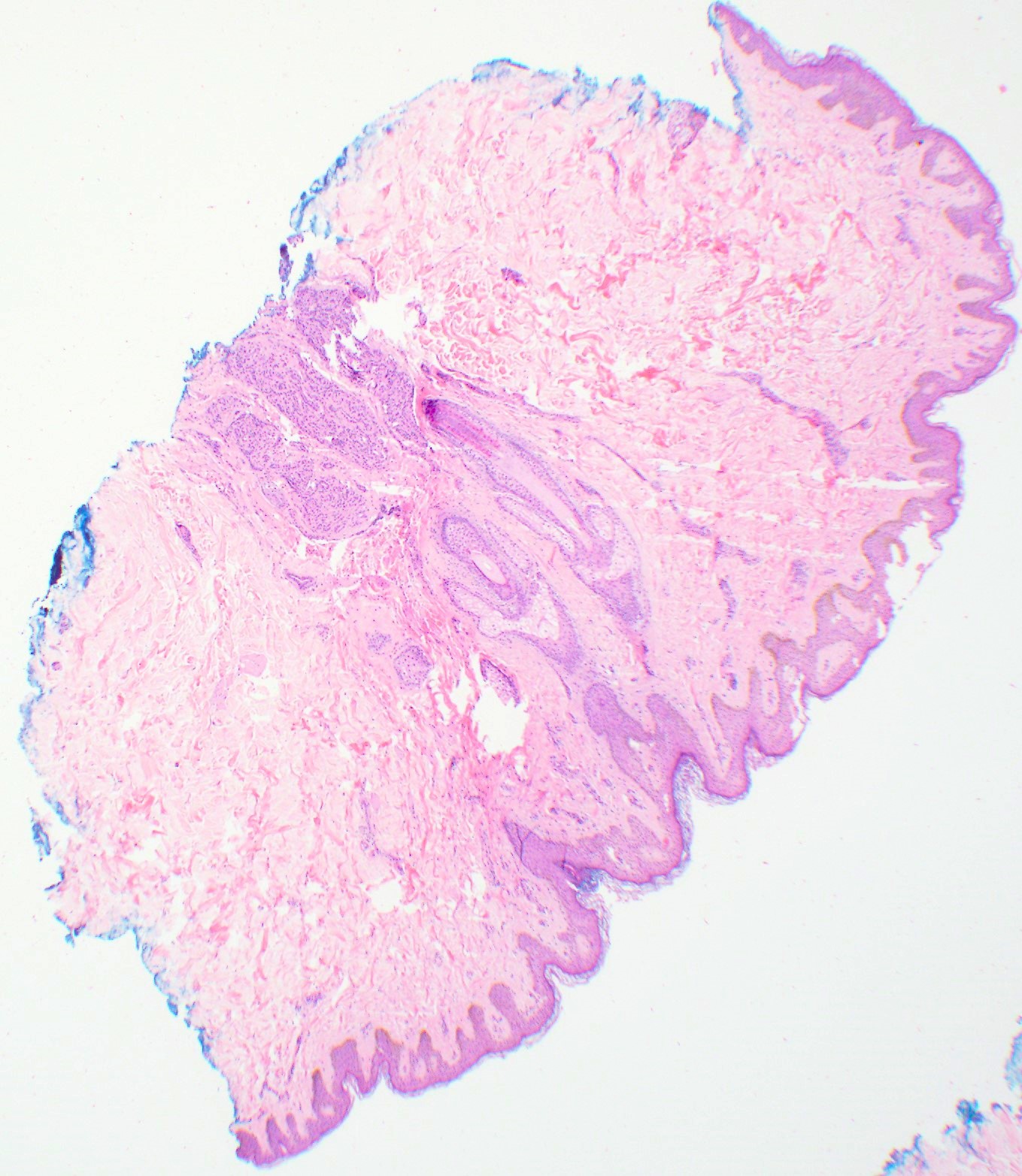
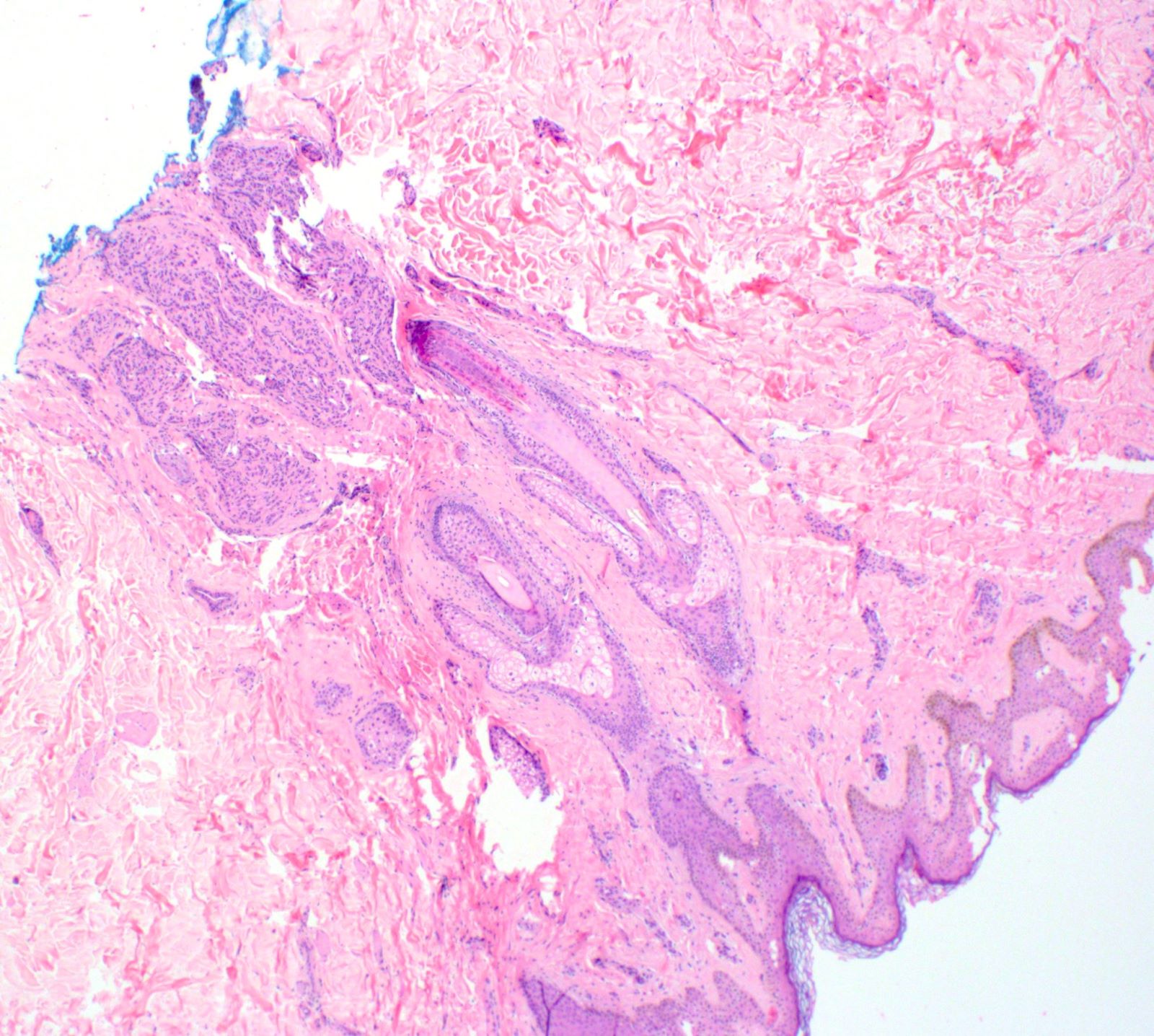
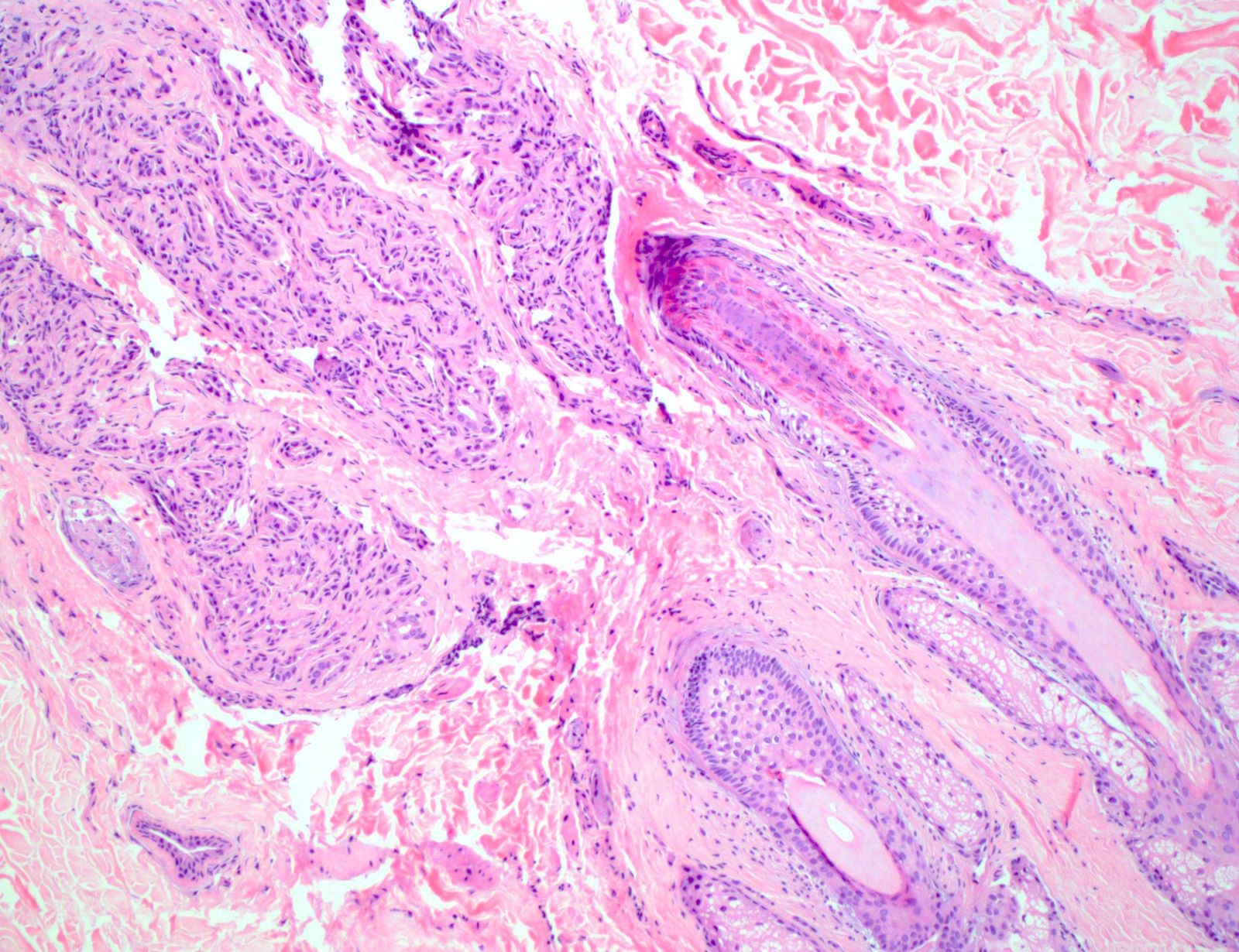
Normal appearing mammary glands
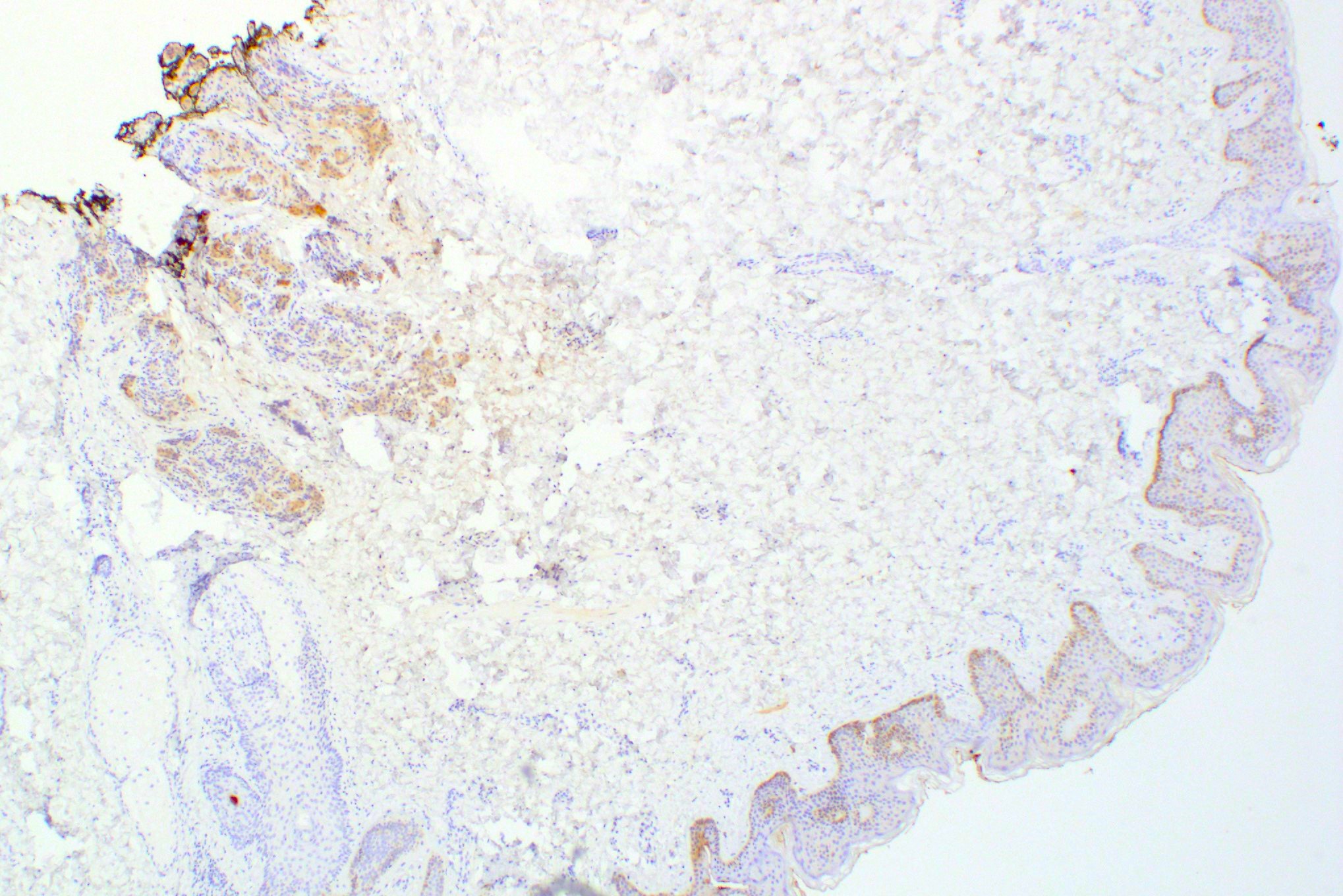
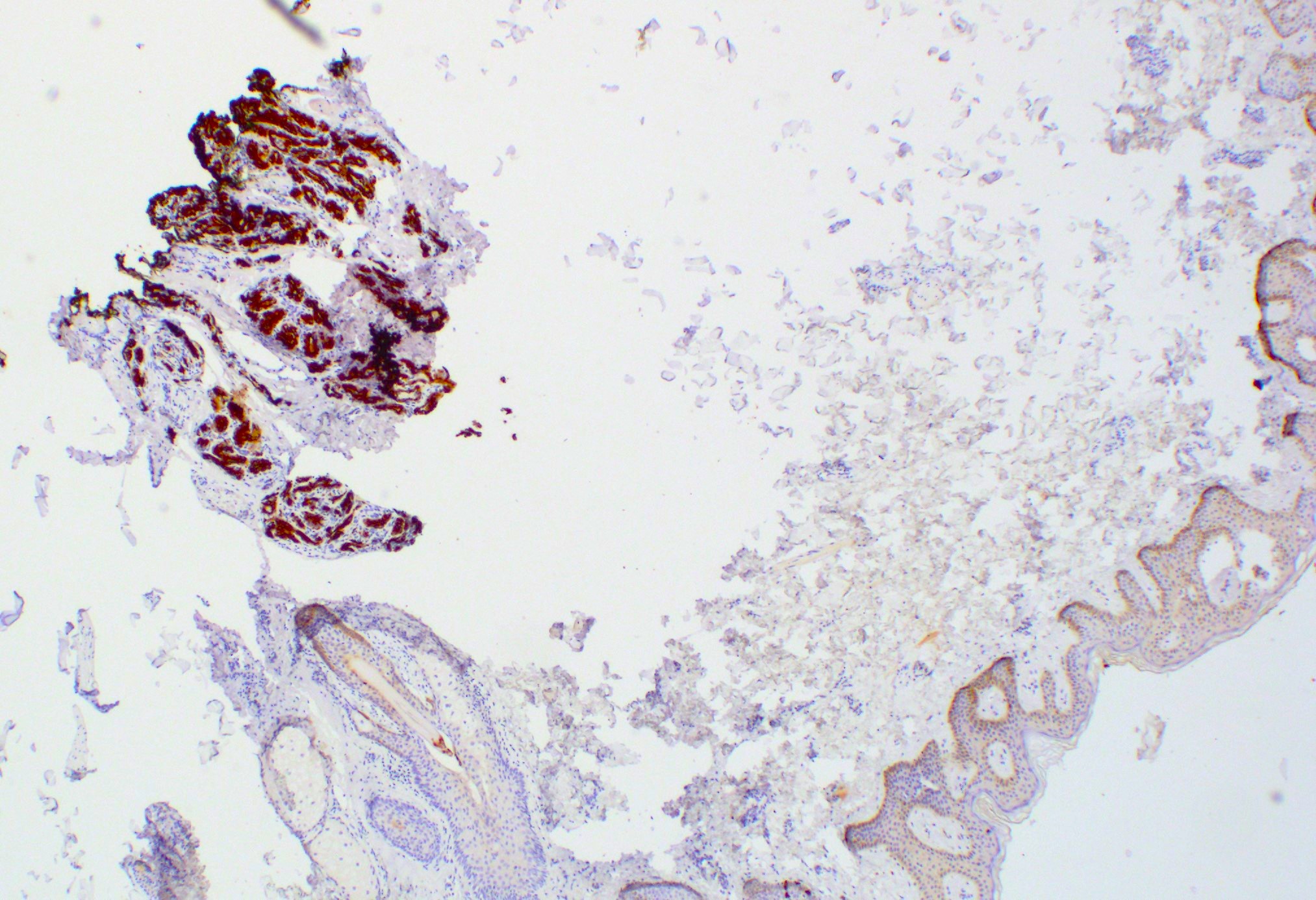
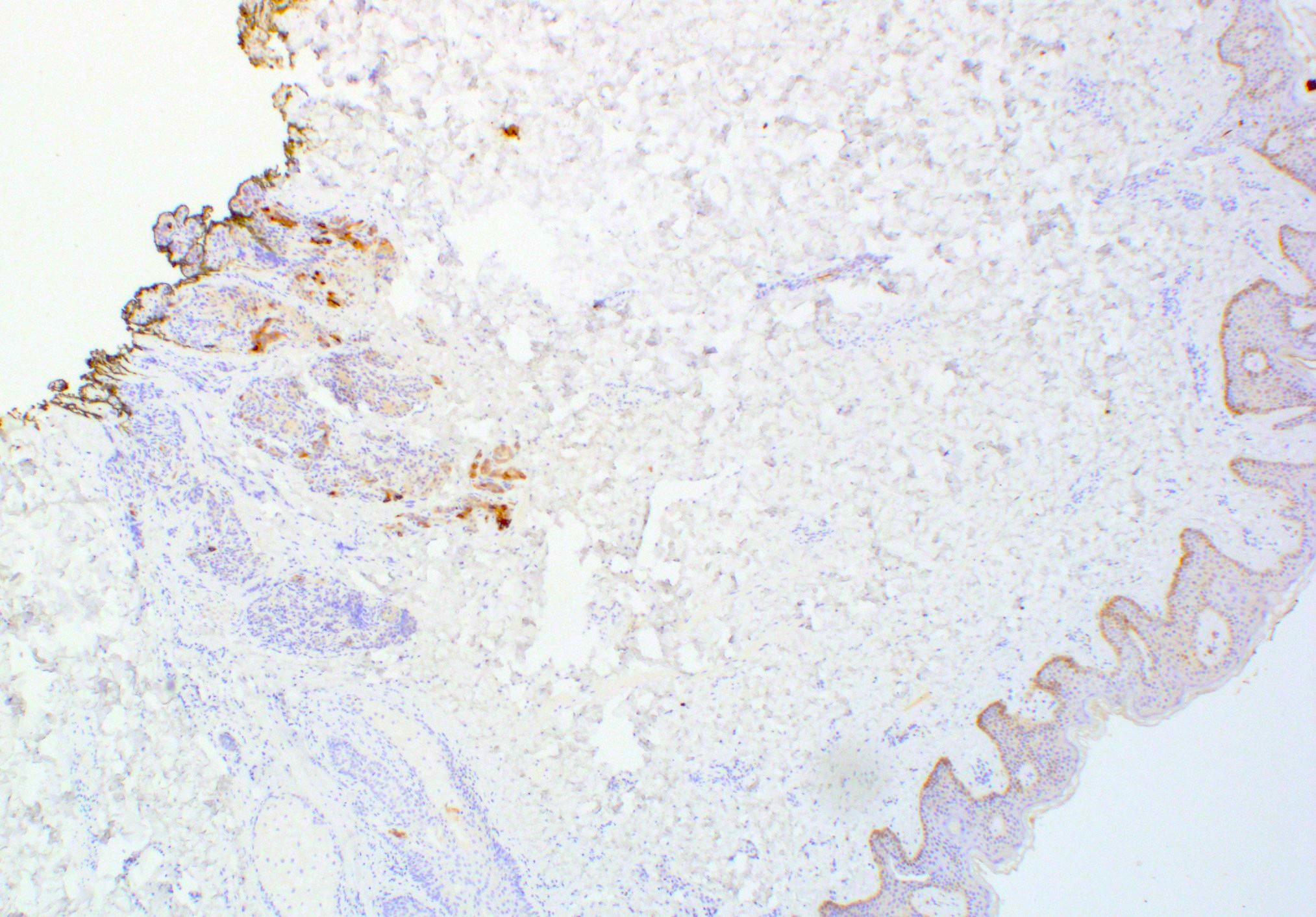
Mammary type glands in the deep dermis
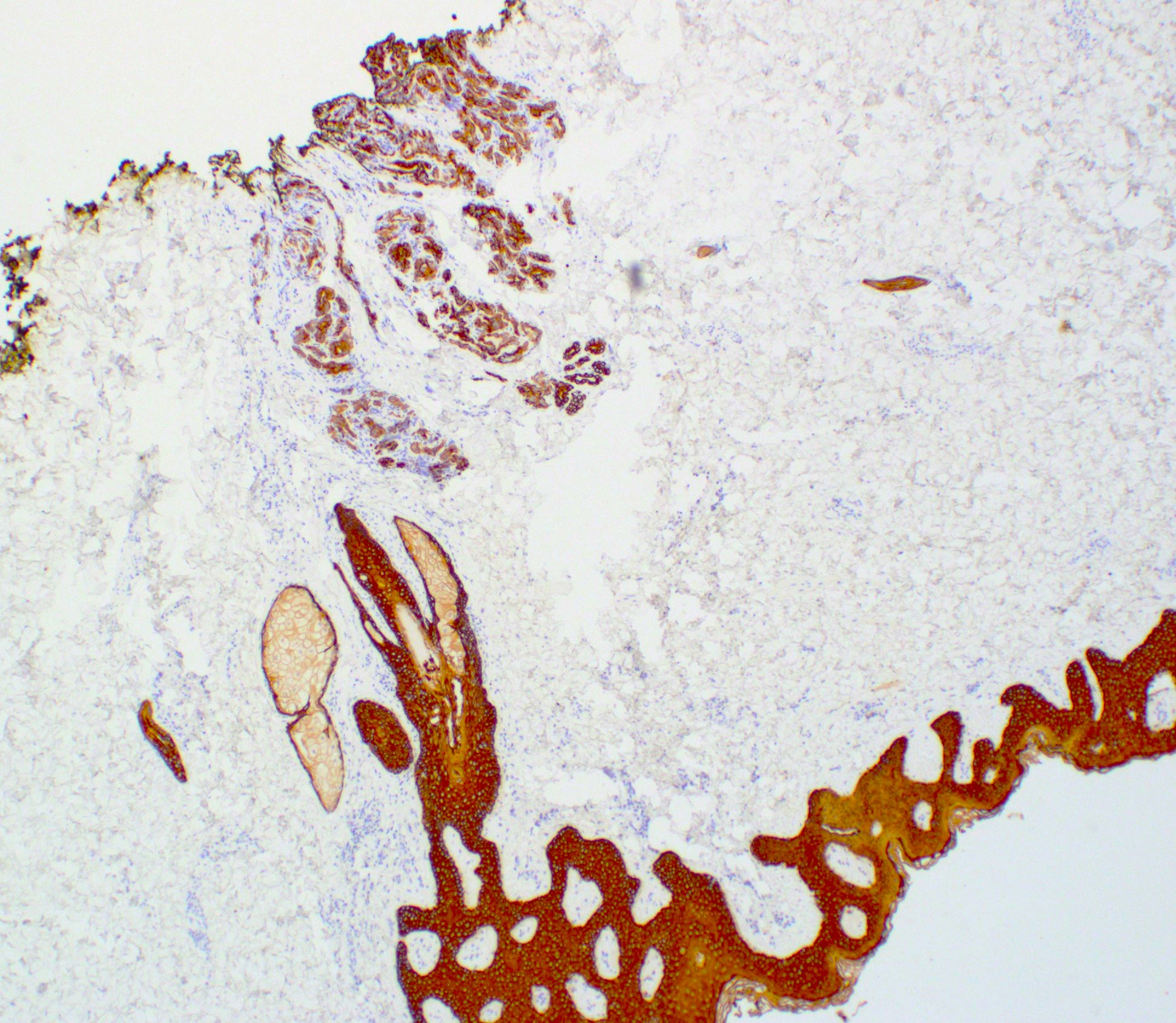

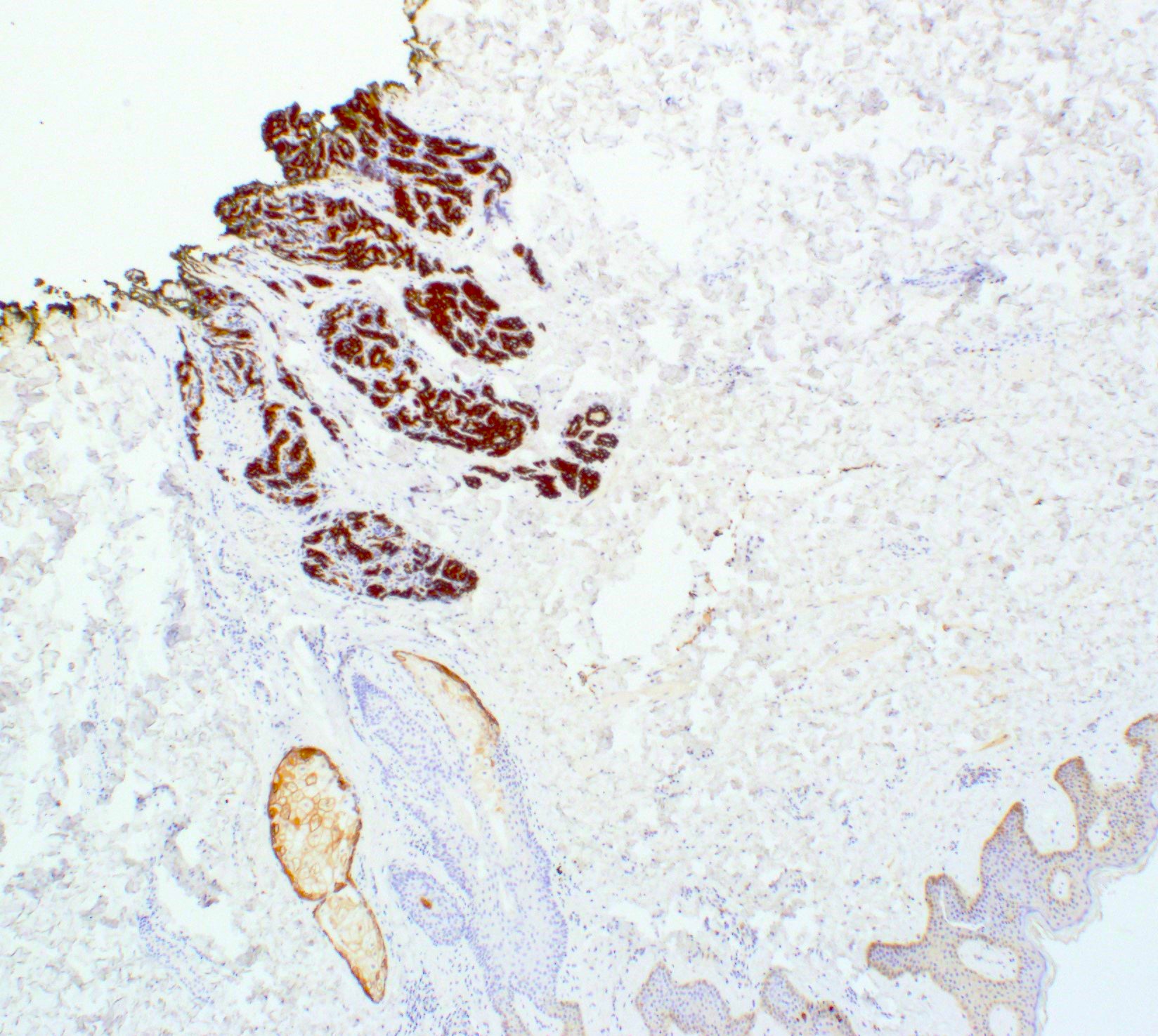
Glands in the deep dermis
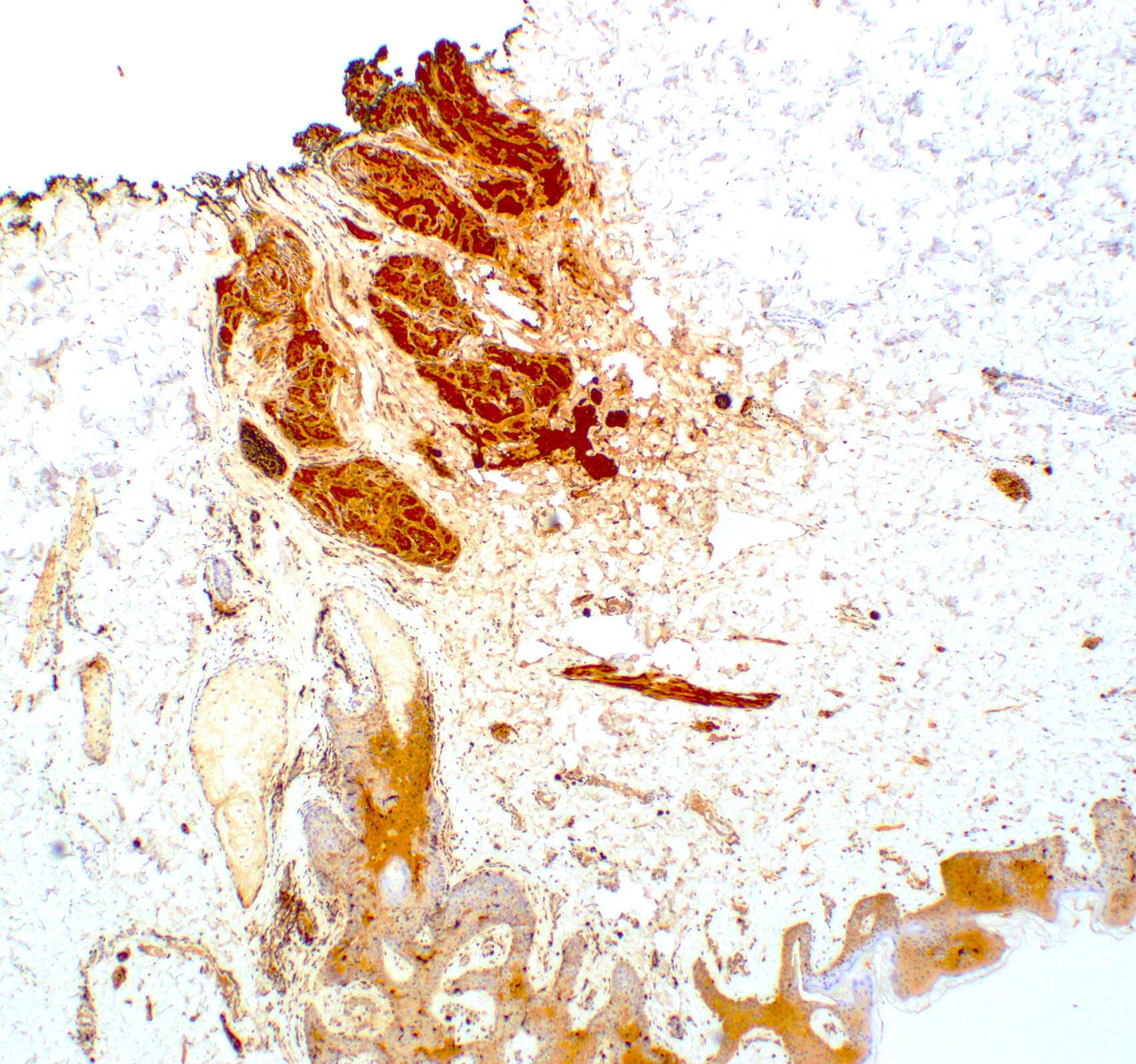
Mammary glands in the dermis
Positive stains
- BRST2, mammaglobin, GATA3, CK7, estrogen receptor in glandular epithelium if present
Videos
Extra nipple under the microscope
Sample pathology report
- Skin lesion, punch biopsy / excision:
- Skin with benign mammary glandular tissue in deep dermis suggestive of accessory breast tissue (see comment)
- Comment: IHC stains of the glands are positive for BRST2, mammaglobin and GATA3, consistent with mammary glands. All controls showed appropriate reactivity.
Differential diagnosis
- Lentigo and melanocytic nevi:
- Show no smooth muscle proliferation and papillomatosis or acanthosis
- Have melanocytic nests with no pilosebaceous structure of Montgomery tubercles
- Lack breast glandular tissue
- Dermatofibroma or fibrous histiocytoma:
- Show fascicular proliferation of fibroblastic cells with bland spindled to histiocytoid shaped cells
- Lack breast glandular tissue
- Positive for factor XIIIa and CD163
- Becker nevus:
- Epidermal acanthosis with increased basal cell layer pigmentation due to benign melanocyte hyperplasia
- Lacks breast glandular tissue
- Smooth muscle hamartoma:
- Increased, irregular, dermal smooth muscle bundles that are not associated with hair follicles or sebaceous glands
- Lacks breast glandular tissue
Board review style question #1
Which of the following statements is true regarding supernumerary breast?
- Develops during the fifteenth week of gestation along the milk line
- Ectopic breast tissue never demonstrates breast cancer
- Mammary ridge involutes during the fifth week of gestation
- Varies by ethnicity with highest prevalence in Japanese population
Board review style answer #1
D. The accessory breast tissue varies by ethnicity with highest prevalence in Japanese population and the lowest in white populations. Answer A is incorrect because the milk line forms during the fifth week of gestation. Answer B is incorrect because ectopic breast tissue can give rise to malignancy. Answer C is incorrect because the mammary ridge involutes during the fifteenth week of gestation.
Comment Here
Reference: Supernumerary / accessory tissue
Comment Here
Reference: Supernumerary / accessory tissue
Board review style question #2
Patients with the lesions shown in the image above have increased risk of which of the following malignancies?
- Dermatologic malignancies
- Gastrointestinal malignancies
- Genitourinary malignancies
- Gynecologic malignancies
- Sarcomas of the bone
Board review style answer #2
C. Genitourinary malignancies. Supernumerary nipples have been reported to be associated with increased incidence of genitourinary malignancies and pediatric hematologic disorders (Pediatr Hematol Oncol 2004;21:461). Answers A, B, D and E are incorrect because these conditions can occur in the supernumerary breast tissue, just as in the general population. This means that supernumerary breast tissue does not increase the risk of malignancies other than genitourinary malignancies.
Comment Here
Reference: Supernumerary / accessory tissue
Comment Here
Reference: Supernumerary / accessory tissue
