Skin nonmelanocytic tumor
Fibrous, fibrohistiocytic and myofibroblastic neoplasms
Dermatofibroma (cutaneous fibrous histiocytoma)

Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Benign fibrous histiocytoma
- Dermatofibromas (also known as fibrous histiocytomas) are a spectrum of benign dermal based lesions with fibroblastic and histiocytic differentiation
- There is debate as to whether dermatofibroma is a reactive or neoplastic process
- Benign dermal based, nodular proliferation of fibroblasts and histiocytes
- Collagen trapping at periphery and follicular induction commonly seen
- IHC is nonspecific for dermatofibroma
- Benign fibrous histiocytoma and fibrous histiocytoma
- Common
- All races
- All ages; most common in third and fourth decades
- F > M
- Reference: Am J Surg Pathol 1990;14:801
- Typically occurs on distal extremities (legs > arms > trunk)
- May present on any part of the skin surface
- Cause unknown
- No evidence associates it with insect bites or trauma
- Unclear whether a reactive or neoplastic process
- Cytogenetic data has shown clonality, arguing in favor of a neoplastic process (J Cutan Pathol 2000;27:36, Histopathology 2000;37:212)
- Multiple dermatofibromas may occur in immunosuppressed populations (Eur J Dermatol 1999;9:45)
Images hosted on other servers:

Various presentations under dermoscopy
- Painless
- 5 mm - 2 cm
- Variable color: skin colored to brown to purple
- Variable shape: plaques, nodules or polyps
- Covered by intact skin
- Suspected by pinching the nodule between the fingers and observing that the tumor is fixed within the dermis
- Pinch sign: overlying skin dimples on pinching the lesion (An Bras Dermatol 2014;89:472)
- Combination of clinical and histologic findings
- Excellent prognosis (Am J Surg Pathol 1990;14:801)
- Cellular, atypical, aneurysmal and deep subtypes associated with higher risks of local recurrence (Am J Surg Pathol 1994;18:668, Eur J Dermatol 1998;8:122)
- Very rarely metastasize (Am J Surg Pathol 2008;32:354, Am J Surg Pathol 2002;26:35, Mod Pathol 2013;26:256)
- 2 young children with tumors of skin and conjunctiva and coexisting xeroderma pigmentosum (Arch Pathol Lab Med 1991;115;910)
- 19 year old man with corneoscleral tumor (Br J Ophthalmol 2002;86:477)
- 25 year old man with cystic lesion on calf (Cureus 2020;12:e6736)
- 25 year old man with external auditory canal tumor (Ear Nose Throat J 2019;98:396)
- 36 year old woman with blue-gray pigmented lesion (An Bras Dermatol 2017;92:92)
- 40 year old woman with multiple dermatofibromas associated with pregnancy (Dermatol Online J 2019;25:13030)
- 42 year old man with swelling over the occipital region (J Clin Diagn Res 2017;11:ED08)
- 43 and 48 year old women and 60 year old man with conditions associated with multiple dermatofibromas (Dermatol Online J 2017;23:13030)
- 51 year old woman with swelling of lower jaw (J Clin Diagn Res 2016;10:ZD24)
- 62 year old woman with unusual presentation of dermatofibroma on the face (Clin Case Rep 2019;7:672)
- 85 year old man with lump on his back (Int J Surg Case Rep 2019;60:299)
- Complete excision is curative
- Wide local excision is adequate to prevent recurrence
- Spontaneous regression has been reported
Images hosted on other servers:


Dermatofibroma of the skin


Dermatofibroma of the skin

Pinch sign of dermatofibroma

Hyperpigmented dermatofibroma

Numerous eruptive dermatofibromas

Dermatofibroma of the lower lip

Dermatofibroma presenting as eruptive papules

Dermatofibroma of the shoulder



Patterns of dermatofibroma

Vascular structures in dermatofibromas

Other dermoscopic structures
- Most classic pattern: pigment network and central white patch
- Wide range of presentations
Images hosted on other servers:

Polypoid, ulcerated mass
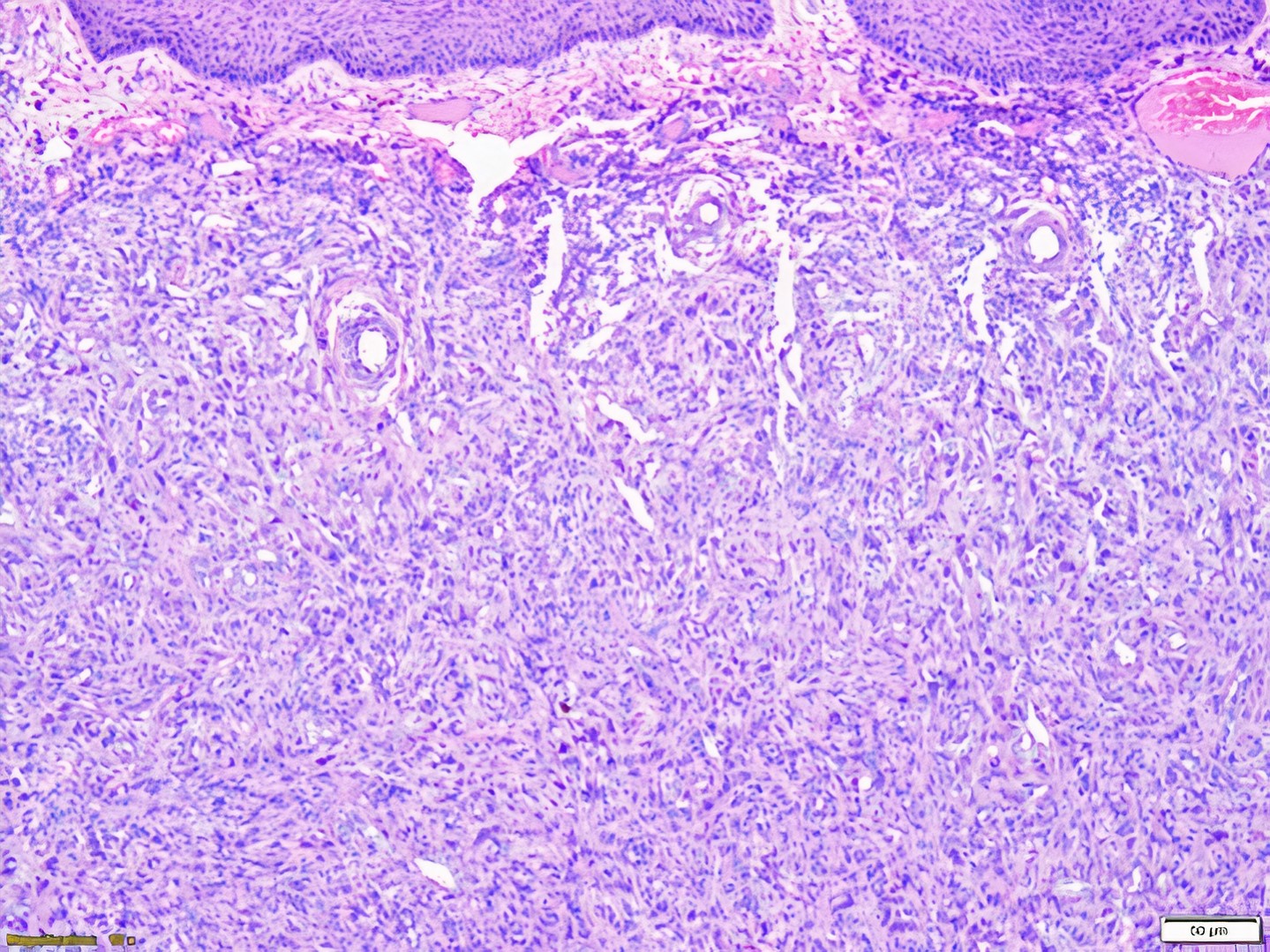
- Symmetric and predominantly dermal based
- Relatively circumscribed but have irregular and unencapsulated borders
- Patterns range from diffuse to reticular to hemangioma-like to keloid-like
- Classic pattern: storiform, pinwheel or curlicue pattern
- Made up of spindled fibroblasts or histiocytes
- Some areas densely cellular, while others are sclerotic and hypocellular
- Early lesions: more cellular
- Later lesions: more sclerotic
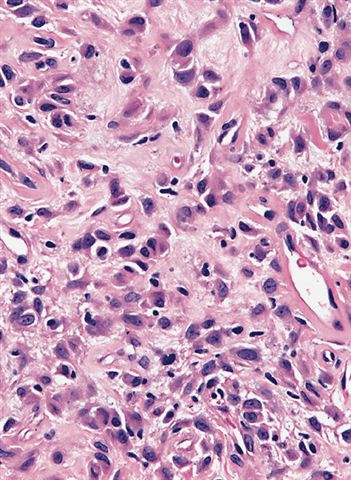
- Spindled cells: thin, elongated nuclei with pointed ends and eosinophilic cytoplasm
- Histiocytic cells: epithelioid shaped cells with abundant pale cytoplasm
- May see varying amounts of inflammatory cells
- Cytologic atypia and pleomorphism are variable
- Mitotic activity is variable
- Touton giant cells and ringed lipidized siderophages may be present
- Collagen trapping at periphery
- Spheres of eosinophilic collagen (collagen balls) surrounded by the fibroblast proliferation
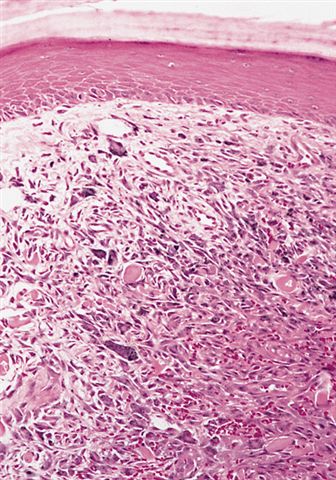
- Grenz zone (sparing of the superficial papillary dermis) commonly seen
- Follicular or sebaceous induction and basilar hyperpigmentation
- Tumor may extend into superficial fat
- Numerous histological subtypes (An Bras Dermatol 2014;89:472):
- Aneurysmal and hemosiderotic variants are both characterized by numerous multinucleate cells and prominent hemosiderin deposition due to red blood cell extravasation; distinction between these two is the pseudovascular spaces with blood in aneurysmal type (Histopathology 1995;26:323)
- Hemosiderotic frequently has extracellular hemosiderin pigmentation present
- Deep fibrous histiocytoma: may extend into hypodermis (Am J Surg Pathol 2008;32:354)
- Cellular: highly cellular and look blue at low power with thick collagen bundles (Am J Surg Pathol 1994;18:668)
- Lipidized: also known as 'ankle type' Am J Dermatopathol 2000;22:126
- Atypical: also has prominent pleomorphism, mitotic activity including atypical forms (Am J Dermatopathol. 1987 Oct;9(5):380)
- Epithelioid fibrous histiocytoma: epidermal collarette, binucleate cells (Mod Pathol 2015;28:904)
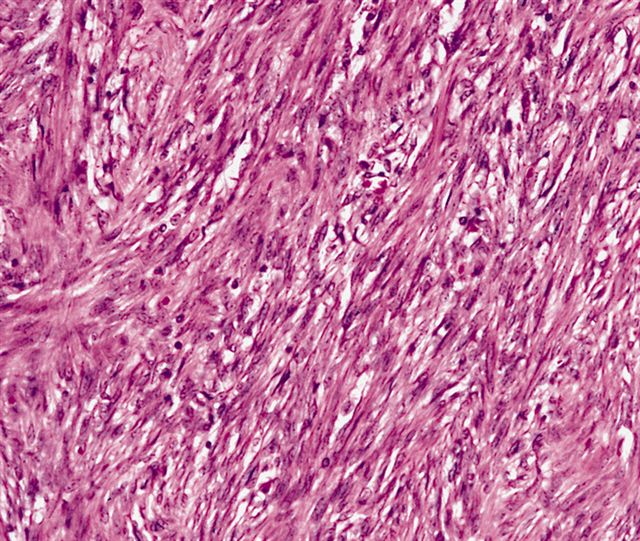
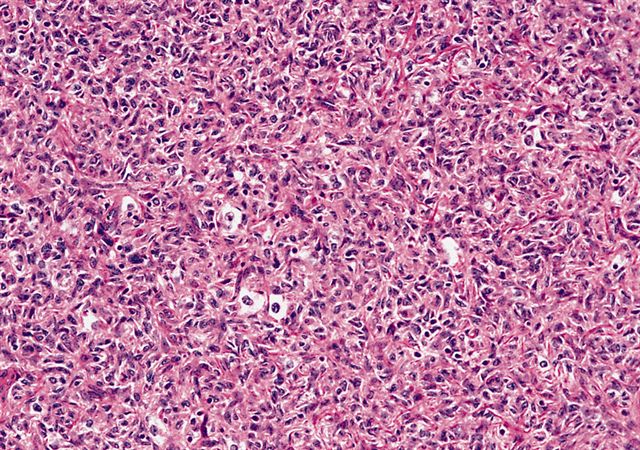
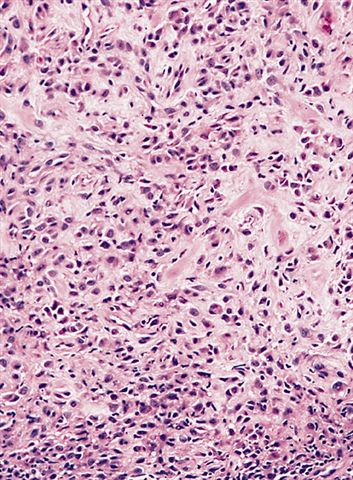
Contributed by Brandon Zelman, D.O. and Jodi Speiser, M.D.
Spindled fibroblasts and epithelioid histiocytes
Dermal based proliferation
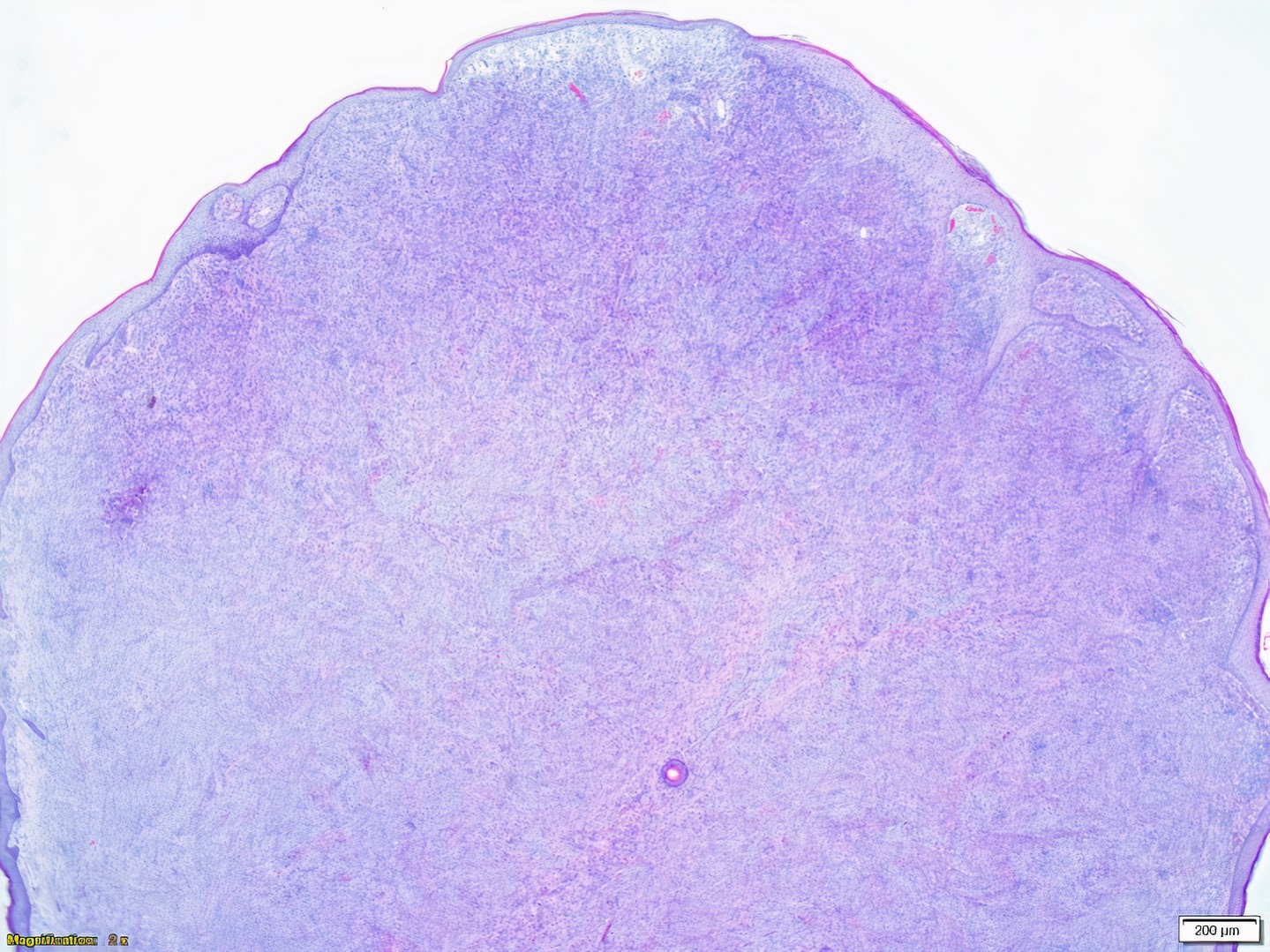
Dermal proliferation

Whirled appearance
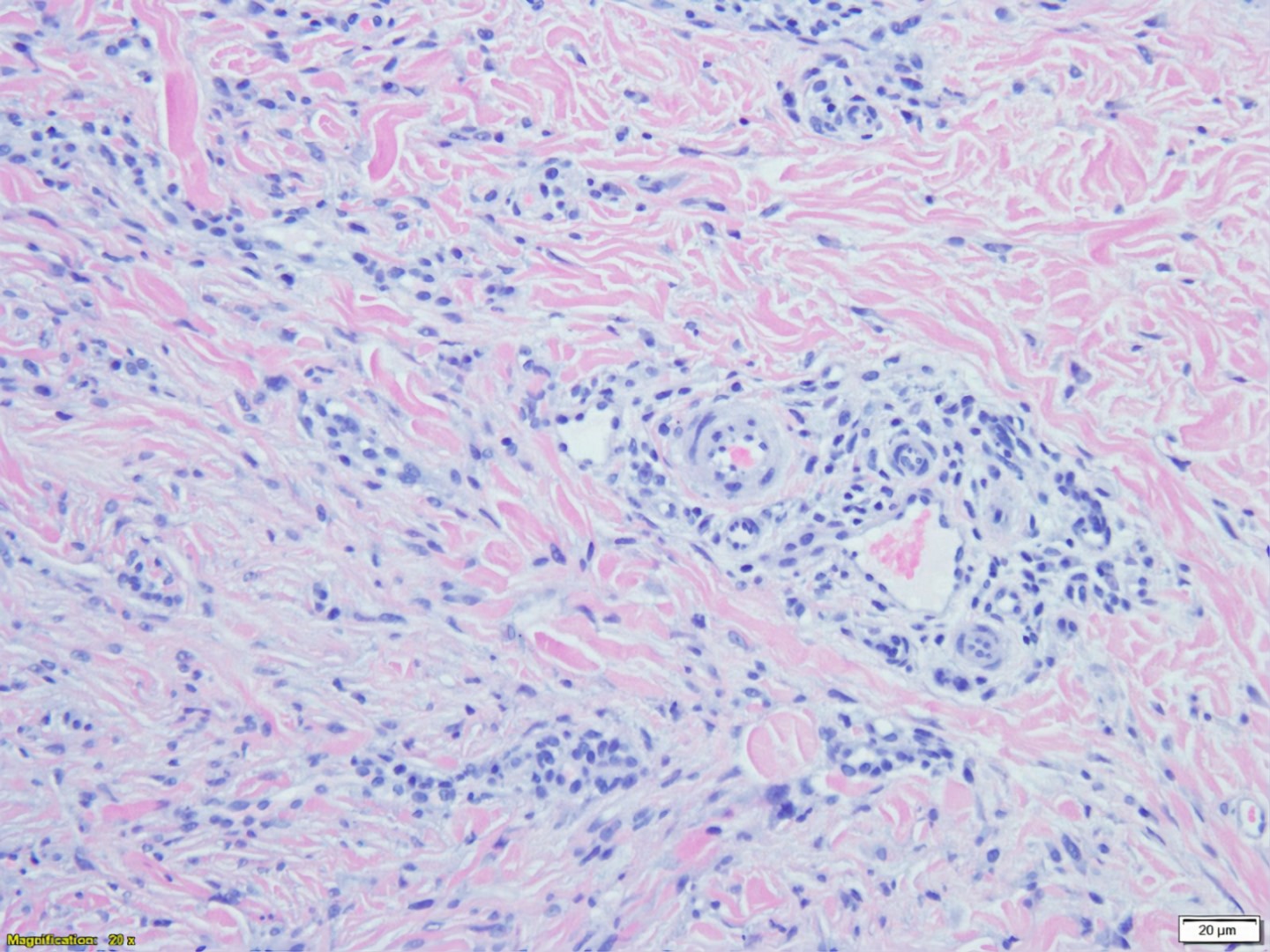
Collagen trapping
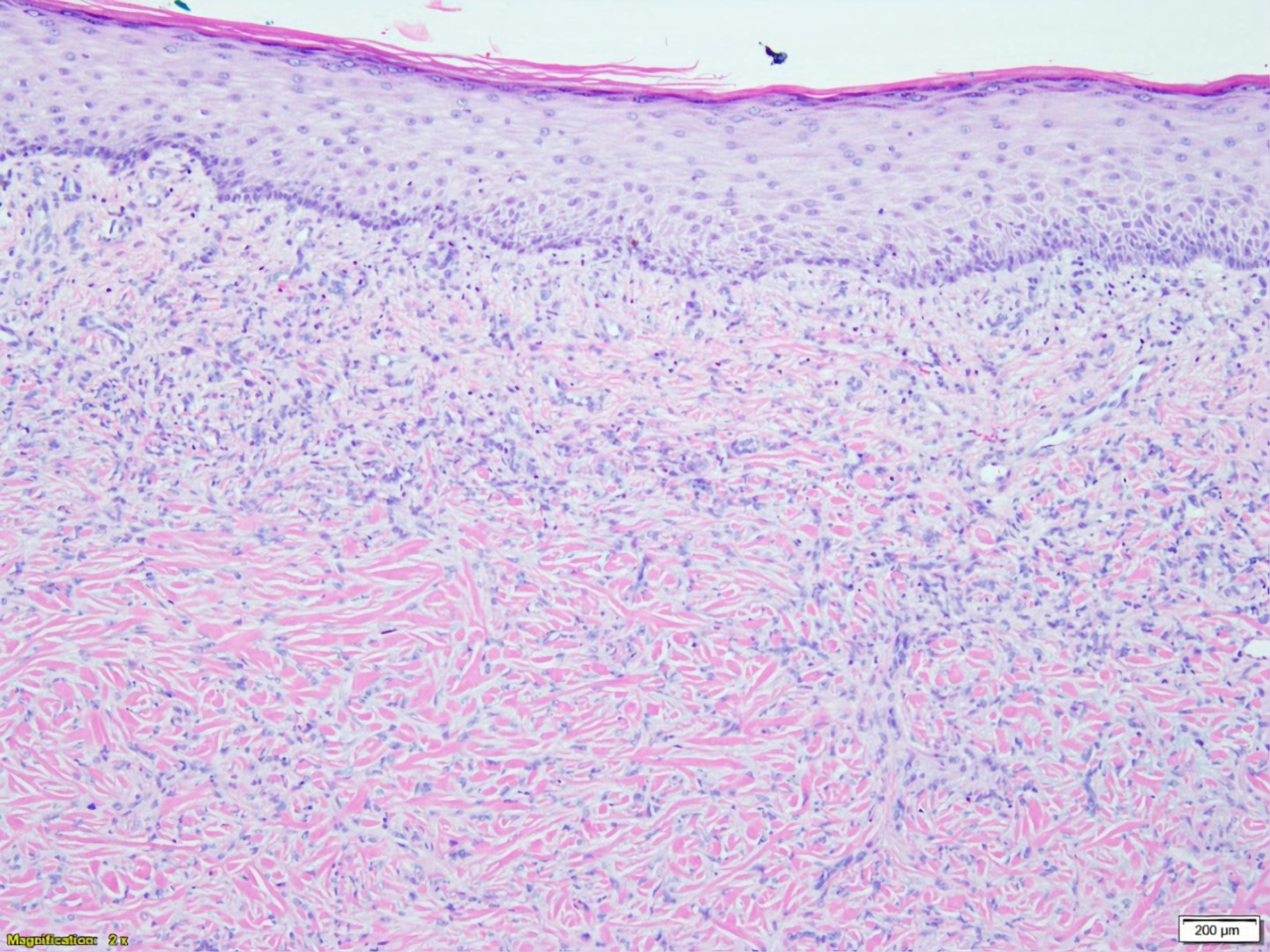
Increased cellularity and collagen trapping
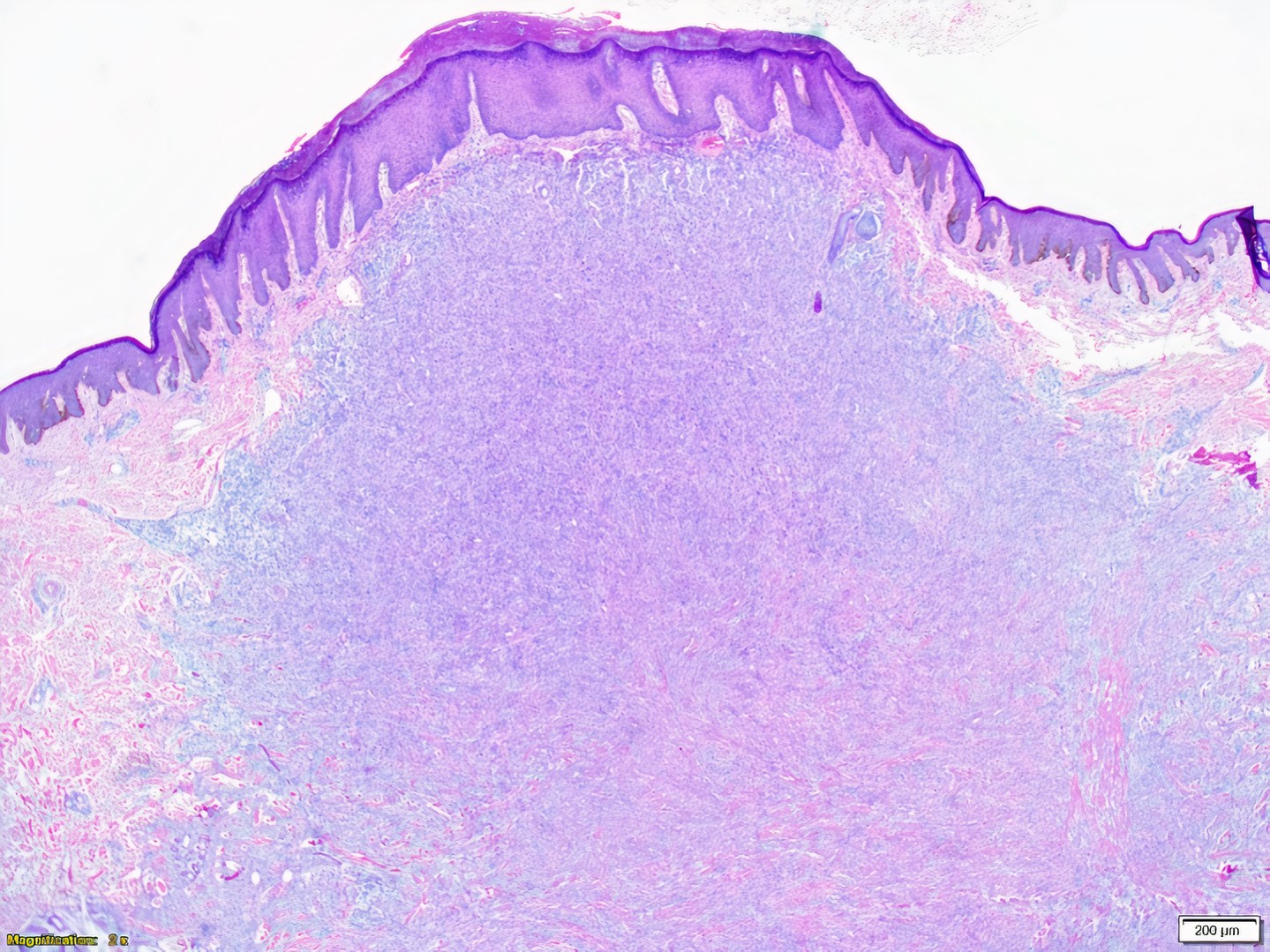
Dermal based proliferation that appears busy
Increased dermal cellularity
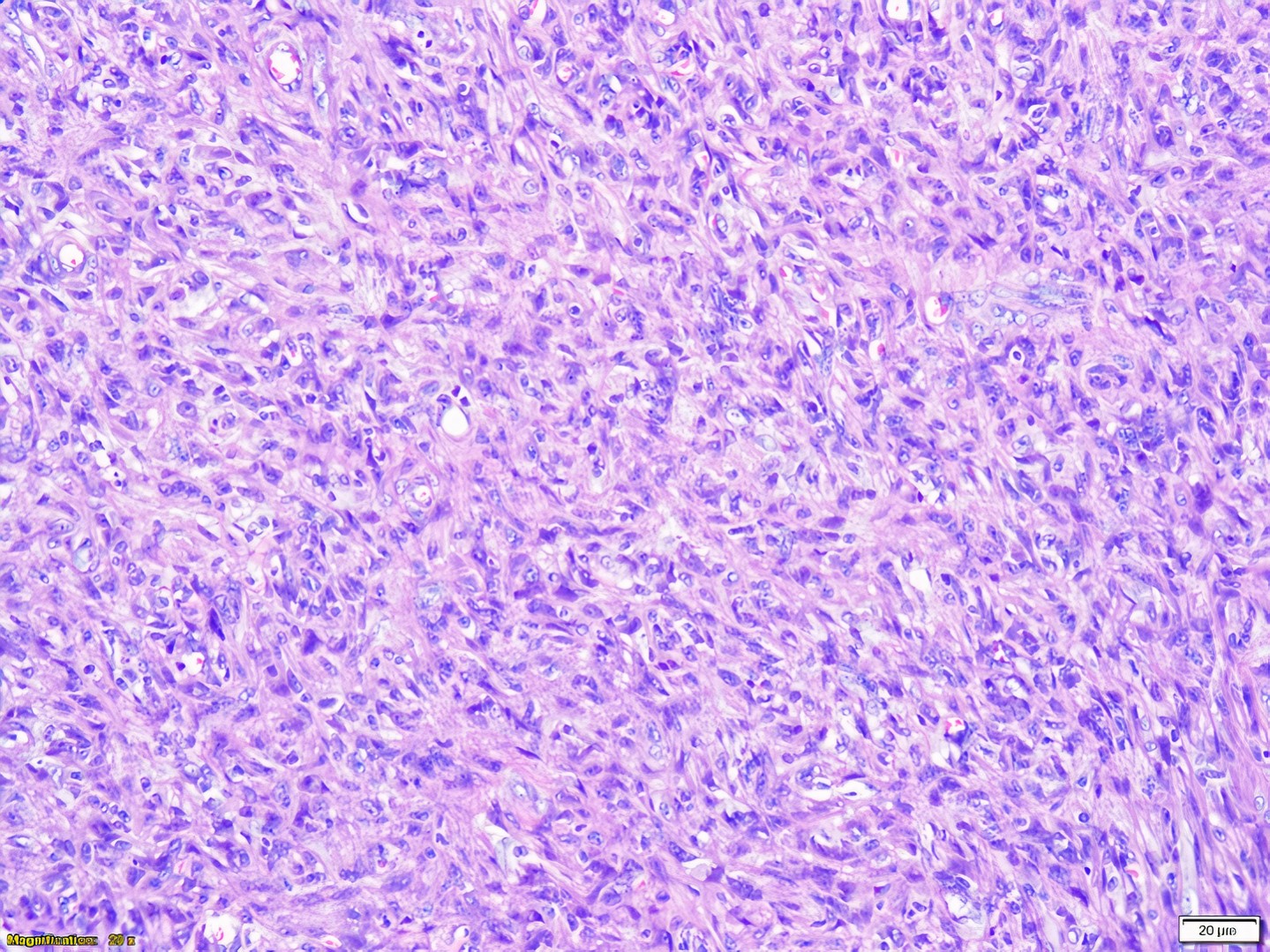
Spindled fibroblasts and epithelioid histiocytes
CD34-
CD10+
Keratin-
S100-

SMA weakly expressed
CD34-
CD10+
AFIP images
Aneurysmal
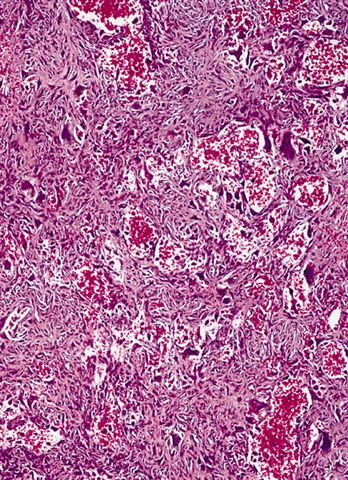
Nonendothelial lined clefts or lakes containing blood
Large amounts of hemosiderin

Hemosiderin with marked sclerosis
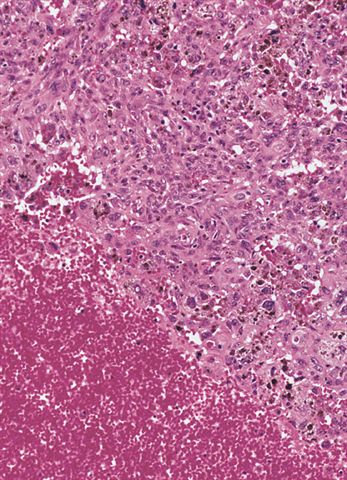
Cellular

More cellular than classic fibrous histiocytoma
Elongated cells are arranged in fascicles or a storiform pattern
Tumor cells are more histiocyte like and foam cells are present
Epithelioid
Histiocyte-like cells with abundant cytoplasm, no / rare spindle cells
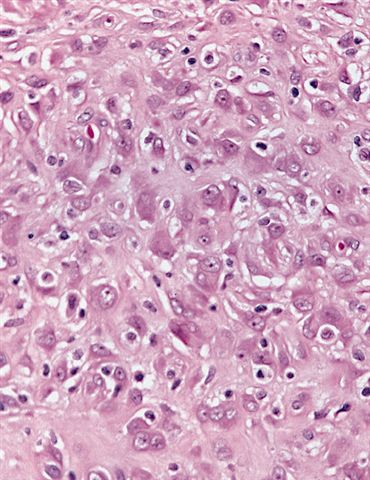
Epithelioid cells in hyalinized stroma
Images hosted on other servers:

Dermatofibroma
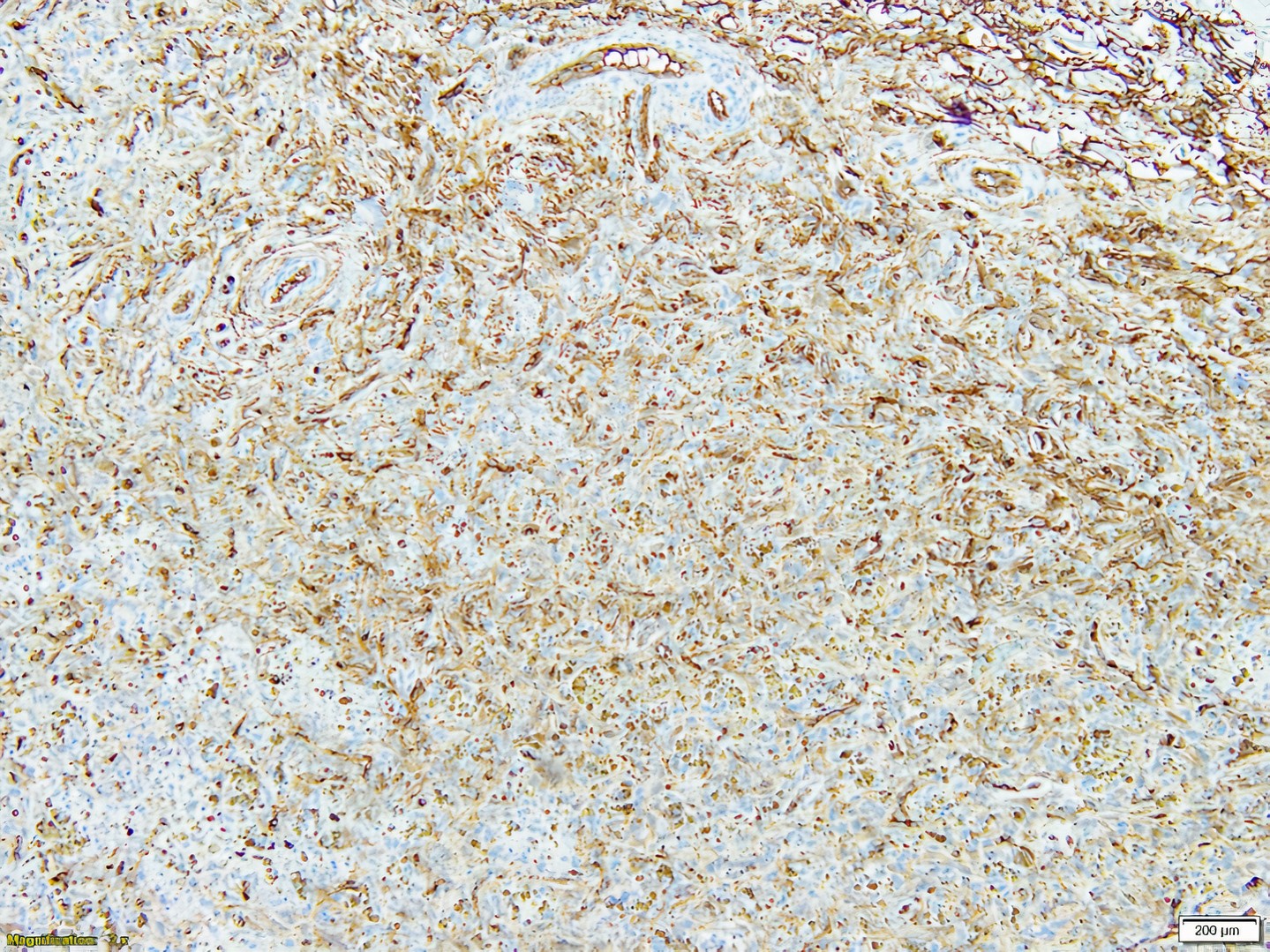
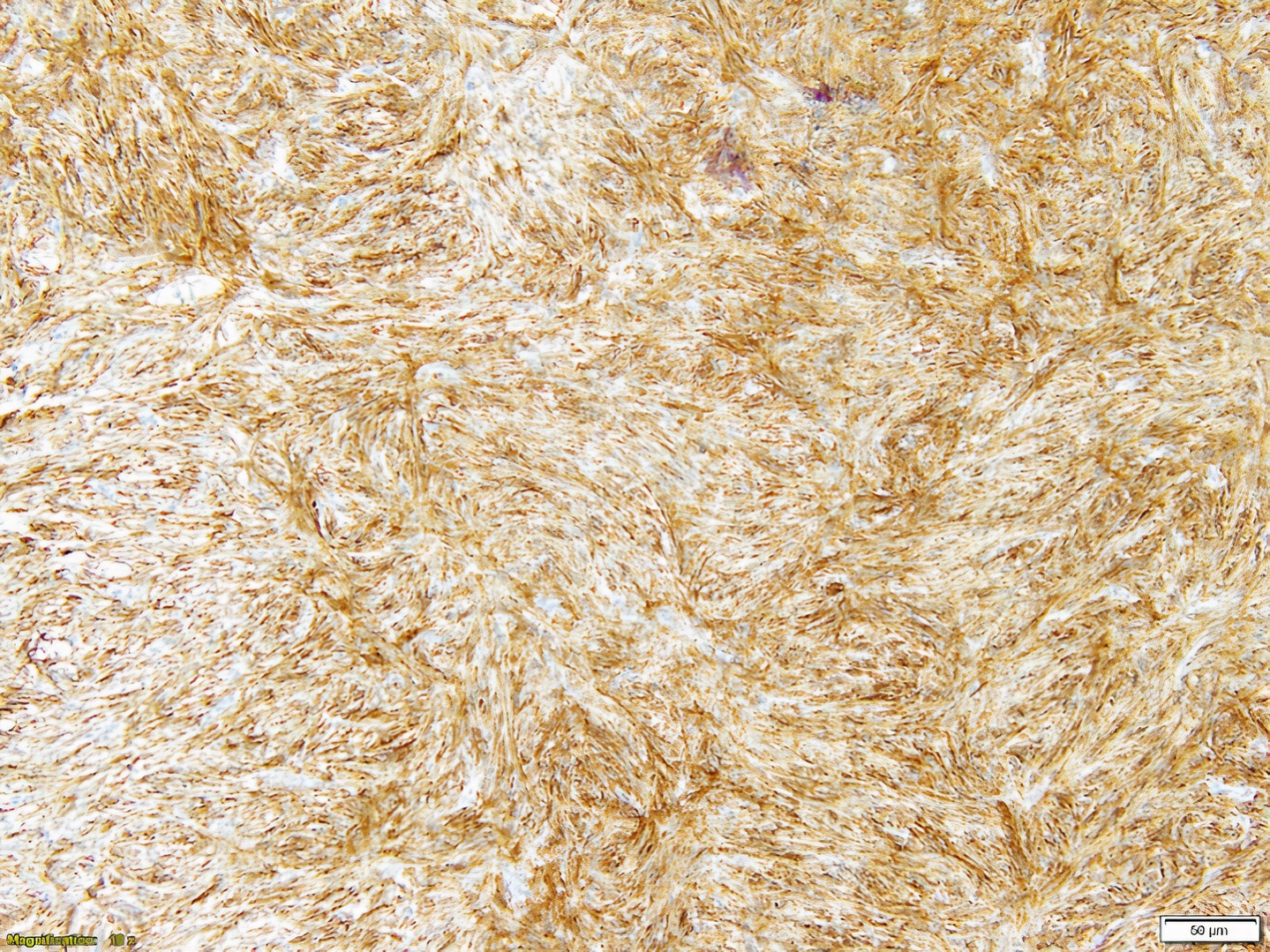
- Most useful stain based on evidence is CD163; factor XIIIa is variable in dermatofibroma; CD68 and CD10 are less specific for fibrohistiocytic lineage
- Ki67 and PHH3 can also be used to show increased proliferation index in dermatofibroma (compared to low index in dermatofibrosarcoma protuberans) (Am J Dermatopathol 2017;39:504)
- ALK nuclear and cytoplasmic reactivity in epithelioid fibrous histiocytoma due to ALK rearrangement and overexpression
- Staining pattern is highly variable and nonspecific but the following stains may be positive:
- Factor XIIIa, CD163, CD10
- Factor XIIIa is usually negative in dermatofibrosarcoma protuberans
- CD68 may highlight histiocytic cells (Patterson: Weedon's Skin Pathology, 5th Edition, 2020)
- Factor XIIIa, CD163, CD10
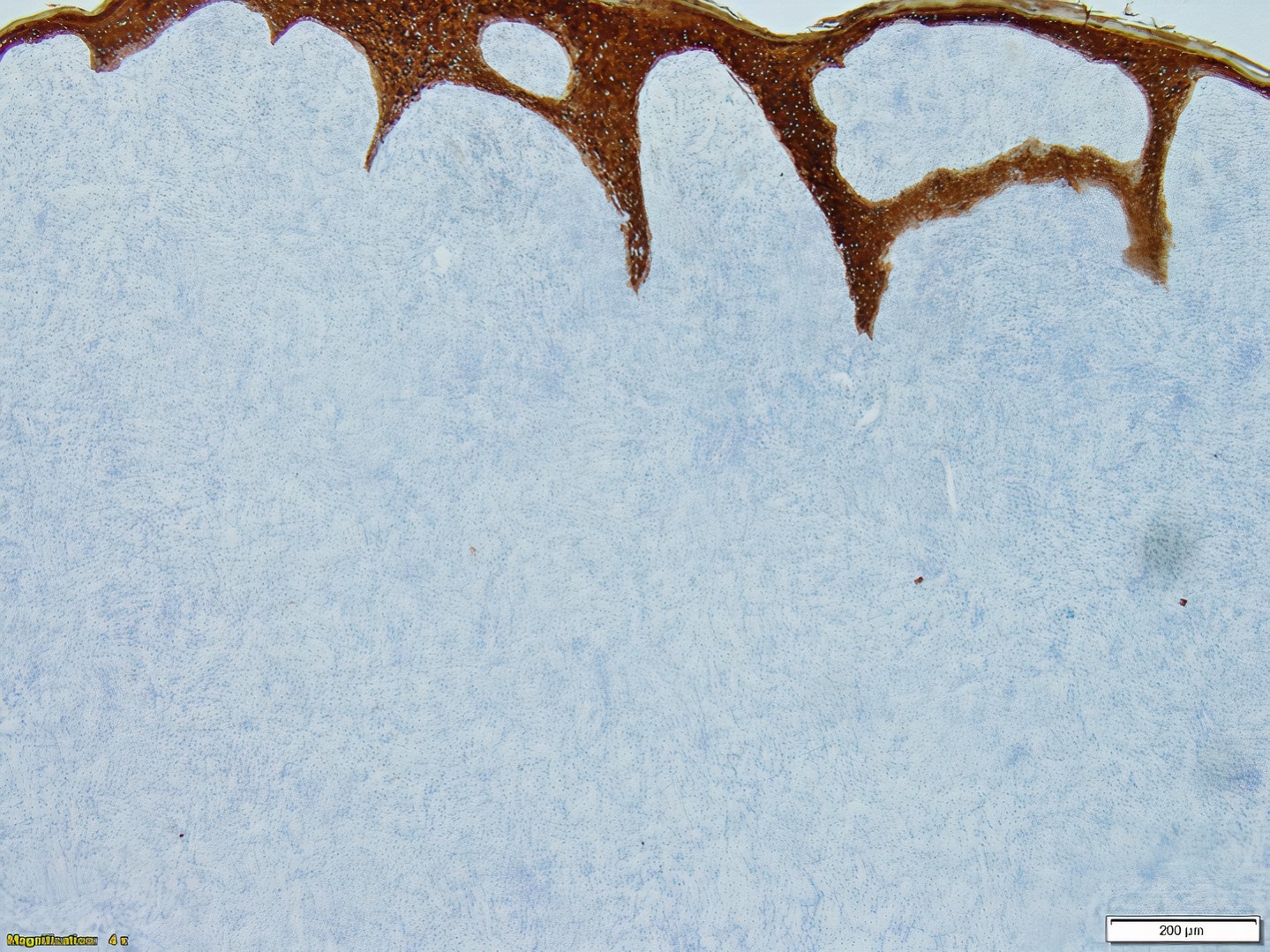
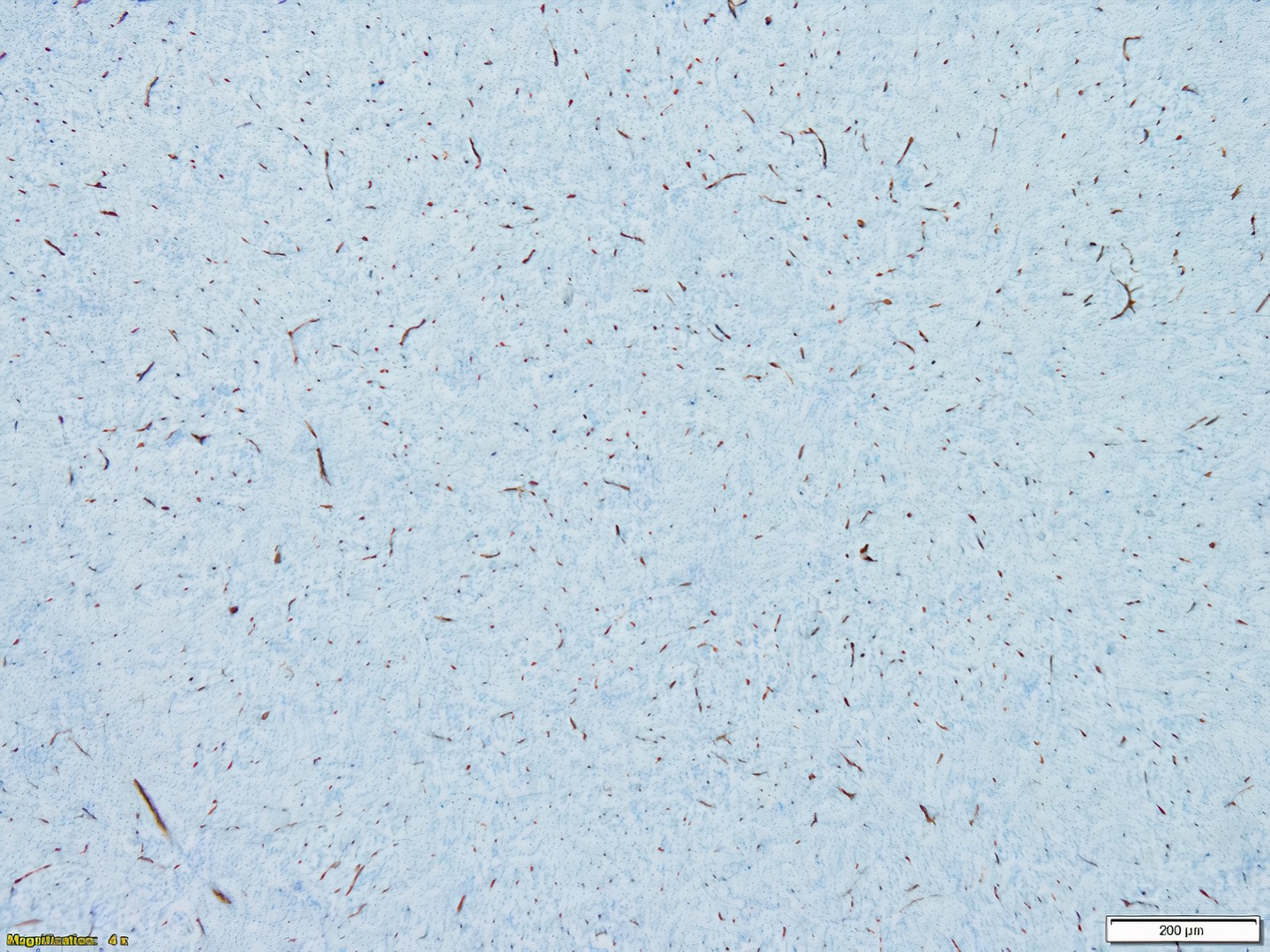
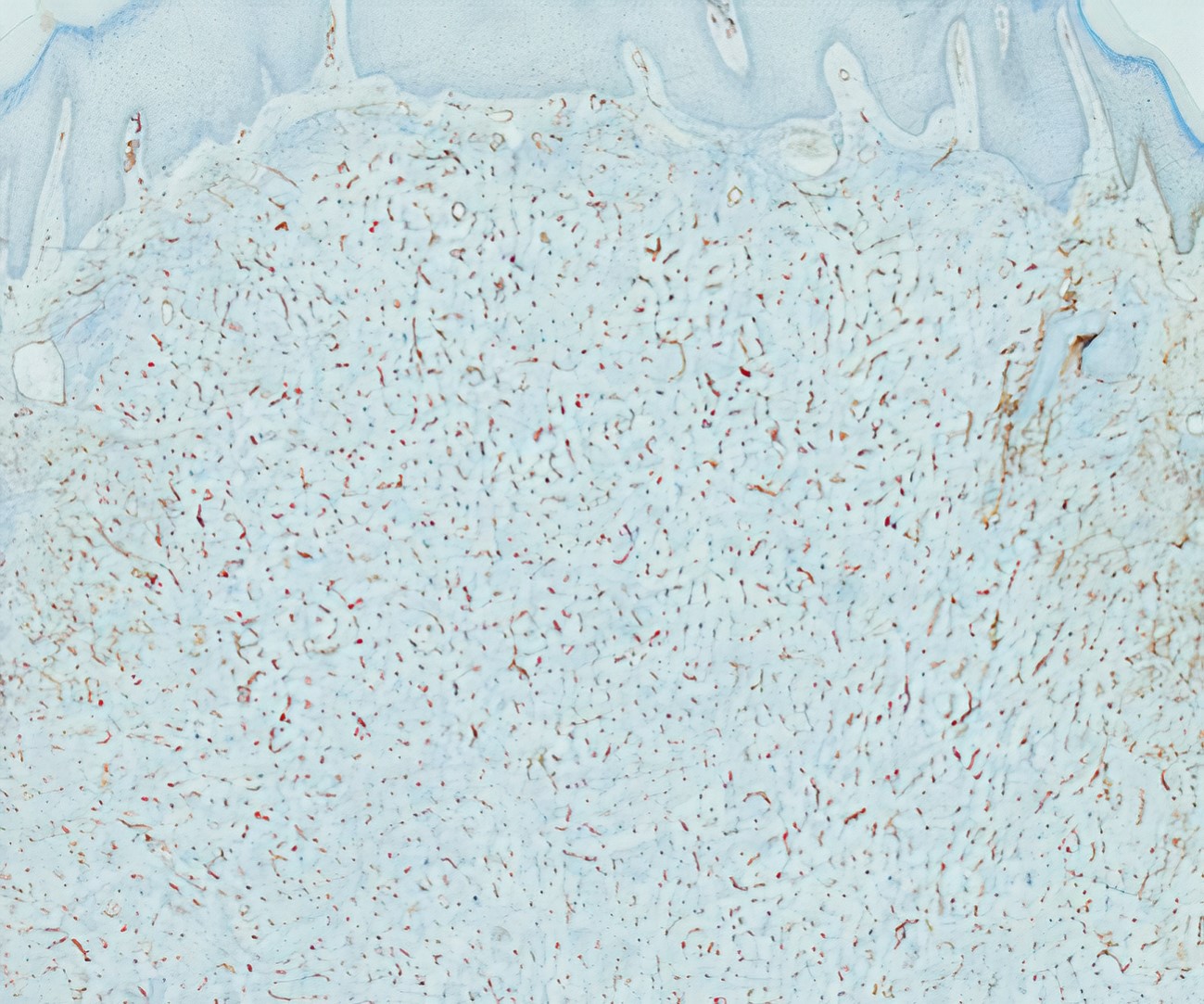
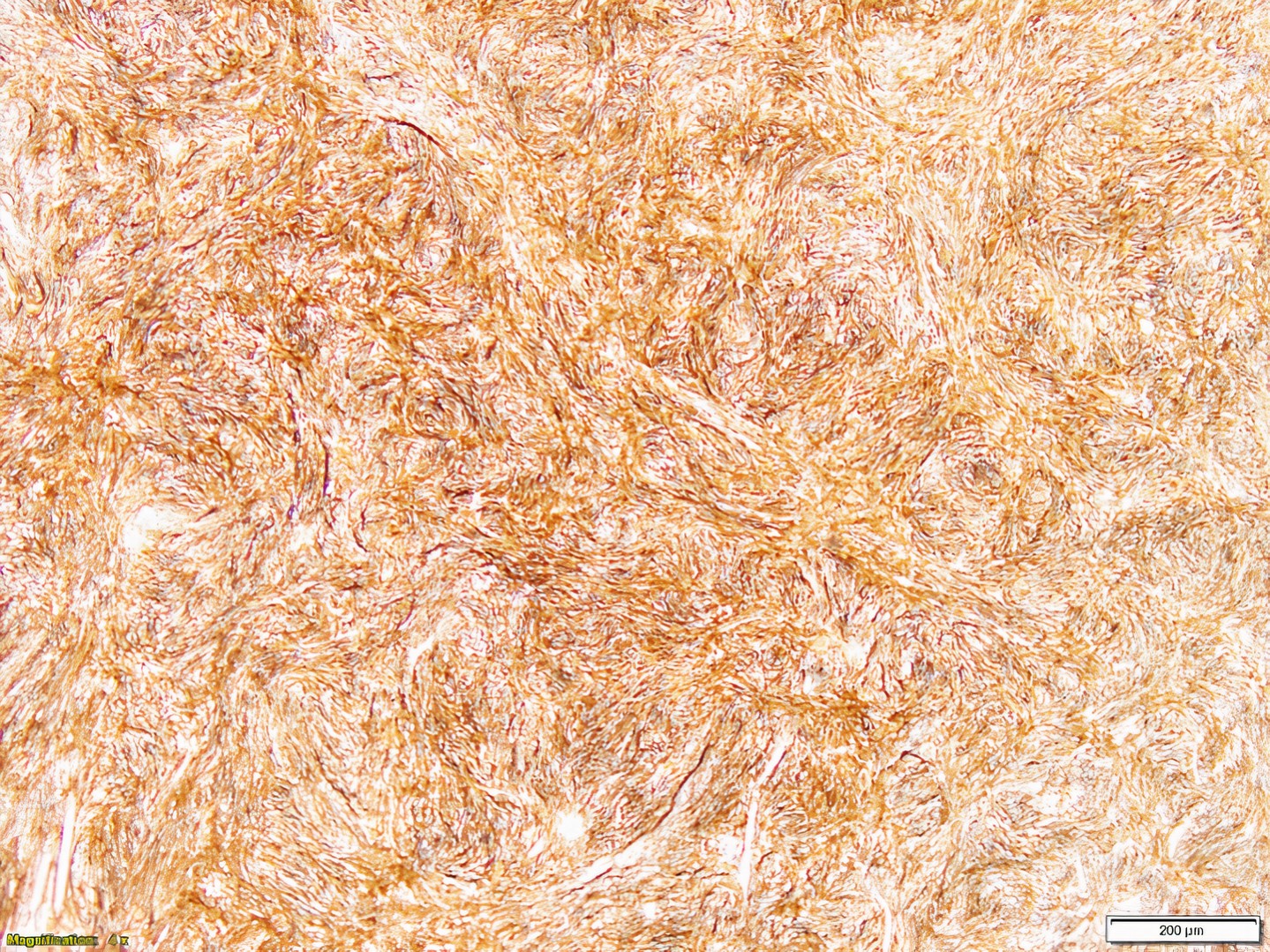
- CD34 shows a characteristic staining pattern:
- CD34 is usually positive in the periphery of dermatofibroma, and negative in the middle
- CD34 is positive in dermatofibrosarcoma protuberans
- CD34 peripheral staining in dermatofibroma is observed in cellular dermatofibroma and deep FH and is weak and patchy
- CD34 is strong and diffuse throughout dermatofibrosarcoma protuberans
- S100, HMB45, MelanA / MART1, nestin (Patterson: Weedon's Skin Pathology, 5th Edition, 2020)
Dermatofibroma
Anerysmal fibrous histiocytoma
Cellular dermatofibroma
Lipidized dermatofibroma
- Skin, right arm, excision:
- Dermatofibroma
- Skin, left shin, excision:
- Dermatofibroma (see comment)
- Comment: Immunohistochemical stains were performed on the above specimen. The cells are positive for factor XIIIa and negative for CD34. This supports the above diagnosis.
- Dermatofibrosarcoma protuberans (DFSP):
- Lower mitotic activity
- Greater cellularity
- Absence of inflammation
- Involvement of subcutis is infiltrative and extensive rather than pushing and focal in deep and cellular variants of fibrous histiocytoma
- CD163 is negative
- Monotonous cells
- Usually deeper, with adnexal structures and fat within
- CD34+ and factor XIIIa-
- COL1A1::PDGFB fusion
- Melanoma, especially desmoplastic type:
- S100+
- Prominent lymphoid aggregates
- Dermatomyofibroma:
- Corkscrew nuclei running parallel to epidermis
- Respects adnexal structures
- Thick elastic fibers present
- Dermal scar:
- Loss of dermal papilla and adnexal structures
- Dense collagen fibers run parallel to dermal epidermal junction
- Factor XIIIa-
- Neurofibroma:
- Mucinous stroma
- Slightly wavy spindle cells with loose appearance
- Mast cells
- Poor circumscription
- S100+
- CD34+ plaque-like dermal fibroma
- Nodular fasciitis
- Atypical fibroxanthoma
- Cellular proliferation involves both the epidermis and dermis
- CD34 is positive at the center of the lesion
- Collagen trapping is seen at the periphery of the lesion
- Deep margins of the lesion typically show extensive infiltration
Comment Here
Reference: Dermatofibroma (cutaneous fibrous histiocytoma)
- S100- / CD34- / CD163+ / MART1-
- S100- / CD34+ / CD163+ / MART1-
- S100+ / CD34- / CD163- / MART1+
- S100+ / CD34- / CD163+ / MART1-
- S100+ / CD34+ / CD163+ / MART1-
Comment Here
Reference: Dermatofibroma (cutaneous fibrous histiocytoma)
