
Colon
Polyps
Traditional serrated adenoma
Authors: Enoch Kuo, M.D., Raul S. Gonzalez, M.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.


Last author update: 29 October 2021
Last staff update: 6 May 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Colon tumor traditional serrated adenoma [title]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Kuo E, Gonzalez RS. Traditional serrated adenoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colontumortraditionalserratedadenoma.html. Accessed May 13th, 2024.
Definition / general
- Serrated neoplastic precursor lesion for aggressive BRAF mutated microsatellite instability (MSI) stable subtype of colorectal carcinoma (World J Gastrointest Oncol 2016;8:805)
- Characterized by prominent eosinophilic cytoplasm, elongated nuclei, tubulovillous (filiform) architecture and ectopic crypts (Am J Gastroenterol 2012;107:1315)
Essential features
- Neoplastic polyp of the colon
- Shows dysplastic appearing nuclei and prominent eosinophilic cytoplasm
Terminology
- Abbreviated as TSA
- Filiform serrated adenoma sometimes used to refer to a possible variant (Am J Surg Pathol 2007;31:1238, Pathology 2012;44:18)
ICD coding
Epidemiology
- Traditional serrated adenomas account for 0.56 - 1.9% of colonic polyps (Hum Pathol 2015;46:933)
- No gender predilection (Mod Pathol 2015;28:414)
- Usually seen in patients over age 50 (J Gastroenterol Hepatol 2018;33:1039)
Sites
- More often found in the rectosigmoid colon (Mod Pathol 2015;28:414)
- A similar lesion, lacking BRAF mutation, may rarely arise in the small intestine (Histopathology 2015;66:333)
Pathophysiology
- May arise from microvesicular hyperplastic polyps (MVHP) and sessile serrated adenomas (SSA) (Hum Pathol 2015;46:933)
- Generally considered to be intrinsically dysplastic, though some argue against this view (Hum Pathol 2015;46:933)
Etiology
- Associated with obesity and increased triglyceride levels (J Gastroenterol Hepatol 2018;33:1039)
Clinical features
- Incidental finding on colonoscopy
Diagnosis
- Histopathology is the gold standard of diagnosis (World J Gastroenterol 2016;22:7754)
Radiology description
- Screening CT colonography may identify large (~14 mm) traditional serrated adenomas (Radiology 2016;280:455)
Prognostic factors
- Risk of progression to carcinoma is unknown (Am J Gastroenterol 2012;107:1315)
Treatment
- Endoscopic removal of the adenoma
- US Multi Society Task Force on Colorectal Cancer recommends a 3 year surveillance interval after initial diagnosis of traditional serrated adenomas (Gastroenterology 2012;143:844)
Gross description
- May be flat, pinecone shaped or fern-like (Mod Pathol 2015;28:414, World J Gastrointest Oncol 2016;8:805)
Microscopic (histologic) description
- Protuberant villiform growth pattern with slit-like serrations
- Pseudostratified epithelial columnar cells with eosinophilic cytoplasm and dark, pencillate, dysplastic-like nuclei
- Ectopic crypt foci / formations are a key feature (abnormally positioned crypts with bases not seated at the muscularis mucosae) (Am J Surg Pathol 2008;32:21)
- High grade adenomatous dysplasia may be present
- Goblet cells present
- Mucin rich variant is characterized by > 50% goblet cells and fewer ectopic crypt formations (Histopathology 2017;71:208)
Microscopic (histologic) images
Contributed by Enoch Kuo, M.D.
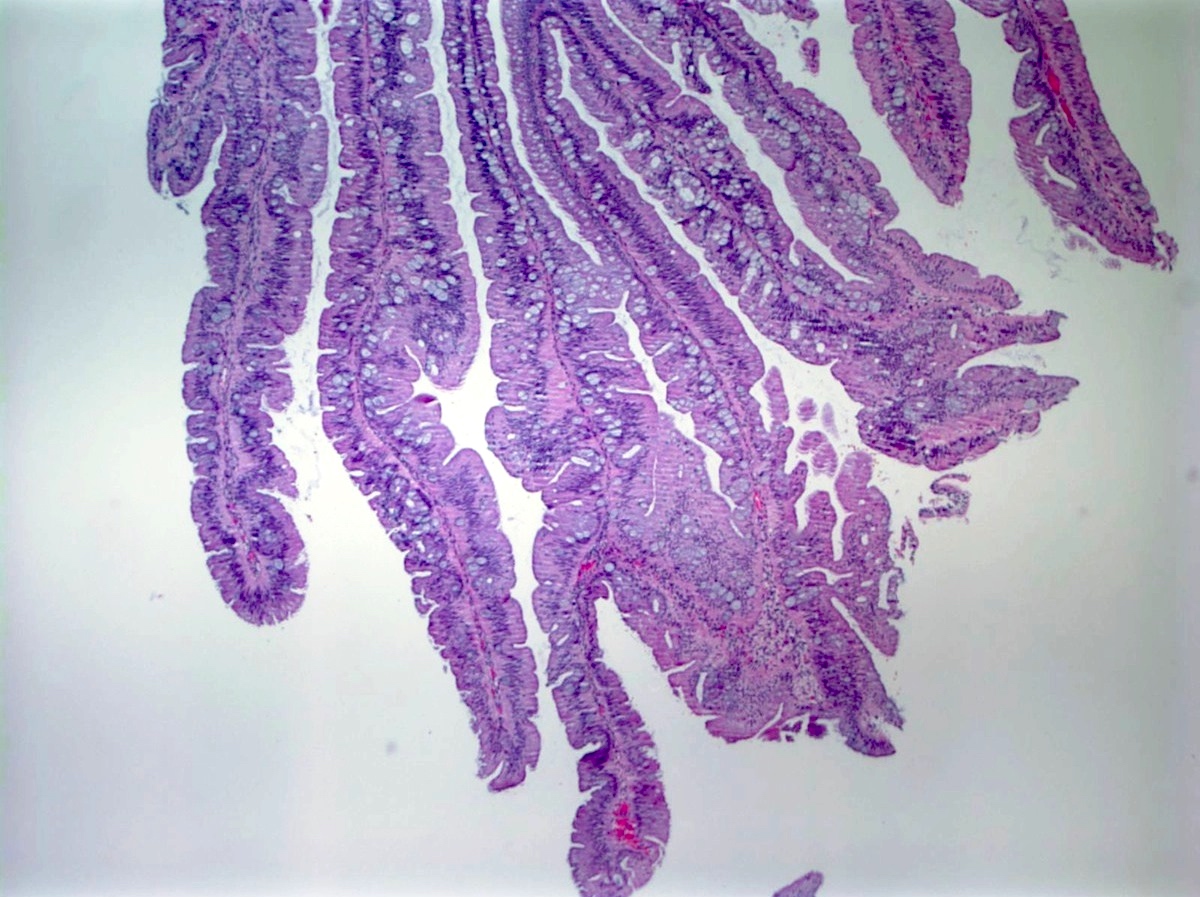
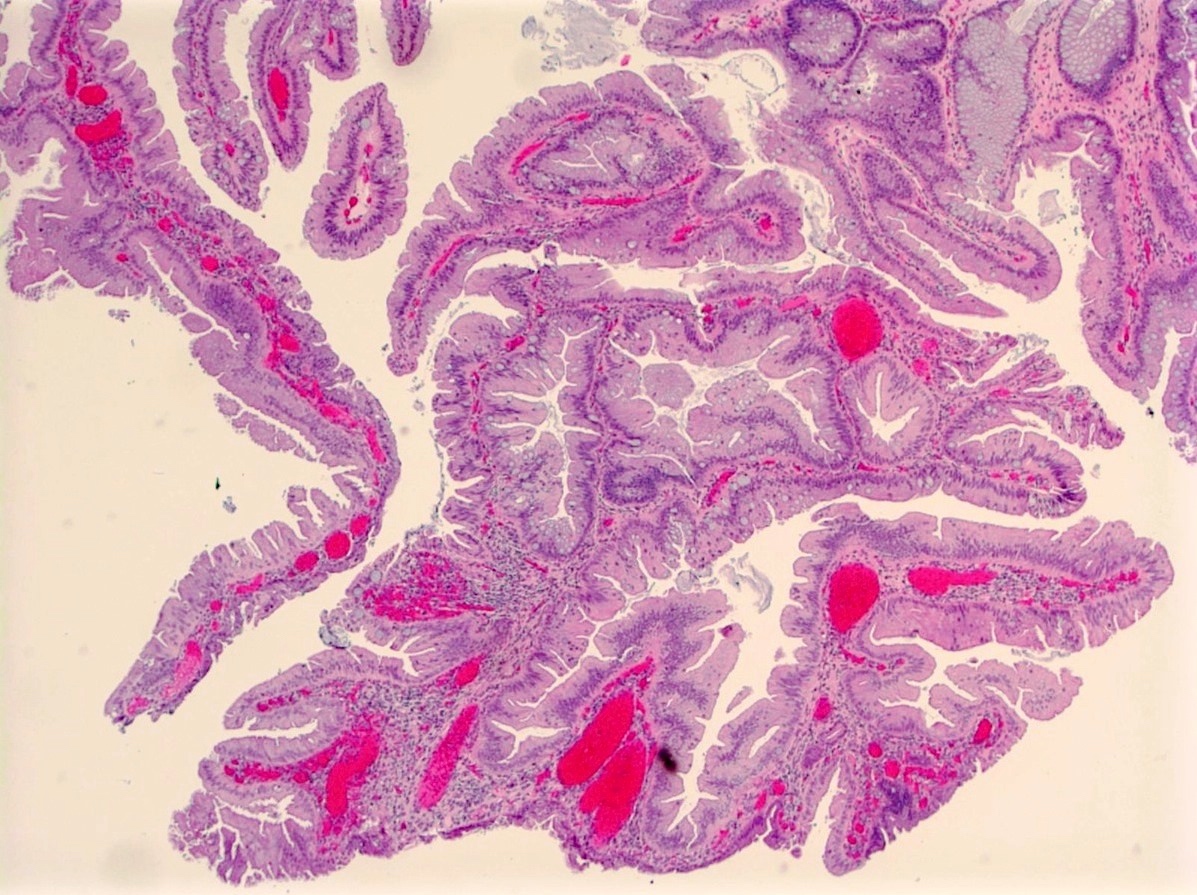
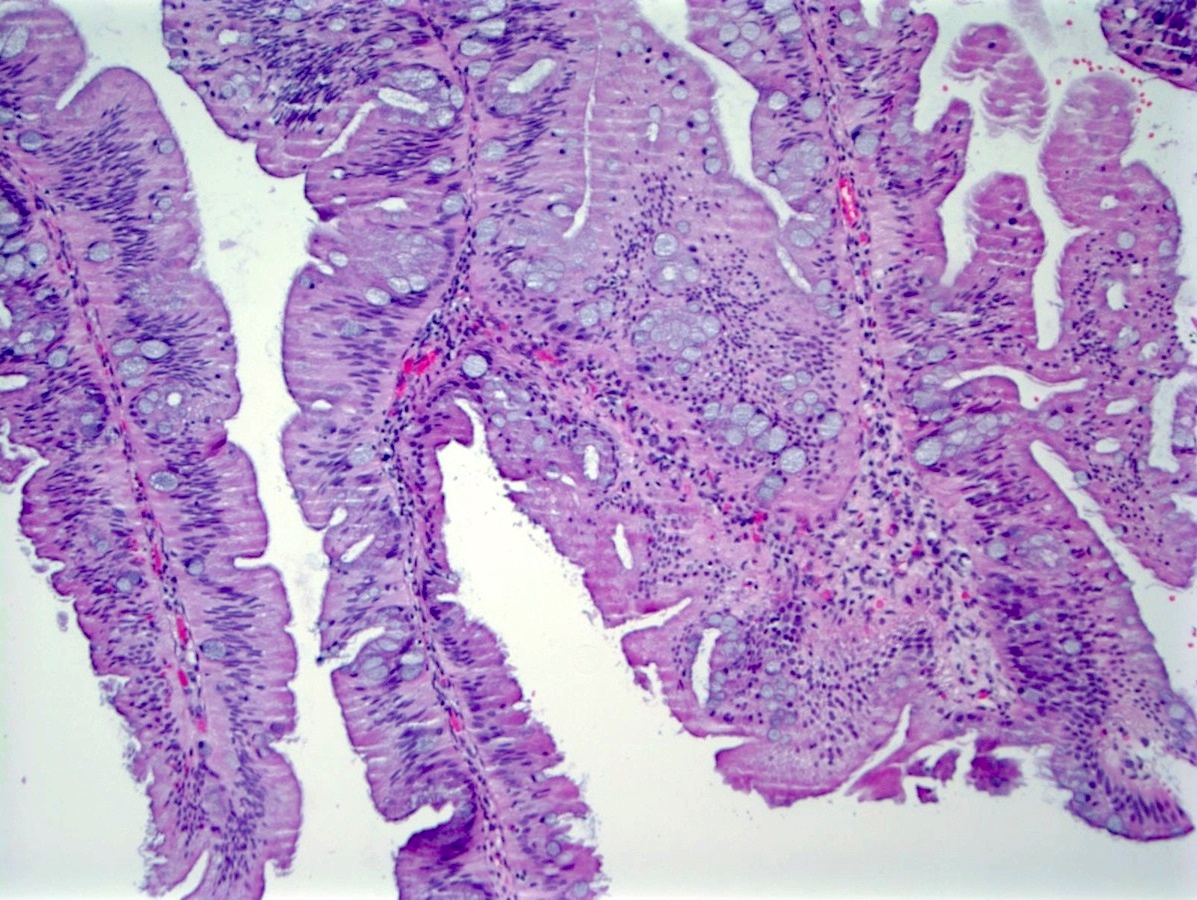
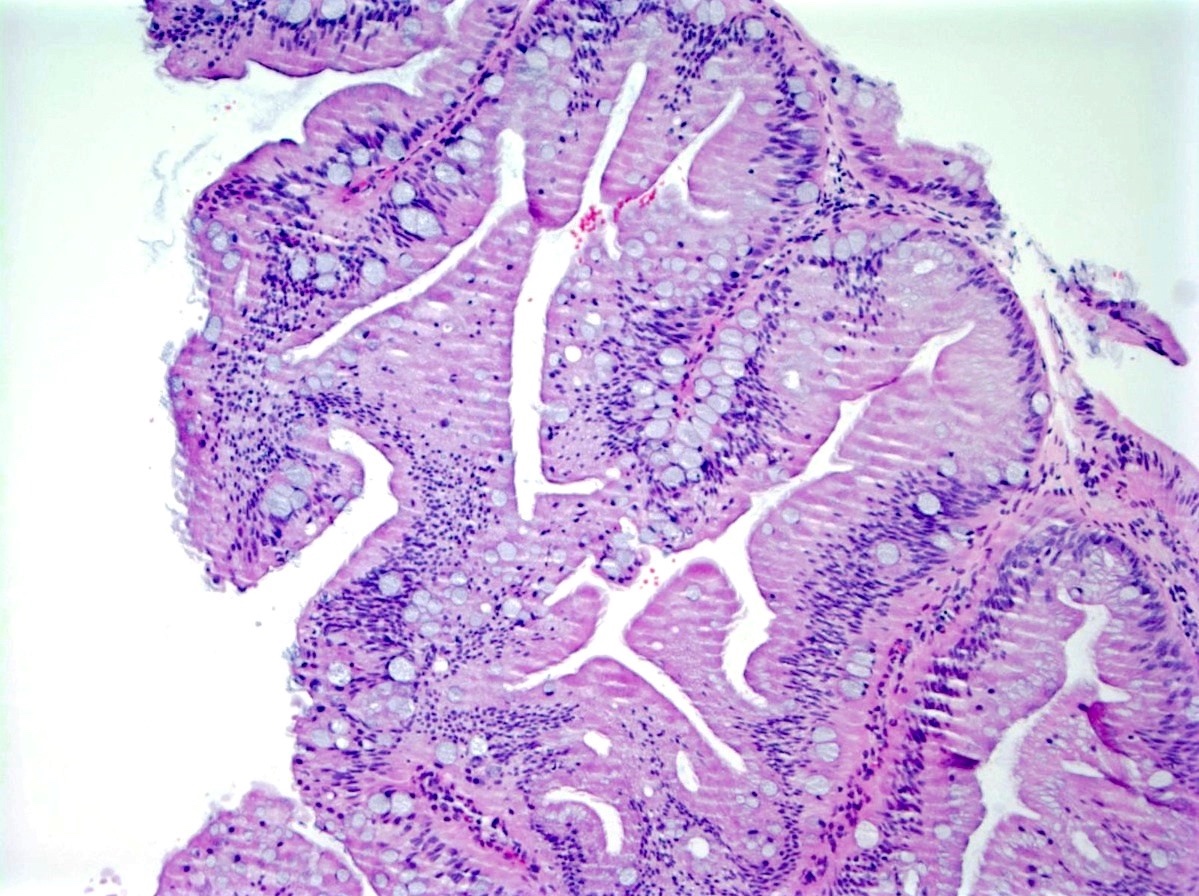
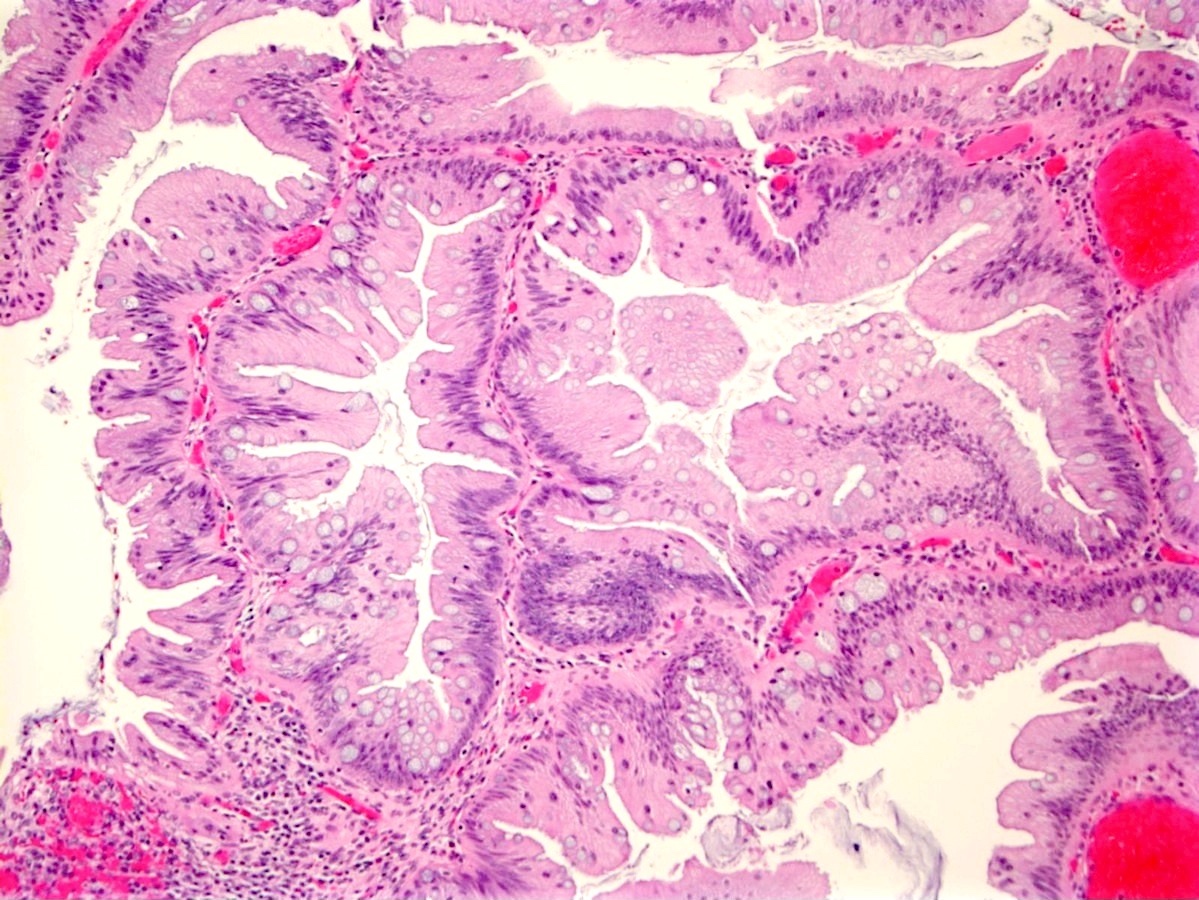
Traditional serrated adenoma
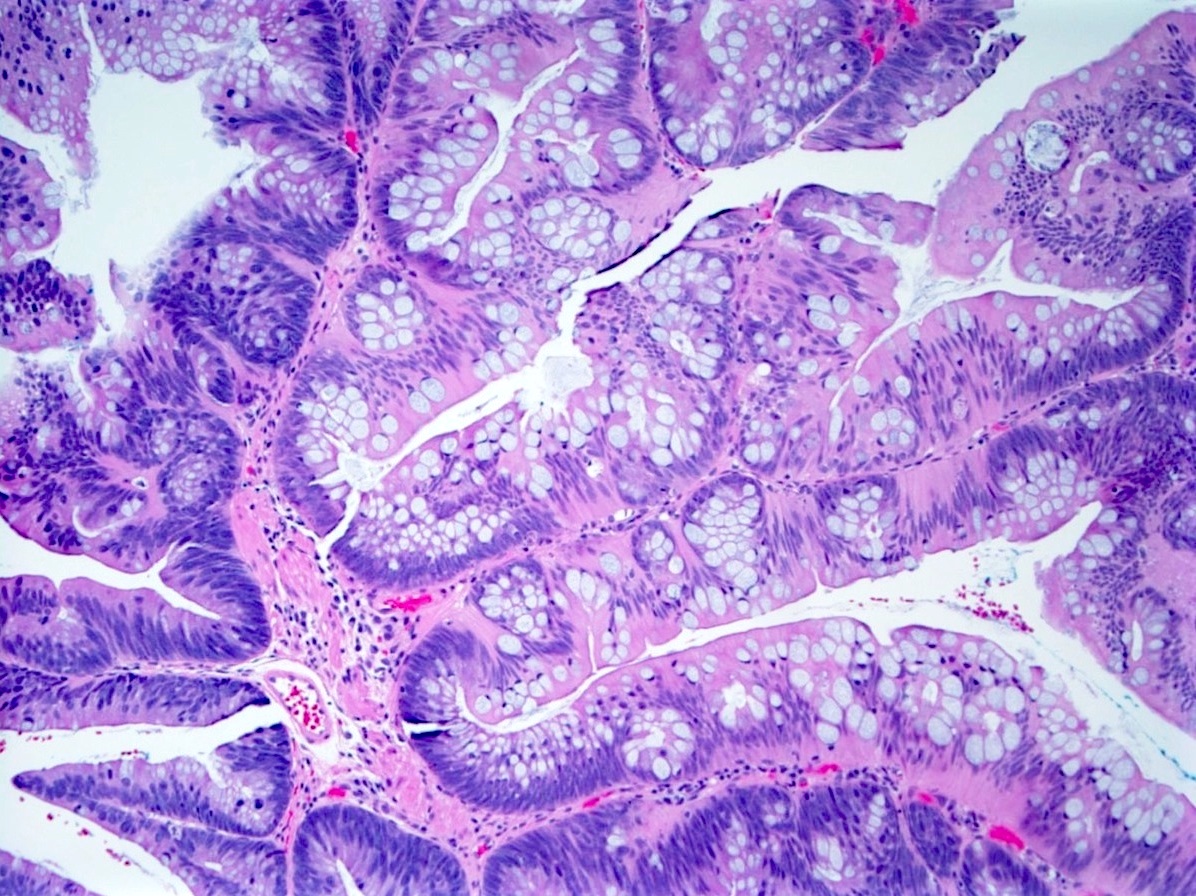
Contributed by Christopher Hartley, M.D.
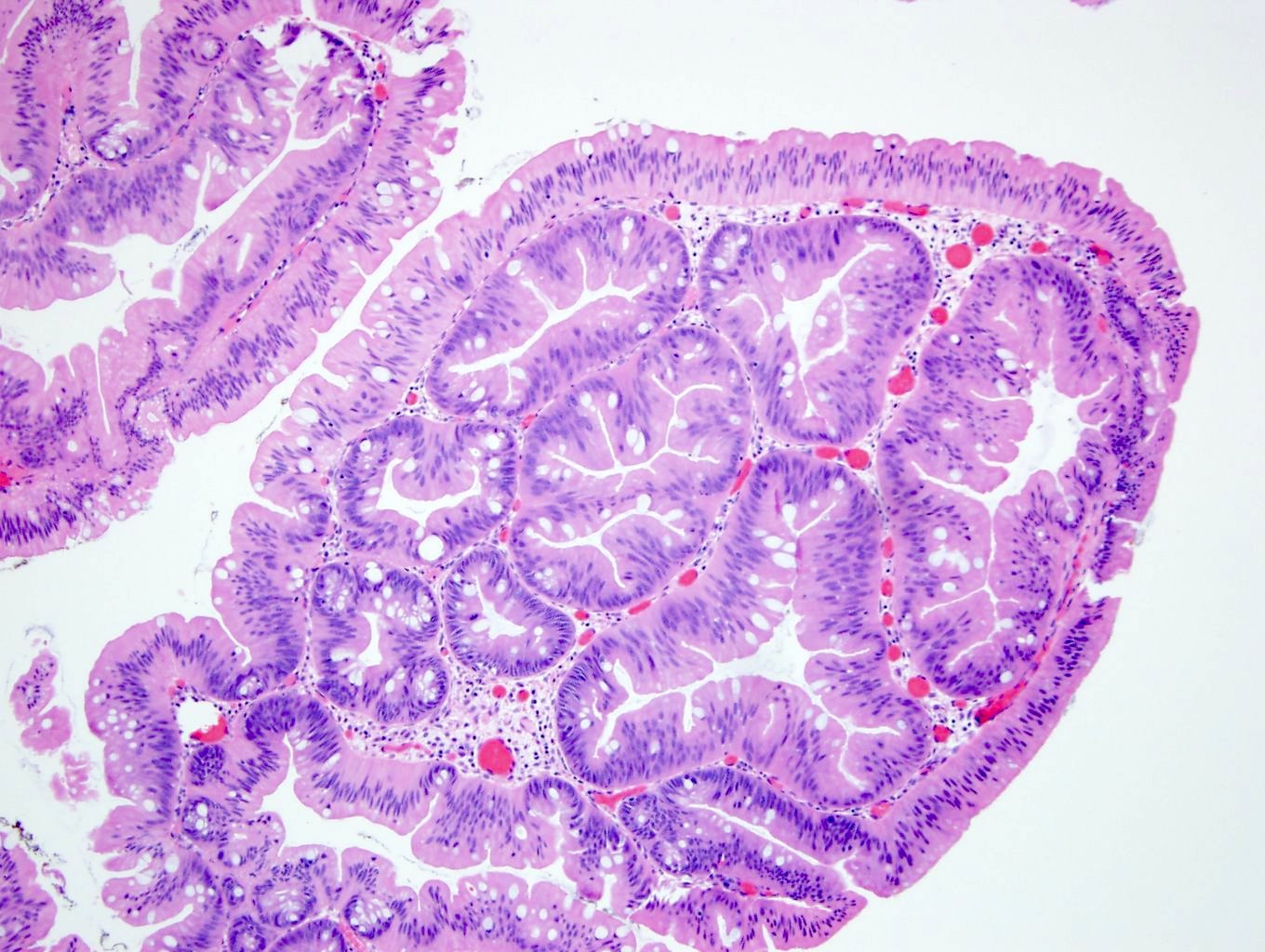
Traditional serrated adenoma
Positive stains
- CK20 stains only the surface epithelial cells and does not stain the ectopic crypt formations (Am J Surg Pathol 2008;32:21)
- Ki67 stains only the ectopic crypt formations
- MUC2 and MUC5AC
- Beta catenin and p53 nuclear staining is present in areas of conventional dysplasia (Mod Pathol 2015;28:414)
Negative stains
Molecular / cytogenetics description
- MAPK pathway activation is a critical initiating event, either by a BRAF or KRAS mutation (Hum Pathol 2015;46:933)
- MAPK pathway activation is followed by CpG island methylator phenotype (CIMP)
- BRAF mutated traditional serrated adenomas are more frequently CpG island methylator phenotype high (Mod Pathol 2015;28:414, Hum Pathol 2015;46:933)
- Most cases have no defects in mismatch repair (microsatellite stable)
- PTPRK-RSPO3 gene fusions may be present (Histopathology 2017;71:601)
Sample pathology report
- Rectum, polypectomy:
- Traditional serrated adenoma
Differential diagnosis
- Hyperplastic polyp and sessile serrated adenoma:
- Cytologic features of pseudostratification and nuclear elongation are most useful in distinguishing traditional serrated adenomas from hyperplastic polyps and sessile serrated adenomas (Virchows Arch 2012;461:495)
- Ectopic crypts, goblet cells and eosinophilic cytoplasm are not distinguishing features since they may be present in sessile serrated adenomas and hyperplastic polyps as well (Am J Gastroenterol 2012;107:1315, Diagn Pathol 2014;9:212)
- Traditional serrated adenomas can be distinguished from sessile serrated adenomas and hyperplastic polyps by their low Ki67 staining, specifically within the ectopic crypts (Am J Surg Pathol 2008;32:21)
- Tubulovillous adenoma:
- Definitive dysplastic nuclei, no eosinophilic cytoplasm, no serrated architecture or ectopic crypts
- Tubulovillous adenomas often have a component resembling traditional serrated adenoma, with significance unclear
Board review style question #1
Which mutation is most common in traditional serrated adenomas?
- BRAF mutation
- CDKN2A mutation
- KRAS mutation
- TP53 mutation
Board review style answer #1
A. BRAF and KRAS mutations in traditional serrated adenomas are almost mutually exclusive with approximately 67% having BRAF mutations and 22% with KRAS mutations. BRAF mutated traditional serrated adenomas are more likely to be CpG island methylator phenotype high. TP53 mutation and CDKN2A silencing by methylation are seen in areas with conventional dysplasia (Mod Pathol 2015;28:414).
Comment here
Reference: Traditional serrated adenoma
Comment here
Reference: Traditional serrated adenoma
