Colon
Polyps
Tubulovillous / villous adenoma
Editorial Board Members: Raul S. Gonzalez, M.D., Naziheh Assarzadegan, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 21 June 2022
Last staff update: 21 June 2022
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Tubulovillous / villous adenoma

Table of Contents
Definition / general | Essential features | ICD coding | Sites | Pathophysiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Martinez Ciarpaglini C. Tubulovillous / villous adenoma . PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colontumortvadenoma.html. Accessed September 16th, 2025.
Definition / general
- Advanced precursor lesion of colorectal cancer (Nat Rev Dis Primers 2015;1:15065)
- Tubulovillous adenoma: 20 - 80% villosity
- Villous adenoma: > 80% villosity (Am J Surg Pathol 2011;35:212)
Essential features
- Recognized as the precursor lesion of chromosomal unstable colorectal cancer (Pathologica 2021;113:218)
- Low grade dysplasia is an intrinsic feature
- Associated with oncogene KRAS mutation in 50% of cases
ICD coding
- ICD-10: D12.6 - benign neoplasm of colon, unspecified
Sites
- More frequent in distal colorectum than in proximal colon (68.4% versus 31.6%) (Am J Surg Pathol 2011;35:212)
Pathophysiology
- Conventional adenoma carcinoma sequence with oncogene (KRAS) activation and tumor suppressor (APC, SMAD4 and TP53) inactivation
- Associated with chromosomal unstable colorectal cancer (Cancer Biol Med 2016;13:120)
Clinical features
- Mean age of 62 years (Eur J Cancer 2005;41:416)
- M:F = 1.6:1
- Though most cases are asymptomatic, some present with a history of rectal bleeding (StatPearls: Villous Adenoma [Accessed 31 May 2022])
Diagnosis
- Screening or surveillance colonoscopy identifies and removes lesion, followed by tissue diagnosis
Prognostic factors
- Villous or tubulovillous histology is associated with increased risk of colorectal neoplasia: 16.8% versus 9.7% compared with tubular adenomas
- Increased risk of malignant transformation in cases with high grade dysplasia (↑ 1.77x) (Gastroenterology 2012;143:844)
- Risk of recurrence with malignancy after excision is associated with piecemeal endoscopic resection (Surg Endosc 2021;35:2500)
Case reports
- 62 year old woman presented with rectal bleeding and fleshy mass protruding from the anal canal (World J Surg Oncol 2019;17:109)
- 69 year old man with acute appendicitis (Int J Surg Case Rep 2019;61:60)
- 78 year old woman with tubulovillous adenoma of the cecum with squamous metaplasia (Int J Surg Pathol 2009;17:340)
Treatment
- Endoscopic resection
- When possible, en bloc resection should be the goal for the management (Surg Endosc 2021;35:2500)
Gross description
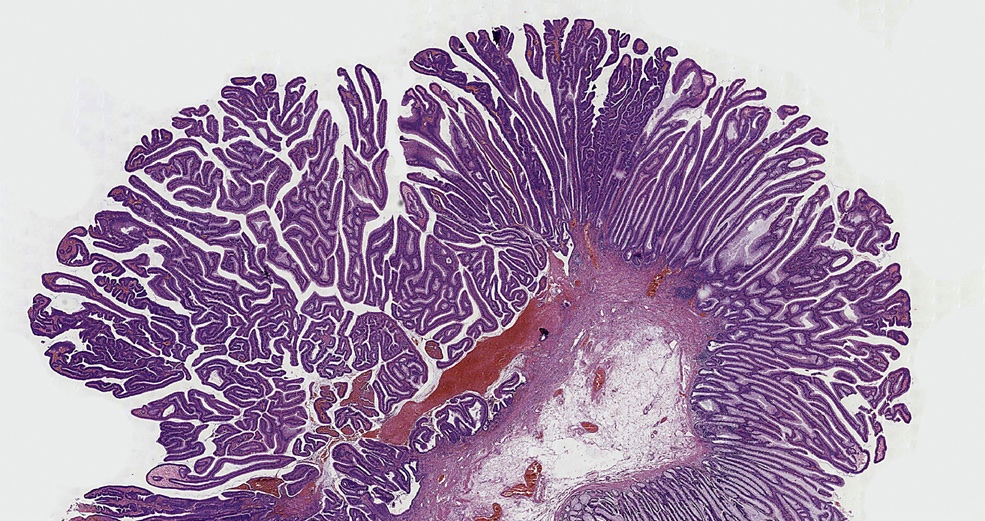
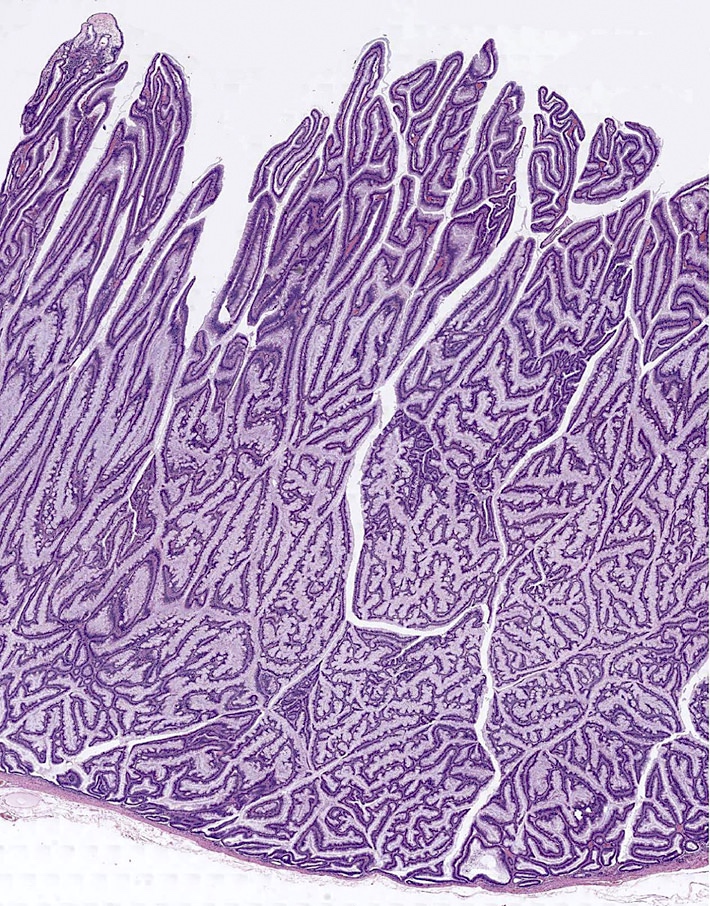
- Pedunculated or sessile polypoid lesions with macroscopic finger-like projections
Gross images
Contributed by Carolina Martinez Ciarpaglini, M.D., Ph.D.

Large villous polyp
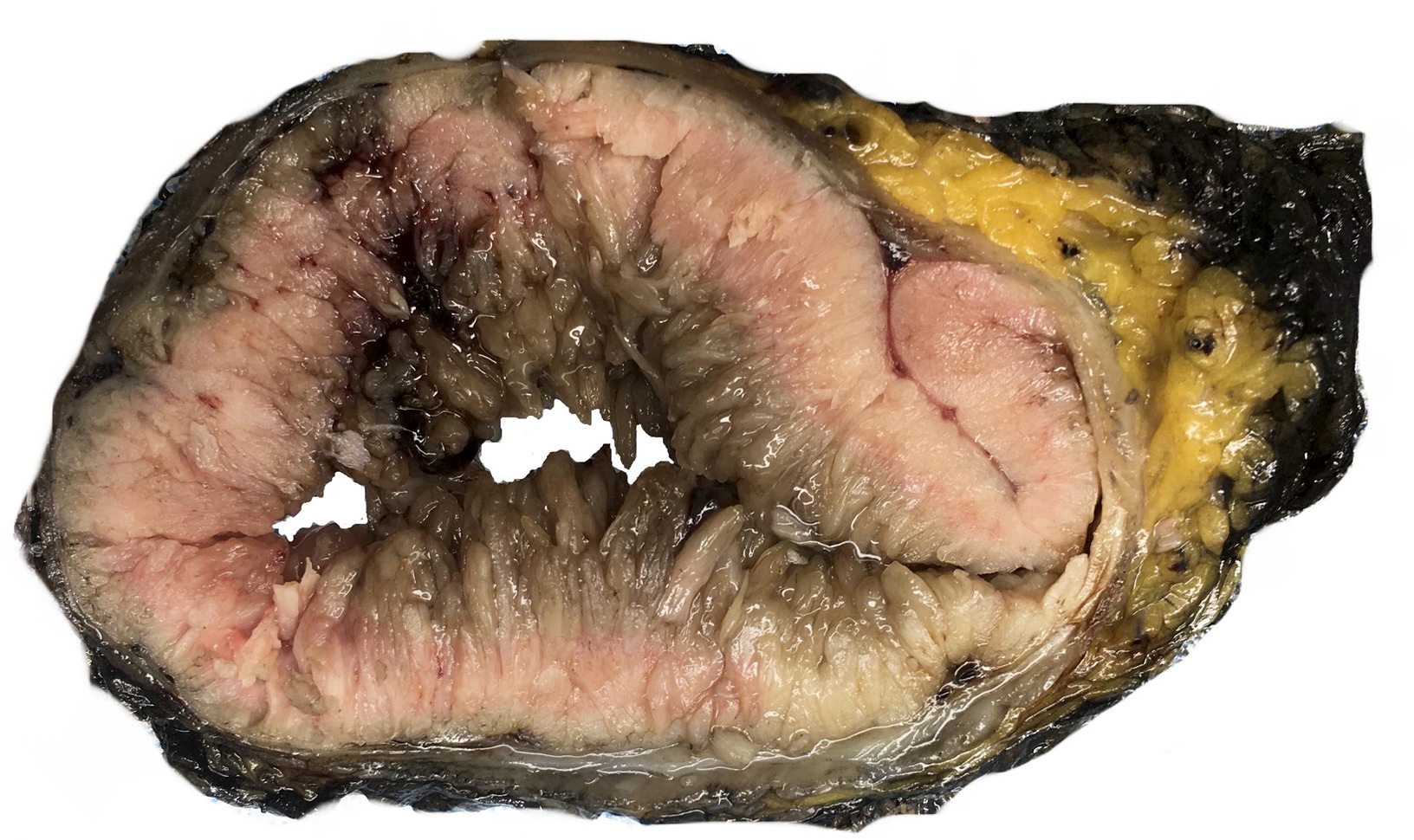
Giant villous adenoma
Images hosted on other servers:

Sessile villous adenoma

Pedunculated villous adenoma

Villous surface

Detailed view of villous projections

Adenocarcinoma arising in villous adenoma
Microscopic (histologic) description
- Low grade dysplasia is a constituent feature
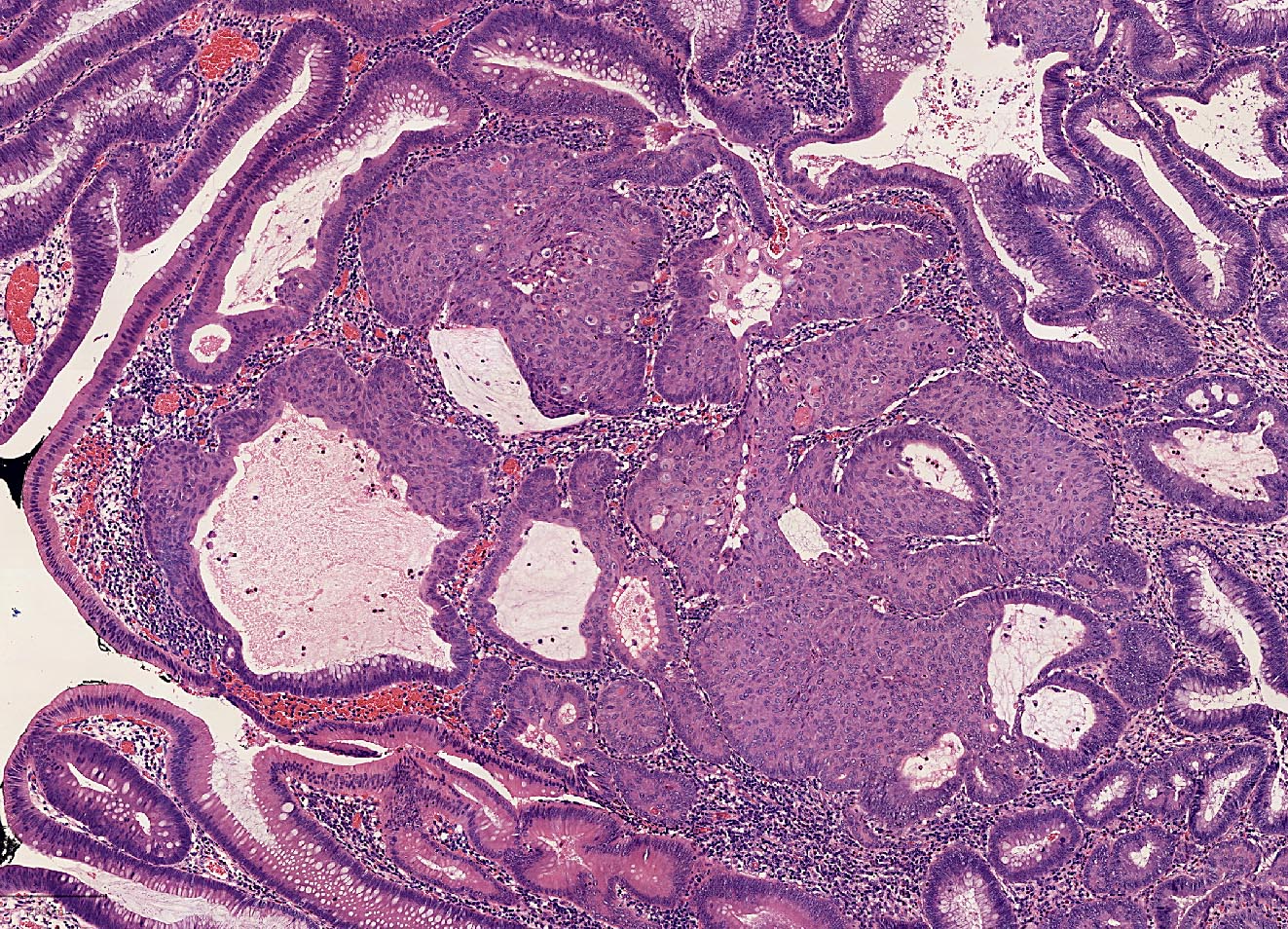
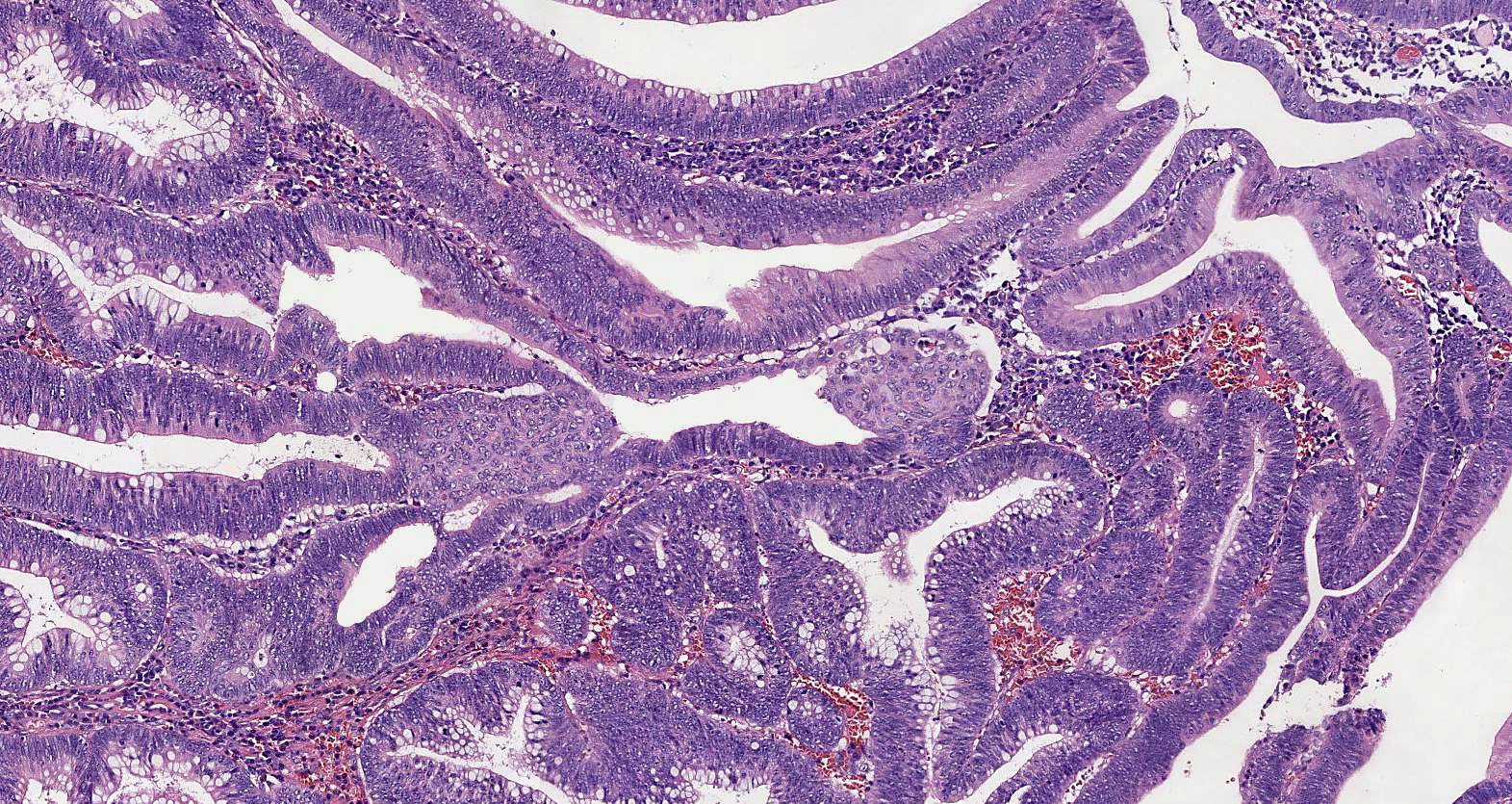
- Epithelial, finger-like projections, away from the muscularis mucosae, formed by fibrovascular cores lined by dysplastic epithelium (villous architecture)
- Percentage of villosity defines diagnostic terminology
- 20 - 80% = tubulovillous adenoma
- > 80% = villous adenoma
- Crowded pseudostratification of cells with elongated nuclei occupying the basal half of the cytoplasm
- Pleomorphism and atypical mitoses should be absent or minimally present
- Mitotic activity and minimal loss of cell polarity are allowed
- Architecturally, the crypts should maintain a resemblance to normal colon, without significant crowding, cribriform or complex forms
- Squamous metaplasia as solid nests of squamous cells in direct continuity with adenomatous glands may be seen in about 0.4% of colorectal adenomas (Histopathology 2021;78:348)
- Paneth cell metaplasia is a frequent finding (17 - 23%), especially in proximal locations; osseous metaplasia has been reported (Histopathology 2021;78:348)
- Neuroendocrine metaplasia refers to the presence of scattered foci of neuroendocrine cells that lack significant nuclear atypia, mitotic activity or necrosis; these cells comprise < 30% of the lesion (Ann Diagn Pathol 2019;42:69)
- Clusters of neuroendocrine metaplasia are usually < 2 mm and limited to the lamina propria without disturbing the overall architecture (Histopathology 2021;78:348)
- Ectopic crypt foci are a frequent finding (J Clin Pathol 2016;69:1063)
- High grade dysplasia can be seen (carcinoma in situ or intraepithelial / intramucosal carcinoma are not recommended terms)
- Increased nucleus to cytoplasm ratio
- Significant loss of cell polarity: nuclear stratification through the entire thickness of the epithelium
- Round nuclei with open appearing chromatin and increasingly prominent nucleoli
- Significant pleomorphism and atypical mitoses
- Abnormal architecture includes cribriform structures with back to back glands, prominent glandular budding and intraluminal papillary tufting (StatPearls: Villous Adenoma [Accessed 31 May 2022])
- Poor interobserver agreement for assessment of the villous component and high grade dysplasia have been demonstrated (Am J Surg Pathol 2013;37:427)
Microscopic (histologic) images
Contributed by Carolina Martinez Ciarpaglini, M.D., Ph.D., Jijgee Munkhdelger, M.D., Ph.D. and Andrey Bychkov, M.D., Ph.D.
Neuroendocrine metaplasia
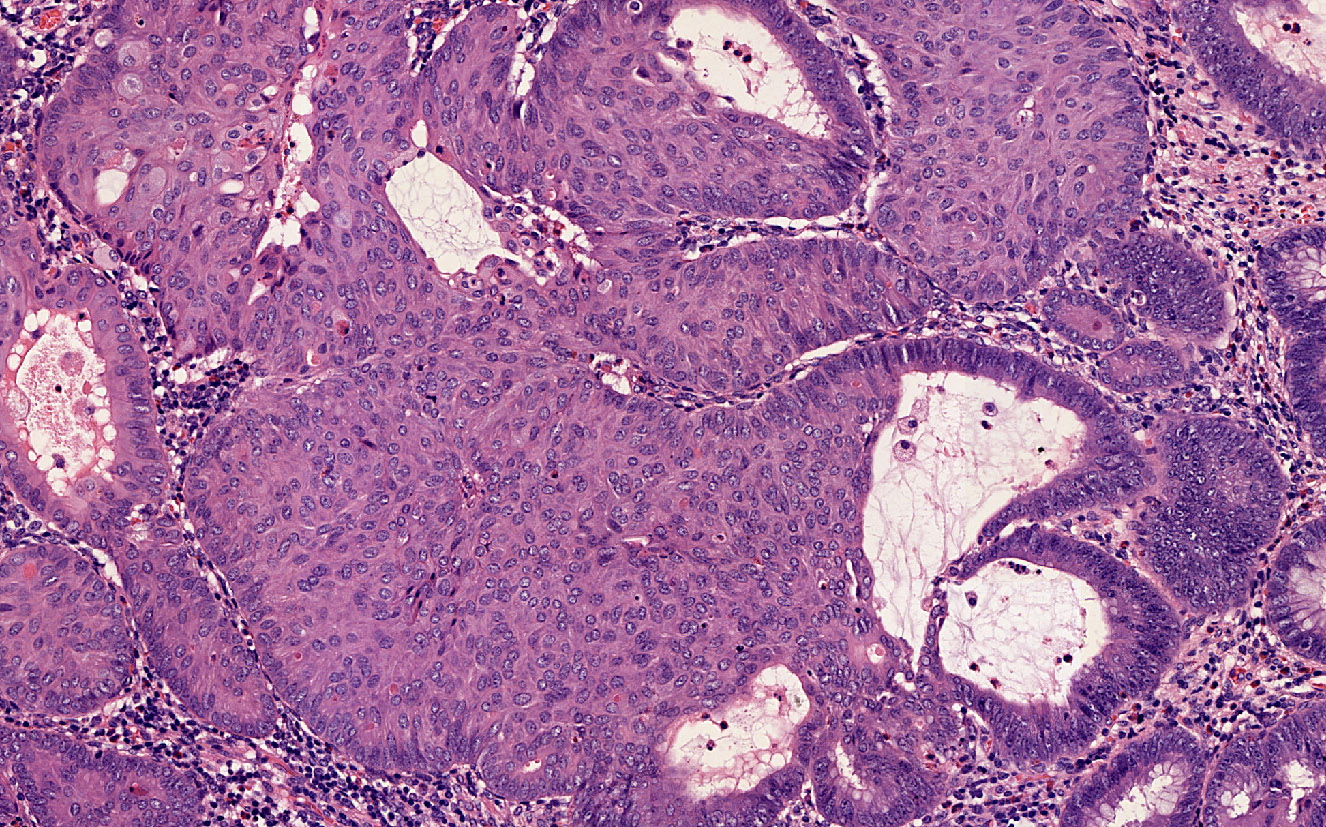
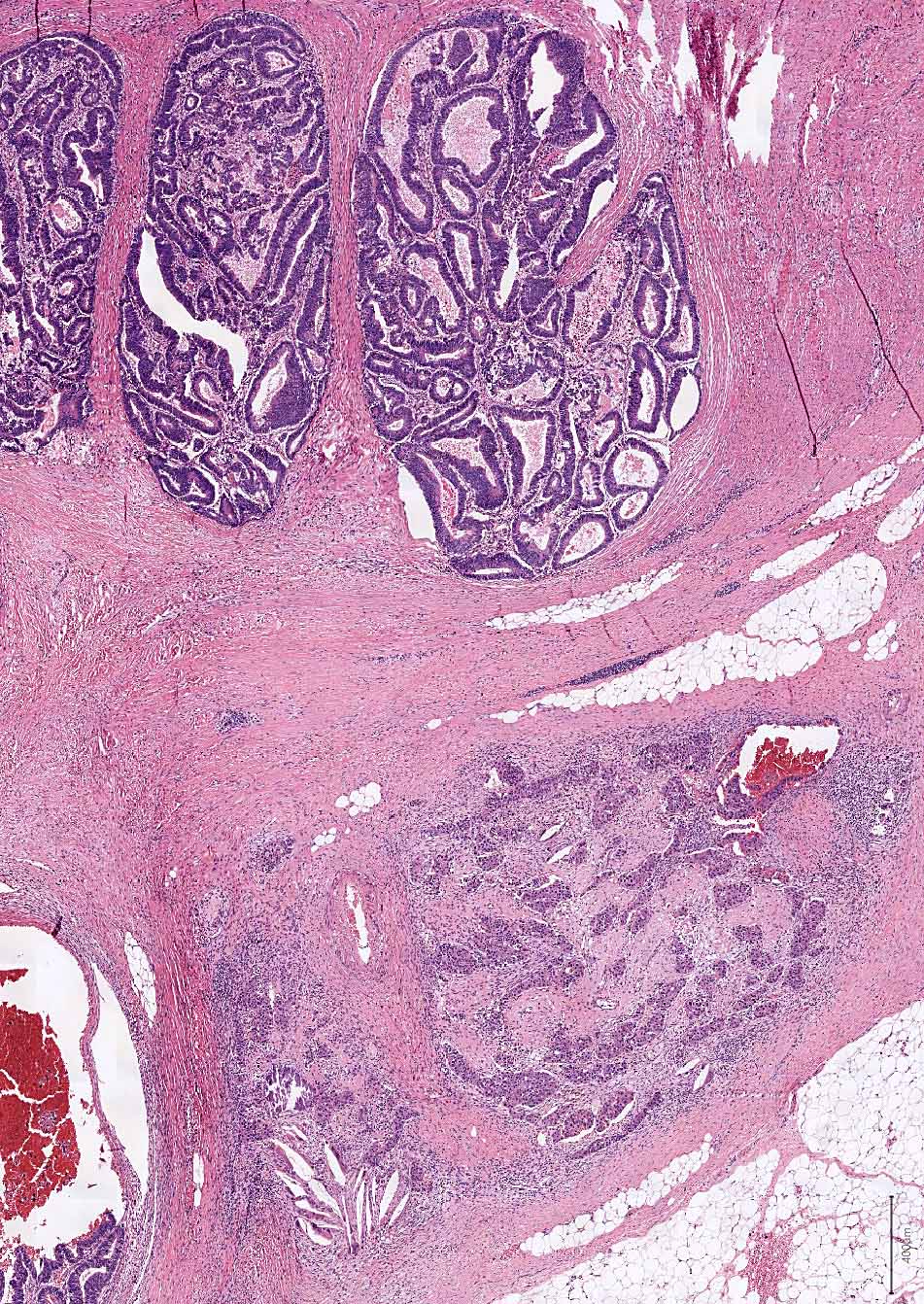
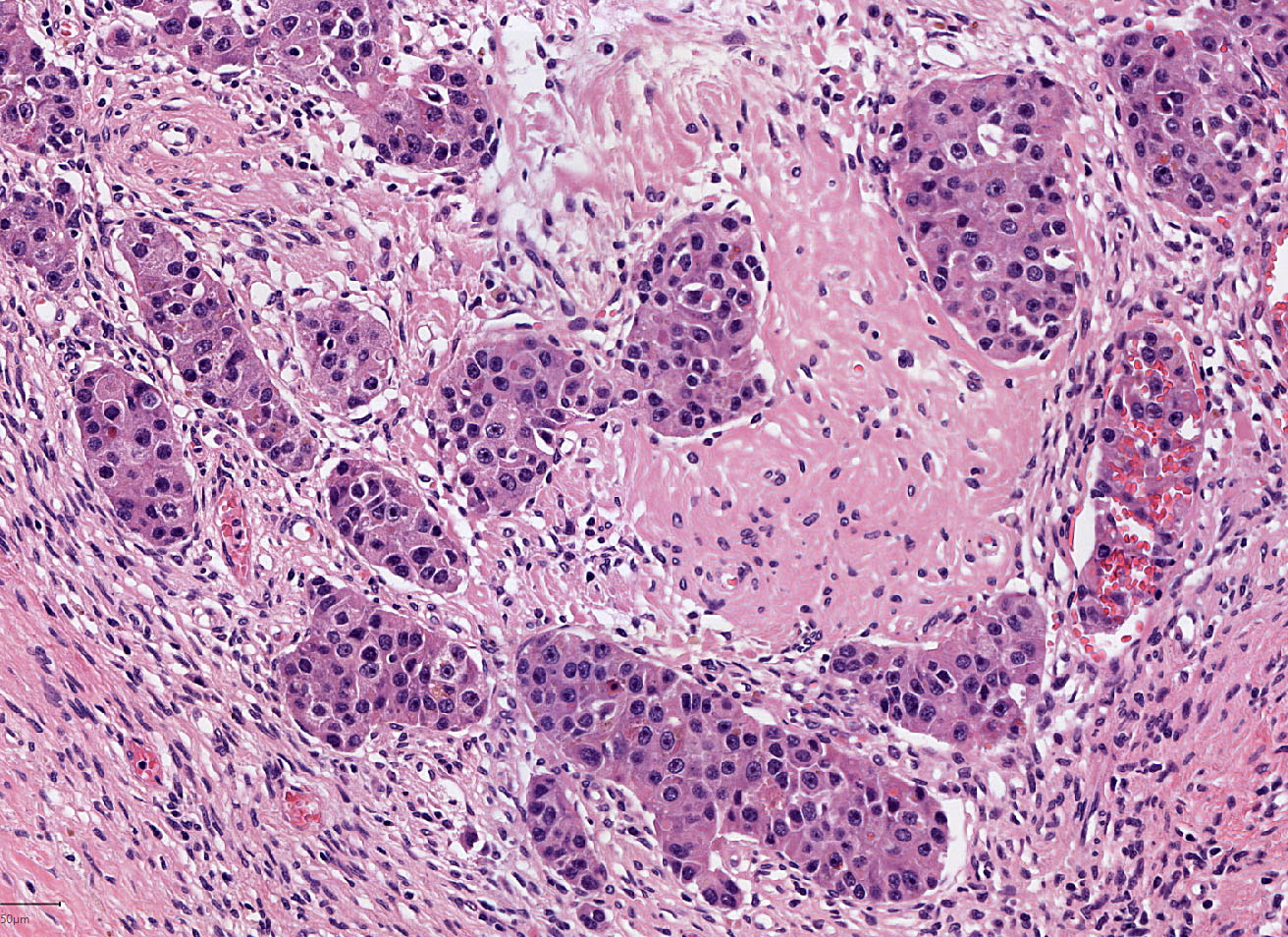
Squamous metaplasia
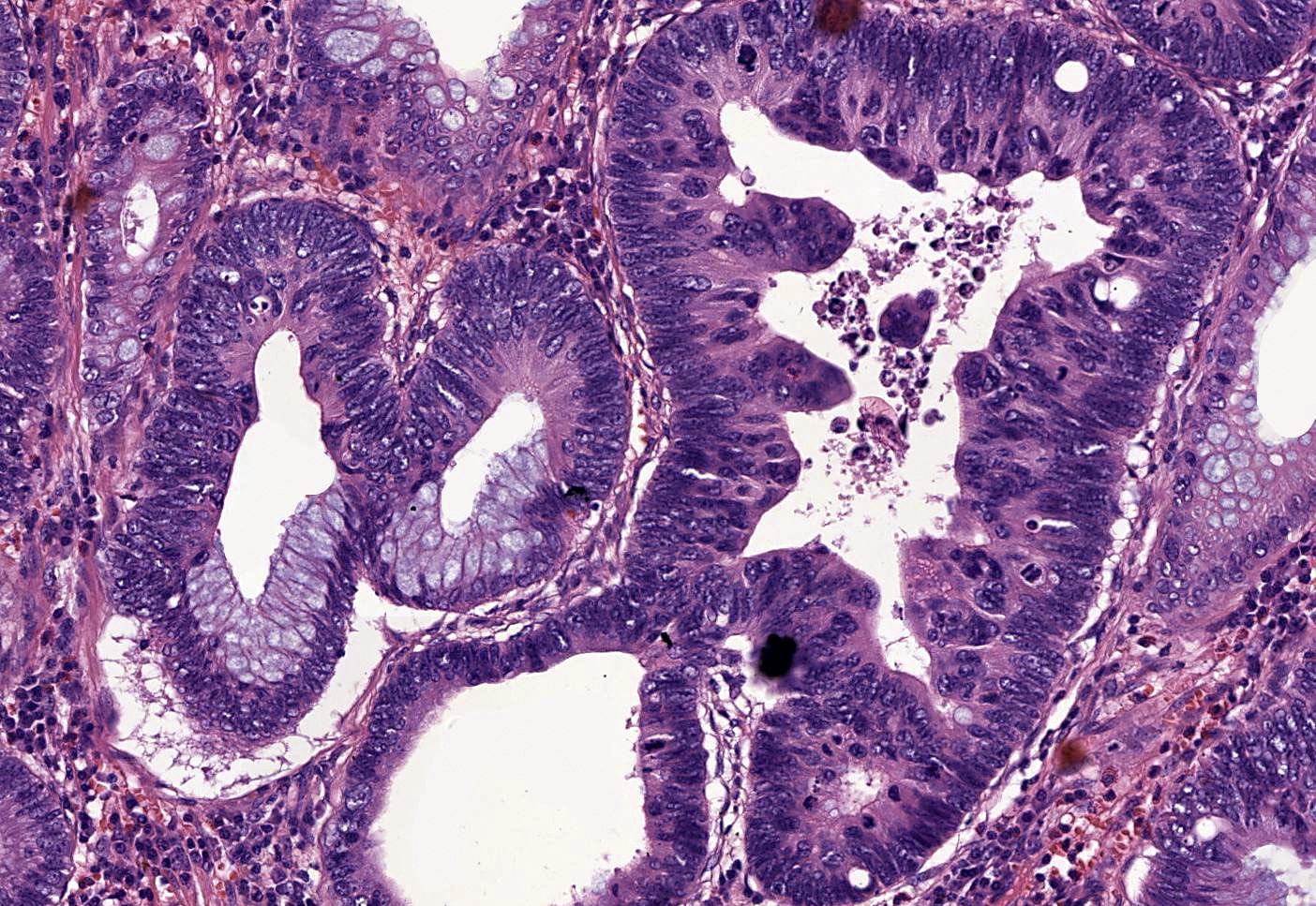
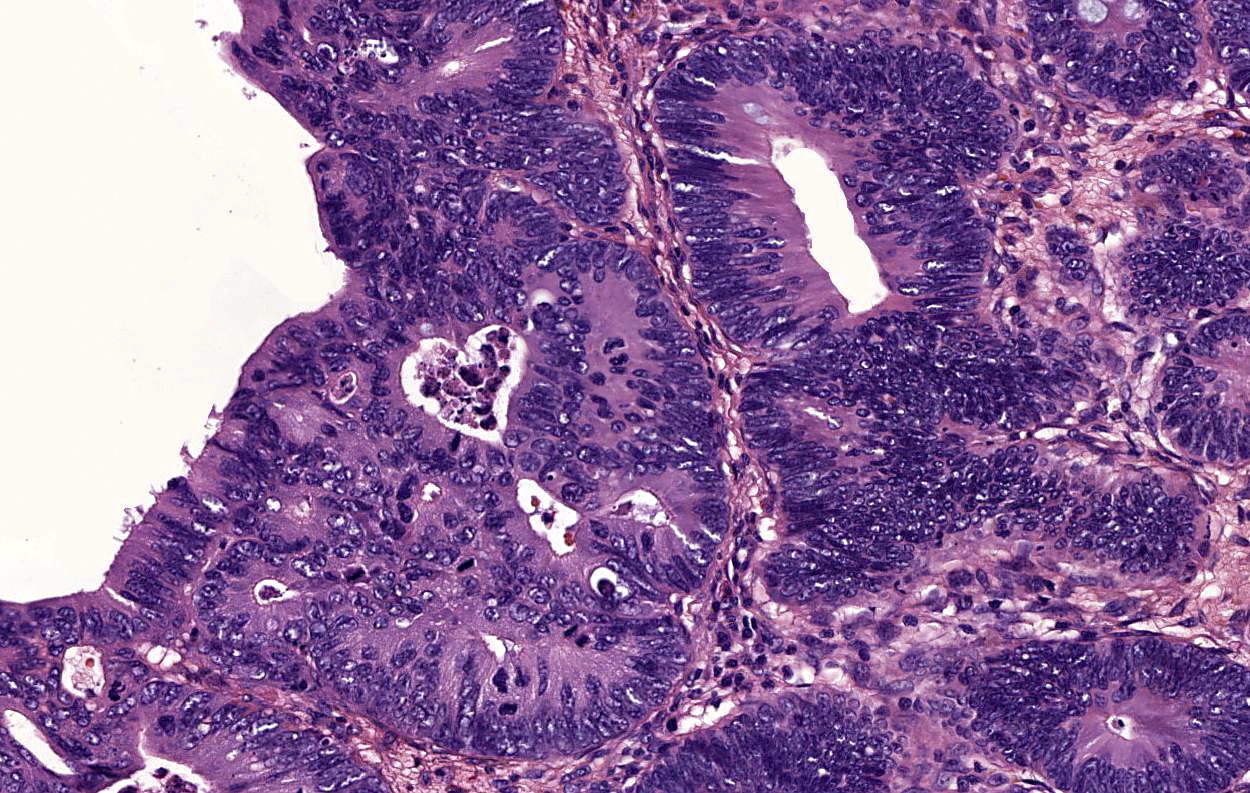
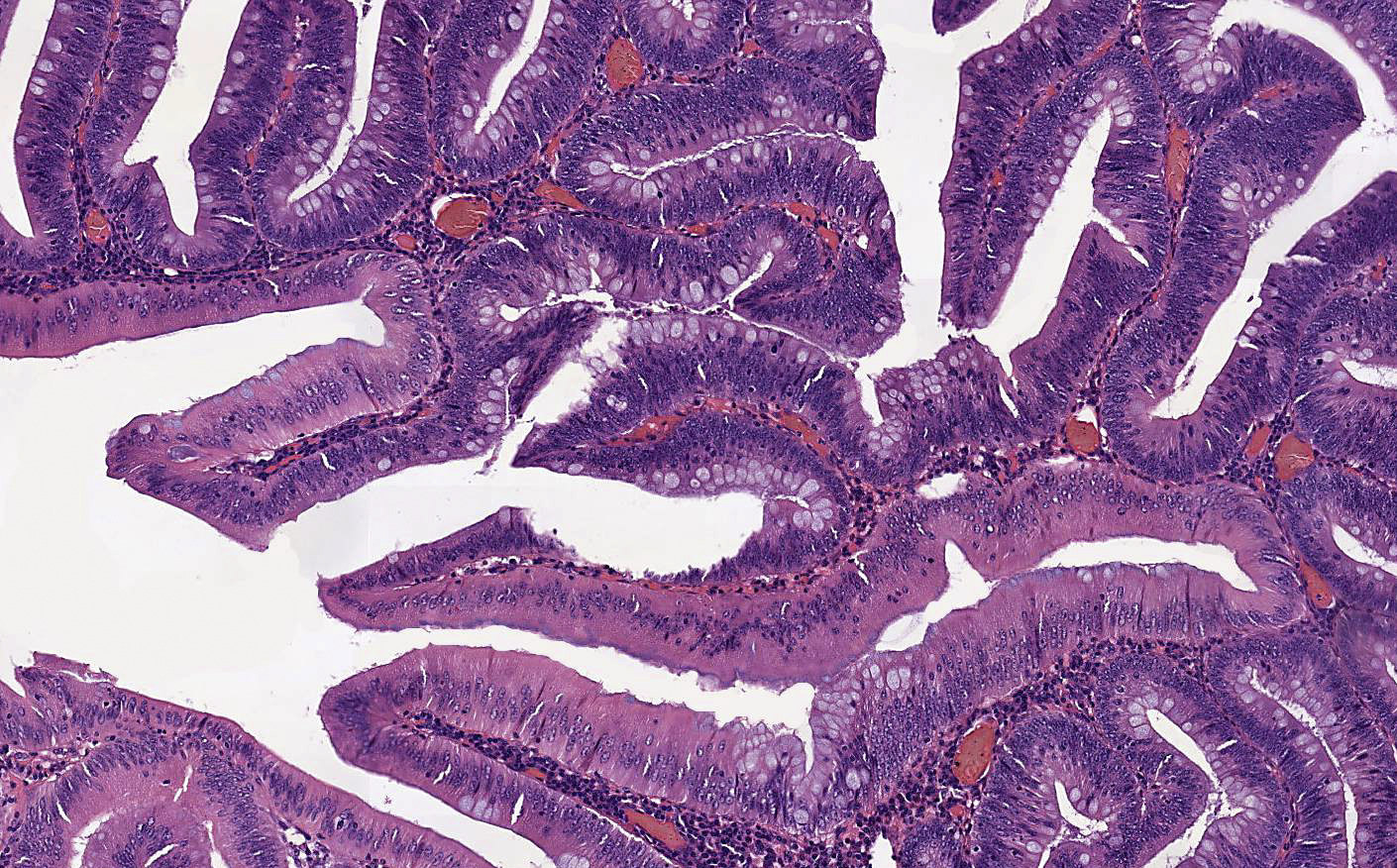
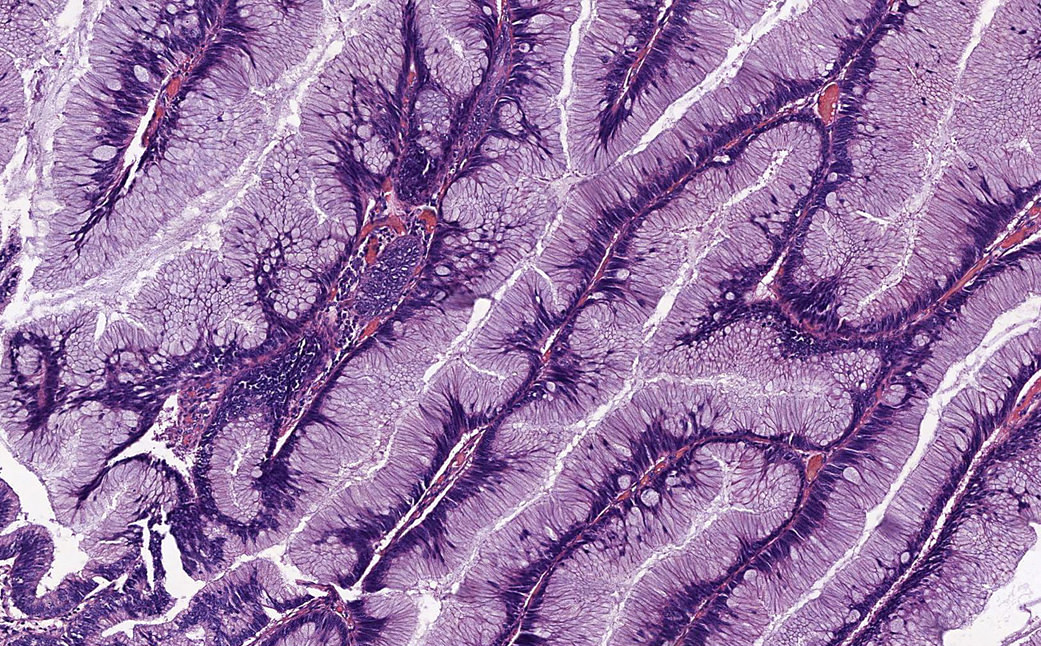
High grade dysplasia
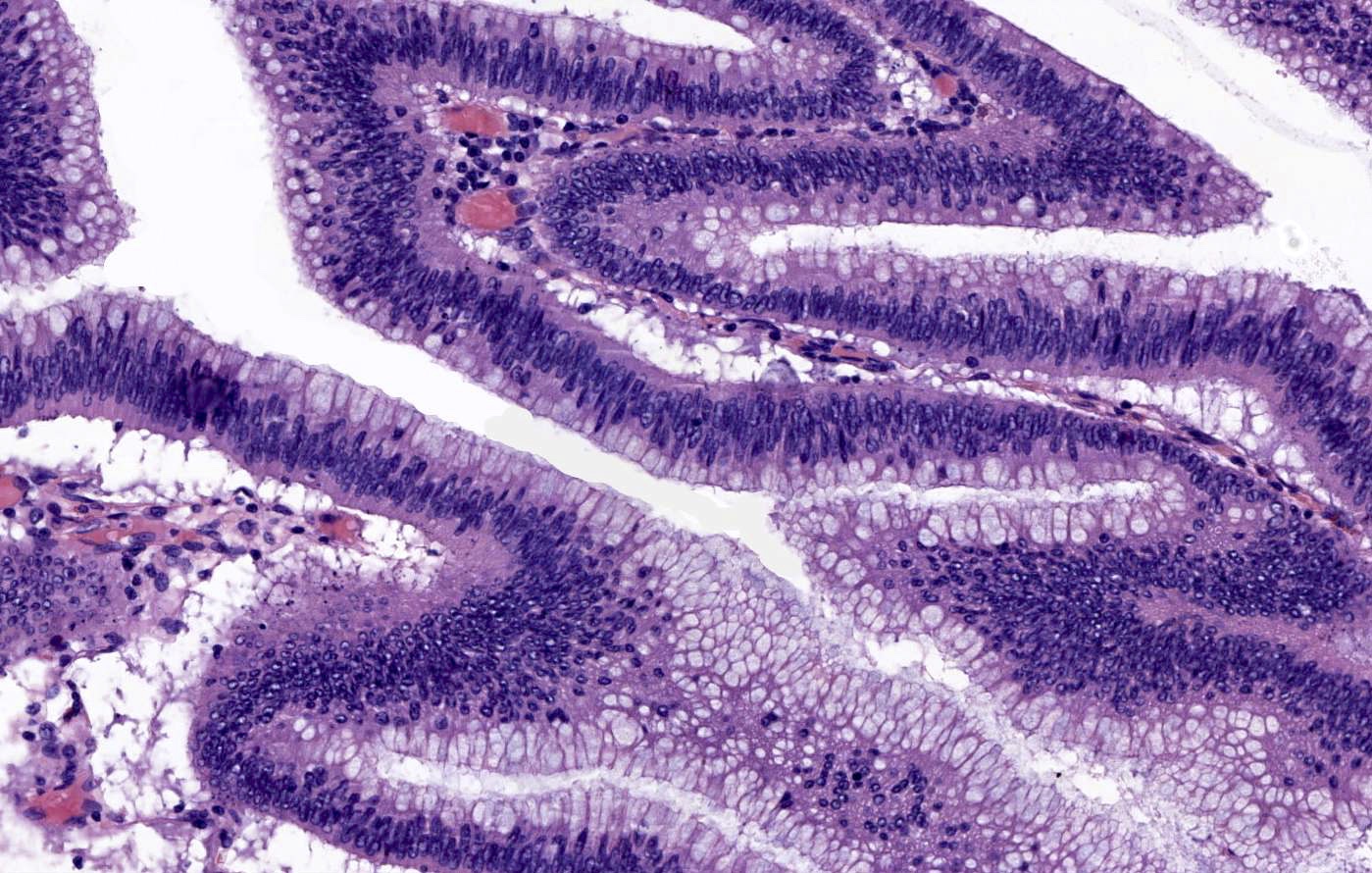
Low grade dysplasia
Villous architecture
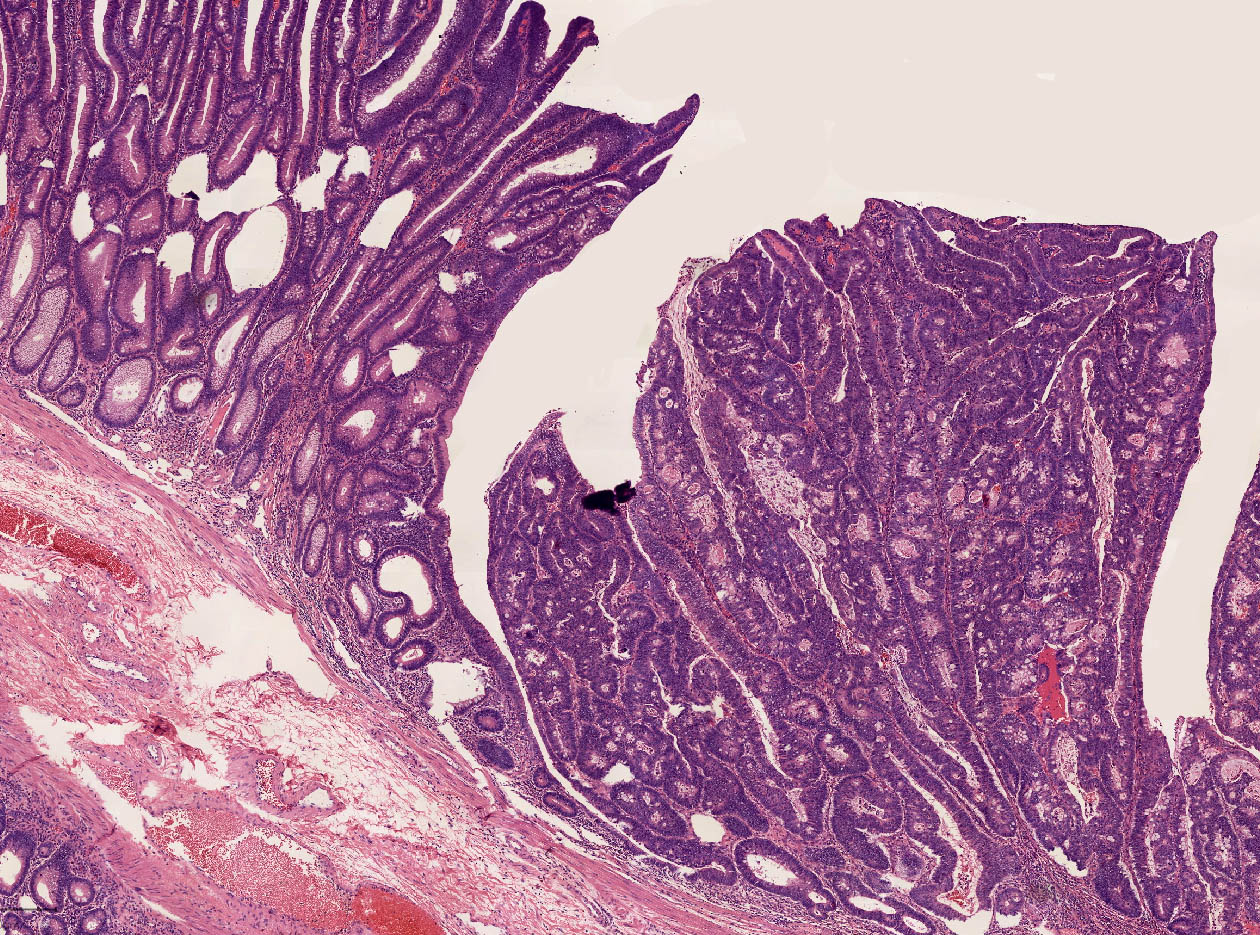
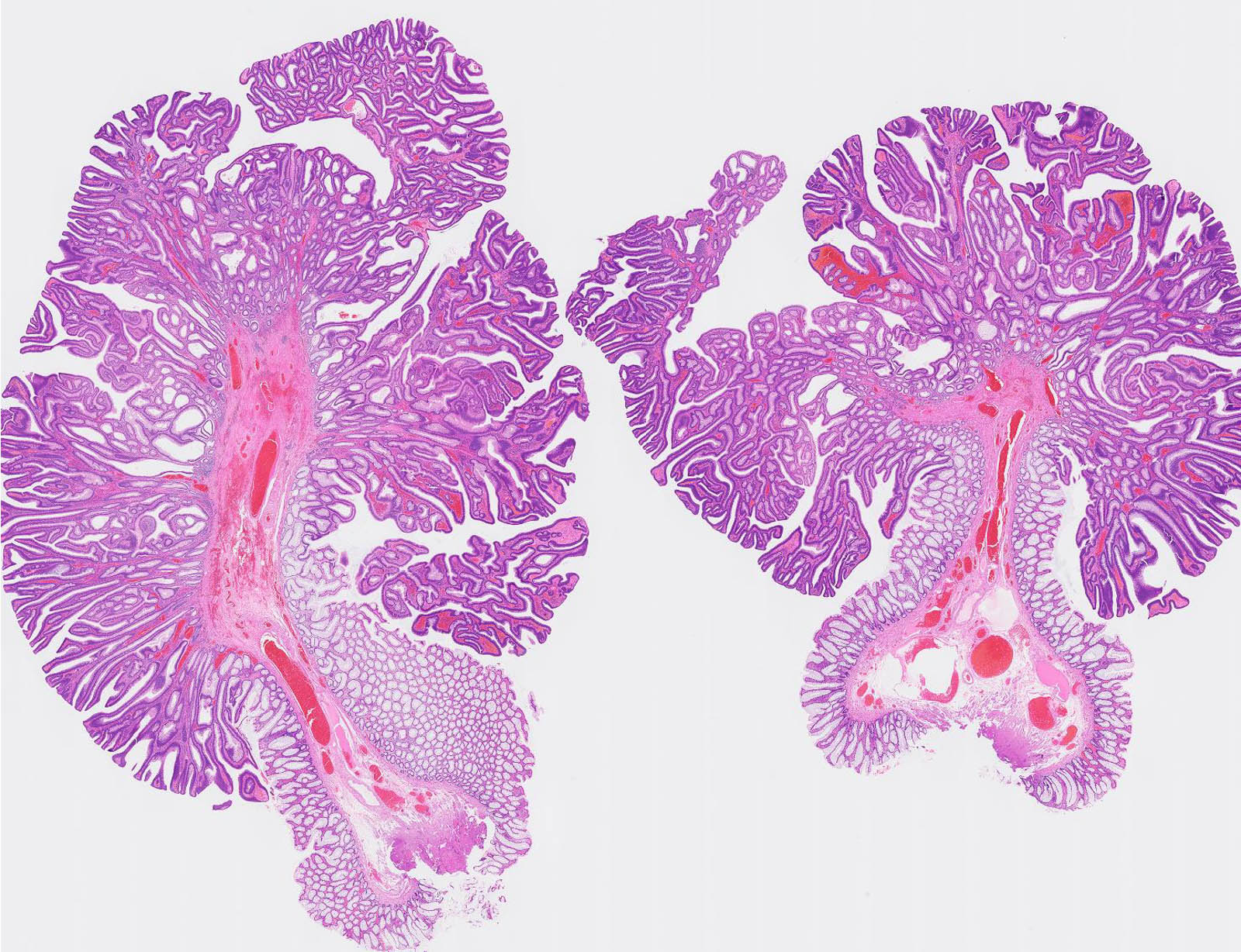
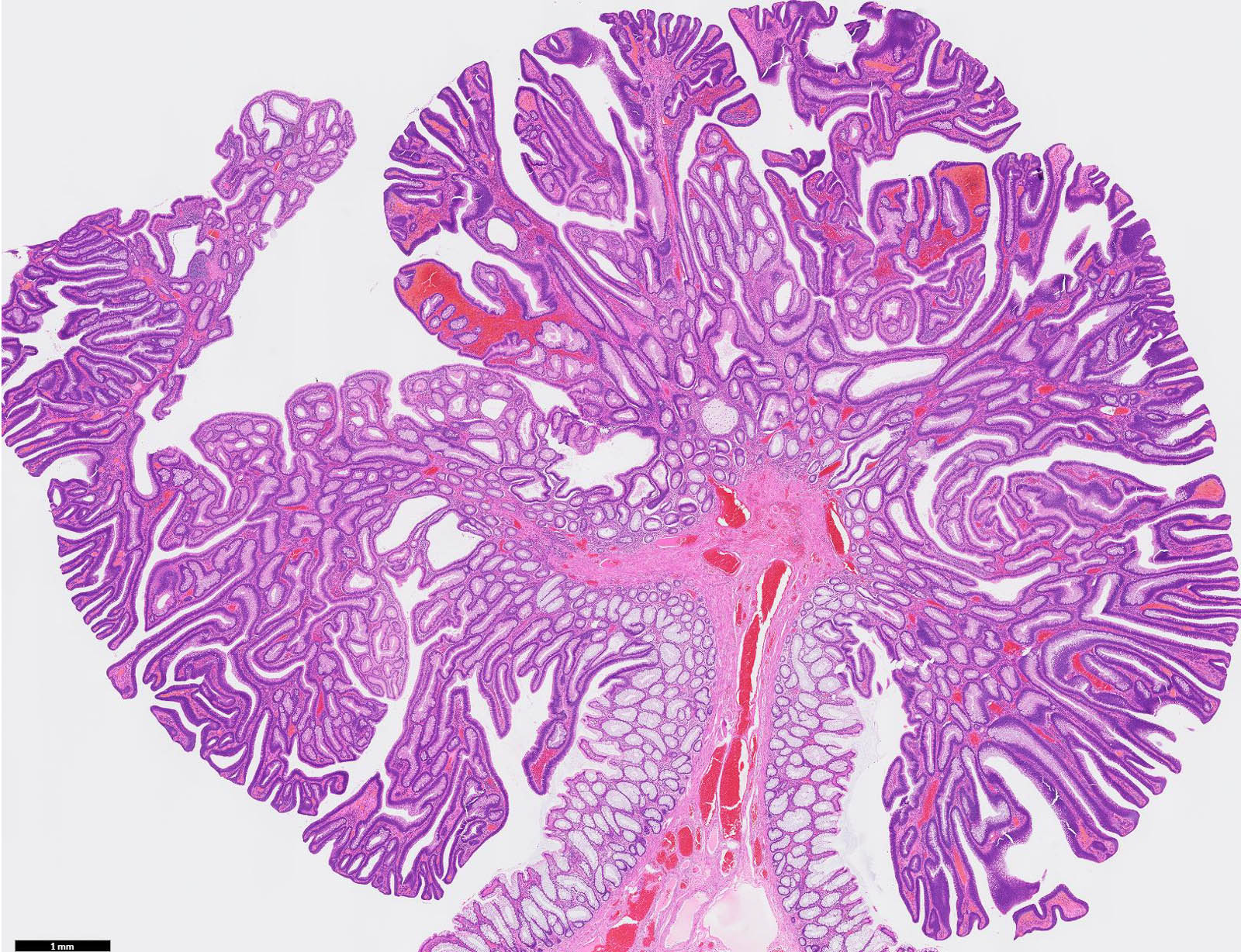
Giant rectal villous adenoma
Focal eosinophilic change
Ectopic crypt foci
Cut section
Pedunculated polyp
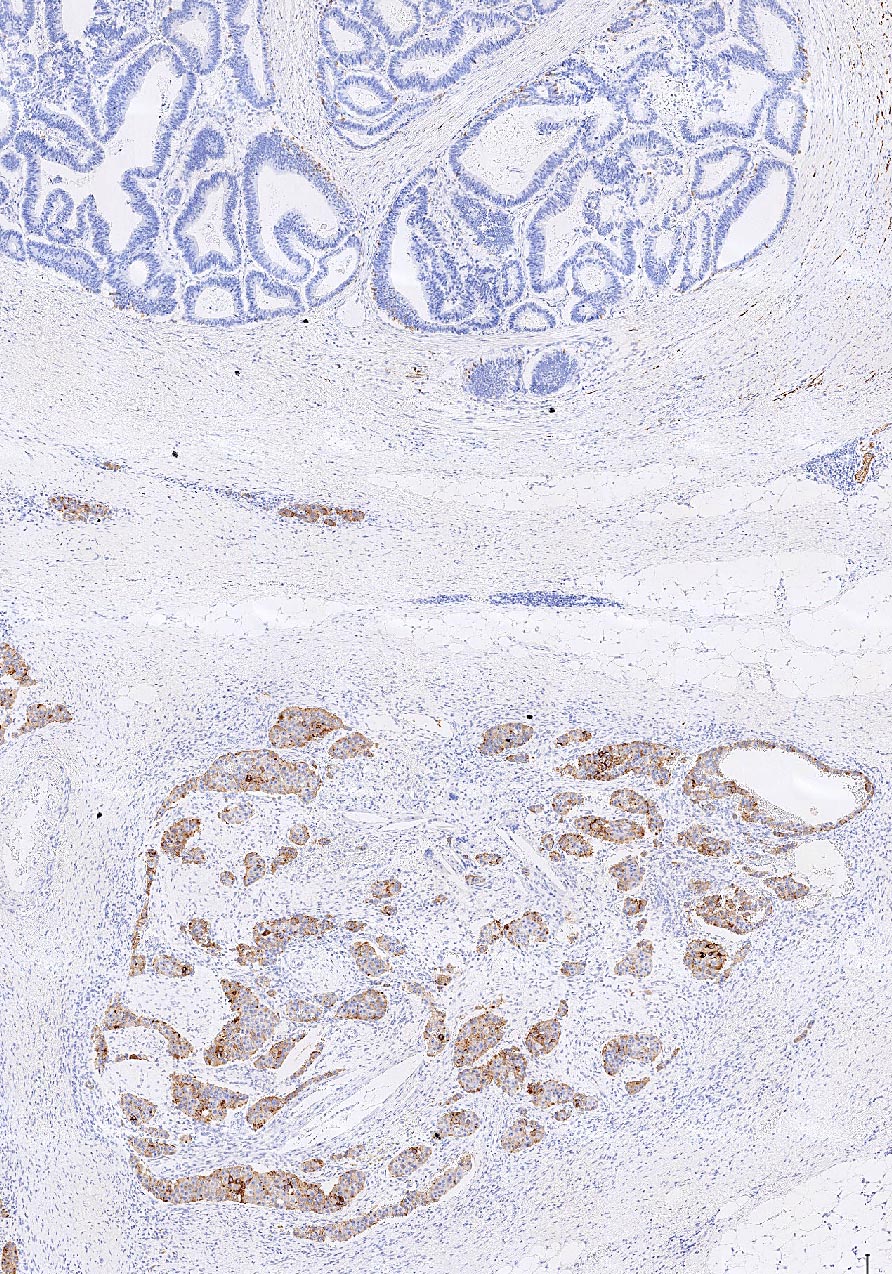
Neuroendocrine metaplasia (marker expression)

Neuroendocrine metaplasia (Ki67)
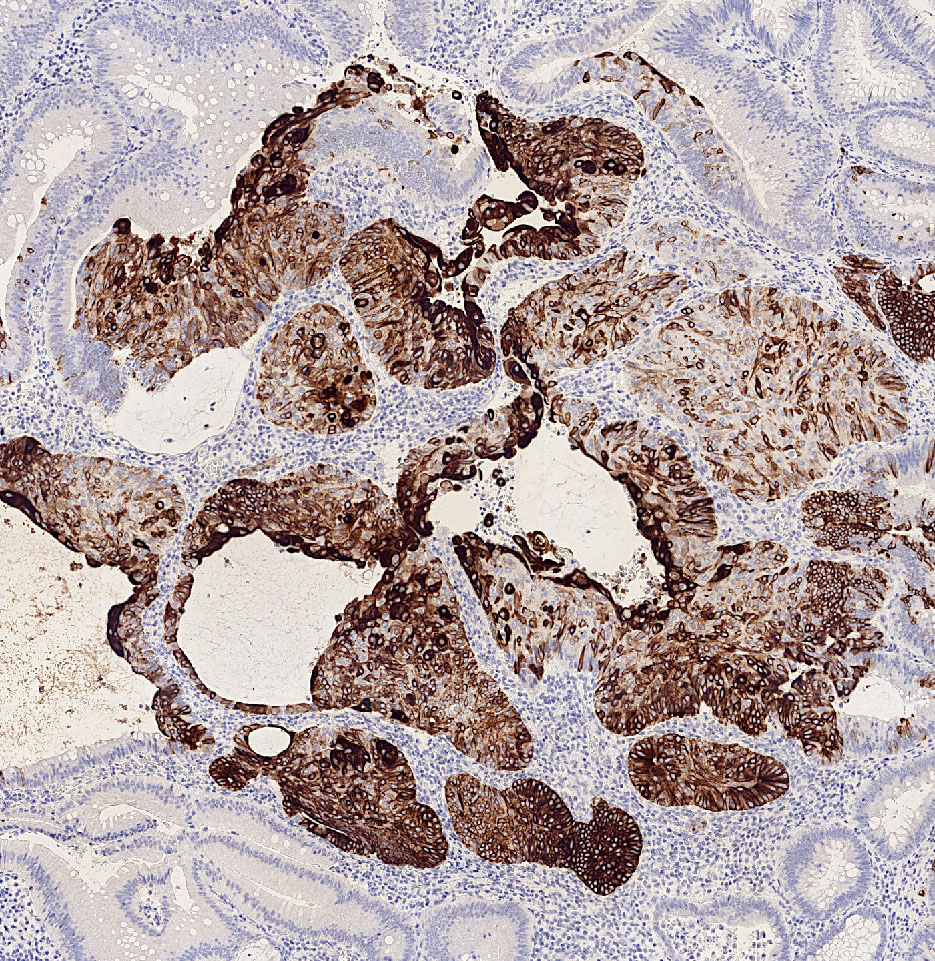
Squamous metaplasia (CK5/6)
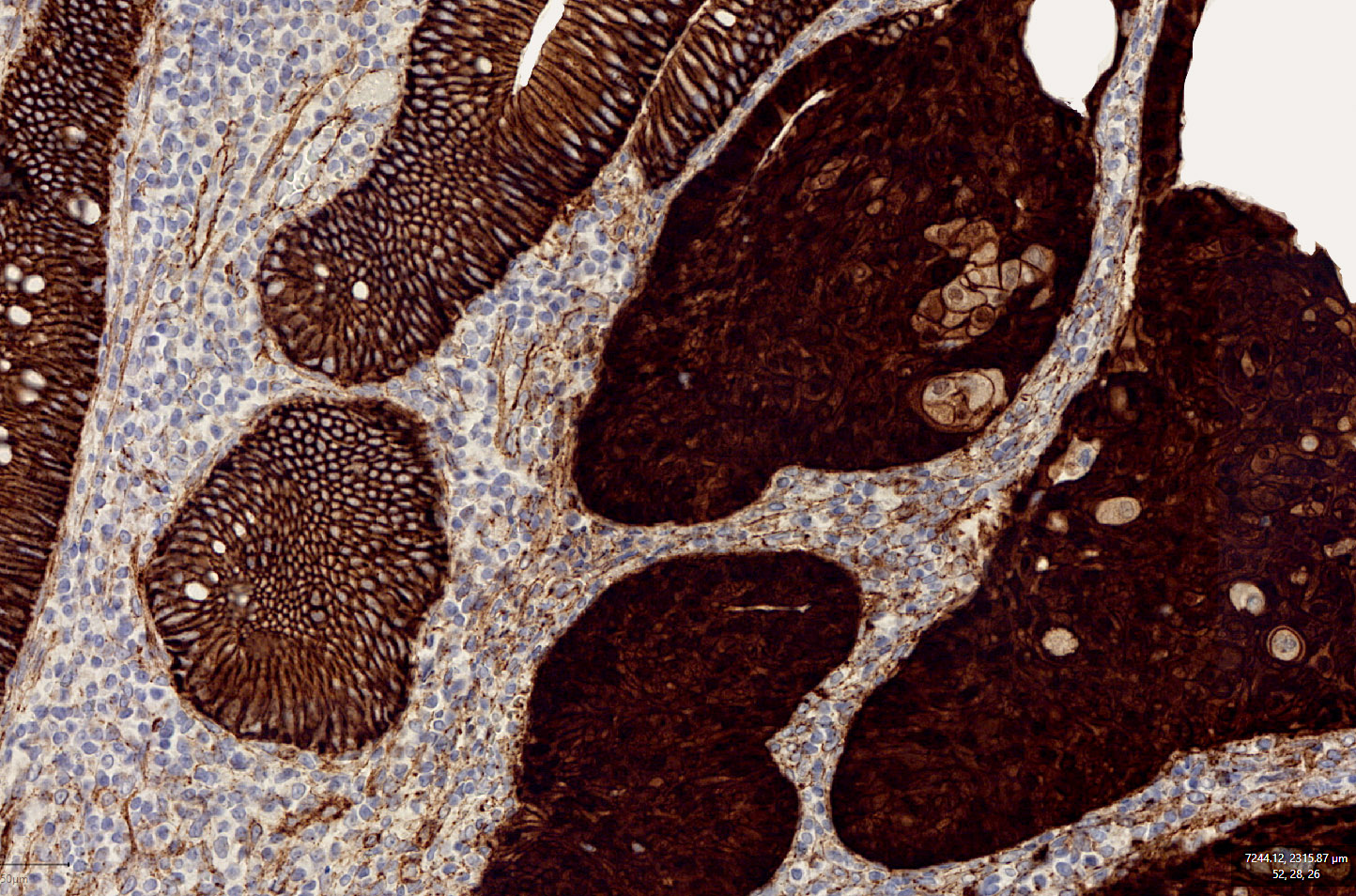
Squamous metaplasia (beta catenin)
Virtual slides
Images hosted on other servers:

Villous adenoma
Positive stains
- CK20: positive in 95% of cases (Dig Dis Sci 2005;50:1741)
- CDX2 (Gut 2002;51:184)
- p53: more frequent and intense in adenomas with high grade dysplasia (50%) than in those with low grade dysplasia (28%) (Am J Gastroenterol 1998;93:980)
- Beta catenin: cytoplasmic and nuclear immunoreactivity in areas of intestinal metaplasia (Histopathology 2021;78:348)
- CK5/6 and cyclin D1 overexpression in areas of squamous metaplasia (Histopathology 2021;78:348)
Negative stains
- CK7: usually negative but may be positive in approximately 5% of cases (Dig Dis Sci 2005;50:1741)
Molecular / cytogenetics description
- KRAS mutations in 52% (Pathol Oncol Res 2012;18:1077)
- Even subtle villous change in tubular adenoma is associated with more frequent KRAS and P53 mutations (Nat Rev Dis Primers 2015;1:15065)
- Routine screening of mismatch repair proteins (MMR) in polyps is not effective in identifying Lynch syndrome carriers (Clin Colorectal Cancer 2017;16:173)
- Most cases associated with Lynch syndrome show loss of MMR protein expression, especially when high grade dysplasia in present (Mod Pathol 2012;25:722)
Sample pathology report
- Colon, polyp at 12 cm, endoscopic polypectomy:
- Tubulovillous adenoma with high grade dysplasia
- Colon, polyp at 14 cm, endoscopic polypectomy:
- Villous adenoma
Differential diagnosis
- Traditional serrated adenoma:
- Exophytic tubulovillous or villous polypoid architecture with at least 2 of 3 constituent features (J Clin Pathol 2016;69:6, BMJ Open Gastroenterol 2019;6:e000317):
- Striking granular eosinophilic cytoplasm; prominent cytoplasmic eosinophilia that occupies > 50% of tubulovillous / villous adenoma is uncommon (Am J Surg Pathol 2011;35:212)
- Presence of ectopic crypt foci: more extensive small and short crypts with no relation to the underlying muscularis mucosae (Histopathology 2015;66:308)
- Luminal serration is defined as deep clefts and slit-like spaces that lead to broad luminal fronds imparting a mushroom-like appearance (not present in tubulovillous and villous adenoma) (Histopathology 2015;66:308)
- Exophytic tubulovillous or villous polypoid architecture with at least 2 of 3 constituent features (J Clin Pathol 2016;69:6, BMJ Open Gastroenterol 2019;6:e000317):
- Tubular adenoma:
- Adenomatous polyp with disorganized glands (tubular appearance) and flat surface
- May show some villous component, representing < 20% of the lesion (Am J Surg Pathol 2011;35:212)
- Adenoma-like adenocarcinoma:
- Invasive carcinoma with architectural and cytologic features resembling villous adenoma; differential diagnosis with villous adenoma may be a challenge
- Finding of epithelial islands surrounded by desmoplastic stroma favors this diagnosis (Am J Surg Pathol 2004;28:1460)
Practice question #1
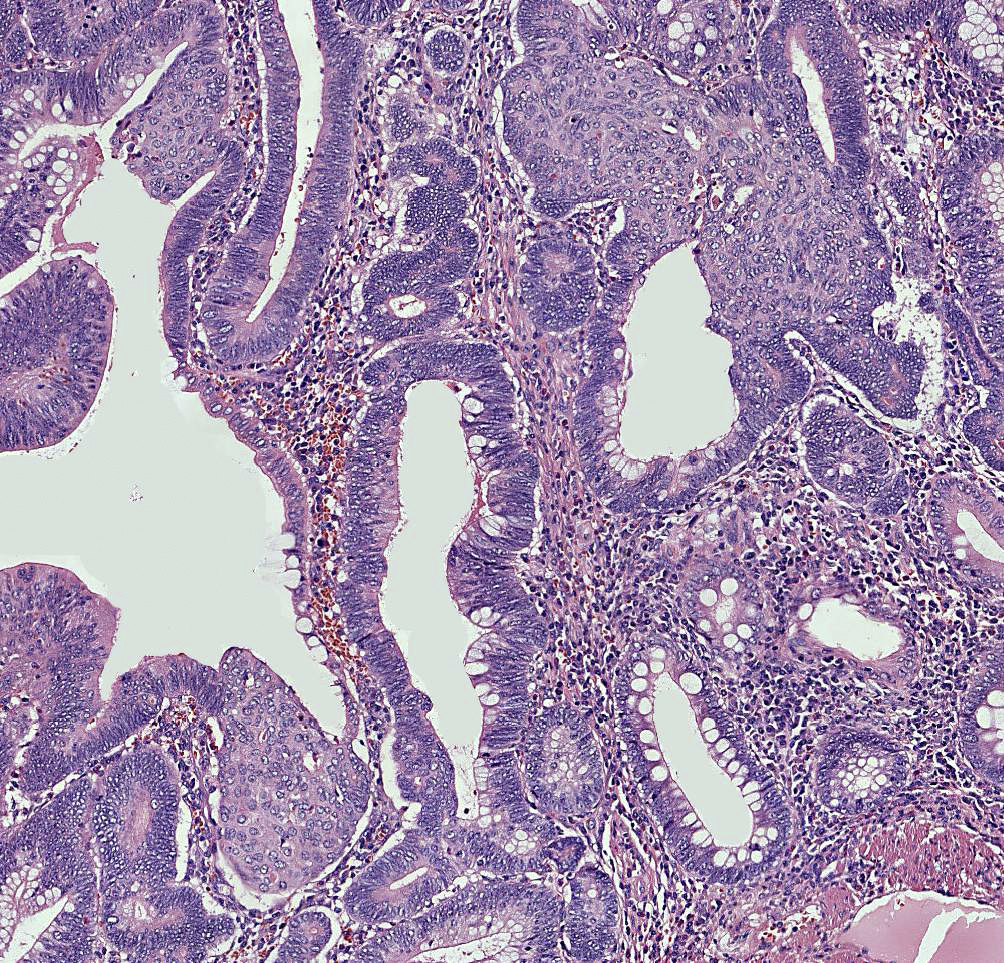
A colon polyp is resected. The image shown above is representative of the lesion. What is your diagnosis?
- Composite adenoma neuroendocrine carcinoma
- Composite adenoma neuroendocrine tumor
- Tubulovillous adenoma with high grade dysplasia
- Tubulovillous adenoma with squamous metaplasia
Practice answer #1
D. Tubulovillous adenoma with squamous metaplasia
Comment here
Reference: Tubulovillous / villous adenoma
Comment here
Reference: Tubulovillous / villous adenoma
Practice question #2
Which of the following is true about villous adenoma?
- Frequently associated with KRAS mutations
- Precursor lesion in the serrated pathway of colorectal development
- Presents the same risk of malignant transformation as tubular adenoma
- Routine screening of MMR proteins for Lynch syndrome in this lesion is useful
Practice answer #2
A. Frequently associated with KRAS mutations
Comment here
Reference: Tubulovillous / villous adenoma
Comment here
Reference: Tubulovillous / villous adenoma
