

Prostate gland & seminal vesicles
Acinar / ductal adenocarcinomas
Adenocarcinoma
Authors: Emma Short, B.M.B.Ch., Murali Varma, M.B.B.S.
Editorial Board Member: Bonnie Choy, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.


Last author update: 3 March 2022
Last staff update: 10 May 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Prostatic adenocarcinoma[TI] pathology review[PT]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Short E, Varma M. Adenocarcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/prostateadenoNOS.html. Accessed April 29th, 2024.
Definition / general
- Most common malignancy of the prostate gland
- Originates from prostatic secretory epithelium
Essential features
- Clinical and radiological features neither sensitive nor specific
- Often diagnosed by nontargeted needle biopsies investigating raised serum prostate specific antigen (PSA)
- Absence of basal cell layer is a pathognomonic histological feature
- Pathognomonic diagnostic features: circumferential perineural invasion, glomerulations and collagenous micronodules (mucinous fibroplasia)
- Other histological features: infiltrative architecture, nucleolar prominence, amphophilic cytoplasm and some intraluminal contents (crystalloids, blue mucin, pink amorphous material)
Terminology
- Prostate cancer
- Prostate adenocarcinoma
- Subtypes of prostatic adenocarcinoma: acinar adenocarcinoma, ductal adenocarcinoma, atrophic adenocarcinoma, pseudohyperplastic adenocarcinoma, microcystic adenocarcinoma, foamy gland adenocarcinoma, mucinous adenocarcinoma, signet ring variant of adenocarcinoma, pleomorphic giant cell adenocarcinoma, sarcomatoid adenocarcinoma
Epidemiology
- Second most common cancer and second leading cause of cancer related death in American men (SEER data available at NIH: Cancer Stat Facts - Common Cancer Sites [Accessed 10 December 2021])
- 92% of U.S. cases diagnosed in men aged 55+ years; 19.5% in men aged 75+ years (SEER data available at NIH: Cancer Stat Facts - Prostate Cancer [Accessed 10 December 2021])
- Found at autopsy in 40% of men age 60+ years (J Natl Cancer Inst 2013;105:1050)
- Incidental prostate cancer reported in about 25% of cystoprostatectomies performed for treatment of bladder cancer (J Urol 2017;197:385)
- Globally, highest age standardized rates in Oceania, North America, Europe (World J Oncol 2019;10:63)
- Lower rates in developing countries: may be due to different screening programs and diagnostic pathways
- Higher incidence in men of African heritage (World J Oncol 2019;10:63)
Sites
- Most tumors are multifocal (Eur Urol 2019;75:498)
- 75 - 80% are posterior / posterolateral peripheral zone
- Approximately 13 - 20% are in transition (periurethral) zone (Prostate 1997;30:130, Urology 1994;43:11)
- Most clinically significant cancers arise in the peripheral zone that is sampled by needle biopsies
- Transition zone prostate cancer is associated with favorable pathologic features and better recurrence free survival (Prostate 2015;75:183)
- Less frequently involved anterior prostate most likely due to inadequate sampling using standard biopsy approach (Histopathology 2012;60:142)
Pathophysiology
- Germline variants can increase risk of prostate adenocarcinoma; see Molecular / cytogenetics description
- Somatic mutations in genes such as ERG, ETV1/4, FLI1, SPOP, FOXA1, IDH1, PTEN, TP53, MYC, CDH1 (Cell 2015;163:1011, Adv Anat Pathol 2020;27:11)
- Most common somatic genomic rearrangement is fusion of the androgen regulated gene TMPRSS2 with a member of the ETS transcription family (Adv Anat Pathol 2020;27:11)
Etiology
- Obesity increases risk (Oncotarget 2018;9:34485)
- Nonmodifiable risk factors: age, race and family history (Rev Urol 2002;4:S3)
- Genetic susceptibility linked to African heritage (Rev Urol 2002;4:S3)
- Increased risk with first degree relative with prostate cancer (Rev Urol 2002;4:S3)
- BRCA2 mutations increase risk by 5 fold; BRCA2 associated cancers occur at a lower age and have worse survival outcomes (Saudi Med J 2020;41:9, Adv Anat Pathol 2020;27:11)
- Additional germline variants associated with increased cancer risk occur in HOXB13 (Adv Anat Pathol 2020;27:11)
- Increased risk in Lynch syndrome (Genet Med 2014;16:553)
- Numerous single nucleotide polymorphisms (SNPs) that have a low to moderate effect on risk / progression have been identified (Am J Transl Res 2021;13:3868)
- High levels of IGF1 may confer increased risk (Novartis Found Symp 2004;262:193)
Clinical features
- Generally asymptomatic unless locally advanced or metastatic
- Often discovered following investigation of nonspecific lower urinary tract symptoms
- Digital rectal examination (DRE): prostate may feel normal or may be enlarged / asymmetrical / hard / have a palpable nodule present
Diagnosis
- Generally diagnosed by systematic transrectal ultrasound guided prostate biopsies
- Transperineal needle biopsies increasingly used as associated with lower risk of infection
- Prebiopsy MRI followed by systematic biopsies supplemented with targeted biopsies from any radiological abnormality leads to better identification of clinically significant prostate cancer than systematic prostate biopsy alone (Lancet 2017;389:815)
- Incidental prostate cancer sometimes diagnosed in transurethral resections
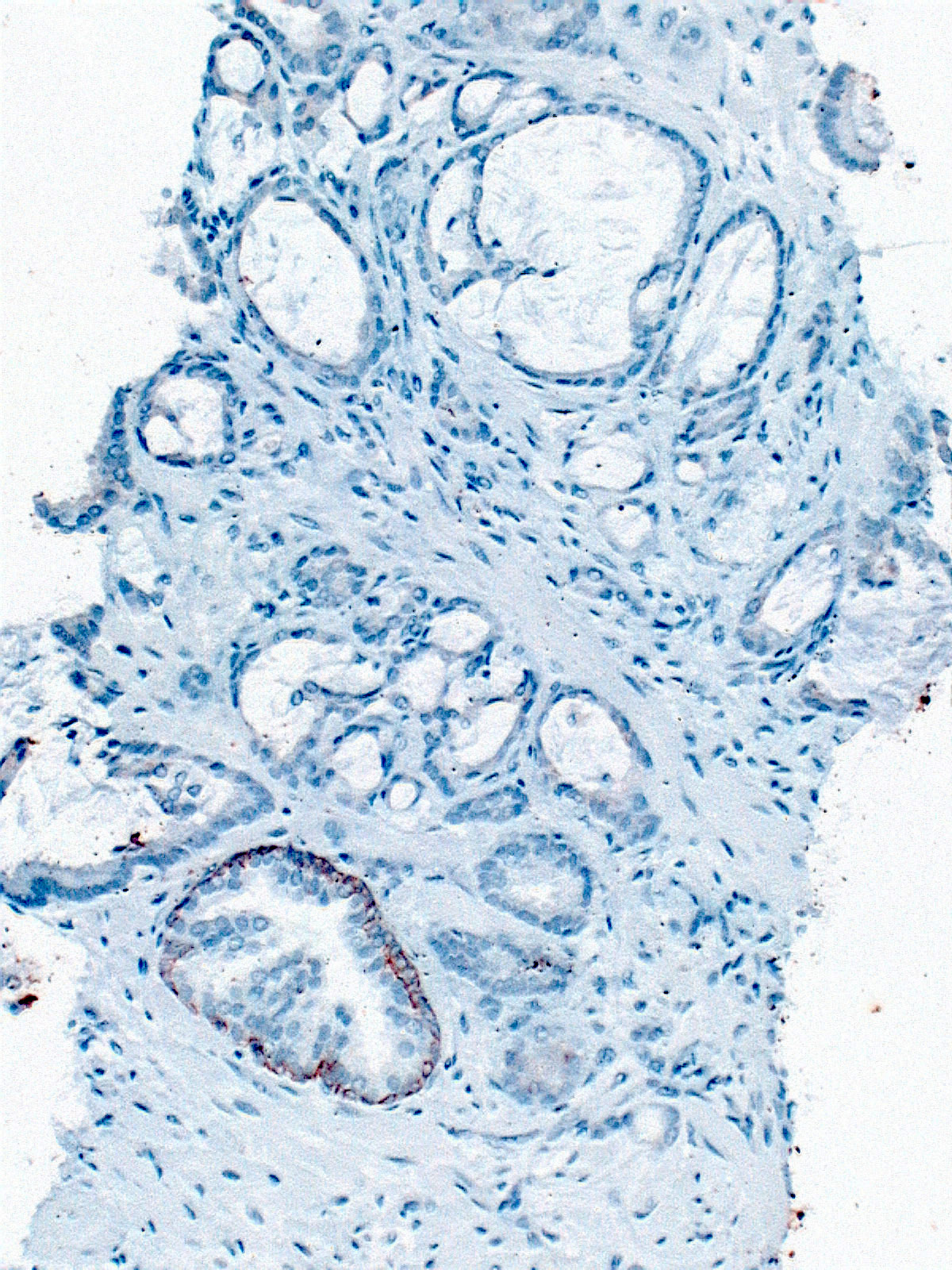
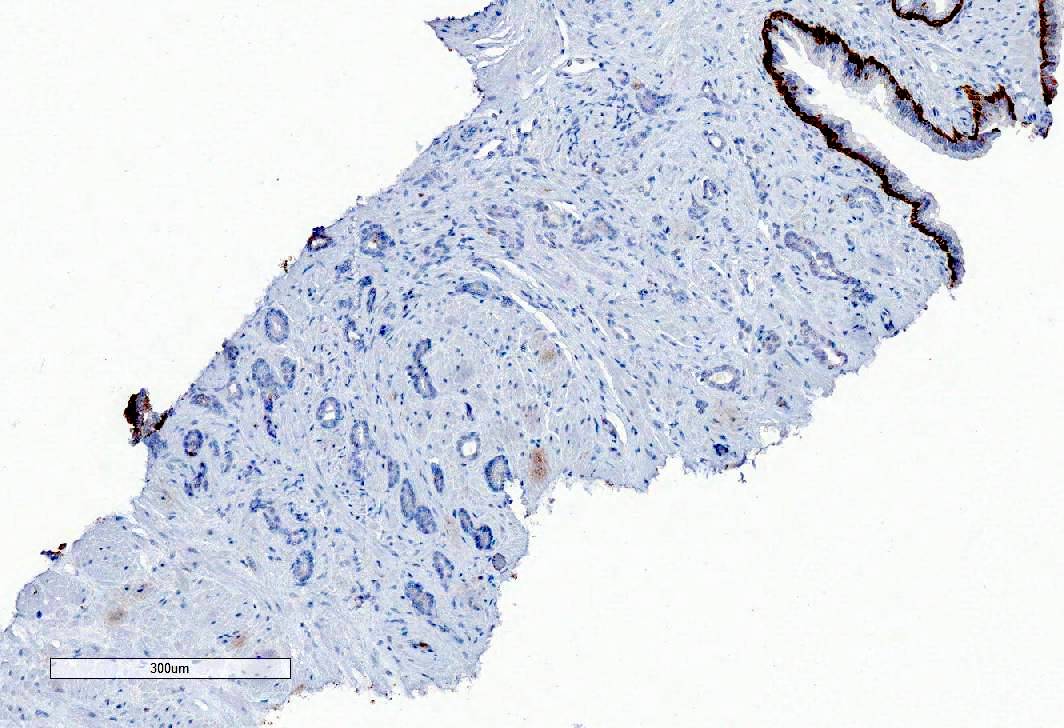
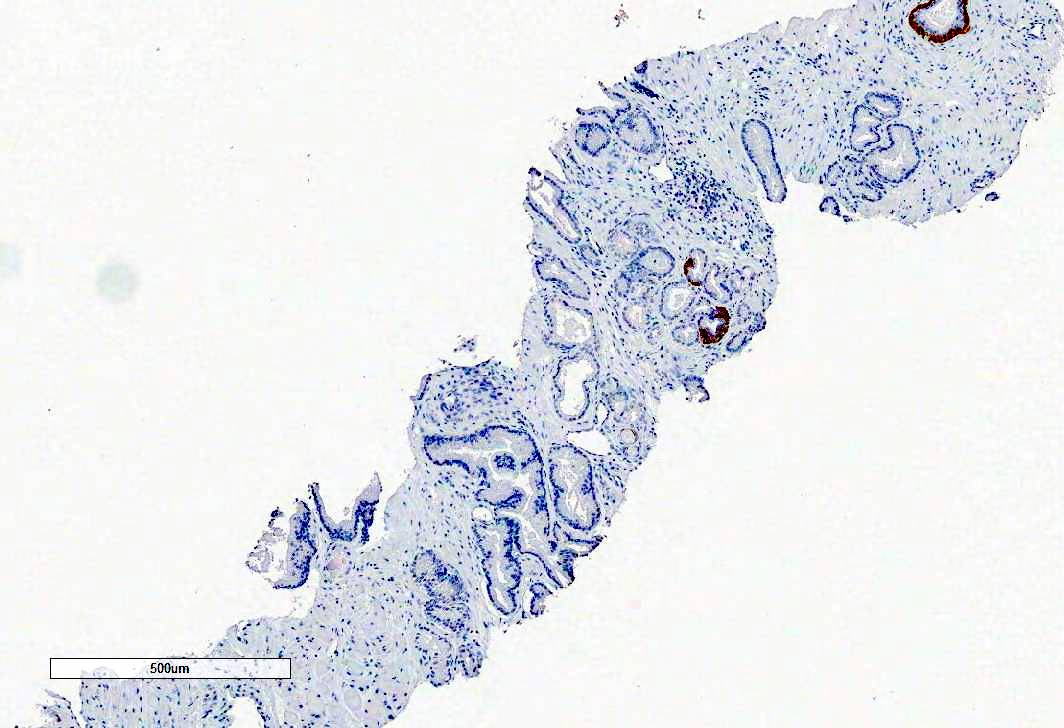
- Immunohistochemistry with basal cell markers (HMWCK, p63) and AMACR used to establish the diagnosis in equivocal cases
Laboratory
- Raised serum PSA
- Different PSA cutoffs have been used to prompt prostate needle biopsy
- Age specific cutoffs, PSA velocity (rate of change in PSA over time) and PSA density (PSA per unit prostate volume - ng/mL/cc) may increase sensitivity and specificity of PSA testing (NCCN Guidelines: Prostate Cancer Early Detection [Accessed 10 December 2021])
- U.S. Preventative Services Task Force (USPSTF) recommends against PSA based screening for prostate cancer in men 70 years and older
- For men aged 55 - 69 years, periodic PSA based screening should be an individual choice
- Screening in this age group offers a small potential benefit of reducing the chance of death from prostate cancer in some men; however, many men will experience potential harm (USPSTF: Recommendation - Prostate Cancer - Screening [Accessed 27 January 2022])
- American Urological Association (AUA) does not recommend PSA screening in men under age 40 years or in men aged 40 - 54 years at average risk
- For men age 55 - 59 years, shared decision making is desirable
- For men aged 70 years and over or men with < 10 - 15 year life expectancy, PSA screening is not recommended (J Urol 2013;190:419)
- Potential urine biomarker for prostate cancer is PCA3 (Adv Anat Pathol 2020;27:11)
Radiology description
- Ultrasound scan (USS) generally used to guide prostate biopsies; prostate cancer may appear hypoechoic but USS neither sensitive nor specific
- Multiparametric MRI commonly used for local tumor staging; may also be used to identify abnormalities for targeting at biopsy
- MRI abnormalities generally reported using either PI-RADS (Prostate Imaging - Reporting and Data System) or Likert score
- CT scan used to identify metastatic disease in lymph nodes
- Bone scan used to detect bony metastases
- PET scan used to detect micrometastatic disease in selected patients, such as men with raised PSA levels after treatment
Prognostic factors
- Biopsy: tumor extent (mm or percentage core involvement), grade (Gleason score and grade group), perineural invasion, extraprostatic extension
- Radical prostatectomy: tumor size, Gleason score and grade group, stage, margin status
- Cribriform morphology and intraductal carcinoma associated with invasive prostate cancer are adverse prognostic indicators (Transl Androl Urol 2018;7:145)
- Small cell carcinoma component is associated with aggressive behavior and treated differently
- Some expert groups recommend incorporating intraductal component into the Gleason score while others recommend reporting it separately in a comment (Am J Surg Pathol 2020;44:e87, Arch Pathol Lab Med 2021;145:461, Histopathology 2021;78:231)
Case reports
- 53 year old man presented with prostate adenocarcinoma with retained basal cells in lymph node metastases (Histopathology 2016;69:338)
- 56 year old man with gait disturbance was found to have disseminated prostate carcinoma with bone metastases and a germline mutation in BRCA2 (J Korean Med Sci 2017;32:377)
- 60 year old man presented with metastatic prostate adenocarcinoma to supraclavicular lymph nodes (J Clin Diagn Res 2017;11:PD06)
- 64 year old man with asymptomatic case of oncocytic variant of prostate adenocarcinoma (World J Clin Oncol 2017;8:289)
Treatment
- Preoperative risk stratification based on serum PSA, clinical stage, biopsy parameters (tumor extent, grade, cribriform morphology, intraductal carcinoma, perineural invasion)
- Primary treatment options based on preoperative risk stratification:
- Active surveillance
- Focal therapy (cryotherapy, high intensity ultrasound)
- Radical prostatectomy
- Brachytherapy
- External beam radiotherapy
- Hormone therapy (e.g., luteinizing hormone releasing hormone [LHRH] analogues, antiandrogens)
- Orchidectomy (rare in contemporary practice)
- Chemotherapy (for metastatic disease)
- Postprostatectomy options:
- Generally, PSA monitoring and early salvage therapy if rising serum PSA
- Less commonly adjuvant therapy for high stage disease or margin positivity
Gross description
- Often grossly inapparent
- May form a cream mass
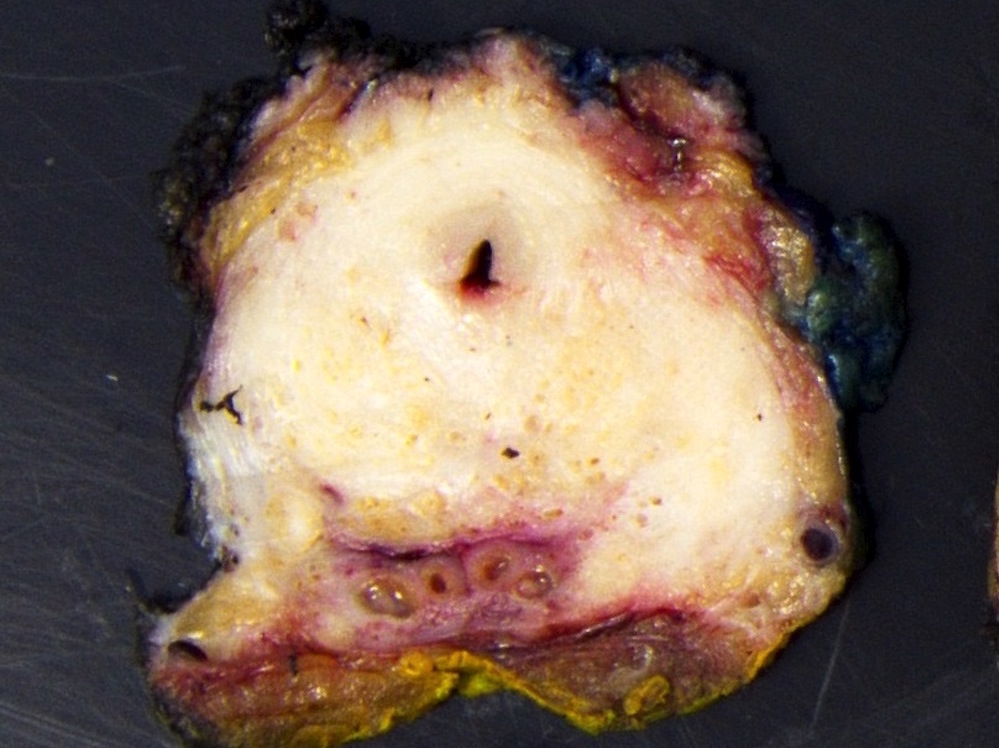
Gross images
Contributed by Debra Zynger, M.D. and Kenneth A. Iczkowski, M.D.
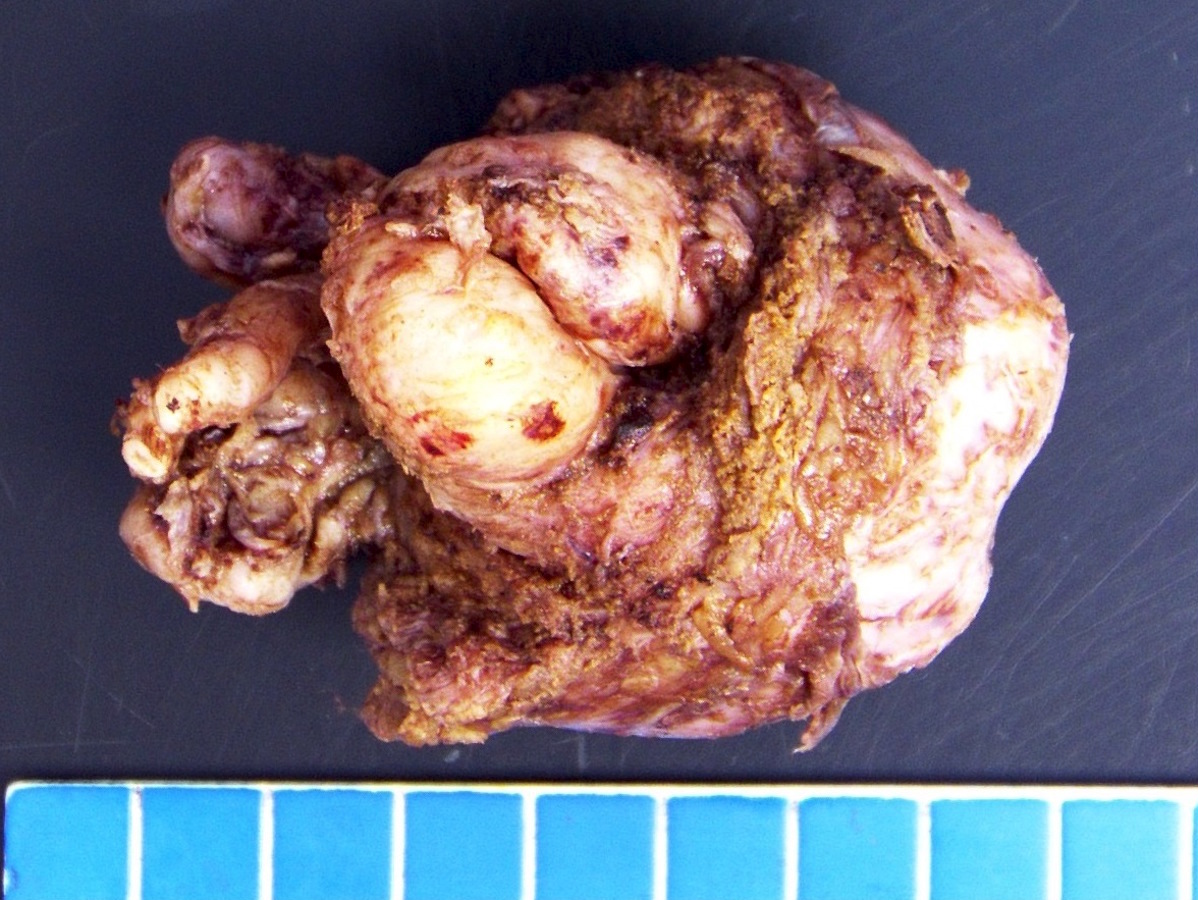
Prostatectomy specimen
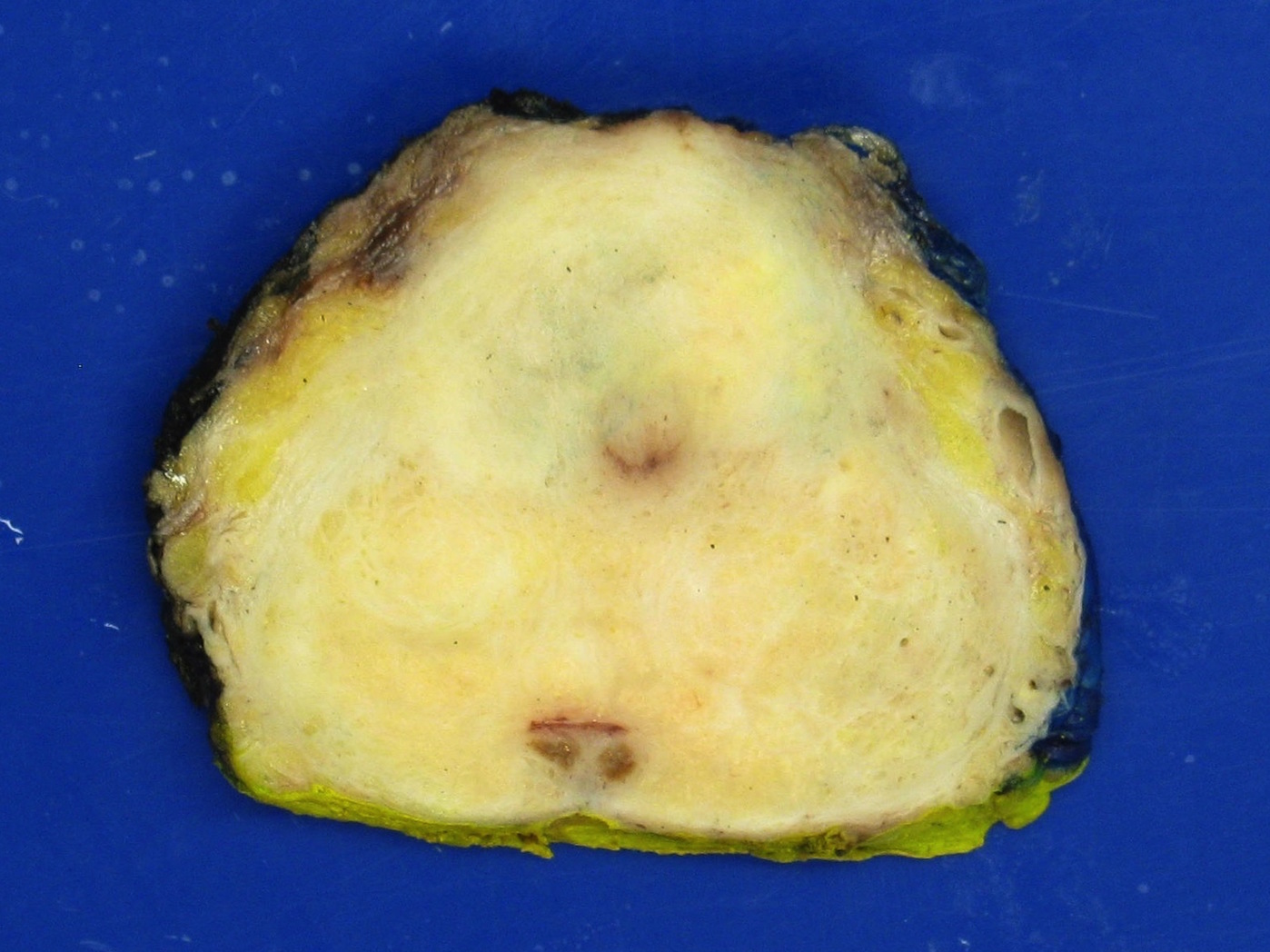
Extraprostatic extension (pT3a)
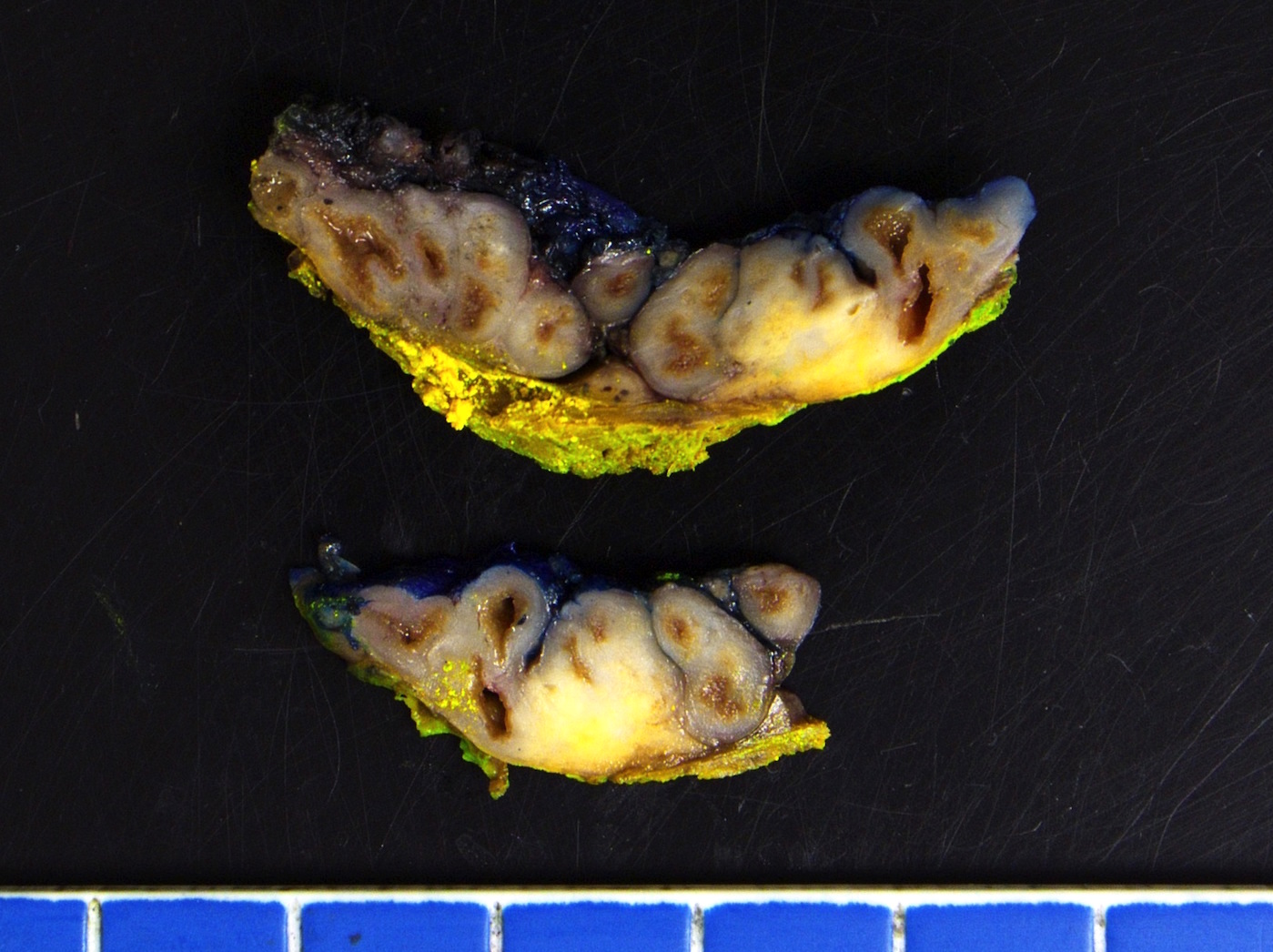
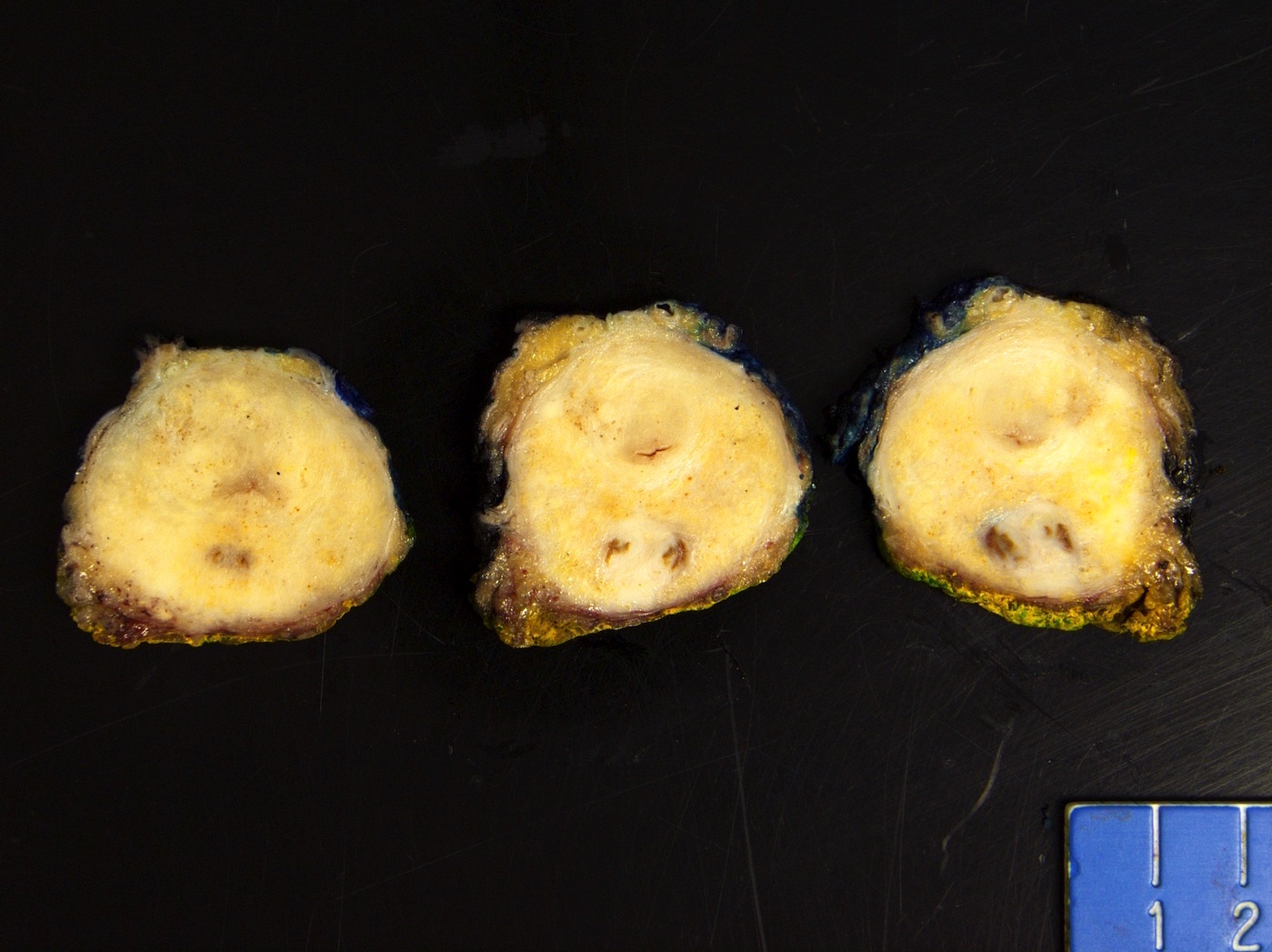
Seminal vesicle invasion (pT3b)

Anterior horn of
peripheral zone
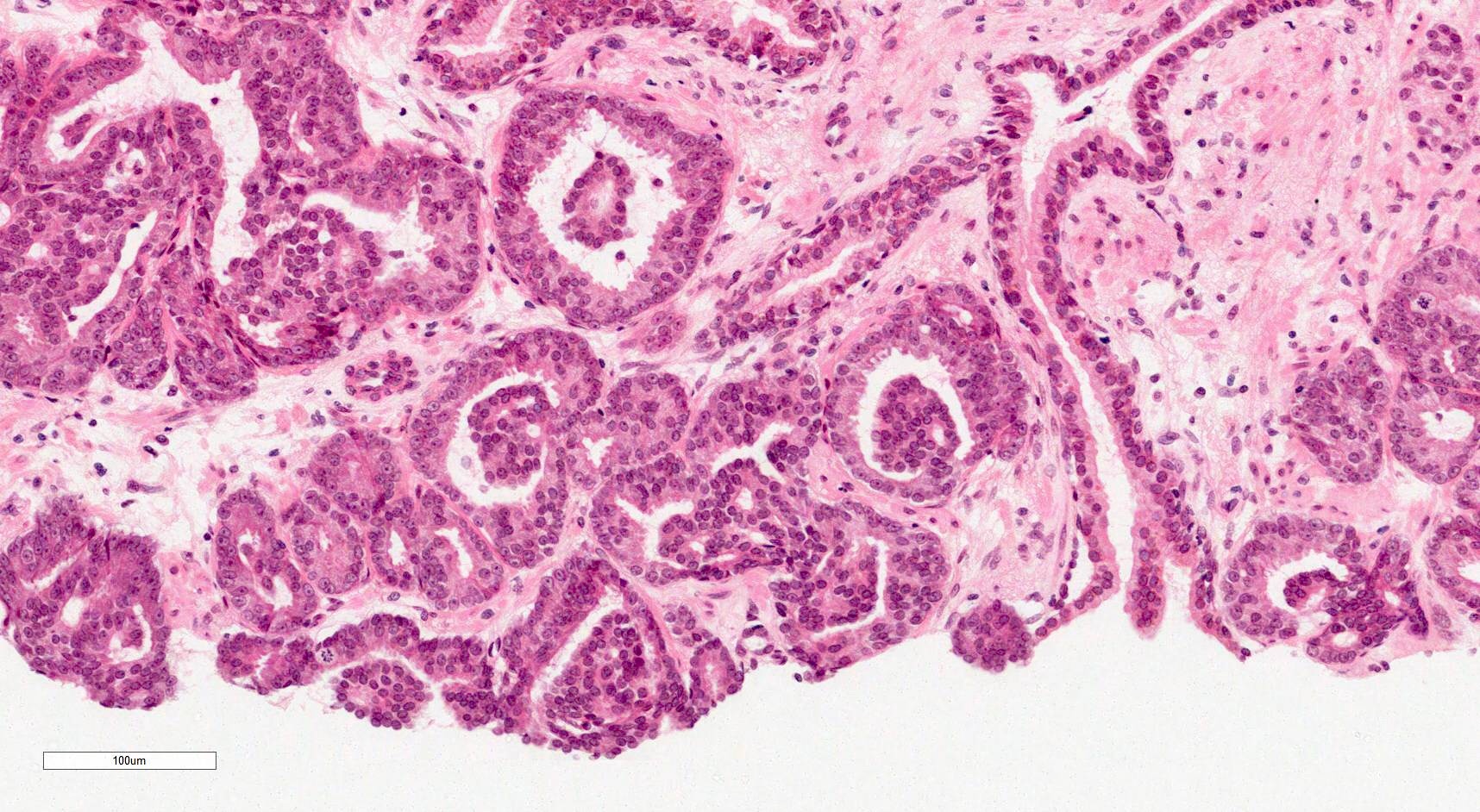
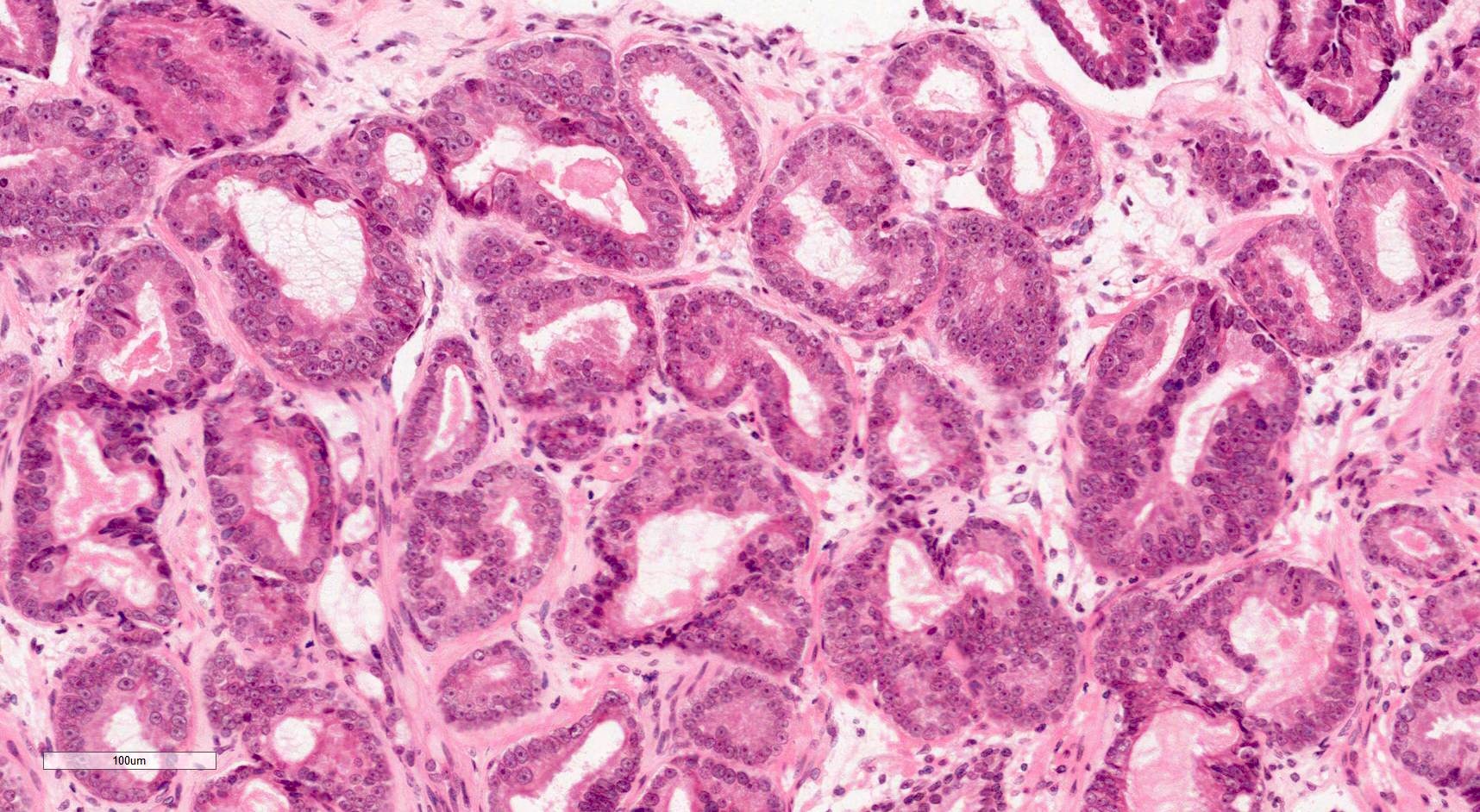
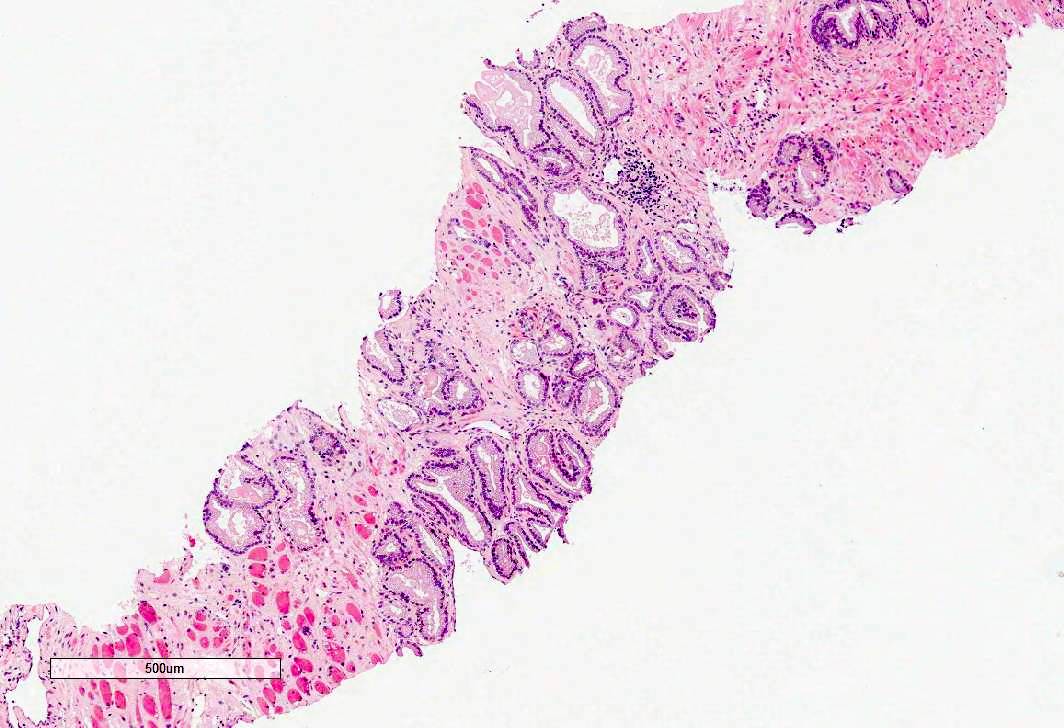
Microscopic (histologic) description
- Gleason grading is based on the architecture of the tumor
- Gleason grades represent a morphological spectrum from well formed glands (pattern 3) to increasingly complicated glandular proliferations (pattern 4) to almost no glandular differentiation (pattern 5) (Diagnostic Histopathology 2019;25:371)
- Glandular crowding and infiltrative growth pattern
- Nuclear enlargement, nucleolar prominence
- Round generally monomorphic nuclei
- Amphophilic cytoplasm
- Mitoses
- Apoptotic bodies
- Stromal desmoplasia
- Intraluminal contents: crystalloids, pink amorphous secretions, blue mucin
- Glomerulations, collagenous micronodules (mucinous fibroplasia)
- Absence of basal cell layer (generally requires immunohistochemical confirmation)
- Reference: Cold Spring Harb Perspect Med 2017;7:a030411
Microscopic (histologic) images
Contributed by Murali Varma, M.B.B.S.
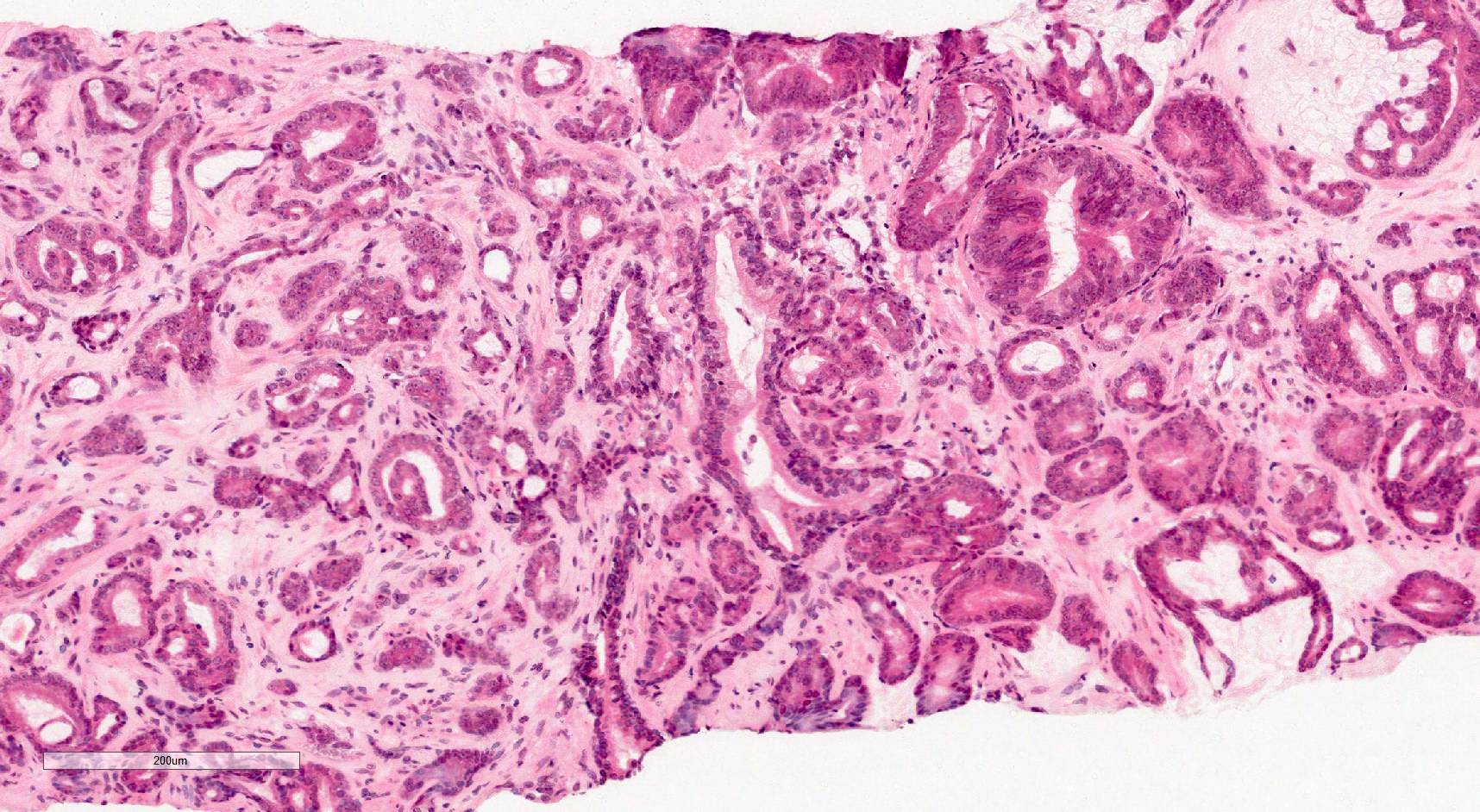
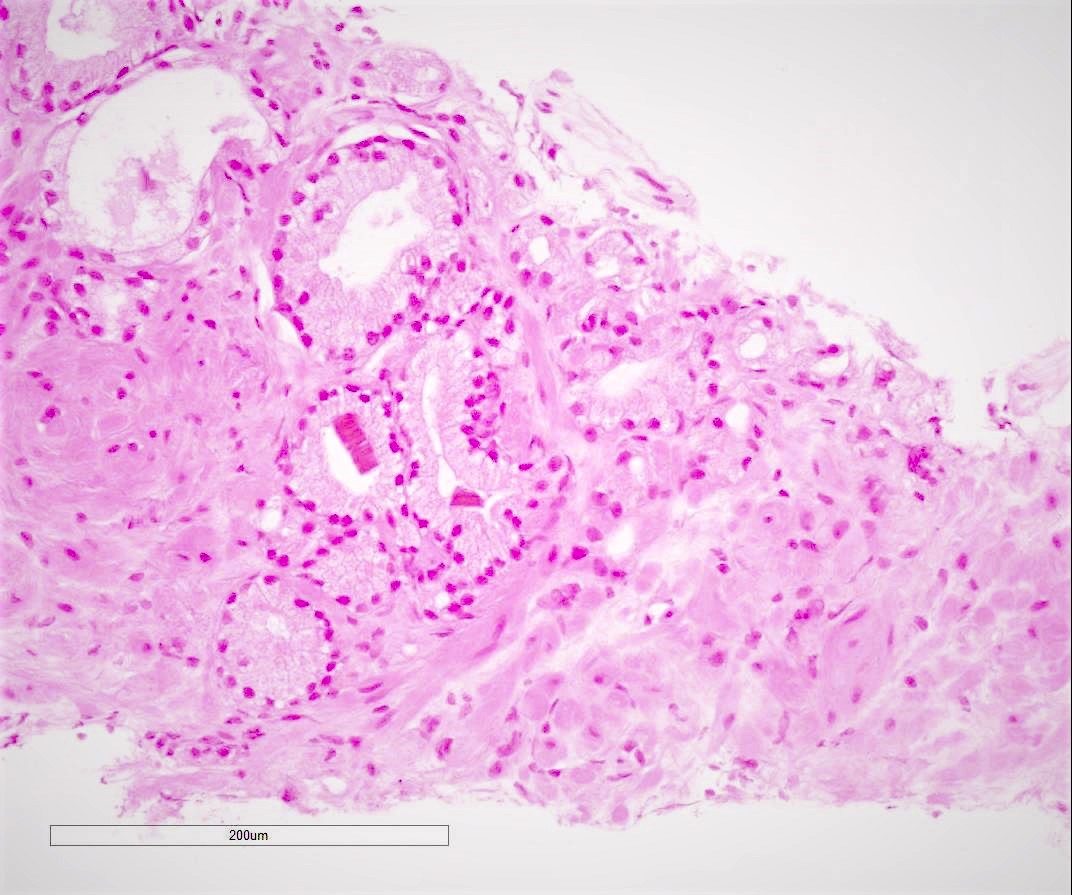
Infiltrative growth pattern
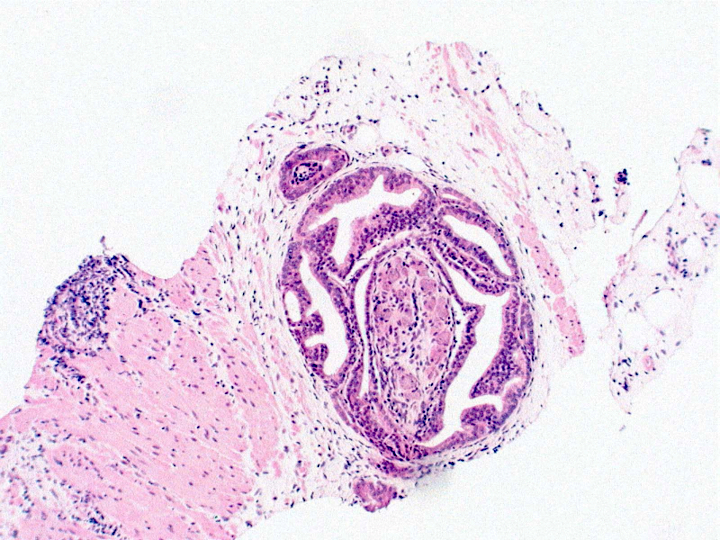
Glomerulations
Prominent nucleoli
Perineural invasion
Atrophic variant of prostate cancer
Atrophic variant of prostate cancer
Pseudohyperplastic variant of prostate cancer
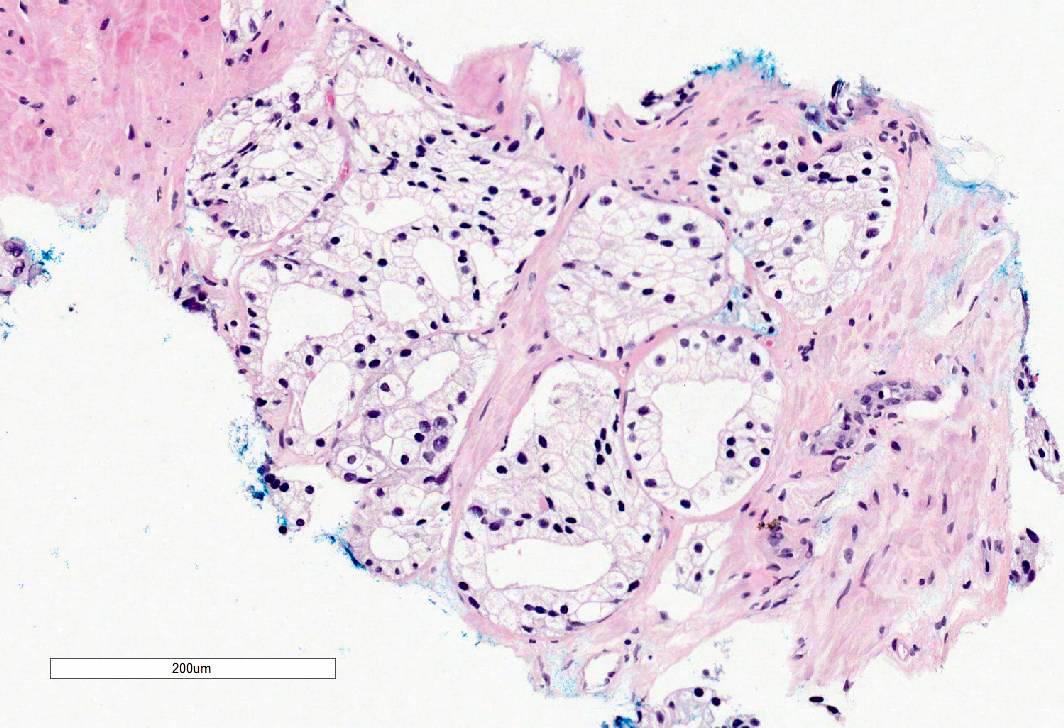
Foamy gland variant of prostate cancer
Crystals in gland lumens
Pink amorphous material within gland lumens
Amphophilic cytoplasm
Mitosis
Collagenous micronodules
Virtual slides
Images hosted on other servers:

Prostate adenocarcinoma Gleason 4+3=7

Prostate adenocarcinoma Gleason 4+4=8

Prostate ductal adenocarcinoma
Cytology description
- Urine cytology for detecting prostate cancer has a very low sensitivity (Prostate Cancer Prostatic Dis 2019;22:362)
- Urine cytology is not used clinically in the diagnosis of prostate cancer
- FNA of metastatic prostate cancer to a lymph node may show microacinar complexes / cell clusters / single cells with fragile cytoplasm and prominent nucleoli (Diagn Cytopathol 2007;35:565)
Positive stains
- PSA
- NKX3.1
- AMACR (P504S, racemase)
- Prostein (P501S)
- PSMA
- Rare tumors may have aberrant expression of p63 (Mod Pathol 2015;28:446)
- Reference: Am J Surg Pathol 2014;38:e6
Negative stains
- CK7
- CK20
- High molecular weight cytokeratins (34 beta E12, CK5, CK5/6)
- p63
- CDX2
- GATA3
- TTF1
- Reference: Am J Surg Pathol 2014;38:e6
Molecular / cytogenetics description
- Prostate cancer is a heritable disease
- Family history of a first degree relative with prostate cancer increases the risk of developing prostate cancer by 2 fold (Nat Rev Urol 2014;11:18)
- 30 - 40% of familial risk is due to genetic factors (Adv Anat Pathol 2020;27:11)
- Genetic factors include highly penetrable rare variants and more common low to moderate risk variants (Adv Anat Pathol 2020;27:11)
- Highly penetrant variants occur in BRCA2 and HOXB13
- Over 280 SNPs have been identified as prostate cancer risk factors (Adv Anat Pathol 2020;27:11)
- For most SNPs, the molecular mechanism of cancer association is generally unknown, as they occur in noncoding regions of the genome (Adv Anat Pathol 2020;27:11)
- Somatic mutations occur in genes such as ERG, ETV1/4, FLI1, SPOP, FOXA1, IDH1, PTEN, TP53, MYC, CDH1 (Cell 2015;163:1011, Adv Anat Pathol 2020;27:11)
- Most common somatic genomic rearrangement is fusion of the androgen regulated gene TMPRSS2 with a member of the ETS transcription family (Adv Anat Pathol 2020;27:11)
- Somatic mutation profiles of prostate cancer are associated with clinical and pathological outcomes
- There are 7 major subtypes, which are defined by either specific gene fusions of ETS transcription family members (ERG, ETV1, ETV4 and FLI1) or mutations (SPOP, FOXA1, IDH1) (Oncotarget 2018;9:14723)
- Different subtypes have different molecular profiles, for example (Oncotarget 2018;9:14723):
- ETS subset (59% of cases) are enriched in PTEN mutations
- SPOP mutant subset (11%) of cases have distinct somatic copy number alteration profiles, including deletions of CHD1, 6q and 2q
Sample pathology report
- Prostate core biopsies:
- Acinar adenocarcinoma (see comment)
- Comment:
- Number of cores involved:
- Right 1/6 cores
- Location(s): right apex
- Left 0/6 cores
- Total number of cores involved: 1/12
- Greatest length of cancer in a core: 5 mm (40%)
- No evidence of perineural invasion or extraprostatic extension
- Gleason score: 3+4=7 (10% pattern 4, no cribriform morphology)
- Grade group 2
- Number of cores involved:
- Radical prostatectomy:
- Histological tumor type: acinar adenocarcinoma
- Gleason score:
- Primary Gleason grade: 3
- Secondary Gleason grade: 3
- Tertiary Gleason grade (< 5%): not applicable
- Gleason score: 3+3=6
- Grade group: 1
- Location of dominant tumor: right apex
- Extraprostatic extension: not identified
- Bladder neck: not involved
- Seminal vessels: not involved
- Margin status: not involved
- Lymphovascular invasion: not identified
- Regional lymph node status:
- Number of nodes examined: 9
- Number of positive lymph nodes: 0
- Primary tumor: pT2 pN0
Differential diagnosis
- Benign prostate tissue:
- Pale cytoplasm
- Corpora amylacea
- No other intraluminal contents
- Basal cell marker immunoreactivity
- Prostatic atrophy:
- Lobular architecture
- Scant cytoplasm
- Basal cell marker immunoreactivity
- Adenosis:
- Lobular architecture
- Basal cell marker immunoreactivity (often scattered)
- Atypical small acinar proliferation (ASAP):
- Small size
- Lack of significant cytological atypia, including a lack of macronucleoli
- High grade prostatic intraepithelial neoplasia (HGPIN):
- Less architectural atypia
- Maintained basal cells
- Postatrophic hyperplasia:
- Some glands atrophic
- Basal cell marker immunoreactivity (often scattered)
- Partial atrophy:
- Atrophic glands with abundant lateral pale cytoplasm
- Irregularly distributed nuclei
- Basal cell marker immunoreactivity (often scattered)
- Radiation atypia:
- Glandular atrophy
- Nuclear irregularity and pleomorphism
- Atypical stromal cells
- Basal cell marker immunoreactivity
- Urothelial carcinoma:
Board review style question #1
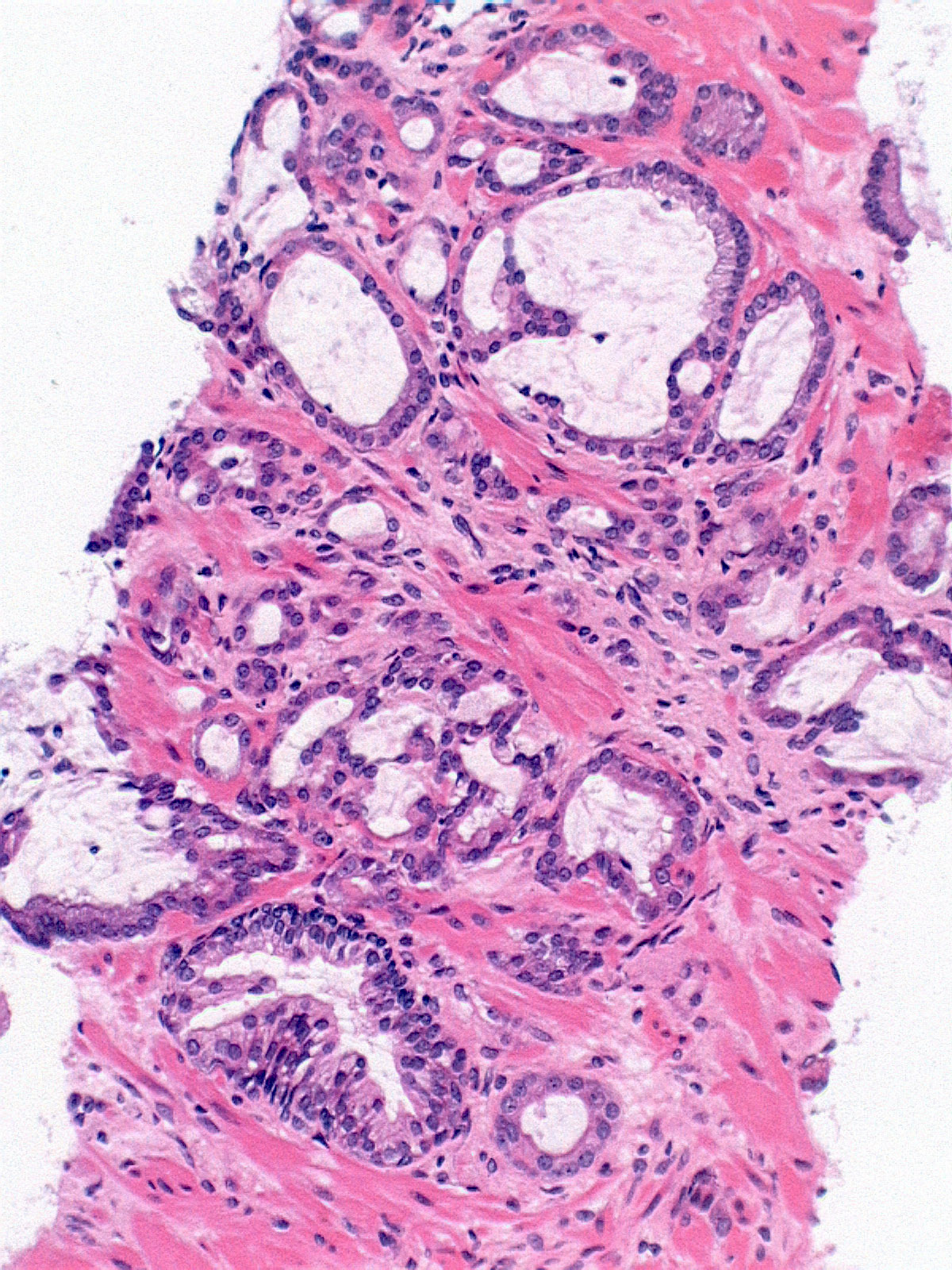
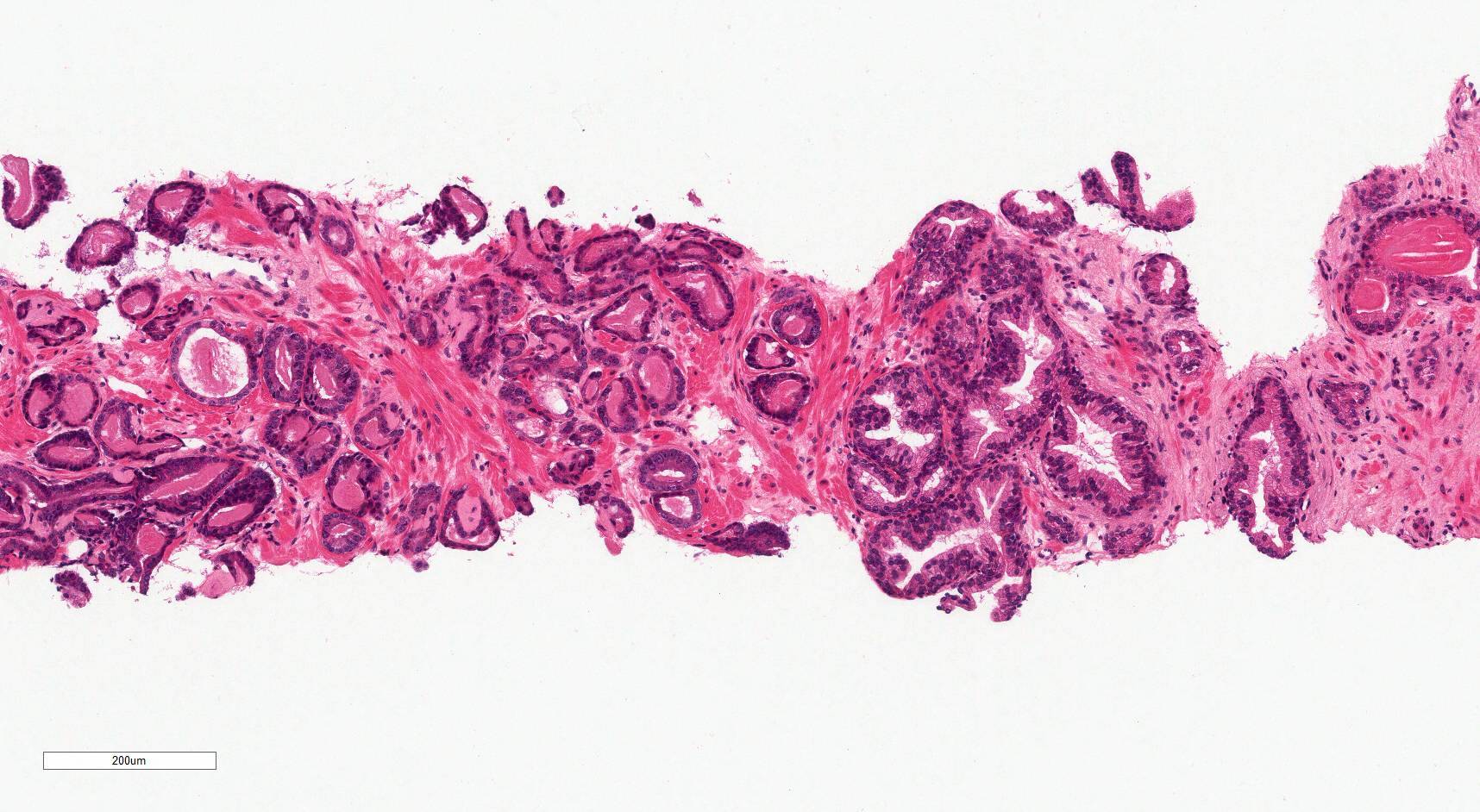
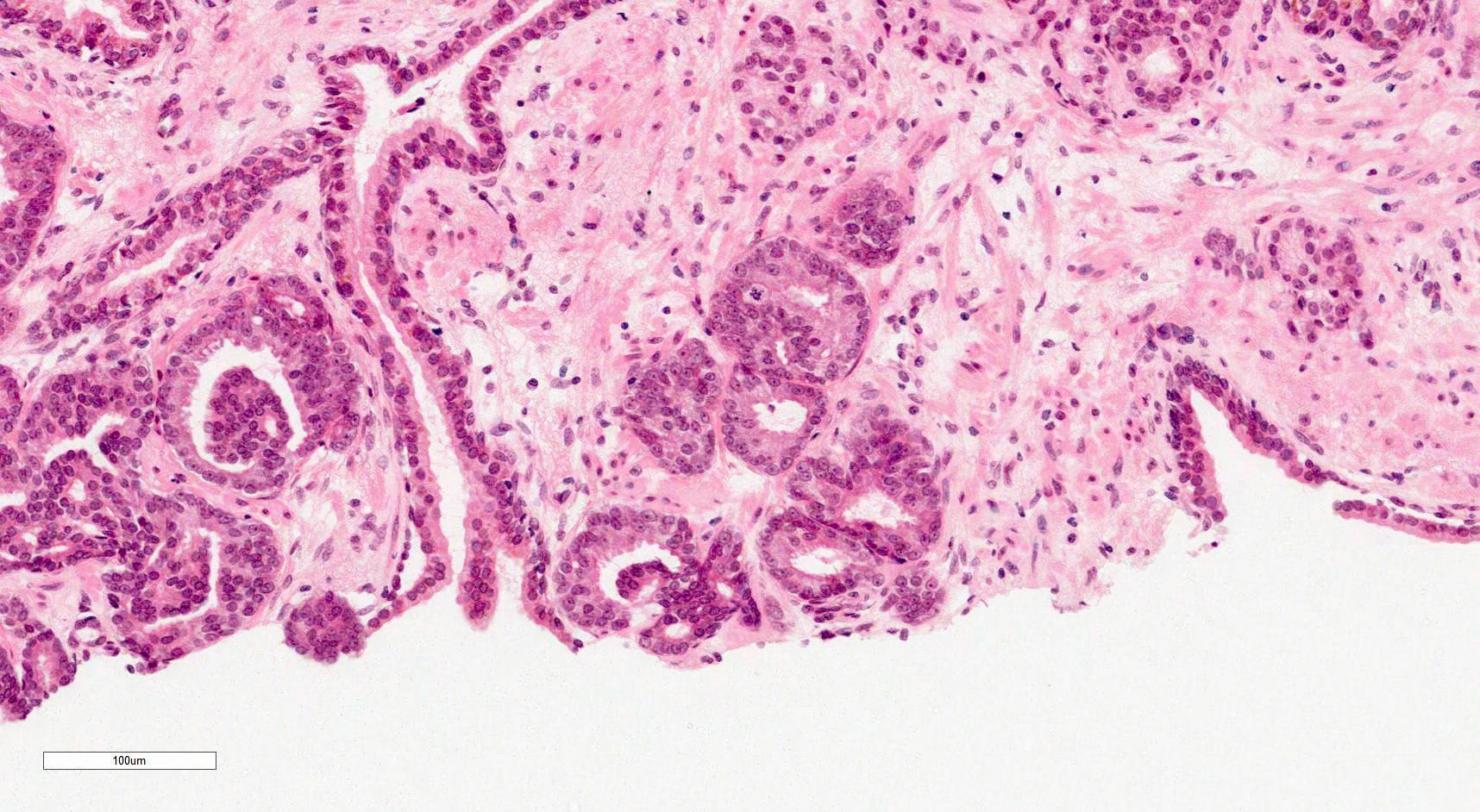
A 74 year old man with urinary hesitancy was found to have a PSA of 8 ng/mL. He had a transrectal ultrasound (TRUS) and prostate biopsy. A representative image is above. Which of the following is the typical immunoprofile of such a tumor?
- CK7- CK20- NKX3.1-
- CK7- CK20- NKX3.1+
- CK7- CK20+ NKX3.1-
- CK7+ CK20- NKX3.1-
- CK7+ CK20+ NKX3.1+
Board review style answer #1
Board review style question #2
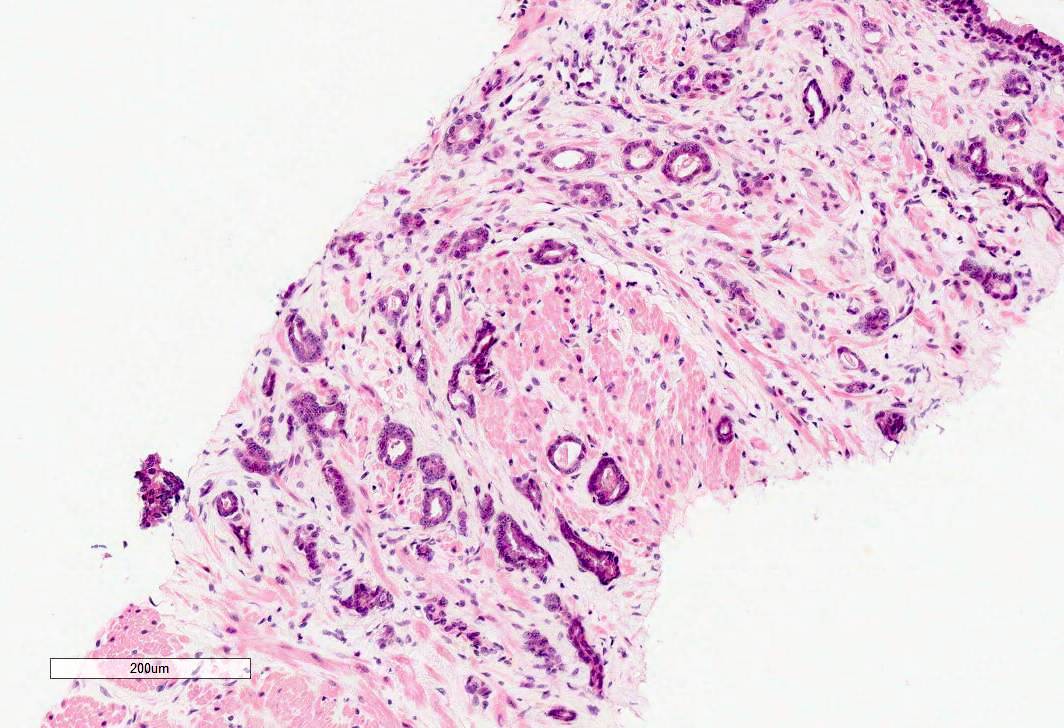
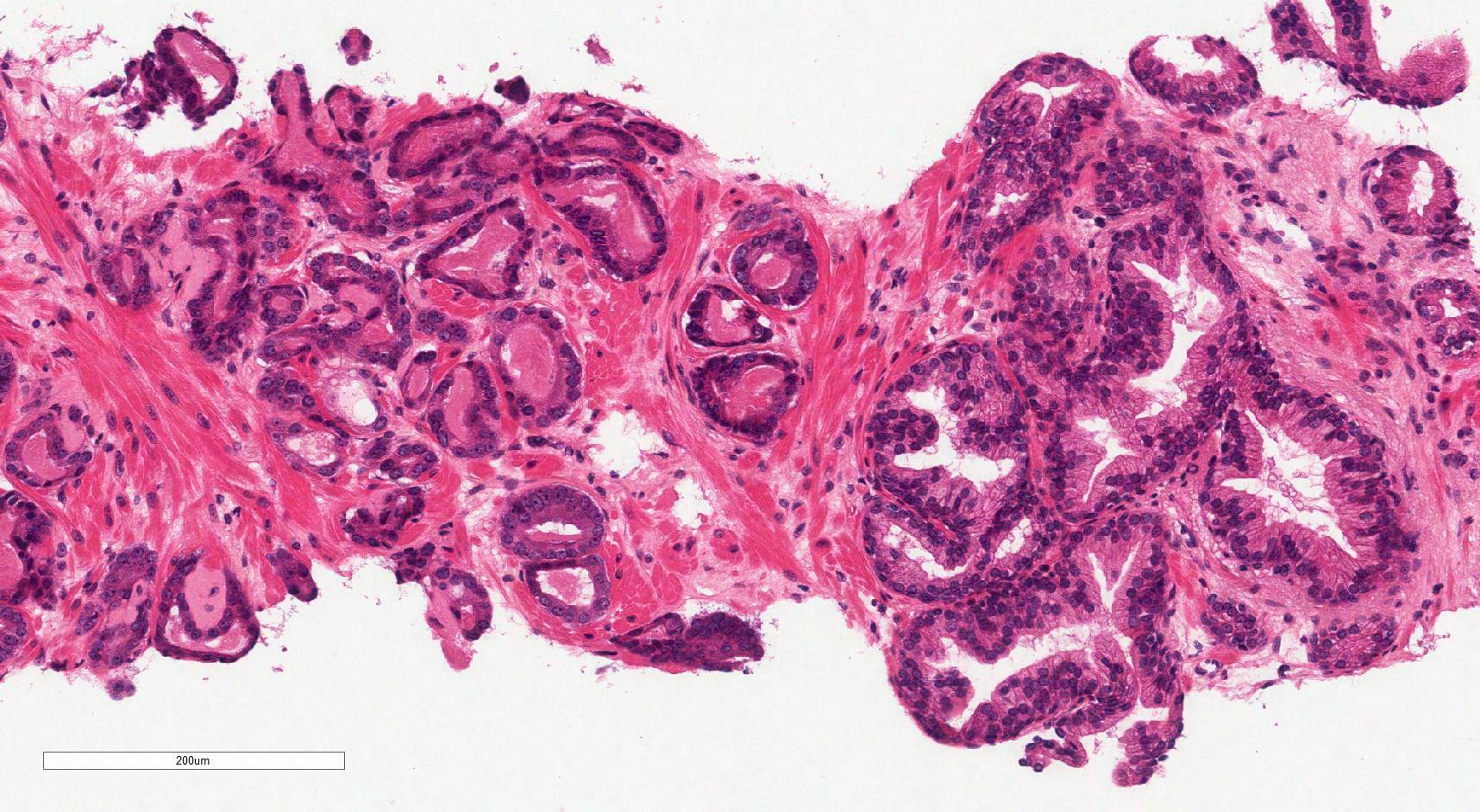
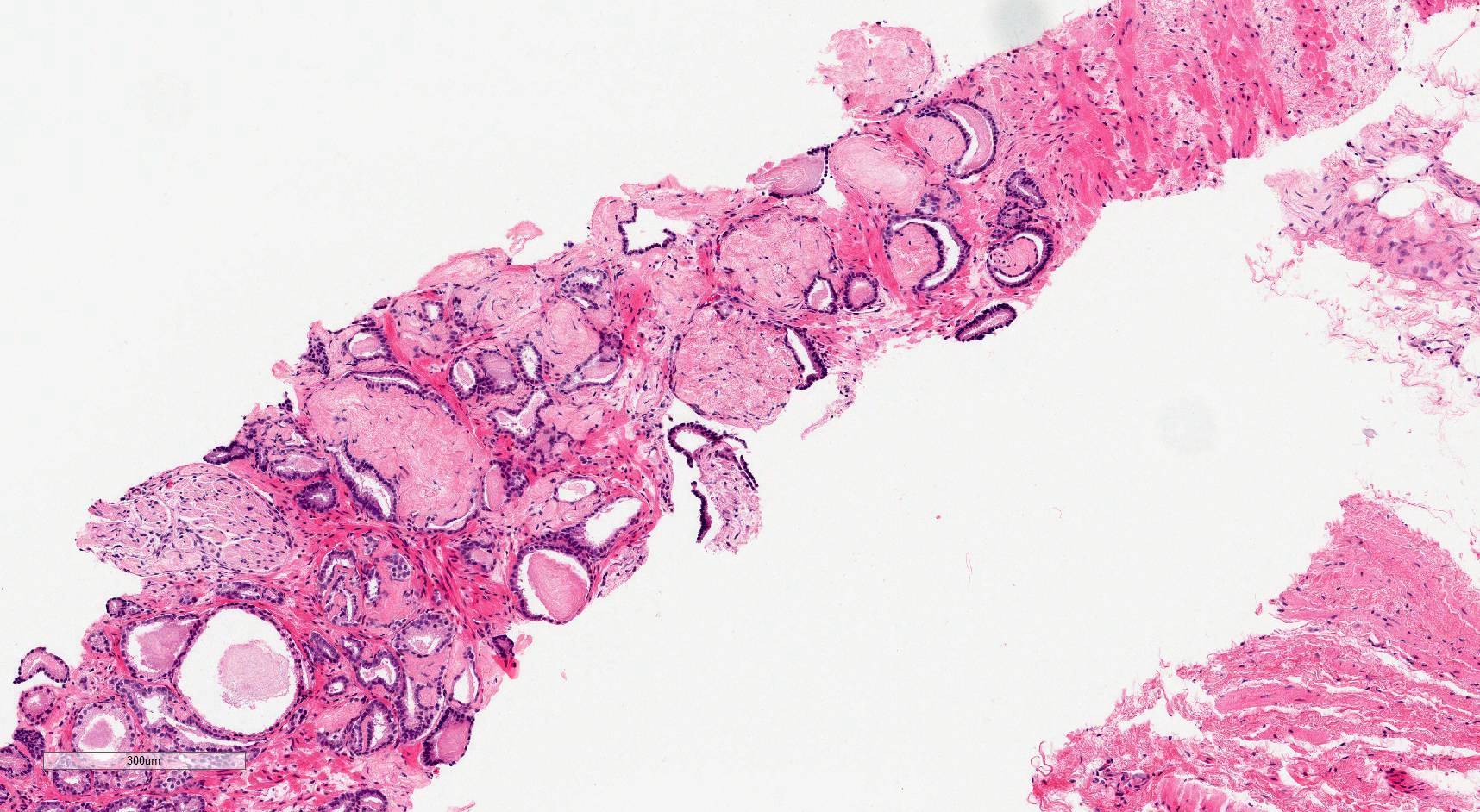
A prostate biopsy shows this tumor. What is its grade?
- Gleason score 2+3, grade group 1
- Gleason score 3+2, grade group 1
- Gleason score 3+3, grade group 1
- Gleason score 3+3, grade group 2
- Gleason score 3+4, grade group 2
Board review style answer #2
