Gallbladder & extrahepatic bile ducts
Gallbladder benign
Pyloric gland adenoma
Author: Xiaoyan Liao, M.D., Ph.D.
Editorial Board Members: Kimberley J. Evason, M.D., Ph.D., Claudio Luchini, M.D., Ph.D.

Last author update: 22 August 2023
Last staff update: 22 August 2023
Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: Pyloric gland adenoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Liao X. Pyloric gland adenoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/gallbladderpyloricgland.html. Accessed September 15th, 2025.
Definition / general
- Grossly visible, noninvasive neoplasm of the gallbladder composed of uniform back to back mucinous glands arranged in a tubular configuration
- WHO classification
- Architecture is often complex
- Glands are bland looking pyloric type or Brunner gland-like
- There is minimal cytological atypia in most of the lesions
- By definition, the cytologic atypia is sufficient for low grade dysplasia
- Foci of high grade dysplasia can be seen in larger lesions
- If lesion is > 1 cm with dysplasia present, classification as intracholecystic papillary (tubular) neoplasm is recommended by some authors (Am J Surg Pathol 2012;36:1279)
Essential features
- Grossly visible, complex, back to back, uniform mucinous glands of pyloric type or Brunner gland-like
- Usually > 0.5 cm and < 2 cm
- < 0.5 cm should be distinguished from nodular pyloric gland metaplasia, which by definition bears no cytologic atypia or dysplasia
- > 1 cm with dysplasia may be classified as intracholecystic papillary (tubular) neoplasm
Terminology
- Intracholecystic papillary tubular neoplasm, gastric pyloric, simple mucinous type
ICD coding
Epidemiology
- Found in 0.1 - 10% of gallbladders removed for cholelithiasis or chronic cholecystitis (Diagnostics (Basel) 2022;12:341, PLoS One 2020;15:e0237979, Adv Med 2018;2018:7539694)
- Accounts for ~82% of gallbladder adenomas (Hum Pathol 2012;43:1506)
- M = F (Am J Surg Pathol 2018;42:1237)
- Mean age of 62.8 years (Am J Surg Pathol 2018;42:1237)
Sites
- No specific site preference reported
- Can occur in the cystic duct with malignant transformation (BMC Cancer 2012;12:570)
Etiology
- 50 - 65% associated with cholelithiasis (Hum Pathol 2012;43:1506)
- Commonly associated with pyloric gland metaplasia, which is possibly a precursor
Clinical features
- Usually asymptomatic and is an incidental finding
- When arising in the gallbladder neck, can lead to gallbladder distension and right upper quadrant pain
Radiology description
- Abdominal ultrasound is usually performed and shows polyps within the gallbladder (J Gastrointest Oncol 2016;7:S81)
Radiology images
Images hosted on other servers:

Transverse ultrasound

Sagittal ultrasound
Prognostic factors
- If invasive carcinoma is ruled out, pyloric gland adenoma is cured by cholecystectomy, even when high grade dysplasia is present
Case reports
- 37 year old woman with dyspeptic complaints found to have a 2 cm polypoid lesion (Turk J Gastroenterol 2014;25:234)
- 40 and 53 year old men each presented with a 1 cm polyp (J Gastrointest Oncol 2016;7:S81)
- 44 year old man with upper abdominal pain found to have a 2 cm polyp (Gastroenterology 2011;141:e3)
- 62 year old man with a 2 cm tumor with transition into well differentiated adenocarcinoma and high grade biliary intraepithelial neoplasia (BMC Cancer 2012;12:570)
Treatment
- Surgery (cholecystectomy) is indicated for any polypoid lesions ≥ 1 cm
Gross description
- < 2 cm, sessile or pedunculated
- Usually single but can be multiple
Gross images
Images hosted on other servers:

Intraluminal tumor
Microscopic (histologic) description
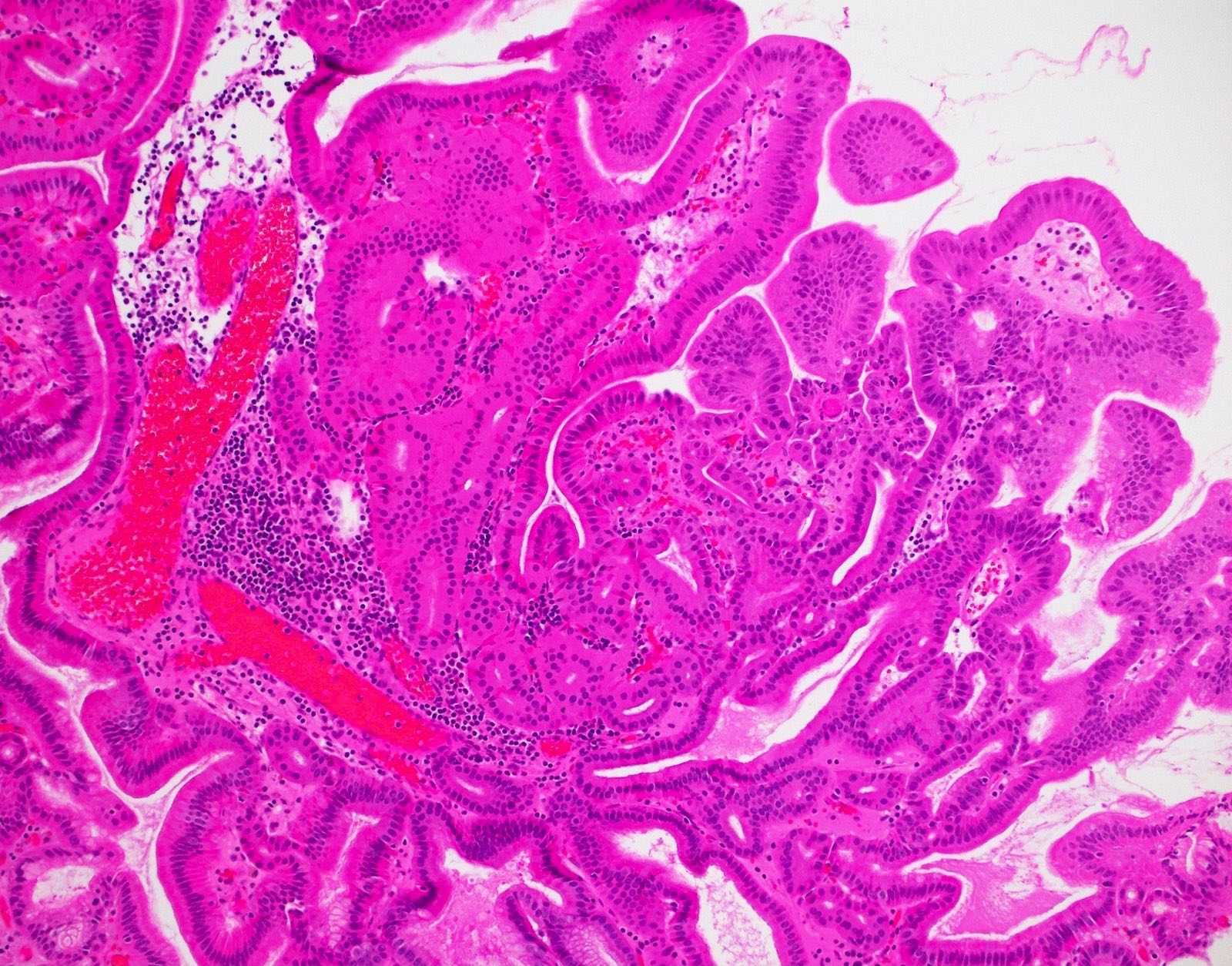
- Tightly packed, bland looking pyloric type or Brunner gland-like glands (Histopathology 2018;72:1007)
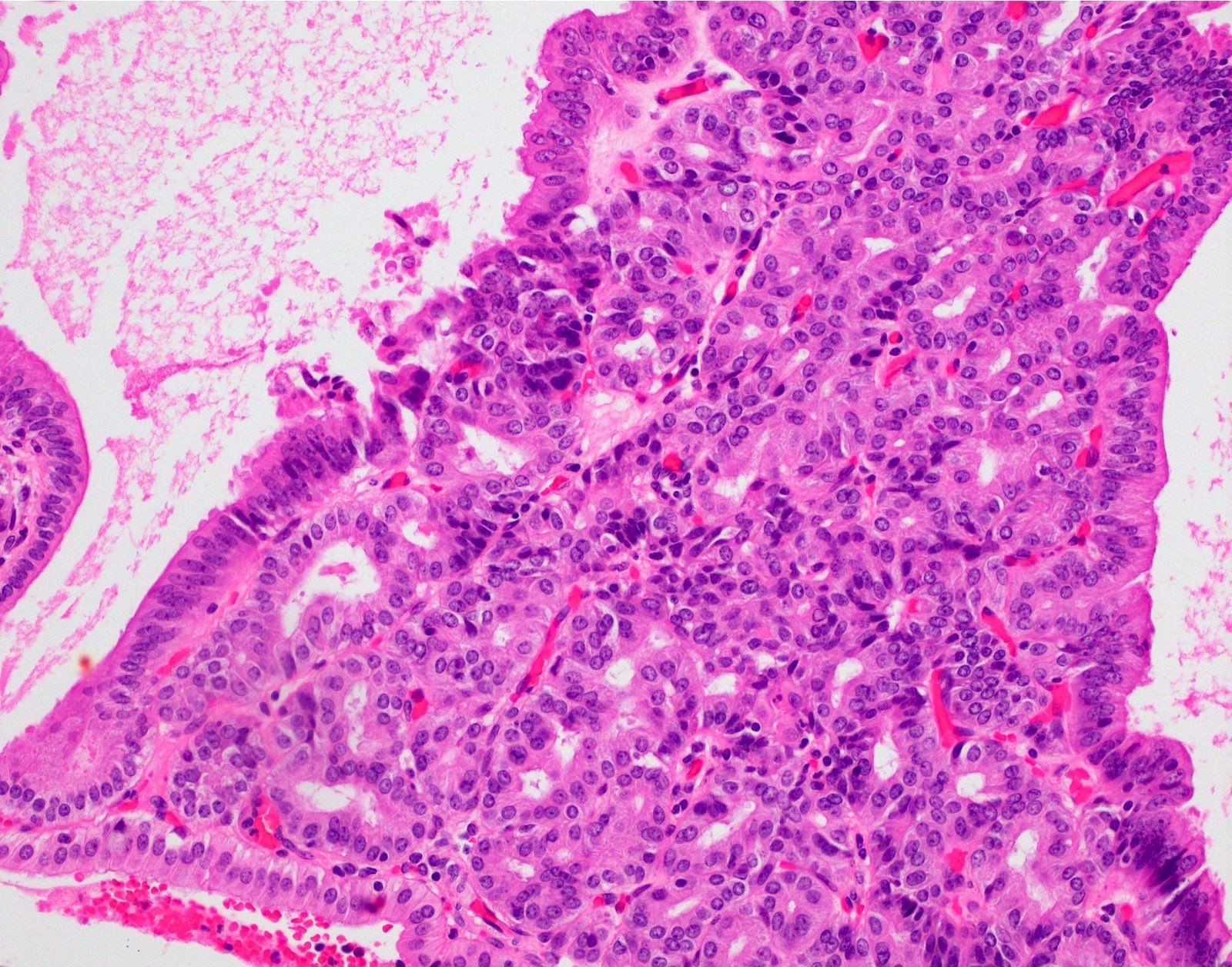
- Lined by cuboidal or columnar mucus secreting cells with apical mucinous cytoplasm
- Round or oval, relatively small, hyperchromatic, basally located nuclei with a small round conspicuous nucleolus
- Slight nuclear overlapping and increased N:C ratios when compared to background normal glands
- High grade dysplasia features more complex architecture, prominent nucleoli and loss of nuclear polarity
- Some glands may be cystically dilated
- There is minimal or no intervening stroma
- Paneth cells and neuroendocrine cells are often present
Microscopic (histologic) images
Contributed by Xiaoyan Liao, M.D.
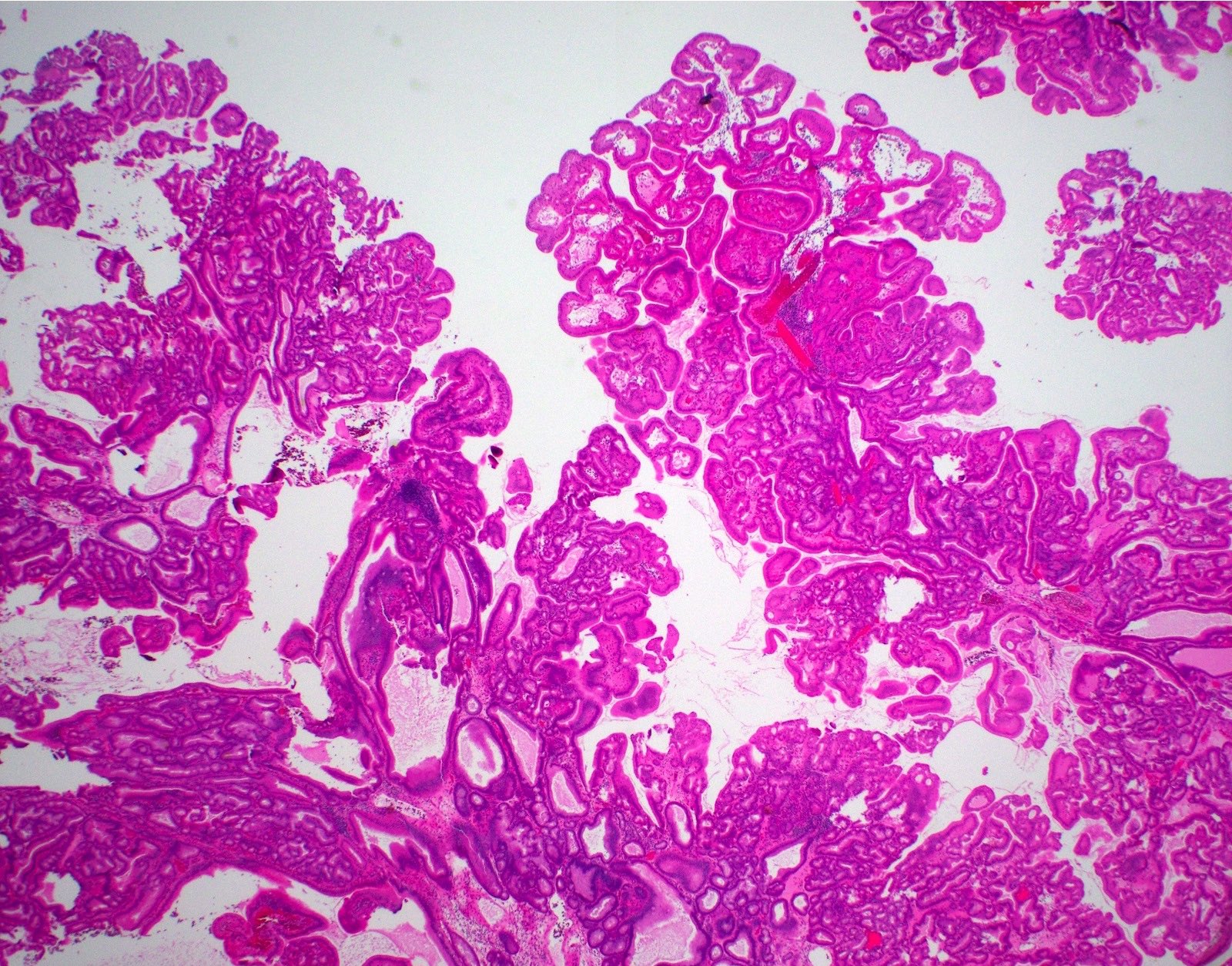
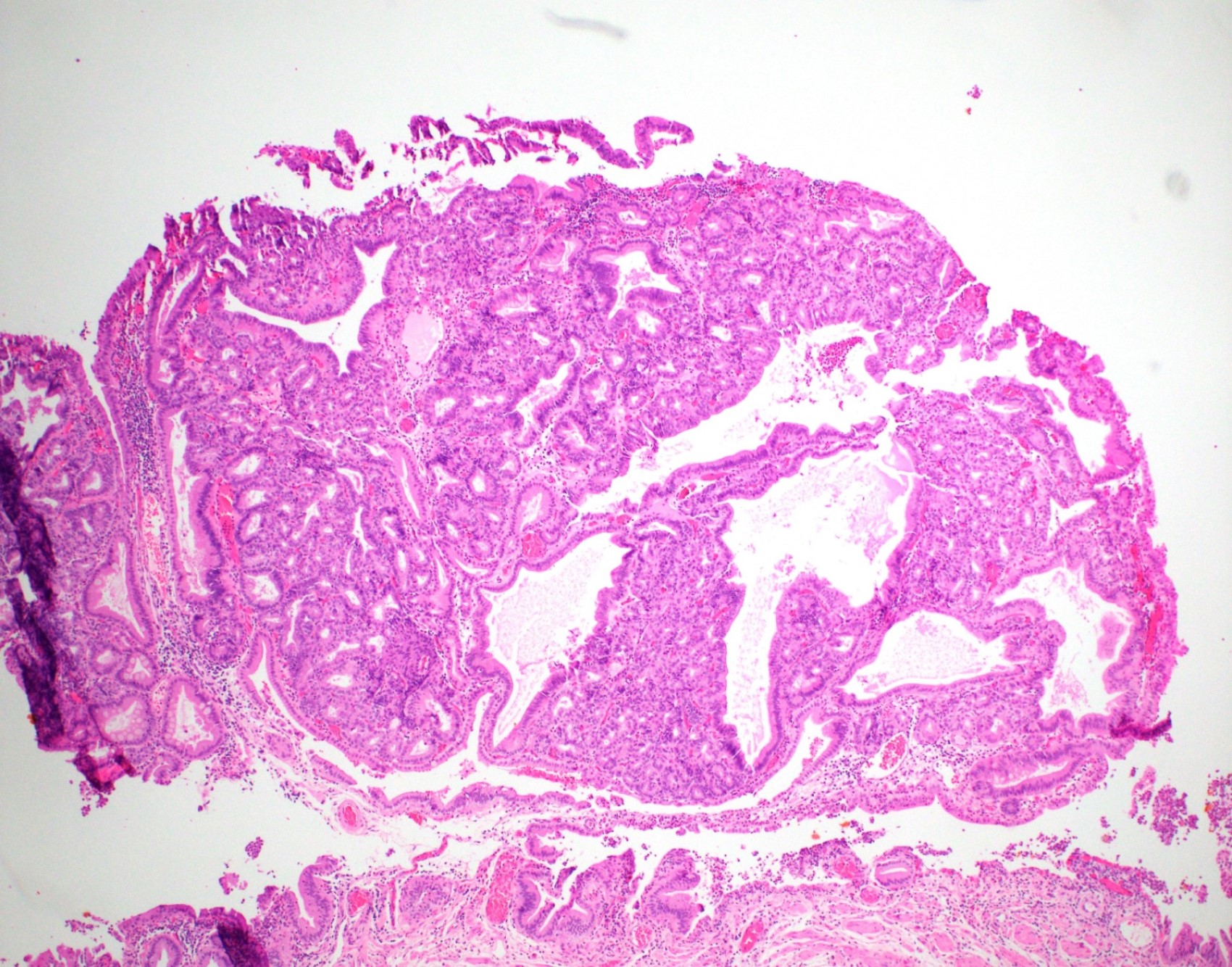
Polypoid lesion
Eosinophilic cytoplasm
Intervening stroma
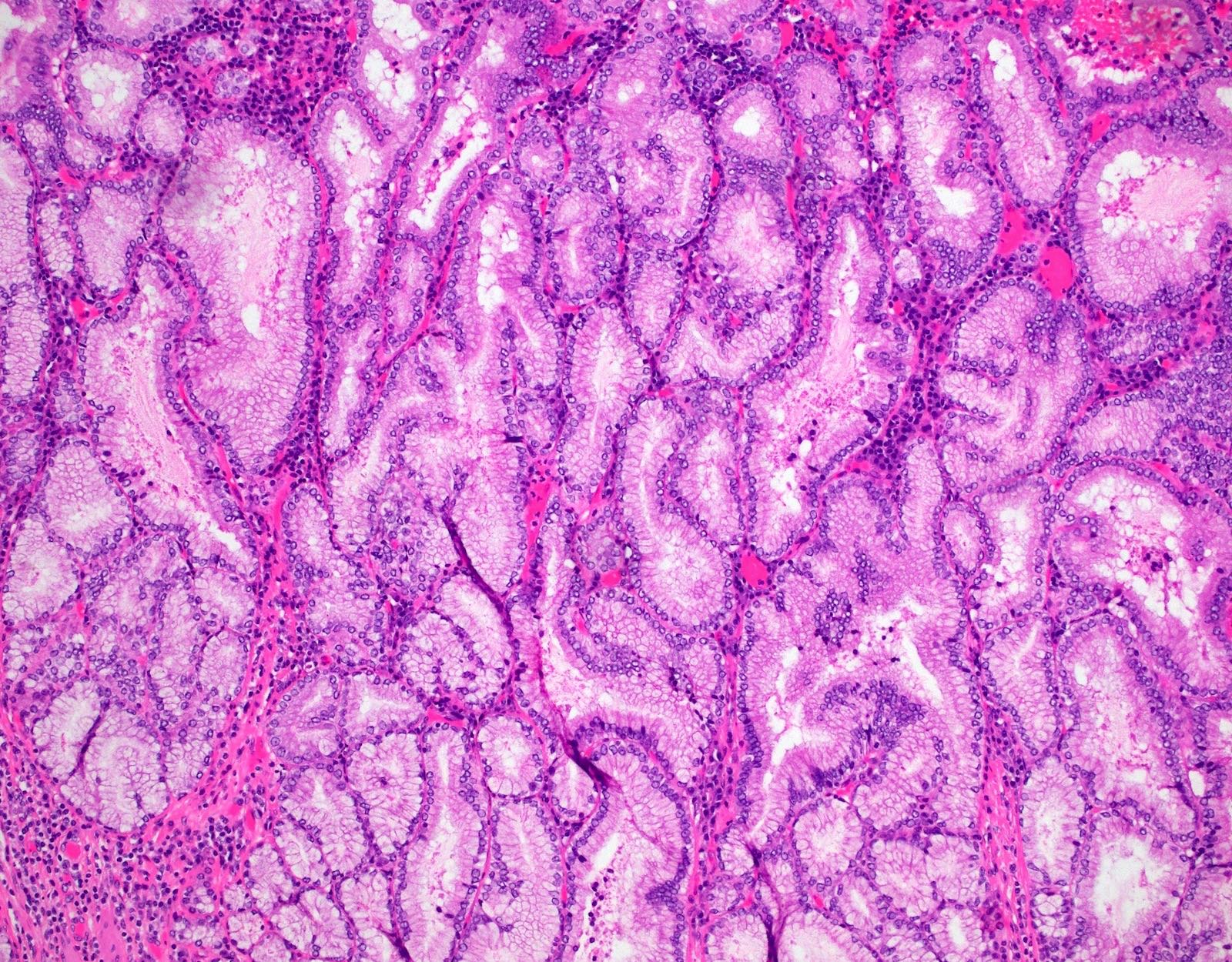
Tightly packed mucinous glands
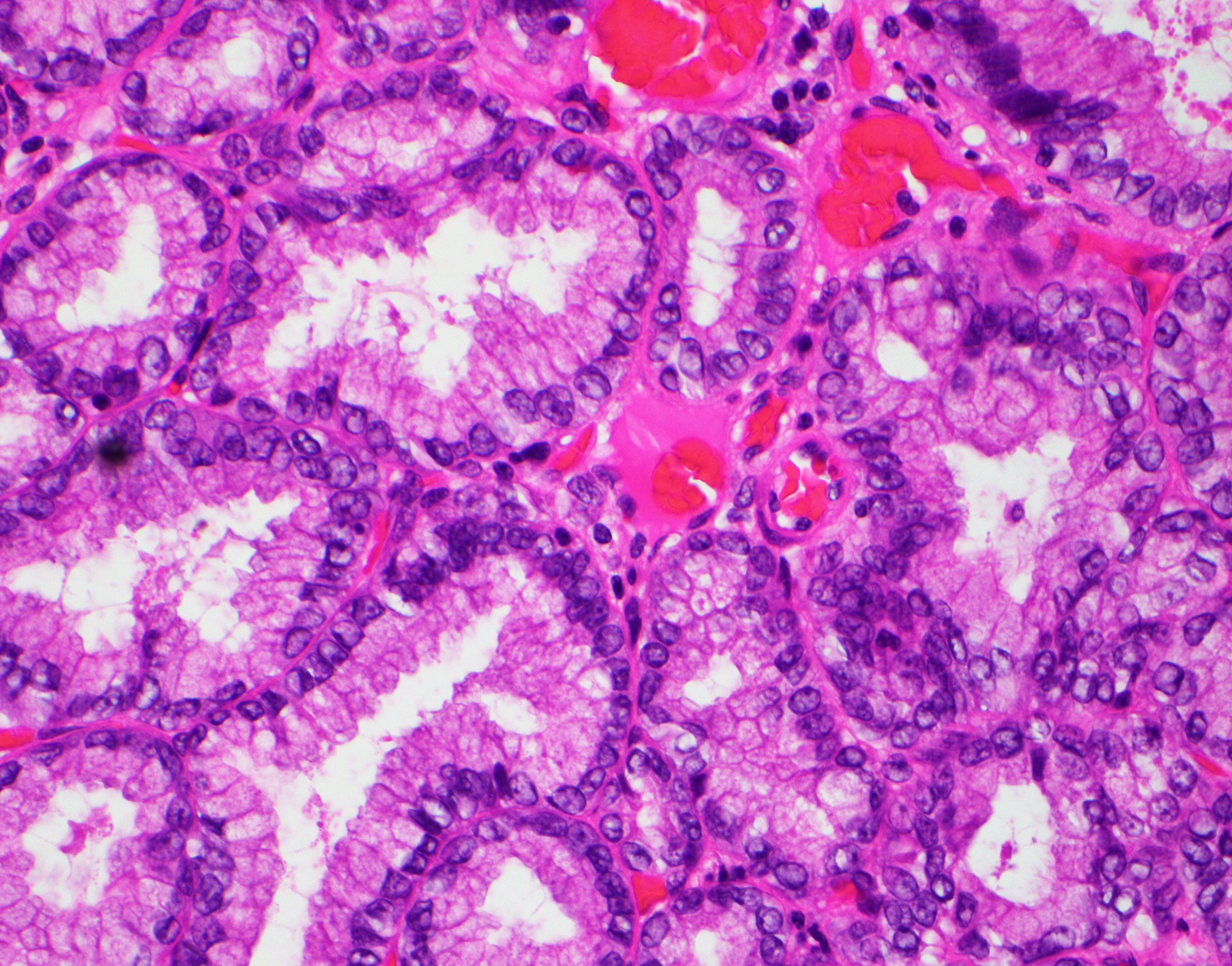
Bland cytologic atypia
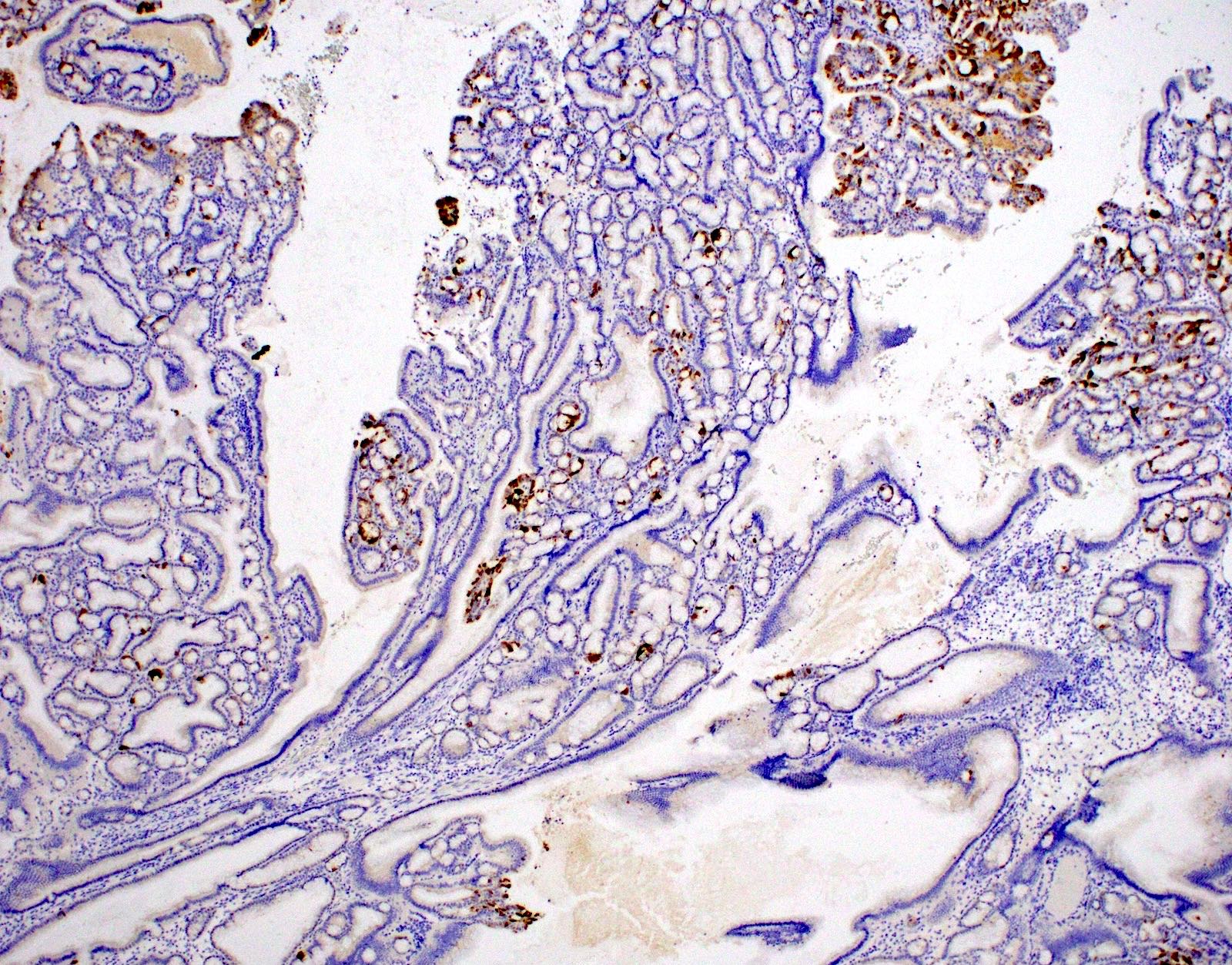
MUC5AC
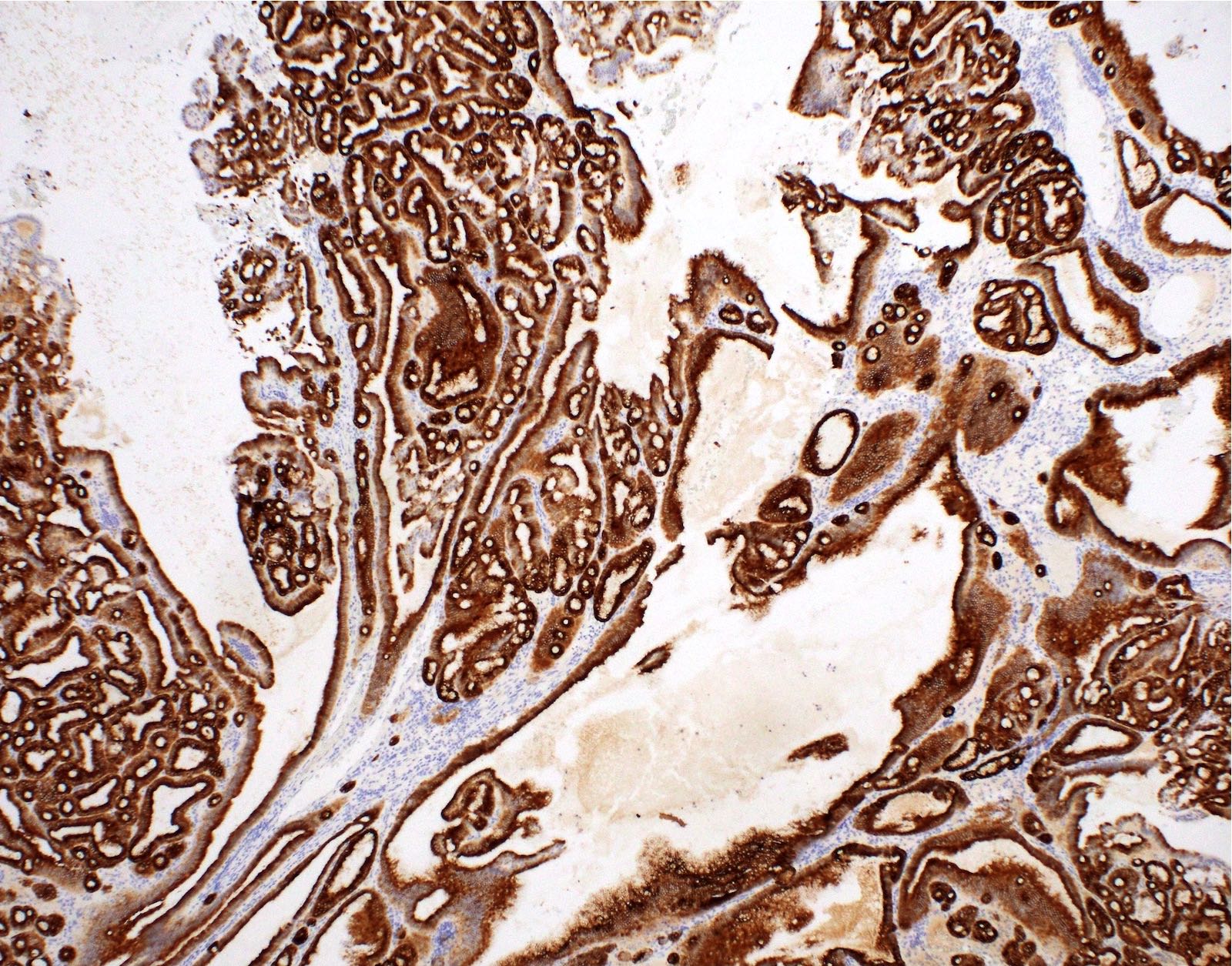
MUC6
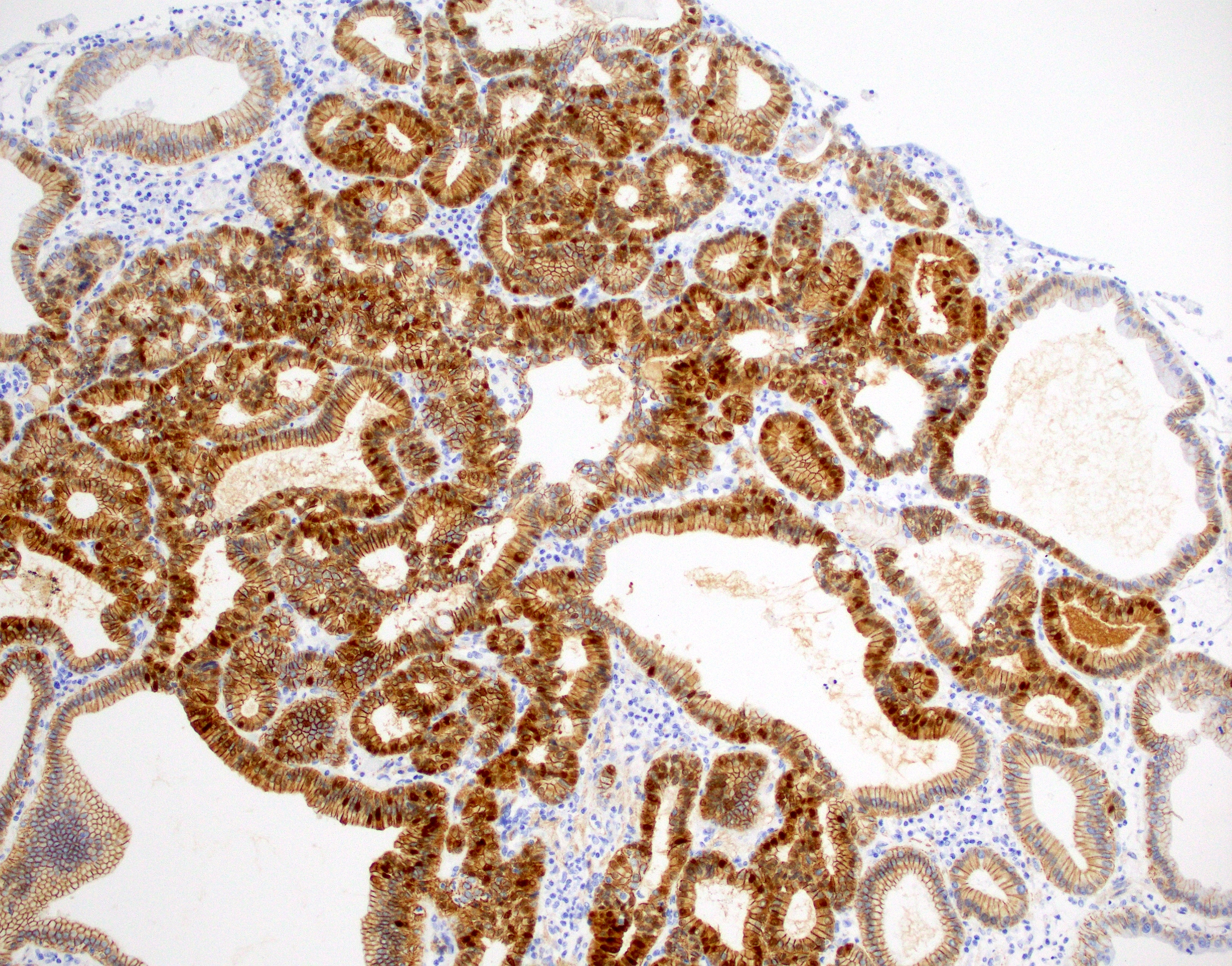
Beta catenin
Positive stains
- CK7 and MUC6 (diffuse and strong)
- Nuclear beta catenin reported (Am J Surg Pathol 2018;42:1237)
Negative stains
- MUC2, MUC5AC and CDX2 usually negative or only focally positive (Am J Surg Pathol 2018;42:1237)
Molecular / cytogenetics description
- CTNNB1 mutations detected in 60% and 100% in 2 separate studies (Hum Pathol 1999;30:21, Am J Surg Pathol 2018;42:1237)
- KRAS mutation reported in a subset (Hum Pathol 1999;30:21, Am J Surg Pathol 2018;42:1237)
- TP53 and GNAS mutations usually not identified
Molecular / cytogenetics images
Images hosted on other servers:

Comparative genomic hybridization
Sample pathology report
- Gallbladder, cholecystectomy:
- Pyloric gland adenoma
- Gallbladder, cholecystectomy:
- Pyloric gland adenoma with focal high grade dysplasia
Differential diagnosis
- Pyloric gland metaplasia:
- Size is the most important criteria; metaplasia is usually < 0.5 cm and does not form a discrete mass
- Intracholecystic papillary (tubular) neoplasm:
- Considered an umbrella term for any neoplastic polyps, adenomas and papillary neoplasms that are ≥ 1 cm
- Can be further divided into several categories by morphology
- Biliary, gastric, intestinal and oncocytic
- Pyloric gland adenoma is currently not included under this umbrella
- However, terms may be interchangeable between intracholecystic papillary (tubular) neoplasm and pyloric gland adenomas that are ≥ 1 cm with invasive carcinoma
Additional references
Practice question #1
A polypoid lesion of the gallbladder is identified by ultrasound and is resected. Based on the photomicrograph above, which of the following statements is true?
- Aberrant expression of CDX2 is a frequent feature
- Frequently shows MUC5AC positivity
- It is a precursor lesion for most of the gallbladder adenocarcinomas
- Occurs predominantly in males
- Usually CK7 positive
Practice answer #1
E. Usually CK7 positive, as this is a pyloric gland adenoma. Answer A is incorrect because they do not often express CDX2. Answer B is incorrect because they frequently show MUC6 positivity. Answer C is incorrect because it is a precursor lesion to some but not most of the gallbladder adenocarcinomas. Answer D is incorrect because they occur predominantly in female patients.
Comment Here
Reference: Pyloric gland adenoma
Comment Here
Reference: Pyloric gland adenoma
Practice question #2
Regarding pyloric gland adenoma of the gallbladder, which of the following is correct?
- Frequently shows p53 aberrant expression
- Lesions > 1 cm can be reclassified as intracholecystic papillary neoplasm
- They are not associated with chronic cholecystitis
- Those are benign lesions and never progress to cancer
Practice answer #2
B. Lesions > 1 cm can be reclassified as intracholecystic papillary neoplasm. If the lesion is > 1 cm with dysplasia present, classification as intracholecystic papillary (tubular) neoplasm is recommended by some authors. Answer C is incorrect because pyloric gland adenoma is often associated with background chronic cholecystitis. Answer A is incorrect because p53 usually shows normal wild type expression in those lesions. Answer D is incorrect because they can progress to cancer.
Comment Here
Reference: Pyloric gland adenoma
Comment Here
Reference: Pyloric gland adenoma
