Liver & intrahepatic bile ducts
Acute and chronic hepatitis
Acute hepatitis-general
Authors: Josef G. Venable, M.D., Annika L. Windon, M.D.
Editorial Board Member: Wei Chen, M.D., Ph.D.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.

Last author update: 18 August 2022
Last staff update: 18 August 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Acute hepatitis
See Also: Hepatitis (acute and chronic)-general
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Venable JG, Windon AL. Acute hepatitis-general. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liveracutehepgeneral.html. Accessed July 24th, 2025.
Definition / general
- Acute hepatitis is largely a clinical term used to describe a sudden elevation in liver enzymes that lasts < 6 months in duration
- Can occur de novo or as a flare of various chronic liver diseases
- Acute liver failure is defined as an abrupt onset of severe liver disease that leads to hepatic encephalopathy and coagulopathy shortly after presentation
Essential features
- Acute hepatitis is a clinical term used to describe a sudden elevation in liver enzymes that lasts < 6 months
- Hepatotropic viruses account for the majority of cases, most commonly hepatitis A and B viruses
- Histologic features are fairly nonspecific displaying lobular disarray and can include lobular inflammation, varying degrees of parenchymal necrosis, bile ductular reaction and bland lobular cholestasis
- Features of chronic injury are not present
- Cases of acute hepatitis can resolve spontaneously with supportive therapy, progress to acute liver failure or develop into chronic liver disease
Terminology
- Acute hepatic injury
- Acute liver injury
Epidemiology
- Hepatotropic viruses
- Hepatitis A (HAV)
- Endemic areas include Central and South America, Africa, the Middle East, Asia and the Western Pacific
- Transmission typically occurs through a fecal - oral route; rarely through blood or solid organ transplants
- 1% of cases progress to acute liver failure (CDC: Statistics & Surveillance Viral Hepatitis Surveillance - United States [Accessed 22 April 2022])
- Hepatitis B (HBV)
- Endemic areas include Asia, Africa, South America and the Caribbean
- Routes of transmission include parenterally or through mucosal exposure
- 2% of acute HBV infections can progress to liver failure; HBV accounts for 7% of acute liver failure cases (CDC: Statistics & Surveillance Viral Hepatitis Surveillance - United States [Accessed 22 April 2022])
- Hepatitis C (HCV)
- Acute liver failure remains unknown in HCV infections and acute infection is usually subclinical
- Transmission routes include bloodborne and through sexual activity
- Hepatitis D (HDV)
- Endemic areas include the Mediterranean, Sub-Saharan Africa, the Middle East and Northern South America
- Transmission occurs via a parenteral or mucosal route
- Requires coinfection or superinfection of HBV
- Hepatitis E (HEV)
- Endemic areas include Central and Southeast Asia, North and West Africa and Mexico
- Transmission occurs through a fecal oral route
- 0.1 - 4% of infections progress to acute liver failure (J Gastroenterol Hepatol 2009;24:1484)
- In pregnant women, 30% of infections progress to acute liver failure (Indian J Gastroenterol 2007;26:6)
- Hepatitis A (HAV)
- Drug induced liver injury
- Direct toxins
- Acetaminophen toxicity is the most common cause of acute liver failure in the developed world and accounts for 40 - 50% of cases in the United States, Canada and Europe
- Other offending drugs include antibiotics, neurologic drugs, NSAIDs, statins, immunomodulatory drugs
- Idiosyncratic drug reactions
- Accounts for 10 - 20% of acute liver failure
- Direct toxins
- Rare causes (account for 1% of cases)
- Autoimmune hepatitis
- Most patients are young to middle aged women; however, pediatric, geriatric and male patients may also be affected
- Acute alcoholic hepatitis
- Prevalence is approximately 20% of patients with alcohol use disorder and is associated with a recent period of heavy drinking
- Wilson disease
- Patients typically present between the ages of 5 and 35 years
- Autoimmune hepatitis
Sites
- Acute liver failure can lead to effects on other body systems, including acute renal failure, gastrointestinal bleeding, respiratory failure, cardiovascular collapse, systemic infection and sepsis
Pathophysiology
- Necrosis of minute groups of hepatocytes occurs initially without disturbing the hepatic architecture, usually resulting in complete recovery when the insult resolves
- In severe disease, large groups of hepatocytes die, which leads to necrosis and collapse of the reticulin framework
- Reference: Zakim: Hepatology - A Textbook of Liver Disease, 2nd Edition, 1990
Etiology
- Viral hepatitis
- Hepatotropic viruses (hepatitis A, B, C, D, E)
- Account for 72% of acute hepatitis (N Engl J Med 1993;329:1862)
- Majority of infections are hepatitis A virus (HAV) and hepatitis B virus (HBV)
- Nonhepatotropic viruses
- Herpes simplex virus (HSV), cytomegalovirus (CMV), Epstein-Barr virus (EBV), adenovirus, hemorrhagic fever associated viruses, varicella zoster virus, yellow fever, dengue
- Other infections
- Tick borne diseases, malaria, visceral leishmaniasis, Q fever, leptospirosis
- Drug induced liver injury
- Direct toxins versus idiosyncratic drug reactions
- Rare causes
- Autoimmune hepatitis, acute alcoholic hepatitis, Budd-Chiari, Wilson disease, ischemic hepatitis
- Hepatotropic viruses (hepatitis A, B, C, D, E)
Clinical features
- Most cases range from asymptomatic or subclinical to self limited symptomatic
- Symptomatic cases may present as fatigue, abdominal pain, nausea and vomiting, muscle aches or jaundice
- Severe cases can lead to acute liver failure and may present as (Saxena: Practical Hepatic Pathology, 2nd Edition, 2017):
- Acute onset hepatic encephalopathy (accumulation of toxic substances, cerebral edema and intracranial hypertension)
- Coagulopathy (decreased production of liver coagulation factors [II, V, VII, IX, X], thrombocytopenia and platelet function defects)
- Acute renal failure (prerenal azotemia, acute tubular necrosis, hepatorenal syndrome, drug induced interstitial nephritis)
- Infections (reticuloendothelial system dysfunctions and decreased opsonization of microorganisms)
Diagnosis
- Clinical diagnosis
- Elevated serum alanine aminotransferase and aspartate aminotransferase (ALT, AST) tests
- Viral hepatitis
- Serum antibody tests (IgG, IgM), PCR tests for viral RNA, enzyme linked immunoassay (ELISA) test
- Drug induced hepatitis
- Exclusion of viral hepatitis
- Clinical history is taken to investigate any temporal relationship of drug administration and the presence of abnormal liver tests
- Biopsies typically not performed unless there is a clinical suspicion of a second independent hepatic insult (i.e., underlying chronic liver disease)
- Reference: N Engl J Med 1993;329:1862
Laboratory
- Clinically defined as elevation in aspartate transaminase (AST) and alanine transaminase (ALT) (at least 2x upper normal reference range) for < 6 months (Saxena: Practical Hepatic Pathology, 2nd Edition, 2017)
- Hepatotropic viruses: increase in AST / ALT > 5 times upper limit of normal and alkaline phosphatase (ALP) < 3 times upper limit of normal
- Acute HAV: anti-HAV IgM present for 4 - 6 months
- Acute HBV: anticore IgM, hepatitis B surface antigen (HBsAg)
- Acute HCV: HCV RNA in serum; anti-HCV antibodies may not appear for 6 weeks to 6 months
- Acute HDV: total anti-HDV (IgG and IgM)
- Acute HEV: anti-HEV antibody
- Nonhepatotropic viruses
- CMV: CMV antigenemia
- EBV: monospot test, IgM against EBV viral capsid antigen or EBV viral levels
- Acetaminophen toxicity
- Very high AST and ALT (100x upper limit of normal)
- Acute alcoholic hepatitis
- Marked elevation in bilirubin; slight elevation in transaminases (< 10x upper limit of normal)
- Autoimmune hepatitis
- Increased total IgG, presence of autoantibodies (antinuclear antibody, anti smooth muscle antibody)
- Wilson disease
- Coombs negative hemolytic anemia
- ALP to total bilirubin ratio is low (< 2)
- Hepatotropic viruses: increase in AST / ALT > 5 times upper limit of normal and alkaline phosphatase (ALP) < 3 times upper limit of normal
Prognostic factors
- Cases of acute hepatitis can resolve spontaneously with supportive therapy, progress to acute liver failure or develop into chronic liver disease
- Advanced fibrosis and percentage of necrosis have prognostic significance
- Advanced fibrosis and > 25% necrosis portend a worse prognosis (World J Gastroenterol 2017;23:4303)
Case reports
- 36 year old woman with drug induced liver injury and superimposed acute Epstein-Barr virus hepatitis (Pathology 2019;51:104)
- 51 year old HIV positive man with syphilitic hepatitis presenting as acute cholestatic hepatitis (Hum Pathol 2018;79:184)
- 59 year old woman with cirrhotic primary biliary cholangitis, submassive necrosis and hepatitis E virus (Intern Med 2021;60:1863)
Treatment
- Acute viral hepatitis
- Supportive therapy
- Antiviral therapy for cases of acute hepatitis B
- Drug induced acute hepatitis
- Remove offending medication
- N-acetylcysteine (NAC) for acetaminophen overdose
- Severe acute alcoholic hepatitis
- Supportive therapy combined with or without corticosteroids
- Acute autoimmune hepatitis
- Supportive therapy combined with corticosteroids
- References: Clin Liver Dis 2007;11:525, World J Gastroenterol 2021;27:1691, Lancet Gastroenterol Hepatol 2020;5:494, J Immunol Res 2019;2019:9437043
Gross description
- Description of the excised specimen
- Homogenously enlarged and congested, stretching Glisson capsule
- Cut surface is usually reddish brown but can be green-brown in cholestatic cases
- Reference: Saxena: Practical Hepatic Pathology, 2nd Edition, 2017
Gross images
Contributed by Josef G. Venable, M.D. and Annika L. Windon, M.D.


Severe acute hepatitis
Microscopic (histologic) description
- Lobular disarray
- Disruption of the sinusoidal architecture by cell injury and inflammation
- Lobular inflammation (Saxena: Practical Hepatic Pathology, 2nd Edition, 2017)
- Composed of mainly small T lymphocytes with variable number of macrophages, plasma cells and occasional eosinophils
- Plasma cells may be predominant in acute hepatitis A and B
- Predominantly sinusoidal inflammation with little hepatocyte damage, is characteristic of EBV infection
- Neutrophilic microabscesses or small sinusoidal clusters of neutrophils can sometimes be seen in CMV infection
- Zone 3 accentuation may be seen in some drug induced liver injury
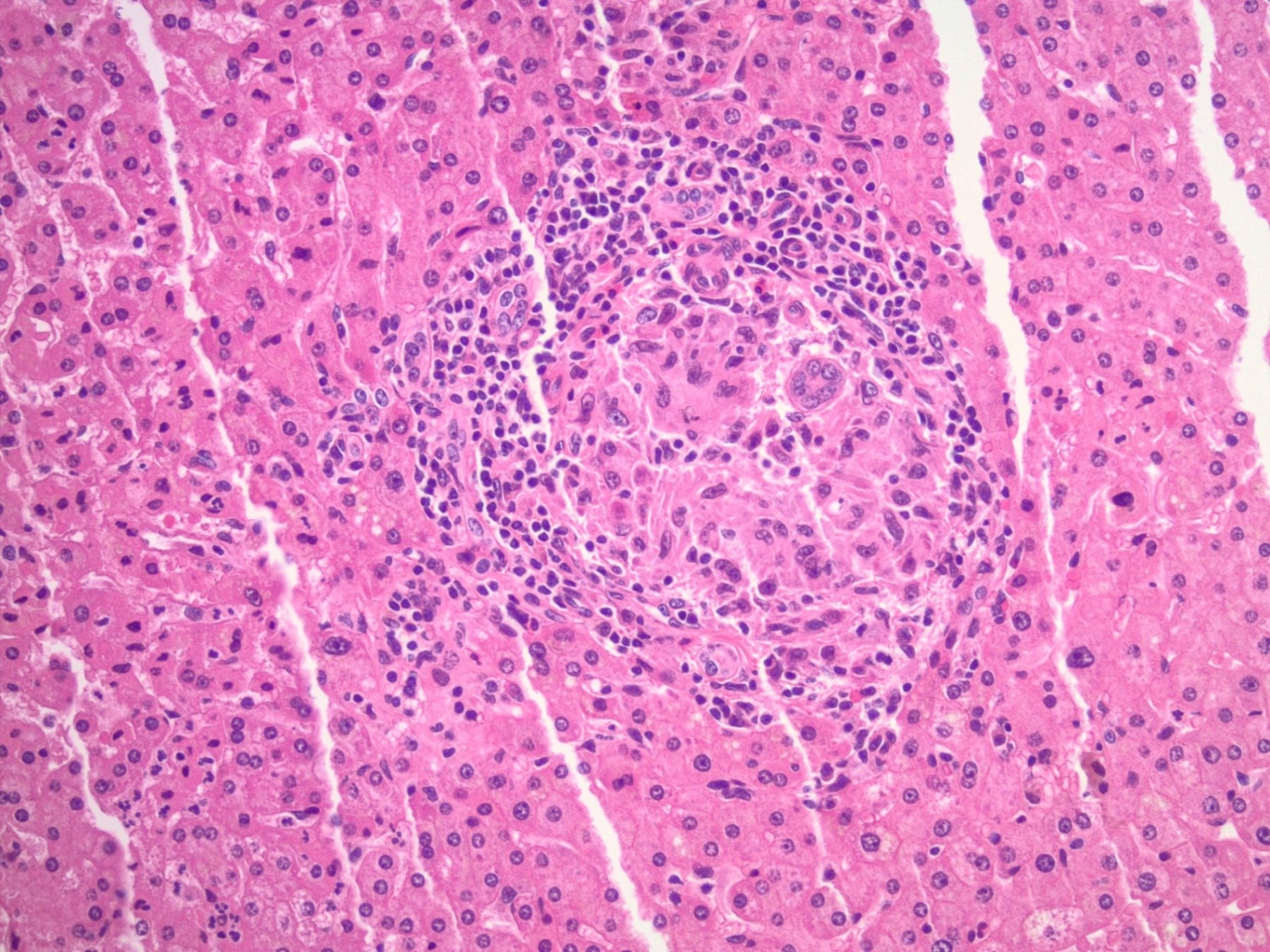
- Granulomas
- Typically seen in infection (tick borne diseases) and drug reactions
- Kupffer cell hyperplasia may be present in more severe cases
- Tick borne diseases, malaria, autoimmune hepatitis
- Resolving cases of acute hepatitis
- Portal tracts have less pronounced inflammation but may be edematous or contain variable amounts of a mononuclear cell infiltrate
- Inflammation from portal tract may spill over, limiting plate mimicking interface activity but hepatocytes are not damaged
- Composed of mainly small T lymphocytes with variable number of macrophages, plasma cells and occasional eosinophils
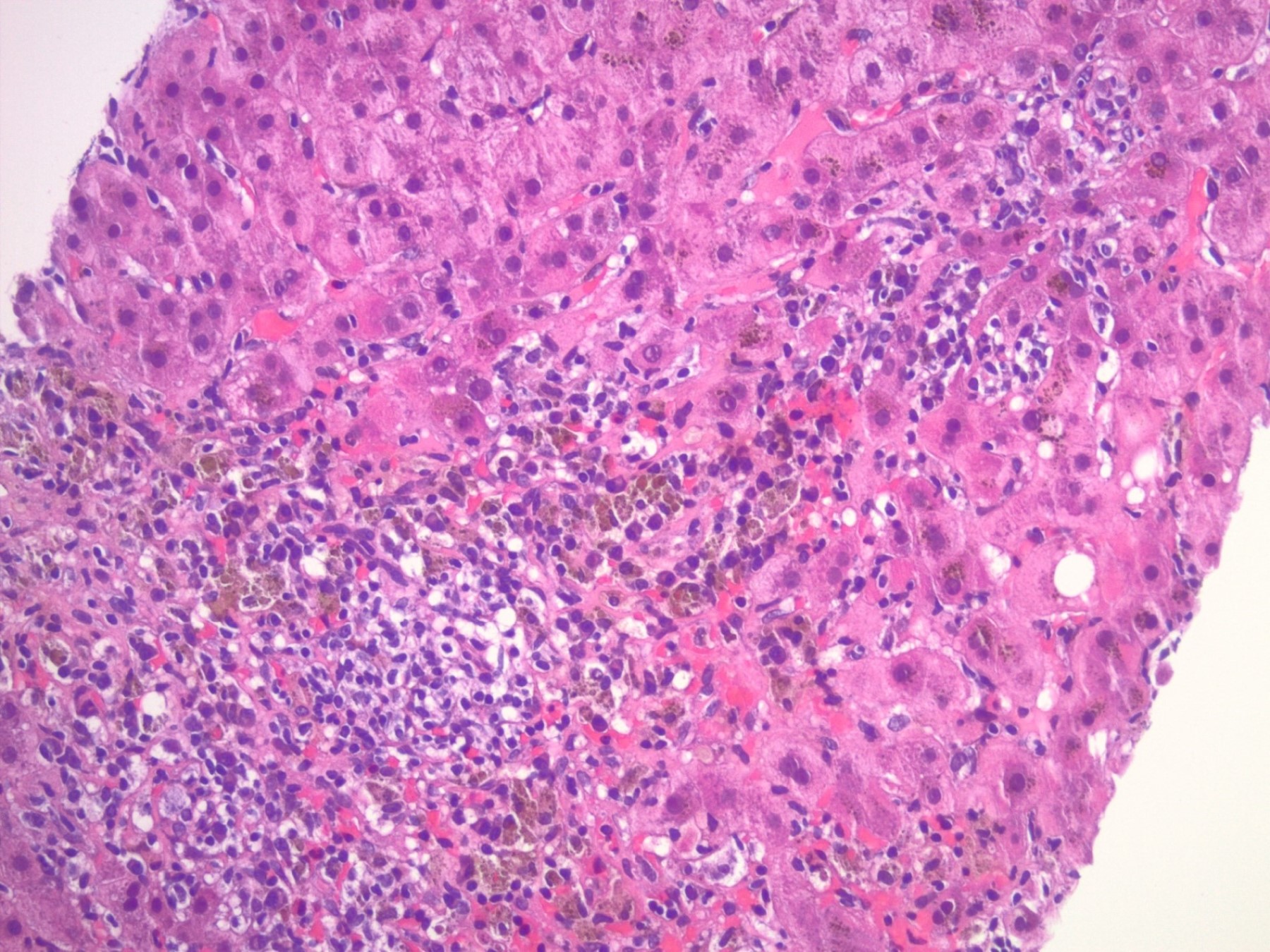
- Necroinflammation is diffuse but can be heterogenous (Saxena: Practical Hepatic Pathology, 2nd Edition, 2017)
- Lytic or spotty necrosis: foci of inflammation surrounding damaged hepatocytes or minute groups of hepatocytes (Gut 2005;54:1162)
- Confluent necrosis: zonal death of larger groups of hepatocytes, leading to collapse of reticulin framework, typically starts in zone 3 (Gut 2005;54:1162)
- Zone 1 or zone 1 - 2 necrosis can rarely be seen in acute hepatitis A infection
- Punched out necrosis can be seen in nonhepatotropic viral infections (adenovirus, HSV) and can have an azonal pattern
- Central hyaline necrosis can be seen in acute alcoholic liver disease and shows central confluent necrosis with obliteration of the central vein and accompanying neutrophilic inflammation
- Bridging necrosis
- Severe acute hepatitis is characterized by confluent necrosis, linking terminal / central venules to portal tracts
- May mimic septa of chronic liver disease
- Panlobular, panacinar, multilobular, multiacinar, submassive (26 - 75% parenchymal volume), massive necrosis (> 75% parenchymal volume)
- Parenchyma replaced by collapsed stromal inflammatory cells and activated macrophages
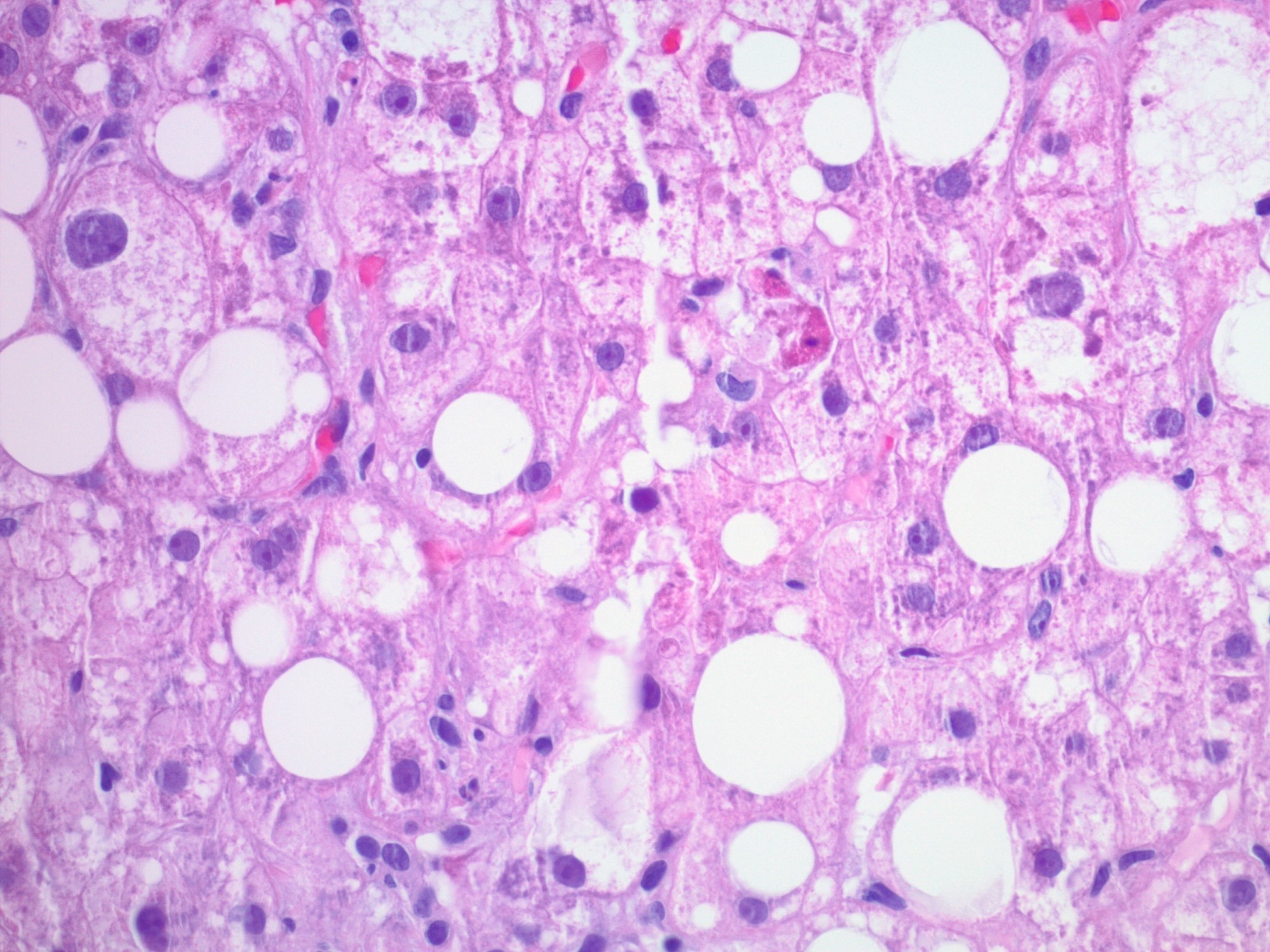
- Hepatocellular damage (Saxena: Practical Hepatic Pathology, 2nd Edition, 2017)
- Apoptotic bodies are degenerated hepatocytes with increased cytoplasmic staining and pyknotic nuclear remnants (Councilman bodies used for yellow fever)
- Minor hepatocyte swelling characterized as rarified, granular or finely vacuolated cytoplasm
- Ballooning degeneration is a more severe swelling characterized by rarified cytoplasm and occasional Mallory hyaline
- Drug reactions, autoimmune hepatitis, acute alcoholic hepatitis, Wilson disease
- Neutrophilic satellitosis: neutrophils surrounding ballooned hepatocytes with Mallory hyaline and is seen in active cases of alcoholic steatohepatitis
- Cholestasis (Saxena: Practical Hepatic Pathology, 2nd Edition, 2017)
- Bland lobular cholestasis may be in canaliculi or (in more severe cases) within the hepatocytes
- Acute hepatitis A, acute hepatitis B
- Drug reactions
- Bland lobular cholestasis may be in canaliculi or (in more severe cases) within the hepatocytes
- Biliary changes
- Bile duct epithelial stratification, cytoplasmic vacuolization, necrosis, altered nuclear polarity, intraepithelial lymphocytosis
- Bile ductular proliferation, which may mimic an obstruction
- Described in some cases symptomatic cases of acute hepatitis C (Am J Surg Pathol 2007;31:1754)
- Drug reactions, Wilson disease
Microscopic (histologic) images
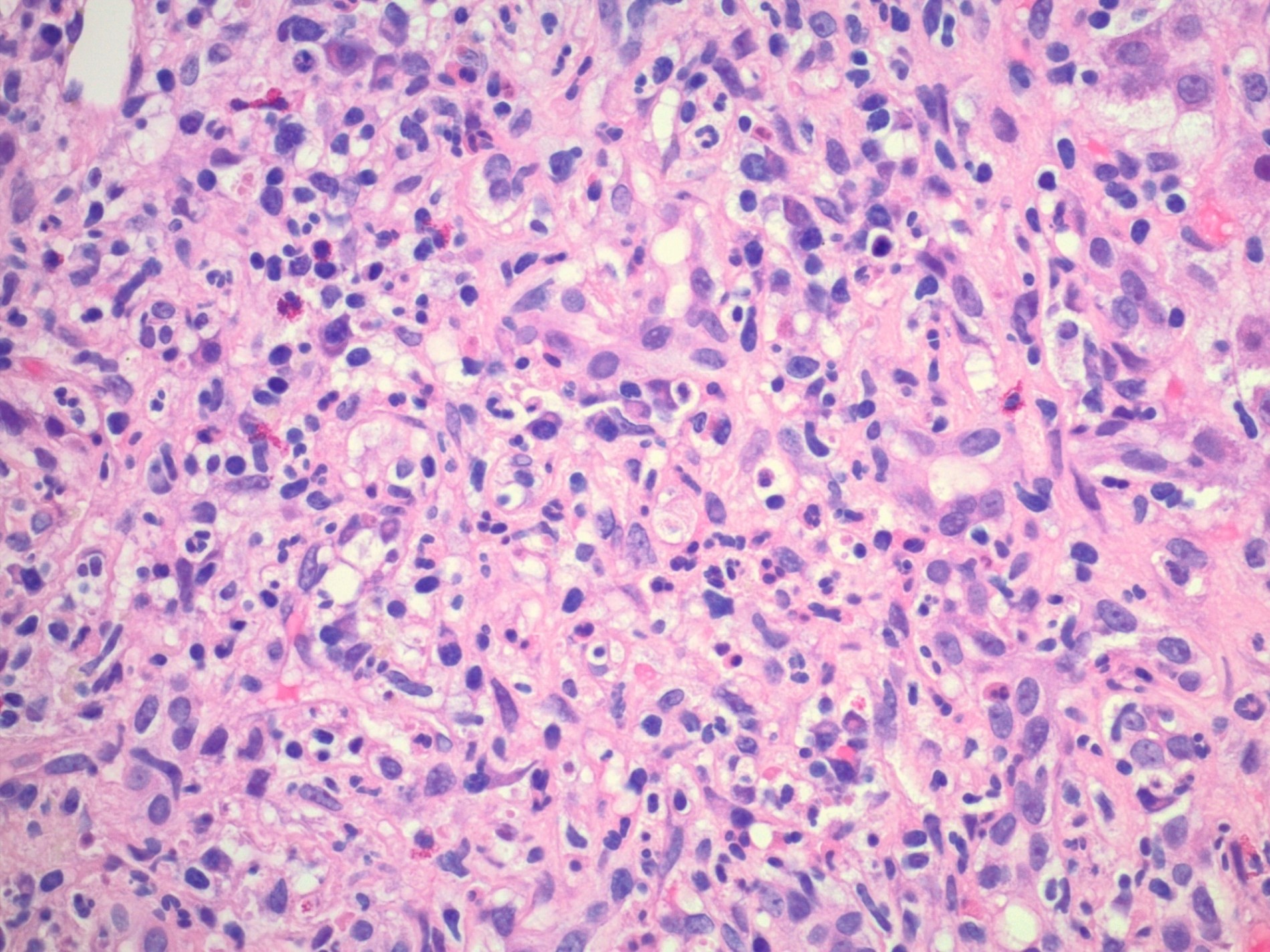
Contributed by Josef G. Venable, M.D. and Annika L. Windon, M.D.
Hepatocyte damage
Granuloma
Interface activity
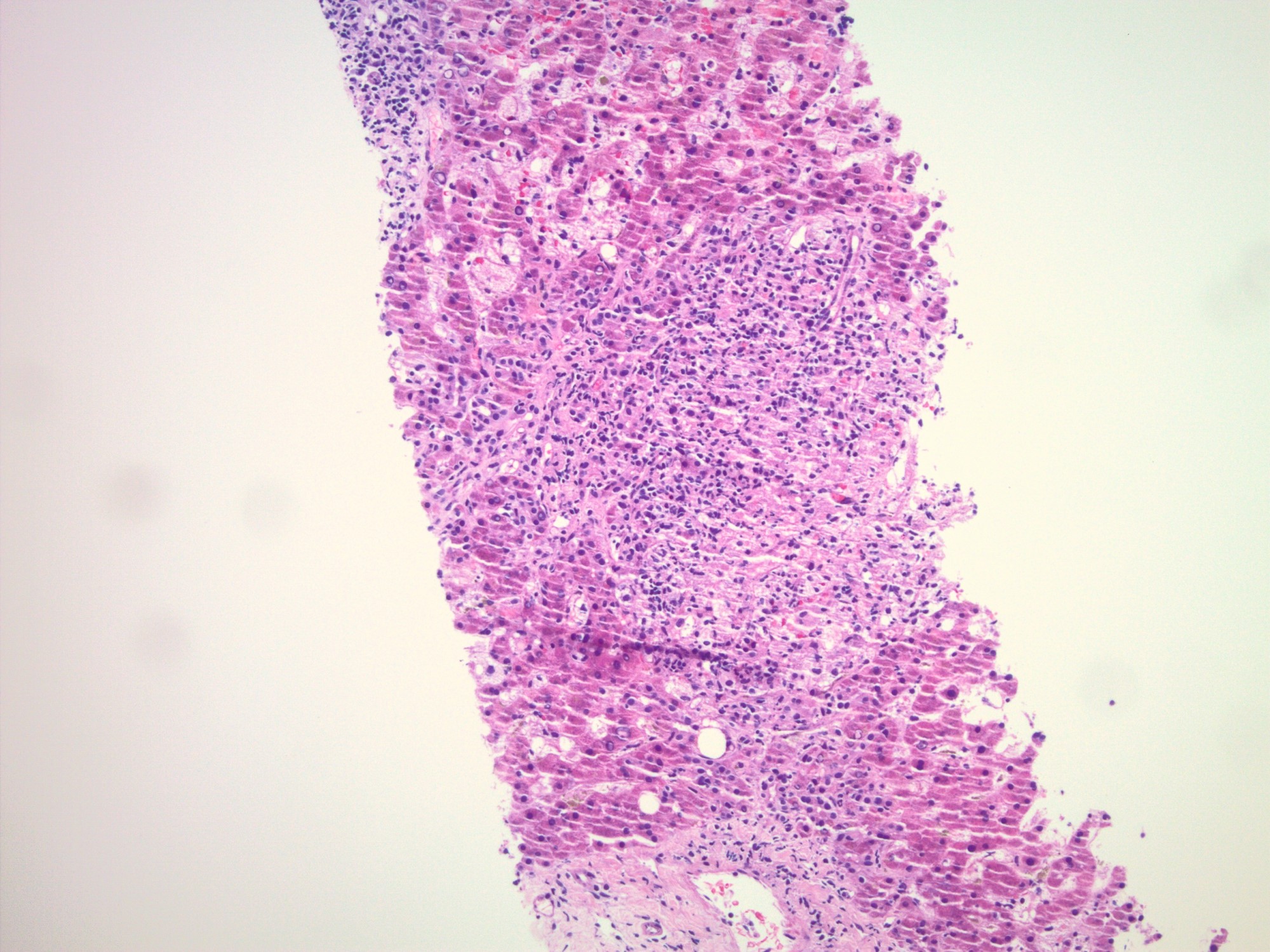
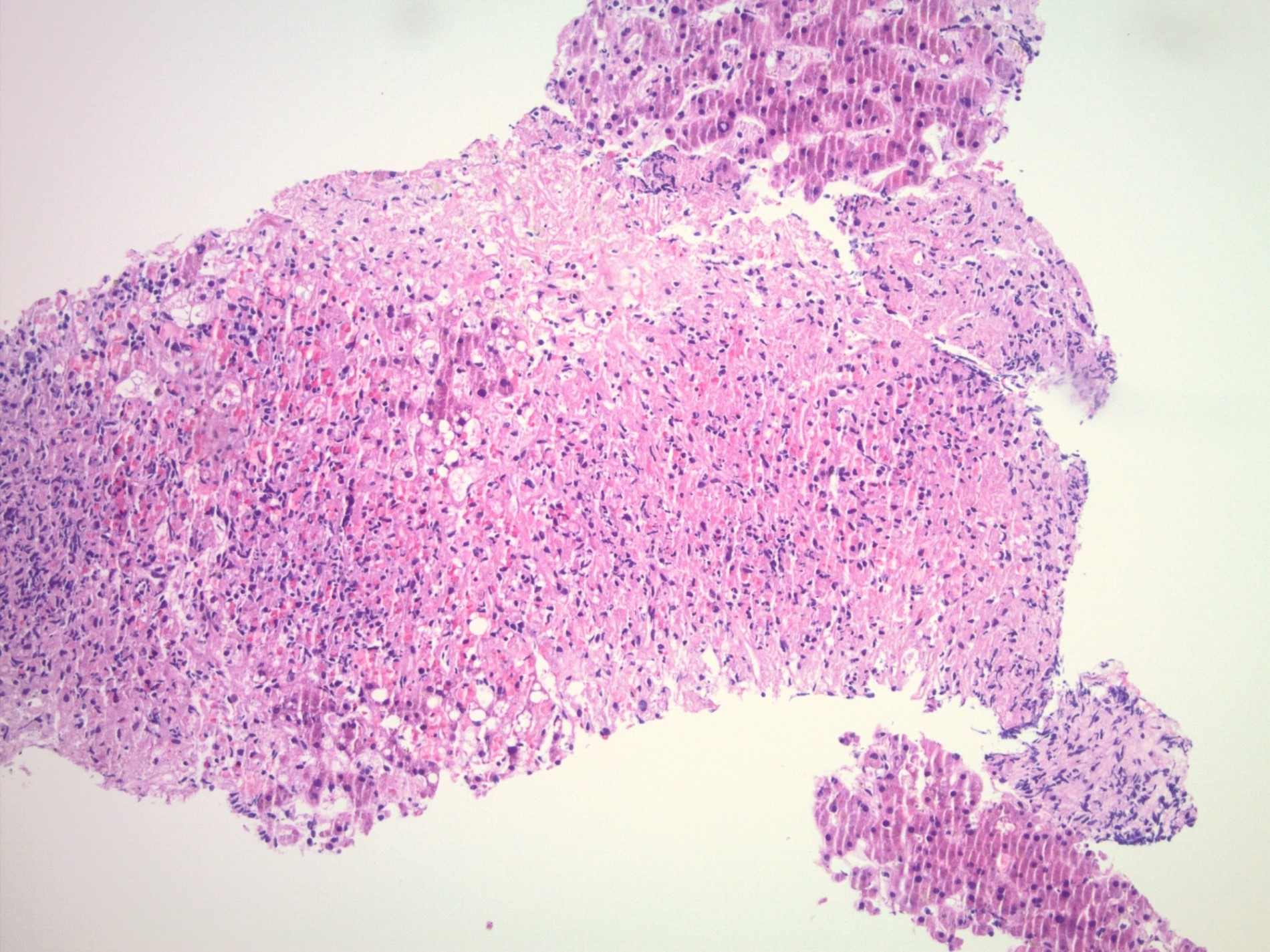
Confluent necrosis
Bile ductular reaction
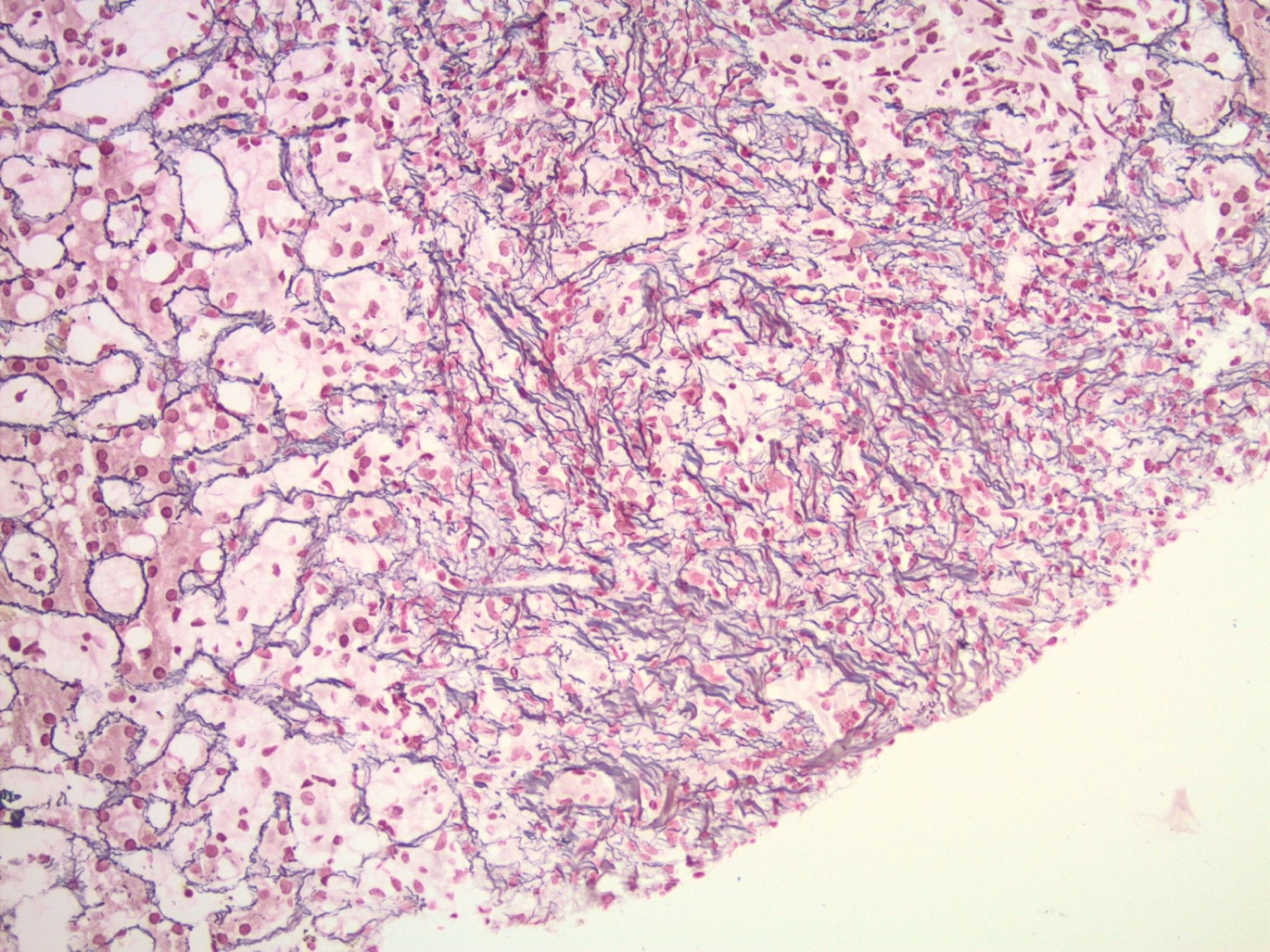
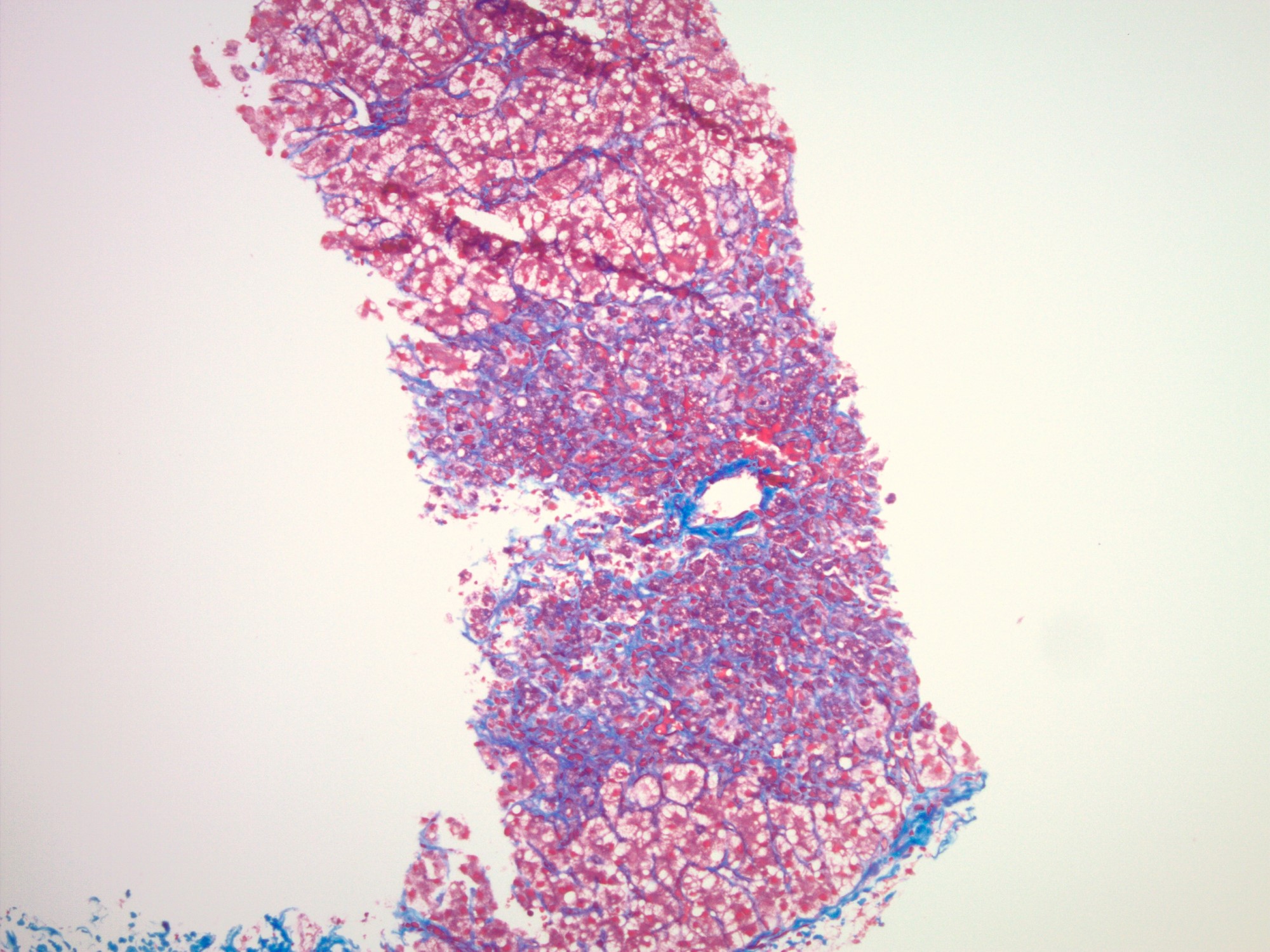
Parenchymal collapse
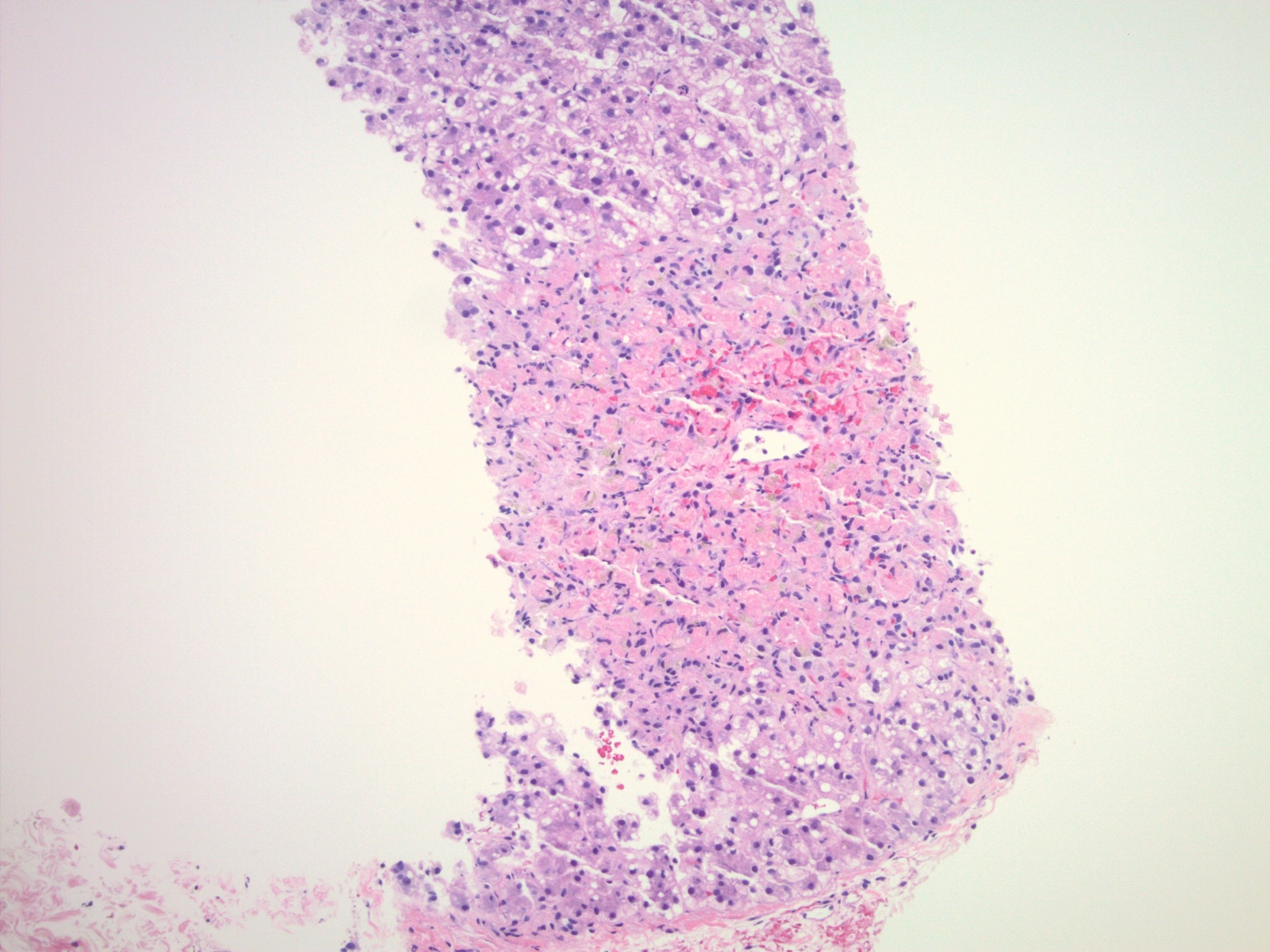
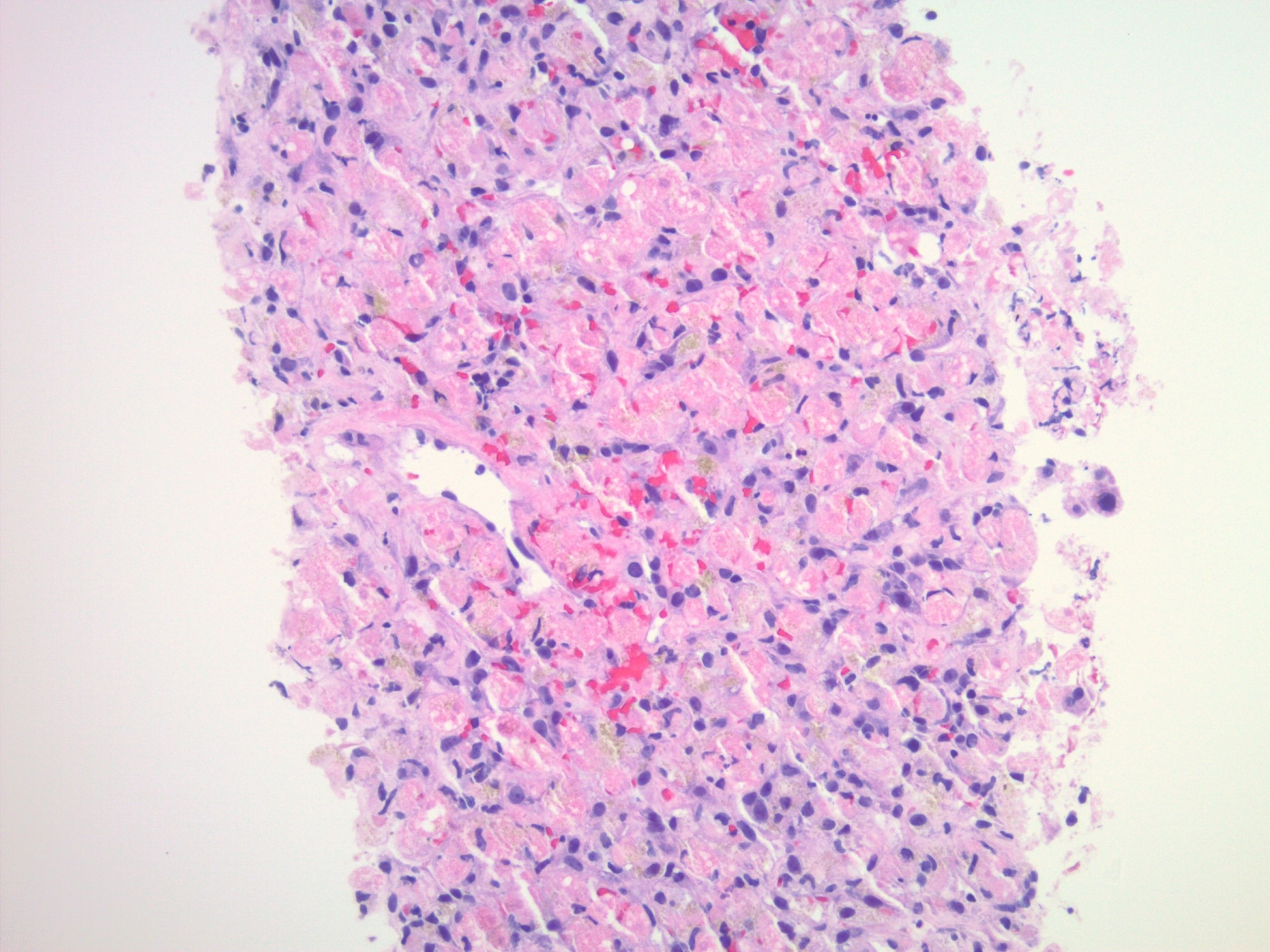
Confluent necrosis
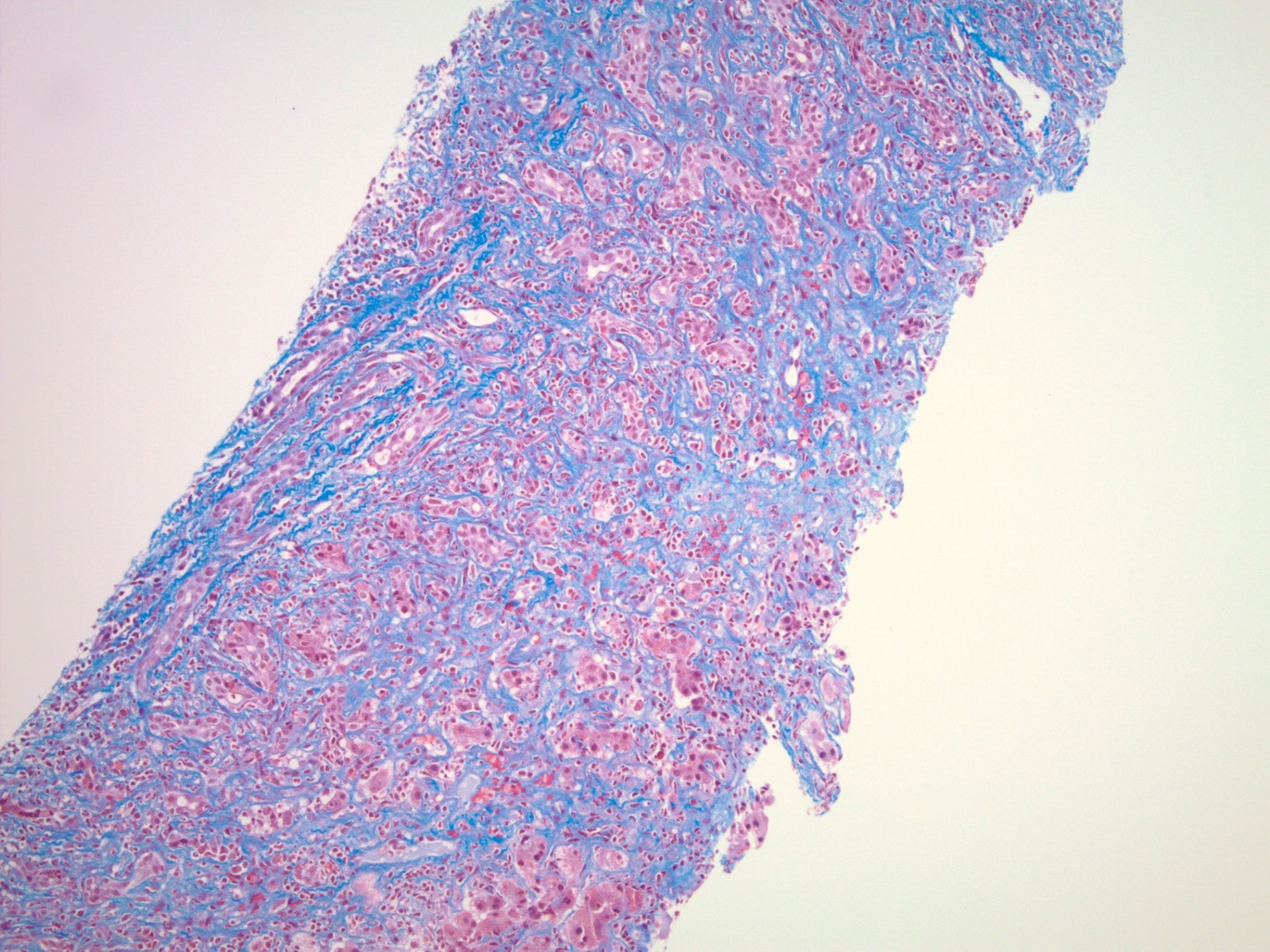
Positive stains
- Reticulin: in areas of parenchymal collapse / necrosis, the reticulin framework will remain and appear condensed as hepatocytes are lost
- Trichrome: areas of necrosis and hepatocyte dropout will appear as pale gray-blue staining
- These areas consist of reticulin fibers composed of type 3 collagen and will appear lighter in staining compared to the type 1 collagen fibers
- Reference: Saxena: Practical Hepatic Pathology, 2nd Edition, 2017
Sample pathology report
- Liver, core needle biopsy:
- Zone 3 predominant hepatocyte necrosis with Kupffer cell hyperplasia and early parenchymal collapse (see comment)
- Comment: The biopsy consists of 3 fragments of hepatic parenchyma with zone 3 predominant hepatocyte necrosis, early parenchymal collapse (trichrome stain) and Kupffer cell hyperplasia. Outside of the areas of early parenchymal collapse, there is no significant fibrosis. The lobules contain scattered balloon cells with focal acute inflammation. There is no significant portal inflammation or bile duct injury. The findings are consistent with an acute hepatitis pattern and the differential includes drug induced liver injury. Clinical and serologic correlation is recommended.
Differential diagnosis
- All etiologies listed have similar histologic features with the following subtle differences:
- Viral hepatitis (hepatotropic versus nonhepatotropic):
- Portal infiltrate in hepatitis A may be more robust, contain more plasma cells and there may be spillover across the limiting plate
- Hepatitis E may have a degree of bile pigment accumulation
- Hepatitis C has less ballooning degeneration and fewer apoptotic bodies, compared to other viruses (Liver 1981;1:201)
- EBV infection will show an activated lymphocytic inflammatory infiltrate in sinusoids and portal tracts
- Drug induced liver injury (direct toxins versus idiosyncratic drug reactions):
- Some cases have ductular reaction, neutrophilic inflammation, Kupffer cells, bile duct injury, prominent eosinophils, granulomas, cholestasis
- Autoimmune hepatitis:
- Typically, plasma cell rich inflammation in lobules and portal tracts, occasionally with emperipolesis
- Acute alcoholic hepatitis:
- Numerous ballooned hepatocytes with Mallory hyaline formation, neutrophilic lobular inflammation and occasional lobular cholestasis
- Central hyaline sclerosis
- Nonviral infections (Kupffer cell hyperplasia, cholestasis, steatosis, granulomas)
- Wilson disease:
- Lipofuscin and copper accumulation
- Often shows some degree of liver fibrosis already at the time of acute liver failure
- Viral hepatitis (hepatotropic versus nonhepatotropic):
Additional references
Practice question #1
Which statement regarding acute hepatitis is true?
- Antibiotics are not considered a drug class that can cause an acute hepatitis
- Hepatitis A and nonhepatotropic viruses do not lead to chronic liver disease
- Hepatitis C can lead to acute liver failure in pregnant women
- Portal fibrosis and neoangiogenesis are features of acute hepatitis
Practice answer #1
B. Hepatitis A and nonhepatotropic viruses do not lead to chronic liver disease
Chronic viral hepatitis is only caused by hepatotropic viruses (mainly B and C). Portal fibrosis and neoangiogenesis are considered patterns of chronic injury and are not seen in acute hepatitis. Acute hepatitis can be seen in drug induced liver injury. The most common drugs include antibiotics, neurologic drugs, NSAIDs, statins, cardiovascular agents and immunomodulatory drugs. 30% of hepatitis E infections can lead to acute liver failure in pregnant women.
Comment Here
Reference: Acute hepatitis-general
Chronic viral hepatitis is only caused by hepatotropic viruses (mainly B and C). Portal fibrosis and neoangiogenesis are considered patterns of chronic injury and are not seen in acute hepatitis. Acute hepatitis can be seen in drug induced liver injury. The most common drugs include antibiotics, neurologic drugs, NSAIDs, statins, cardiovascular agents and immunomodulatory drugs. 30% of hepatitis E infections can lead to acute liver failure in pregnant women.
Comment Here
Reference: Acute hepatitis-general
Practice question #2
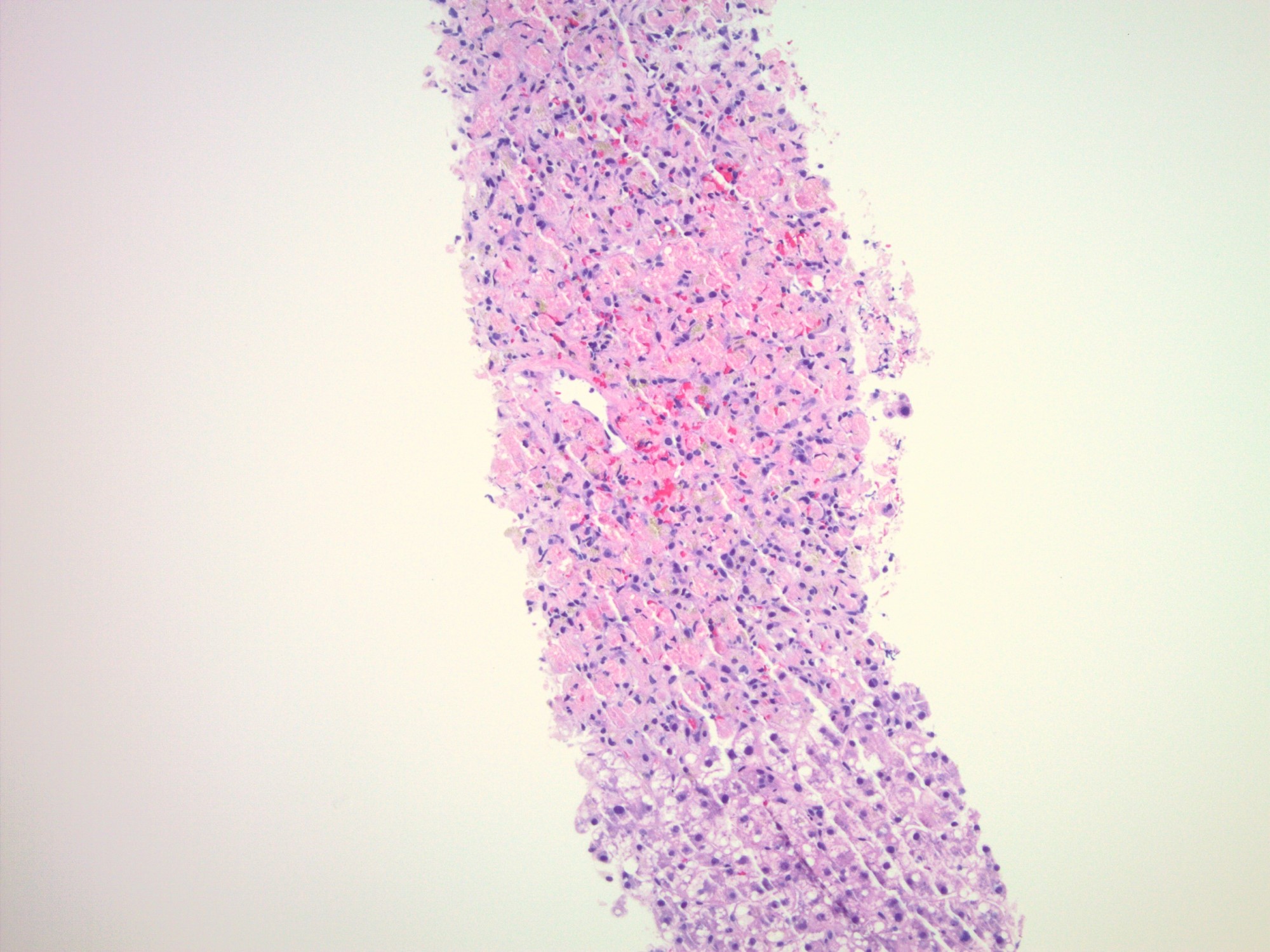
Which of the following entities is least likely to be included in the differential diagnosis for the images shown above?
- Acute autoimmune hepatitis
- Acute hepatitis A infection
- Chronic hepatitis C infection
- Drug induced liver injury
Practice answer #2
C. Chronic hepatitis C infection
The images depict a zone 3 predominant lobular inflammatory infiltrate with associated confluent necrosis. The findings are consistent with an acute hepatitis pattern of injury. Acute hepatitis C infection is rarely biopsied and most cases of hepatitis C that are biopsied reflect a chronic infection. The histologic features include a mild to moderately dense chronic portal inflammatory infiltrate with focal mild interface activity. Lymphoid aggregates can be present with lymphocytic cholangitis (Poulsen-Christofferson lesion).
Comment Here
Reference: Acute hepatitis-general
The images depict a zone 3 predominant lobular inflammatory infiltrate with associated confluent necrosis. The findings are consistent with an acute hepatitis pattern of injury. Acute hepatitis C infection is rarely biopsied and most cases of hepatitis C that are biopsied reflect a chronic infection. The histologic features include a mild to moderately dense chronic portal inflammatory infiltrate with focal mild interface activity. Lymphoid aggregates can be present with lymphocytic cholangitis (Poulsen-Christofferson lesion).
Comment Here
Reference: Acute hepatitis-general
