Liver & intrahepatic bile ducts
Benign / nonneoplastic
Mesenchymal hamartoma
Editorial Board Members: Monika Vyas, M.D., Aaron R. Huber, D.O.


Last author update: 12 December 2022
Last staff update: 9 May 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Mesenchymal hamartoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Liu BL, Ward SC. Mesenchymal hamartoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertumormesenchymalhamart.html. Accessed August 27th, 2025.
Definition / general
- Rare, benign hepatic lesion of young children
- Primitive myxoid mesenchyme with benign dilated or branching bile ducts and clusters of normal appearing hepatocytes
Essential features
- Second most common benign pediatric hepatic tumor after infantile hemangioma (Arch Pathol Lab Med 2006;130:1567)
- 80% are diagnosed in infants and children < 2 years old (Arch Pathol Lab Med 2006;130:1567)
- Excellent prognosis with complete resection; rare malignant transformation to embryonal sarcoma has been described
- Variable proportions of mixed solid and cystic areas with disorganized arrangement of primitive mesenchyme, benign bile ducts and normal appearing hepatocytes (Hepat Oncol 2020;7:HEP19)
- Associated with recurrent genetic alterations resulting in activation of chromosome 19 microRNA cluster (C19MC)
Terminology
- Hepatic or giant lymphangiomas, bile cell fibroadenomas, cavernous lympangiomatoid tumors, hepatic cystic hamartoma (SA J Radiol 2020;24:1891)
ICD coding
- ICD-10: D13.4 - benign neoplasm of liver
Epidemiology
- Second most common benign liver tumor in pediatric population
- Incidence: 0.7 cases per million population per year (J Radiol Case Rep 2013;7:35)
- 80% are diagnosed in patients < 2 years old with a slight male predominance (60 - 70% male) (Arch Pathol Lab Med 2006;130:1567)
- Adults rarely affected, with slight female predominance (Hum Pathol 2002;33:893)
Sites
- Pediatric patients: right liver lobe predilection
- Adults: similar involvement of both liver lobes (Hum Pathol 2002;33:893)
Pathophysiology
- Still debated
- Associated with activation of chromosome 19q13.4 microRNA cluster (C19MC) (Pediatr Dev Pathol 2014;17:75)
Clinical features
- Usually sporadic; associations with Beckwith-Wiedemann syndrome and placental mesenchymal dysplasia have been described (Pediatr Dev Pathol 2014;17:75)
- Typically present as an enlarging abdominal mass
- Small lesions are usually asymptomatic
- Large lesions may be associated with abdominal pain, abdominal distention, vomiting, poor weight gain, respiratory distress, cardiac failure and ascites (J Clin Neonatol 2012;1:211)
- Rarely, may undergo malignant transformation to undifferentiated embryonal sarcoma (Hepat Oncol 2020;7:HEP19)
Diagnosis
- Histologic examination
Laboratory
- AFP usually normal or mildly elevated (SA J Radiol 2020;24:1891)
- Occasionally markedly elevated (J Cytol 2015;32:197)
Radiology description
- Complex cystic mass with internal septations on ultrasound
- Complex cystic mass with septal and solid stromal enhancement on CT or MRI
Radiology images
Images hosted on other servers:

CT scans
Case reports
- 5 month old girl with Beckwith-Wiedemann syndrome with diarrhea and abdominal mass (ACG Case Rep J 2015;2:258)
- 15 month old asymptomatic boy with large hepatic mass (Case #61)
- 34 month old girl with abdominal distention, respiratory distress and bowel obstruction (J Surg Case Rep 2018;2018:rjx260)
- 46 year old woman with abdominal pain and distension (Transplant Proc 2022;54:1636)
Treatment
- Complete surgical excision: best treatment
- Unresectable cases may require liver transplantation (Transplant Proc 2022;54:1636)
Gross description
- Usually solitary; rarely with intrahepatic satellite nodules
- Well circumscribed mass with mixed solid and cystic areas
- Cysts contain clear, yellow or gelatinous fluid separated by white, yellow or tan firm tissue (Burt: MacSween's Pathology of the Liver, 7th Edition, 2017)
- Size ranging from a few centimeters to 30 cm
- Usually no necrosis, hemorrhage or calcification
- Becomes fibrotic with age
Gross images
Contributed by Bella Lingjia Liu, M.D.
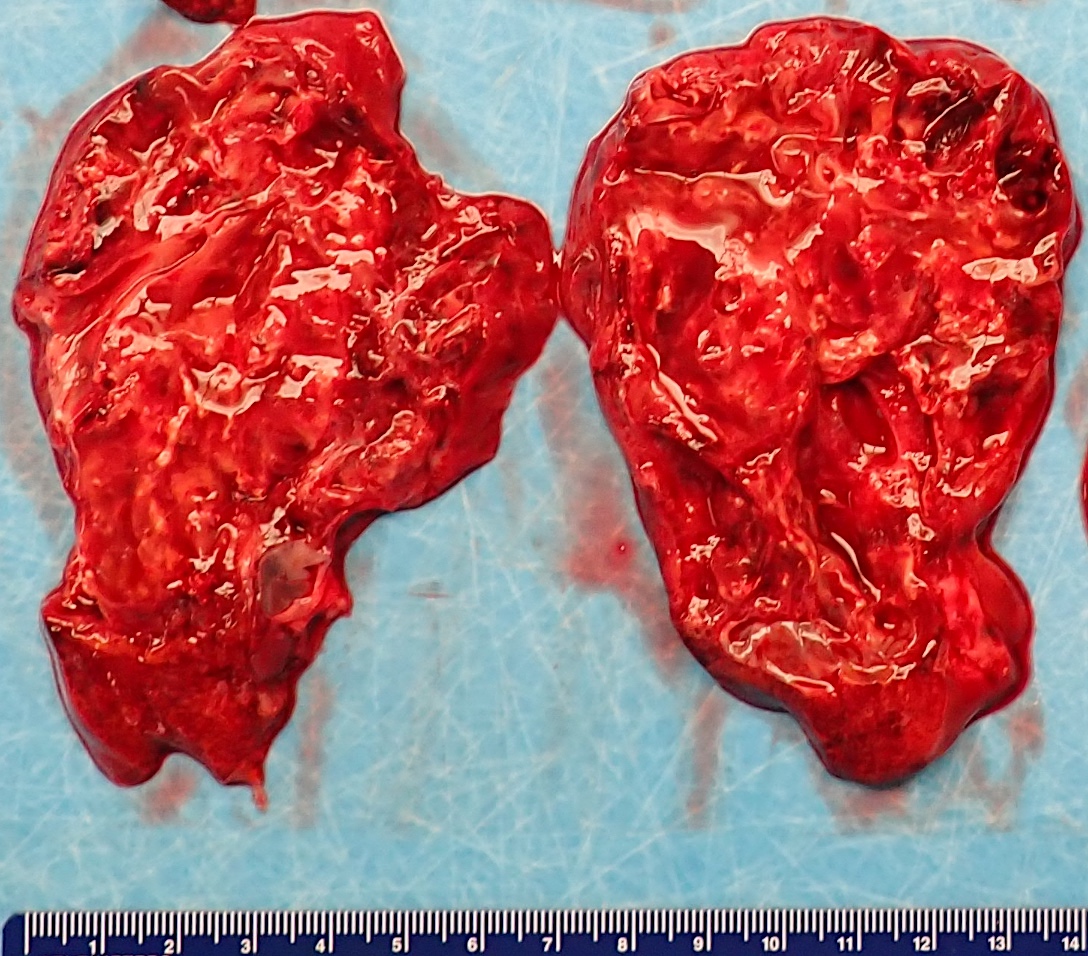

Cut surface of the tumor
Images hosted on other servers:

Cut surface of the tumor
Microscopic (histologic) description
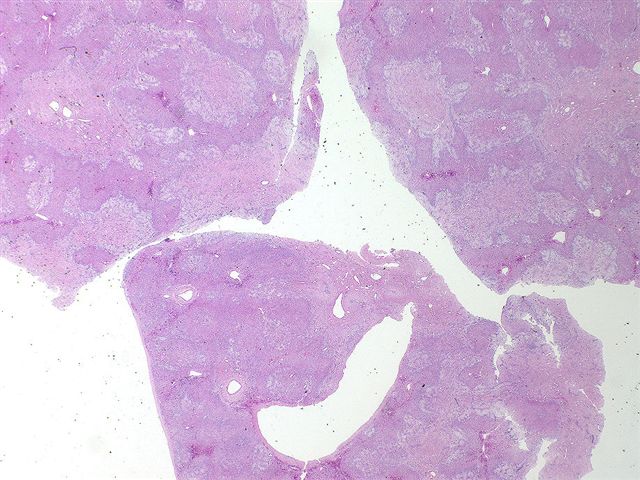
- Variable proportions of solid and cystic components with disorganized arrangements of:
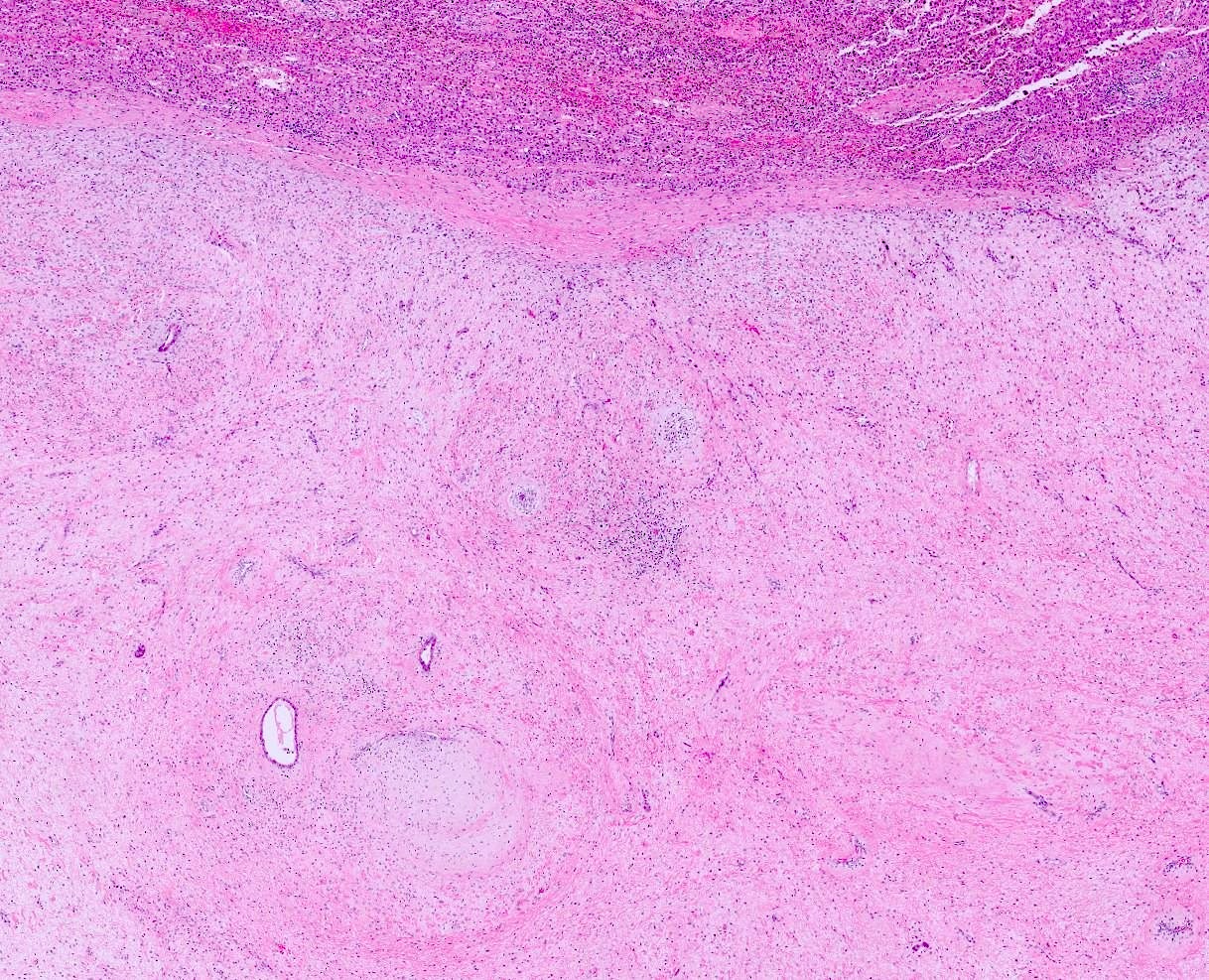
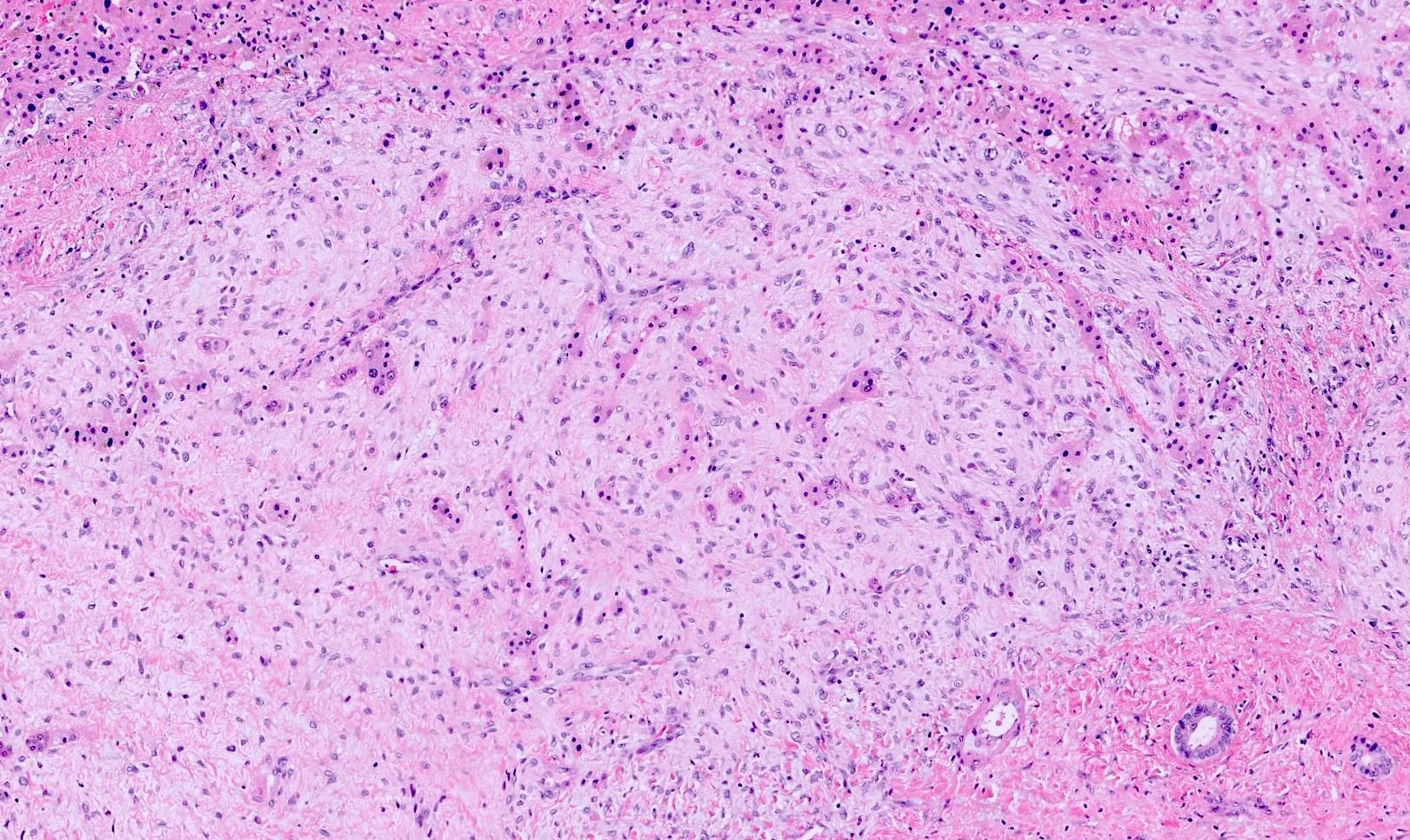
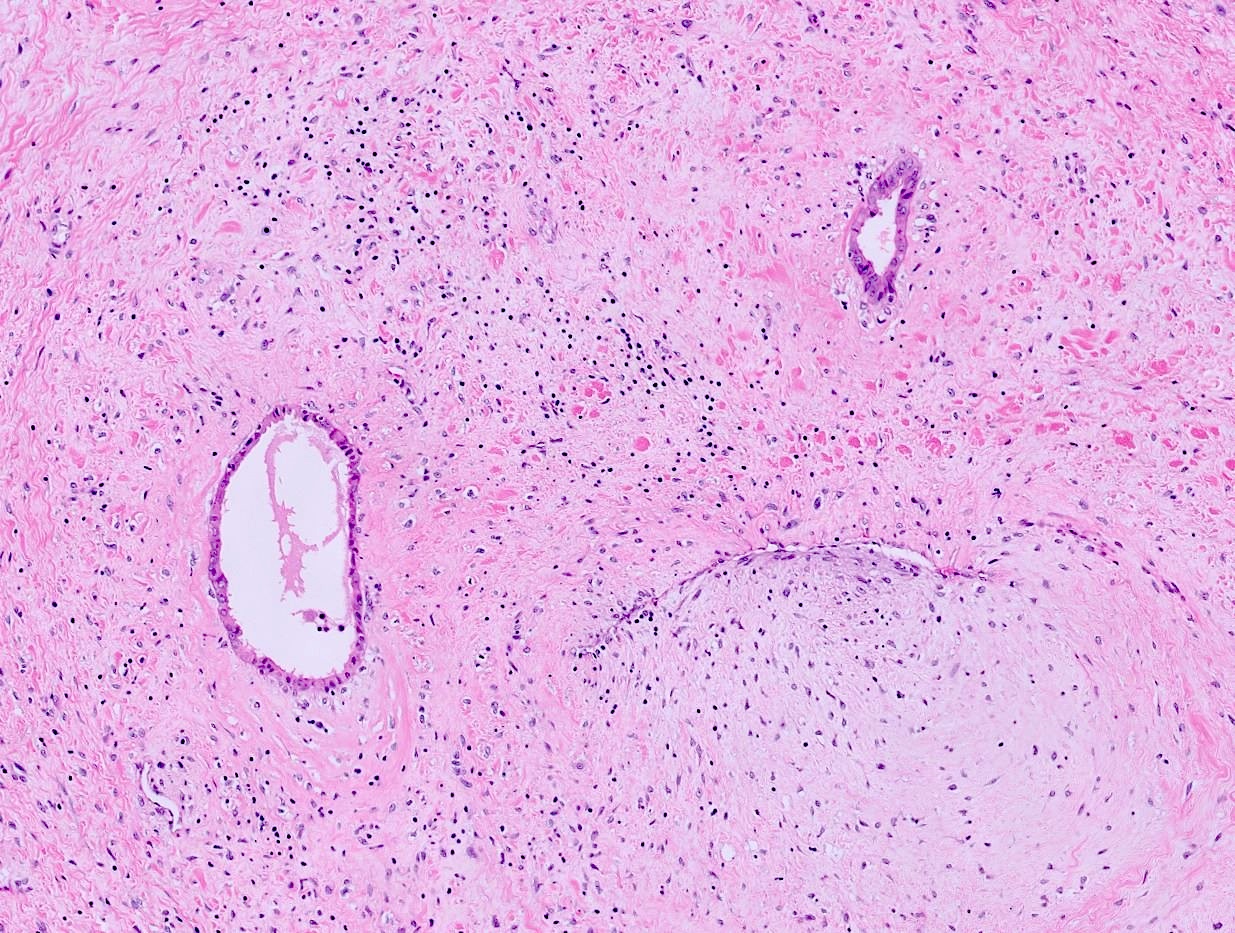
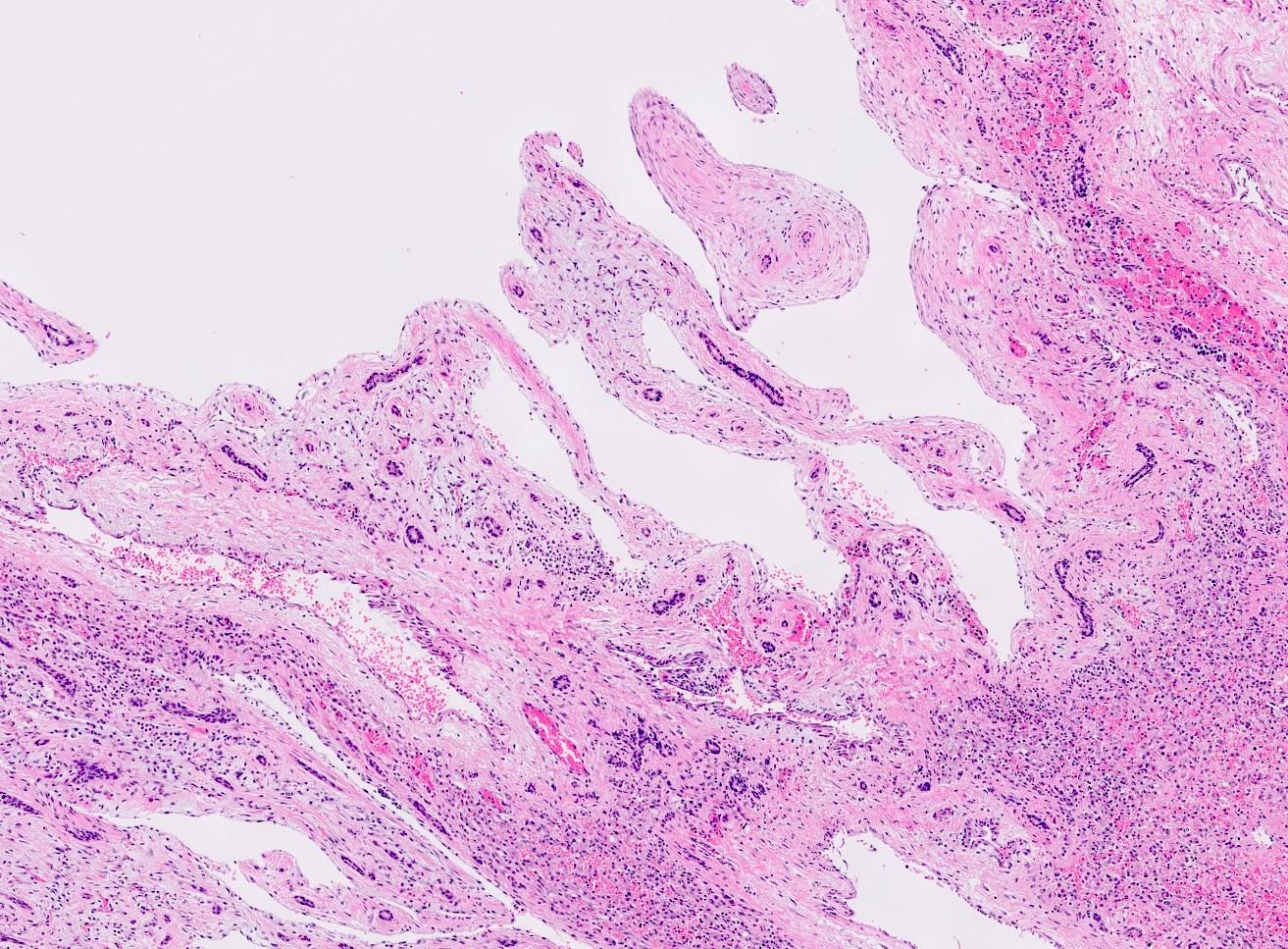
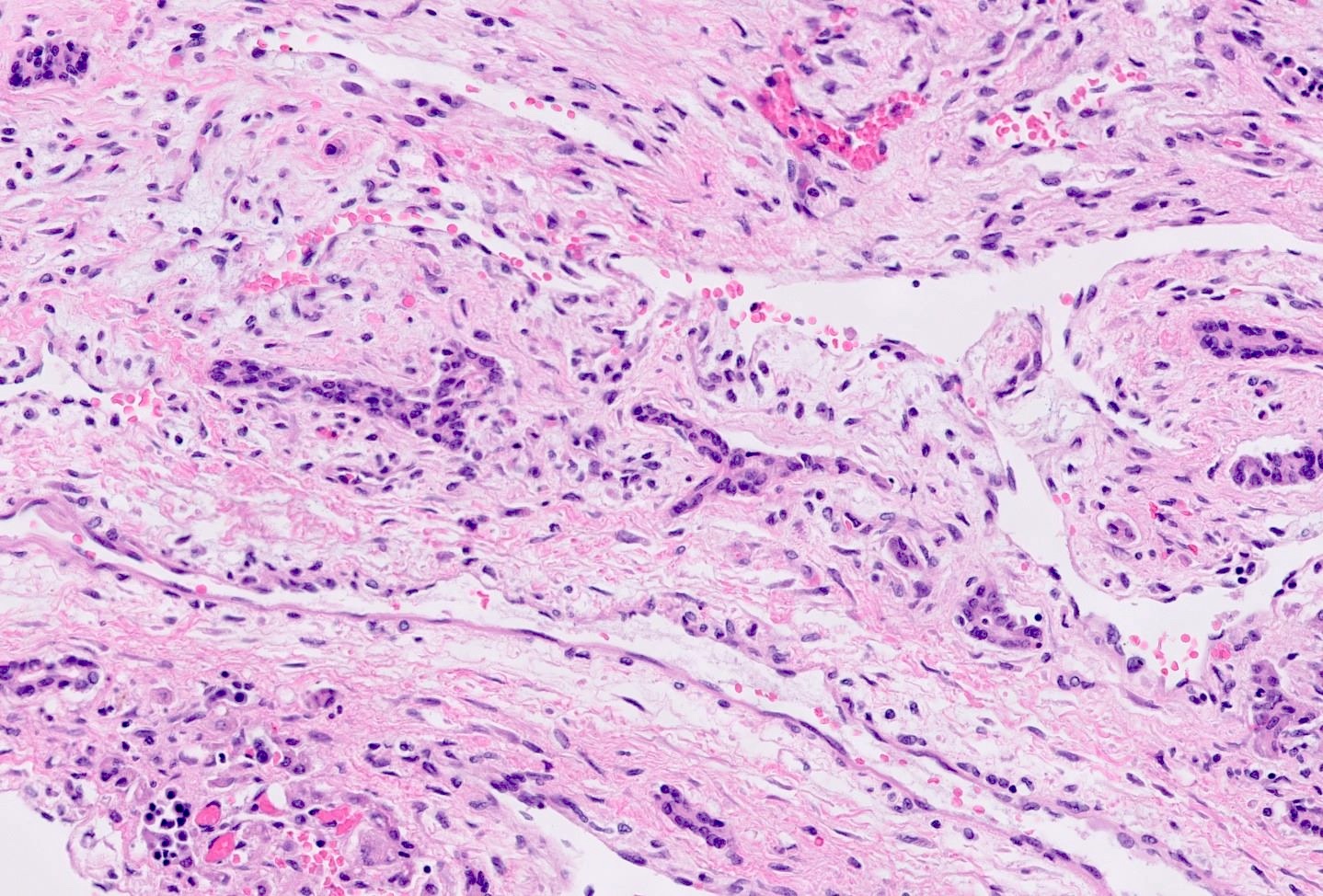
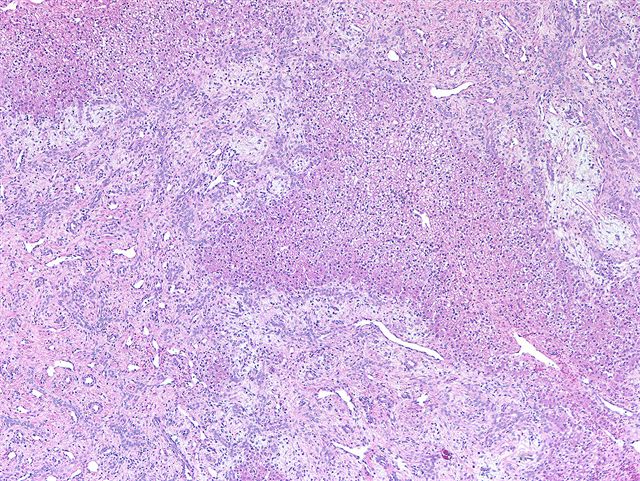
- Primitive mesenchyme, with mixture of bland spindled cells and collagen in a loose, myxoid stroma (Burt: MacSween's Pathology of the Liver, 7th Edition, 2017)
- Epithelial components, including benign dilated or branching bile ducts and normal appearing peripherally located hepatocytes
- Loss of normal lobular architecture; no portal tracts (Burt: MacSween's Pathology of the Liver, 7th Edition, 2017)
- Cystic degeneration is frequently seen, giving rise to lymphangioma-like areas (Burt: MacSween's Pathology of the Liver, 7th Edition, 2017)
- No significant cytologic atypia or increased mitoses (Arch Pathol Lab Med 2006;130:1567)
- May resemble breast fibroadenoma at low power
- Frequent extramedullary hematopoiesis is present (Ishak: Tumors of the Liver and Intrahepatic Bile Ducts, 3rd Series, Volume 31, 2001)
- Tends to have more hyalinized fibrous tissue, fewer ductal structures and show more vascularity in adult patients (J Pediatr Surg 2005;40:1681)
Microscopic (histologic) images
Contributed by Bella Lingjia Liu, M.D. and Ankur R. Sangoi, M.D. (Case #61)
Solid area
Entrapped benign hepatocytes
Bile ducts
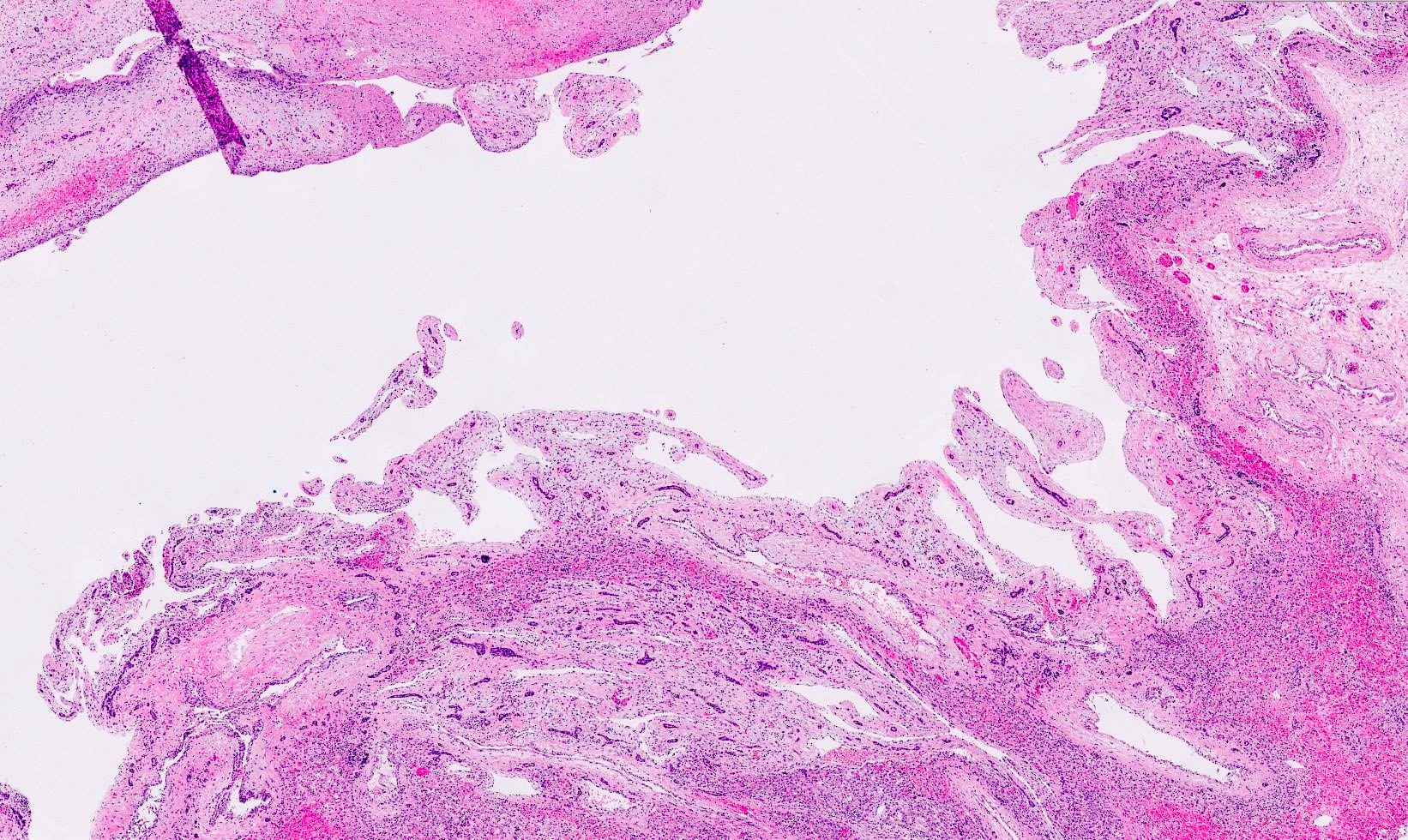
Cystic area
Branching bile ducts
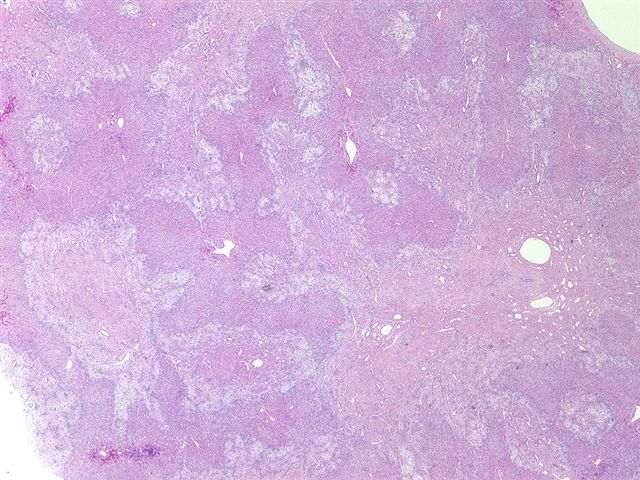
Disorganized hepatic architecture
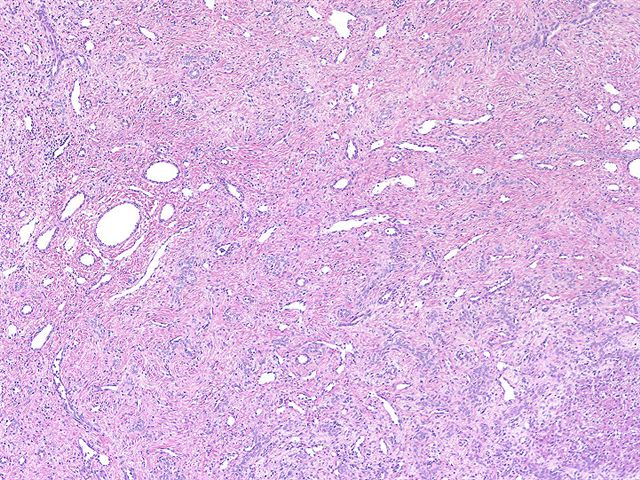
Dilated and branching bile ducts
Hepatocytes in myxoid stroma
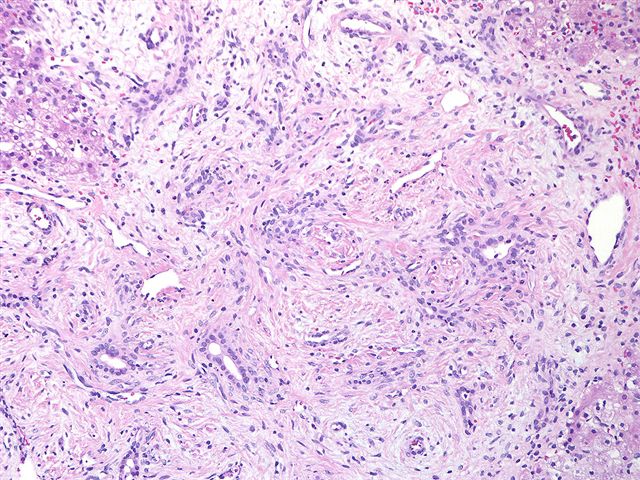
Bland bile duct structures
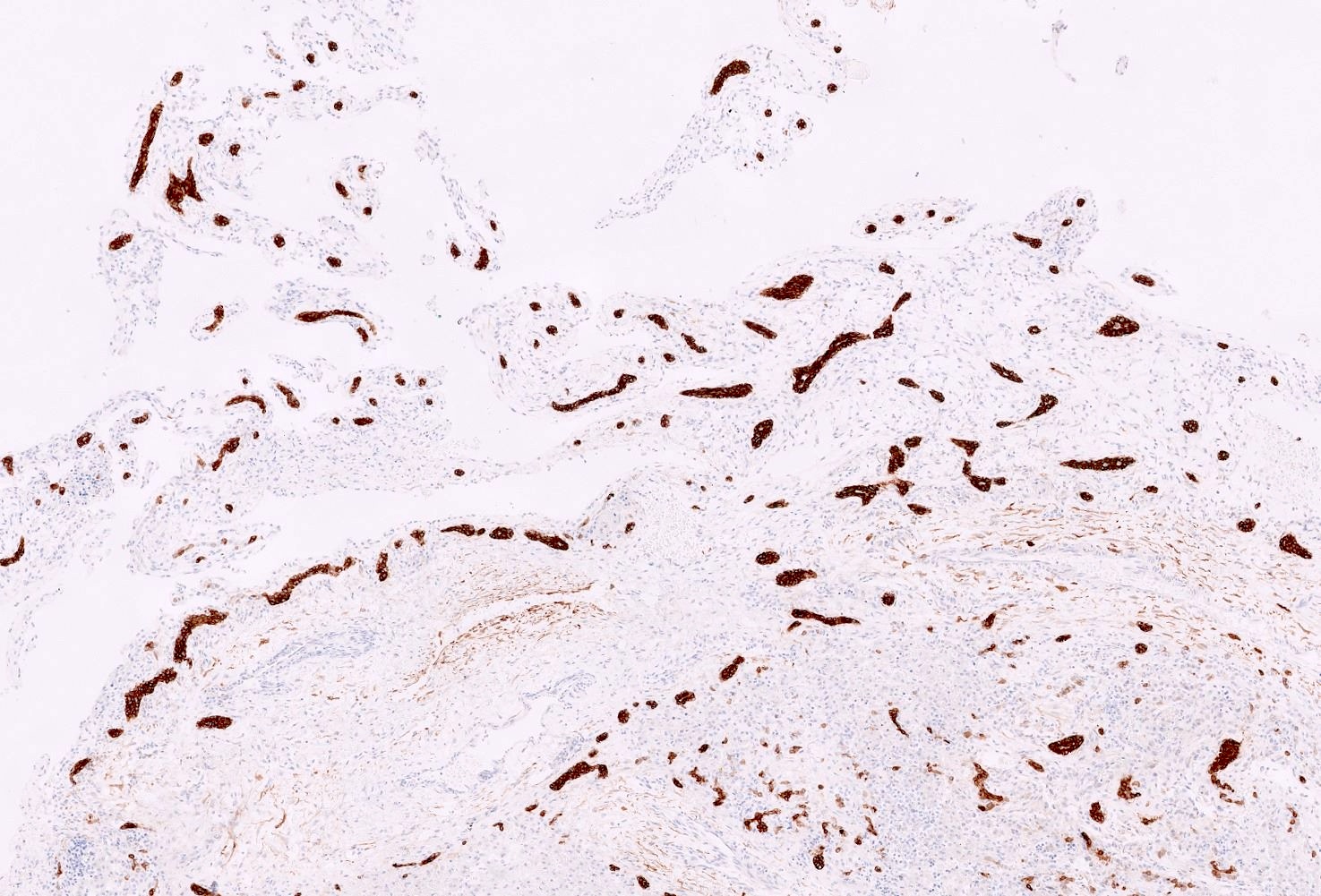
CK7
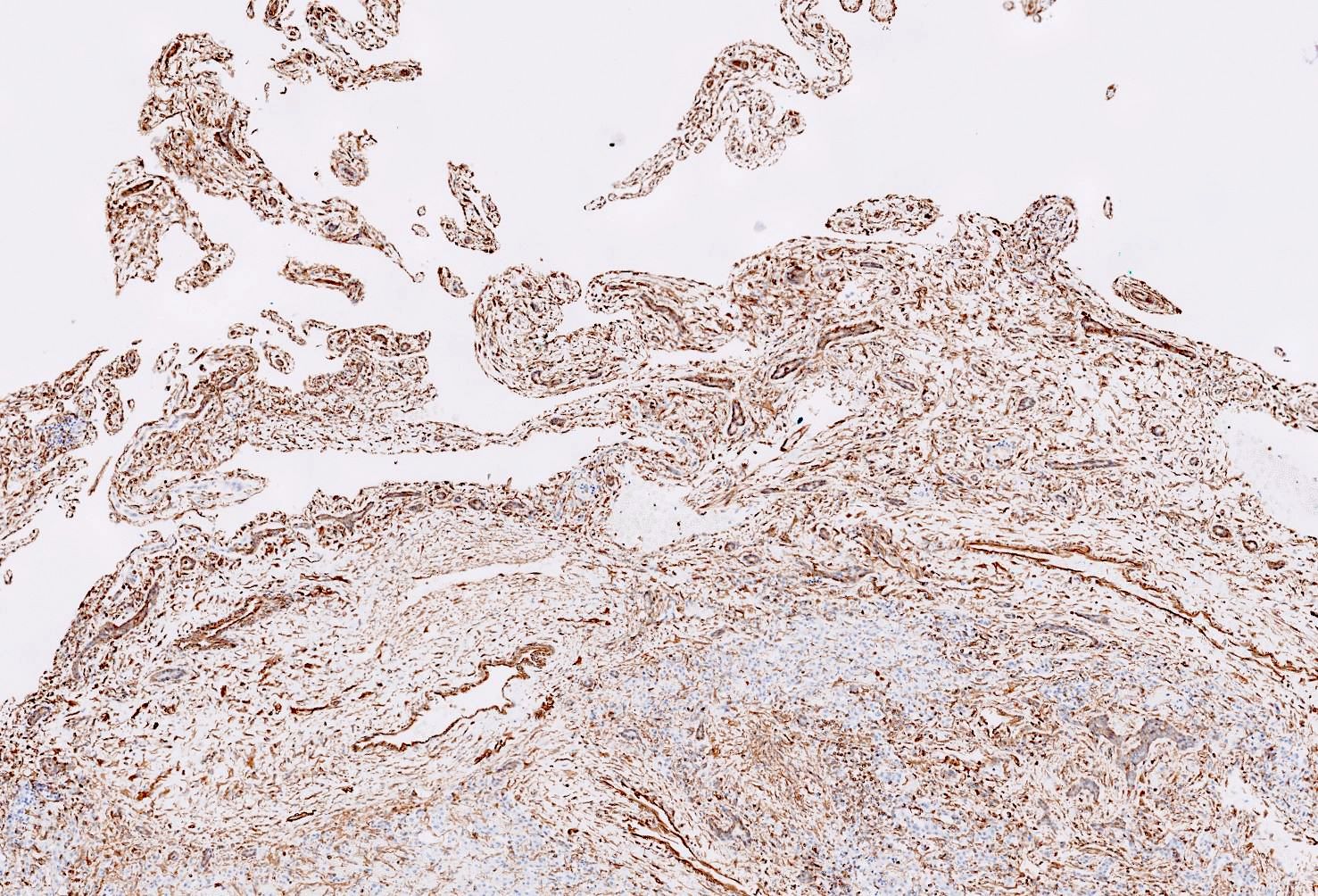
Vimentin
Cytology description
- Clusters of bland cuboidal epithelial cells, spindle stromal cells, hepatocytes, myxoid tissue (Burt: MacSween's Pathology of the Liver, 7th Edition, 2017)
- Limited value
Cytology images
Images hosted on other servers:

Hepatic mesenchymal hamartoma
Positive stains
- CK7: biliary epithelium
- Vimentin, smooth muscle actin, desmin, alpha-1 antitrypsin: mesenchymal cells
- Glypican 3: entrapped hepatocytes (44%, canalicular and cytoplasmic staining pattern) and mesenchymal component (22%) (Hum Pathol 2012;43:695)
Electron microscopy description
- Myofibroblastic features
Molecular / cytogenetics description
- Activation of chromosome 19q13.4 microRNA cluster (C19MC), either by rearrangement of 19q13 or androgenetic biparental mosaicism (Pediatr Dev Pathol 2015;18:218, Pediatr Dev Pathol 2014;17:75)
Sample pathology report
- Liver mass, resection specimen:
- Hepatic mesenchymal hamartoma (16 cm) (see comment)
- Comment: The neoplasm consists of scattered dilated and angulated ducts lined by cuboidal epithelium in a background of loose myxoid tissue with scattered bland spindle cells. Small islands of entrapped benign hepatic parenchyma are noted. No necrosis or mitotic figures are identified. The tumor is located 0.5 cm from the nearest surgical resection margin. Hilar structures are free of tumor. The adjacent hepatic parenchyma shows congestion and mild portal fibrosis, portal inflammation and proliferation of bile ductules consistent with adjacent mass effect.
- Liver, needle biopsy specimen:
- Hepatic mesenchymal hamartoma (see comment)
- Comment: Lesion is characterized by loose myxomatous stroma with scattered bland stellate shaped mesenchymal cells, branching bile ducts and scattered hepatocytes. The findings are consistent with hepatic mesenchymal hamartoma.
Differential diagnosis
- Myxomatous infantile hemangioma / hemangioendothelioma:
- Most common hepatic mesenchymal tumor in childhood
- Majority affects infants < 6 months old, with slight female predominance
- Can be well circumscribed or infiltrative (35%)
- Type 1 with proliferation of capillary-like vascular spaces lined by bland endothelial cells with no / rare mitotic figures and no malignant spindle cell component
- Type 2 with irregular branching vascular structures lined by pleomorphic, hyperchromatic endothelial cells with frequent mitotic activity
- Positive for GLUT1, CD31, CD34 and factor VIII related antigen
- Undifferentiated embryonal sarcoma:
- Third most common pediatric hepatic tumor, mainly affecting children 6 - 10 years old
- Anaplastic, bizarre tumor cells with prominent eosinophilic cytoplasm and PAS+ diastase resistant hyaline globules
- Mixed epithelial mesenchymal hepatoblastoma:
- Epithelial component with embryonal and fetal hepatocytes with high N:C ratios and marked cellular atypia
- Mesenchymal component has spindle cells, osteoid, cartilage
Practice question #1
A 9 month old boy with abdominal distention was found to have a 7.3 x 6.5 x 3.4 cm complex cystic mass in the right liver. Histologic examination of the cyst wall revealed the findings shown above. What is the diagnosis?
- Angiomyolipoma
- Bile duct hamartoma
- Hepatic mesenchymal hamartoma
- Myxomatous infantile hemangioma / hemangioendothelioma
- Undifferentiated embryonal sarcoma
Practice answer #1
Practice question #2
Which of the following statements regarding hepatic mesenchymal hamartoma is true?
- Associated with recurrent genetic alteration resulting in activation of chromosome 19 microRNA cluster (C19MC)
- Has variable proportions of cystic and solid components and is commonly associated with necrosis with frequent mitotic figures and cytological atypia
- It is the second most common benign hepatic tumor, mainly affecting adults between 20 - 50 years old
- Positive for GLUT1 in the epithelial components
- Radiation therapy is the best treatment method
Practice answer #2
A. Associated with recurrent genetic alteration resulting in activation of chromosome 19 microRNA cluster (C19MC)
Comment Here
Reference: Mesenchymal hamartoma
Comment Here
Reference: Mesenchymal hamartoma
