

Lung
Other nonneoplastic conditions
Acute lung injury
Acute fibrinous and organizing pneumonia
Last author update: 1 January 2018
Last staff update: 13 October 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed search: Acute fibrinous and organizing pneumonia
Related topics: Acute respiratory distress syndrome (ARDS) / diffuse alveolar damage (DAD)



Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Yoshikawa, A. and Fukuoka, J. Acute fibrinous and organizing pneumonia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungnontumordiffusealveolardamageafop.html. Accessed April 26th, 2024.
Definition / general
- In 2002, Beasley et al. first described a progressive variant of lung injury with organizing pneumonia and intra-alveolar fibrin, which does not fit the histologic pattern of diffuse alveolar damage (DAD), organizing pneumonia (OP) or eosinophilic pneumonia (Arch Pathol Lab Med 2002;126:1064)
Essential features
- It is a newly proposed subacute interstitial pneumonia similar to organizing pneumonia or organizing diffuse alveolar damage
- Histologically, remarkable fibrin deposition (or "fibrin balls") along with plugs of organizing pneumonia in air spaces are characteristic
Terminology
- Also called acute fibrinous organizing pneumonia
Epidemiology
- Rare disease (no data on prevalence available so far)
- Mean age at onset is about 60 years old, with a wide age range (Arch Pathol Lab Med 2002;126:1064, J Clin Pathol 2015;68:441, Chin Med J (Engl) 2015;128:2701, Medicine (Baltimore) 2016;95:e4073)
- No gender predominance
- No association with smoking history
Sites
- Usually bilateral or sometimes unilateral lobes of the lung
Pathophysiology
- In the initial study, acute fibrinous and organizing pneumonia (AFOP) was described as a possible variant of diffuse alveolar damage because of its similar aggressive behavior and mortality rate (Arch Pathol Lab Med 2002;126:1064)
- However, recent studies and case reports have found that the clinical course and prognosis of AFOP is better and closer to that of organizing pneumonia (J Clin Pathol 2015;68:441, Chin Med J (Engl) 2015;128:2701)
- Nowadays, AFOP is considered a histological variant of organizing pneumonia or a different type of lung disease similar to organizing pneumonia, which sometimes follows an aggressive course
- Some idiopathic AFOP may be due to infection of undiagnosed bacteria
Etiology
- Variety of possible causes and associated conditions have been reported (Arch Pathol Lab Med 2002;126:1064, J Clin Pathol 2015;68:441, Chin Med J (Engl) 2015;128:2701, Medicine (Baltimore) 2016;95:e4073):
- Idiopathic
- Infection: H. influenzae, A. baumannii, P. jirovecii, C. pneumoniae
- Autoimmune disease: polymyositis / dermatomyositis, ankylosing spondylitis, antisynthetase syndrome
- Particle exposure: animal antigens, coal dust, wood dust, hairspray
- Neoplasm: cancer, lymphoma, leukemia, myelodysplastic syndrome
- Immunosuppression: diabetes mellitus, long term corticosteroid therapy
- Drugs
- Hematopoietic stem cell transplantation (J Investig Med High Impact Case Rep 2016;4:2324709616643990)
- Lung transplantation
Clinical features
- Most patients present with mild to moderate subacute respiratory failure (J Clin Pathol 2015;68:441, Chin Med J (Engl) 2015;128:2701)
- Fever, fatigue and malaise
- Cough
- Dyspnea
- Sputum or sometimes hemoptysis
- Duration of symptoms before diagnosis is 1 - 4 weeks
- Some patients may follow fulminant course, need mechanical ventilation and die of the disease, similar to diffuse alveolar damage (Arch Pathol Lab Med 2002;126:1064, Medicine (Baltimore) 2016;95:e4073)
- Abnormal chest auscultation
- End inspiratory fine crackles in affected lobes
- Mild to moderate restrictive or obstructive pattern in pulmonary function tests (Chin Med J (Engl) 2015;128:2701)
- Decreased total lung capacity (TLC)
- Decreased forced vital capacity (FVC)
- Decreased diffusing capacity of the lung for carbon monoxide (DLCO)
Diagnosis
- Based on clinical features, radiology and histology
- No unique clinical or radiological findings have been identified to date
- Open chest lung biopsy is recommended
- Transbronchial lung biopsy or computed tomography guided needle lung biopsy may be diagnostic if clinical and radiological features are suggestive enough
- Acute fibrinous and organizing pneumonia can be a background pattern with other disease present
- If the specimen is too small and the main lesion is not included, acute fibrinous and organizing pneumonia can be underdiagnosed (Int J Clin Exp Pathol 2014;7:4493)
Laboratory
- Increased C reactive protein
- Increased serum surfactant proteins A and D
- Increased serum ferritin may predict prognosis
- Occasional positive sputum bacterial culture
- Negative serum antibodies of connective tissue diseases and hypersensitivity pneumonitis
Radiology description
- Simple chest radiography
- Bilateral or unilateral ground glass opacity and consolidation
- High resolution computed tomography (Radiographics 2013;33:1951):
- Variable images, similar to organizing pneumonia
- Typically, patchy mixture of ground glass opacity and consolidation
- Size varies from a few centimeters to a whole lobe
- Rapidly progressive variant may show bilateral diffuse opacity, similar to diffuse alveolar damage
- Variable images, similar to organizing pneumonia
Radiology images
Images hosted on other servers:



Chest radiograph



Acute fibrinous organizing pneumonia in left upper lobe

Multifocal opacities


Before and after corticosteroid therapy

Before disease onset and before / after corticoid therapy
Prognostic factors
- Most cases achieve remission with treatment (J Clin Pathol 2015;68:441, Chin Med J (Engl) 2015;128:2701)
- Some patients die of rapidly progressive disease (Arch Pathol Lab Med 2002;126:1064, Medicine (Baltimore) 2016;95:e4073)
Case reports
- Idiopathic acute fibrinous and organizing pneumonia (AFOP):
- 42 year old woman with AFOP in whole lobes (Indian J Crit Care Med 2016;20:245)
- 45 year old man with flu-like symptoms (Ann Saudi Med 2013;33:301)
- 46 year old man with rapidly progressive respiratory failure (Curr Probl Diagn Radiol 2015;44:469)
- 68 year old woman with AFOP mimicking pneumonia (BMC Res Notes 2015;8:38)
- 22 year old man who presented with AFOP after lung transplantation and underwent retransplantation (Transplant Proc 2015;47:182)
- 39 year old woman with AFOP associated with undifferentiated connective tissue disease (Case Rep Rheumatol 2012;2012:549298)
- 48 year old woman with AFOP after lung transplantation and good response to corticosteroid pulse therapy (Transplant Proc 2015;47:836)
- 62 year old man with AFOP associated with myelodysplastic syndrome (Intern Med 2016;55:3155)
- 66 year old woman died of AFOP associated with influenza A / H1N1 after lung transplantation (BMC Pulm Med 2013;13:30)
- 68 year old man with AFOP induced by nivolumab (Intern Med 2017;56:2311)
- 78 year old man with AFOP associated with amiodarone (Am J Respir Crit Care Med 2015;191:104)
Treatment
- In general, corticosteroid pulse therapy with / without cyclophosphamide improves the symptoms and prognosis (Arch Pathol Lab Med 2002;126:1064, J Clin Pathol 2015;68:441, Chin Med J (Engl) 2015;128:2701)
- Treatment for underlying cause is also important for secondary acute fibrinous and organizing pneumonia
- Antibiotics are effective for acute fibrinous and organizing pneumonia induced by bacterial infection
- It is questionable if antibiotics can be a general therapeutic choice or not
- Mechanical ventilation may be necessary for aggressive type
Gross description
- Multiple patchy consolidated lesions
- Ill defined, soft to firm gray areas
- Mild increase in weight
- Alveoli are filled with reddish fibrinous exudates
Microscopic (histologic) description
- Major findings
- Dominant findings of intra-alveolar fibrin, so called "fibrin ball"
- Involves more than 20% of the alveolar spaces in the lesion
- Neutrophils are usually scanty or absent
- Organizing pneumonia: fibroblastic plugs in alveolar sacs and ducts with loose collagen matrix
- Diffuse and patchy distribution
- Dominant findings of intra-alveolar fibrin, so called "fibrin ball"
- Minor findings
- Mild to moderate interstitial changes
- Lymphoplasmacytic infiltrate
- Alveolar septal expansion with myxoid connective tissue
- Limited within areas of fibrinous lesion
- Type 2 pneumocyte hyperplasia
- Mild to moderate interstitial changes
- Pertinent negative findings; need to rule out secondary causes and other lung disease if present
- Hyaline membranes
- Eosinophilic inflammation
- Extensive bronchopneumonia or abscess
- Granulomatous inflammation
- Vasculitis including capillaritis
- Areas of necrosis
- Marked dense fibrosis or honeycombing
- See J Clin Pathol 2015;68:441
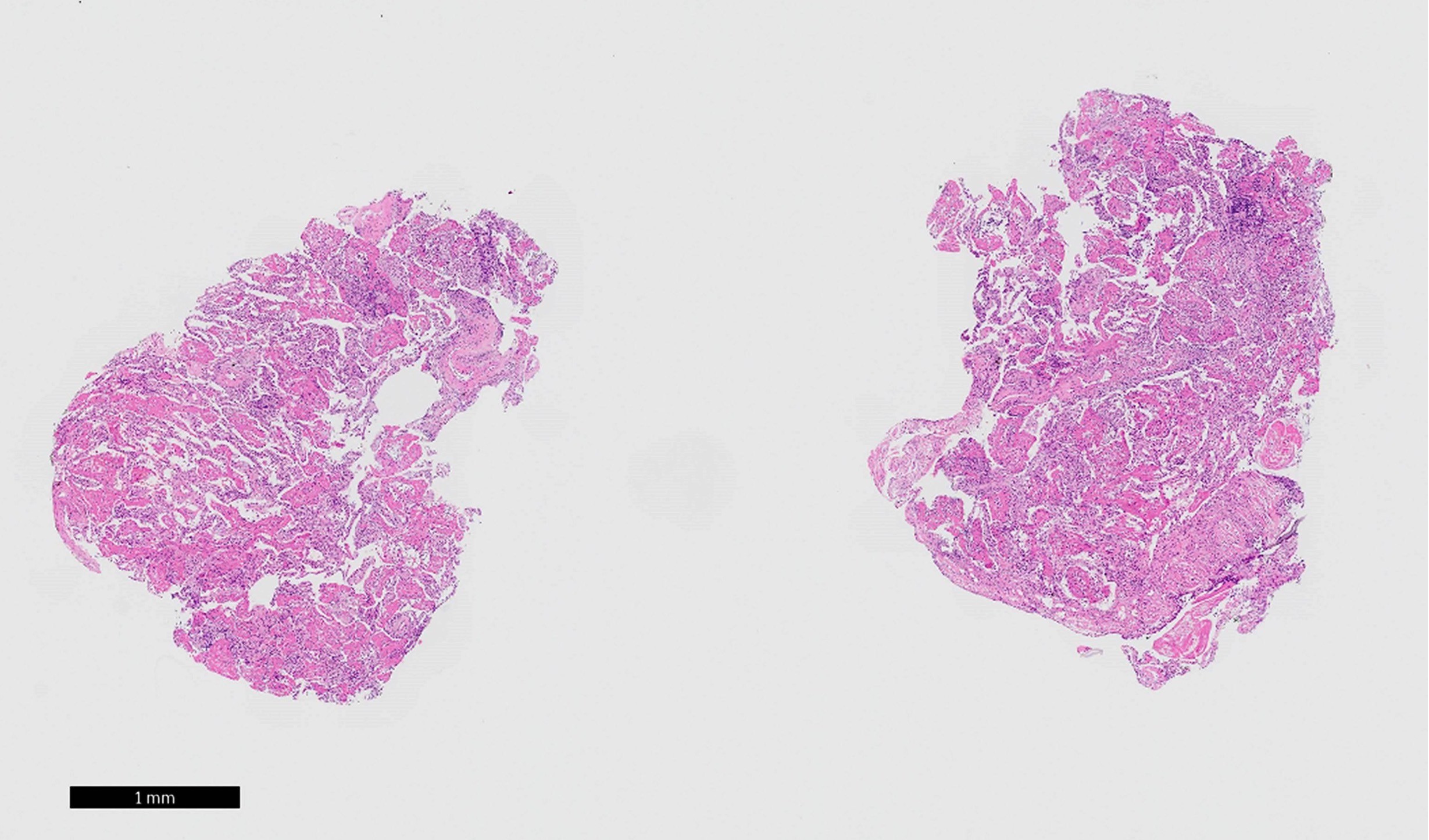
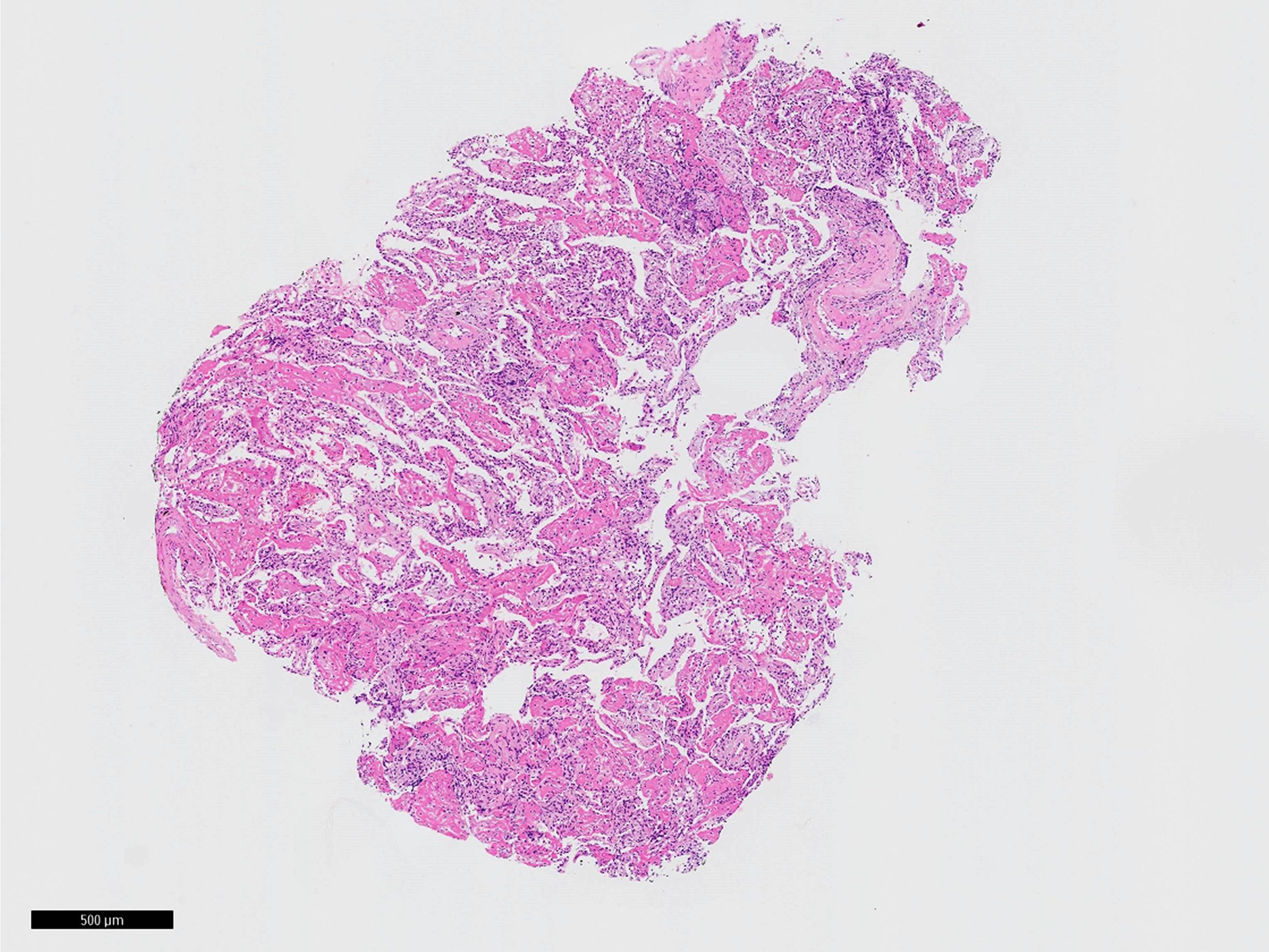
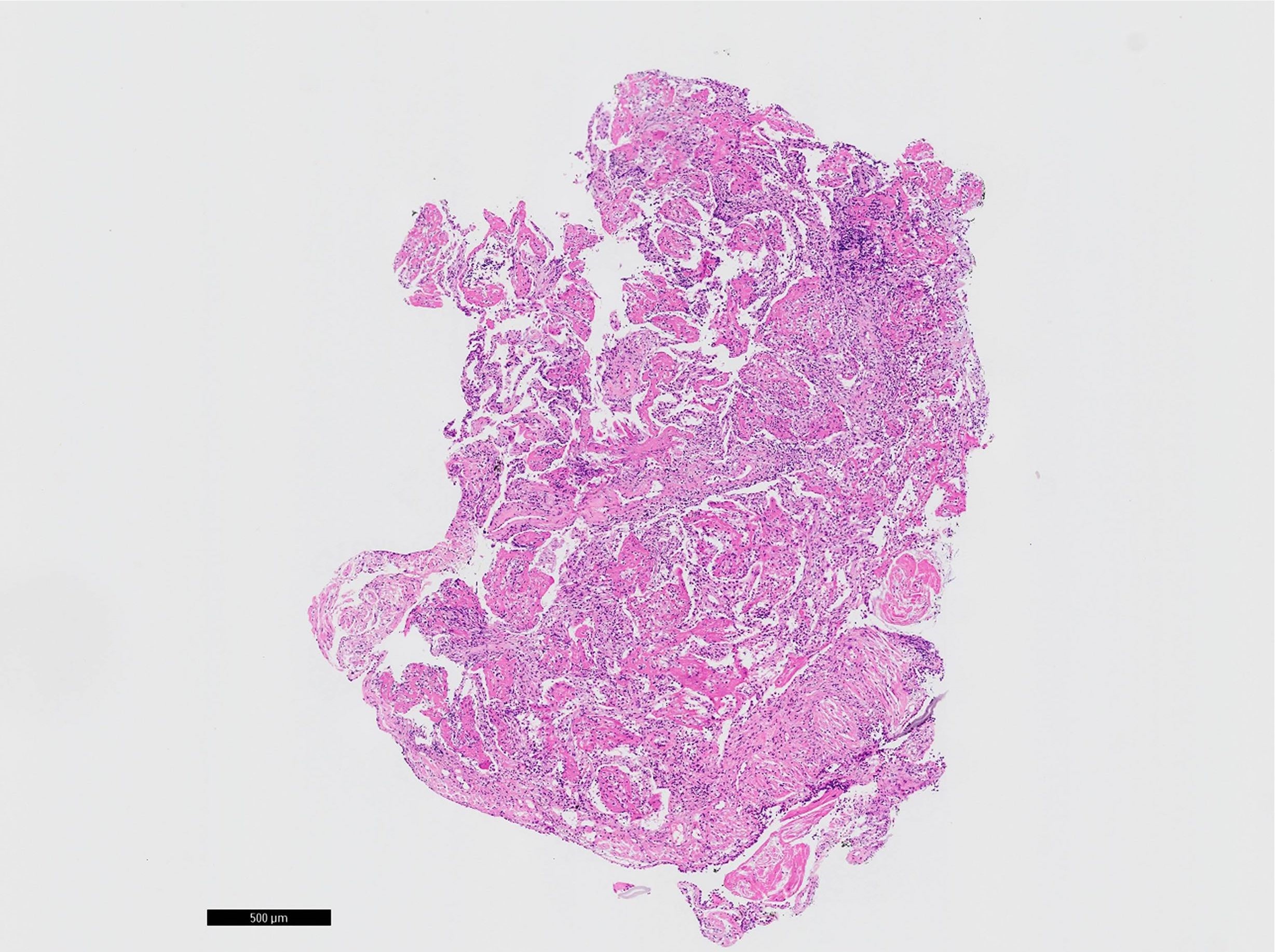
Microscopic (histologic) images
Contributed by Akira Yoshikawa, M.D. and Yale Rosen, M.D.
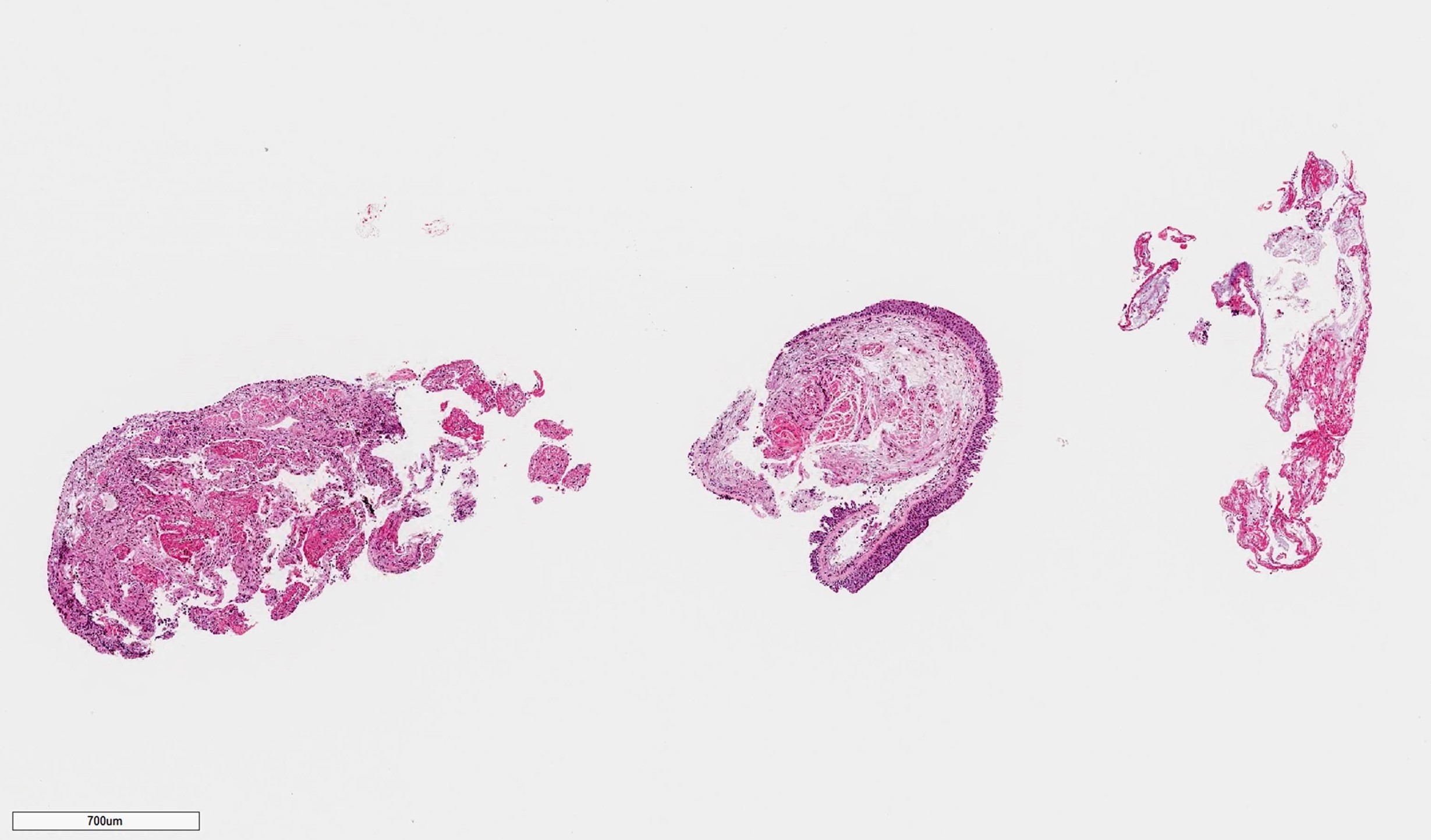
Low power
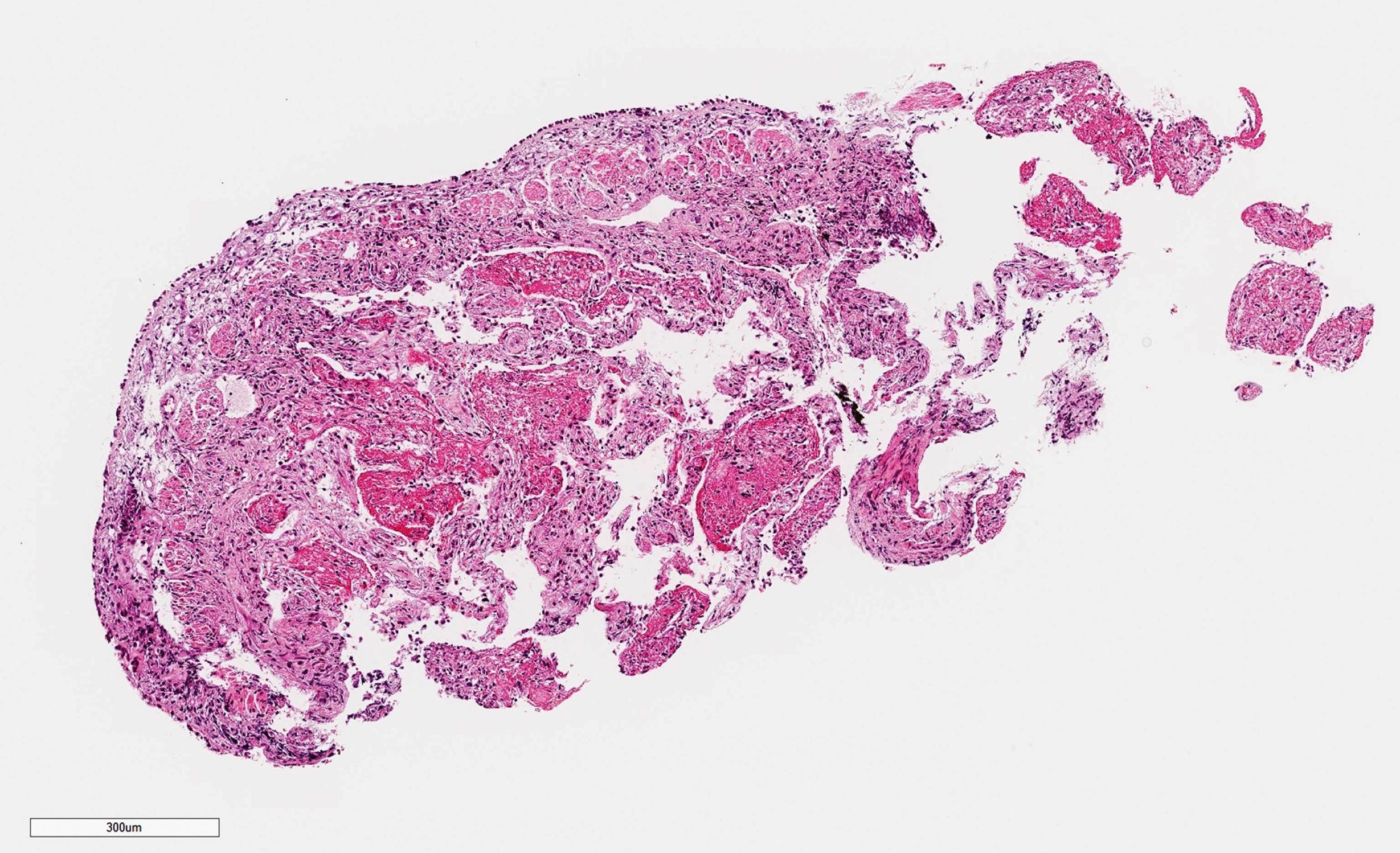
Medium power
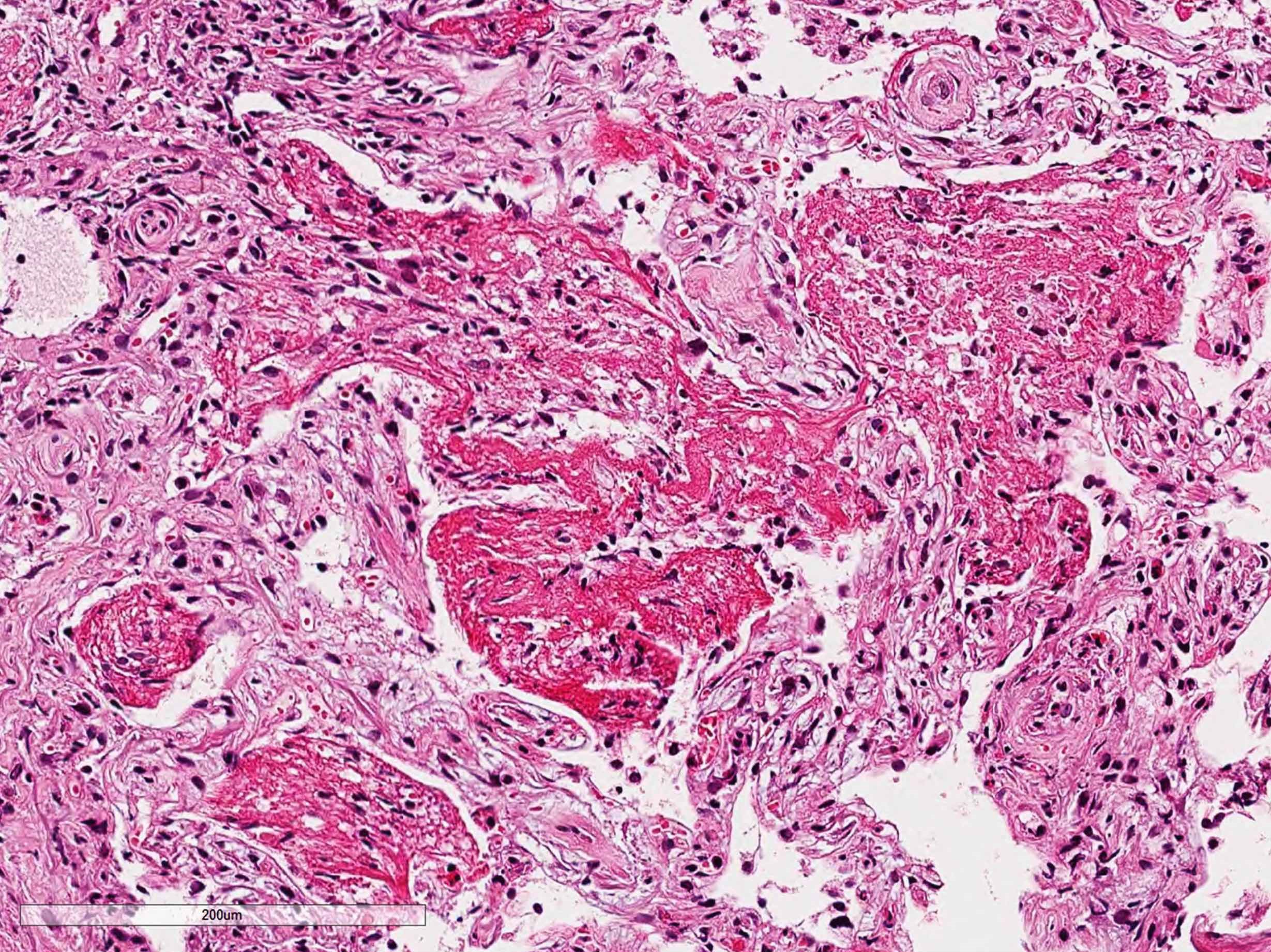
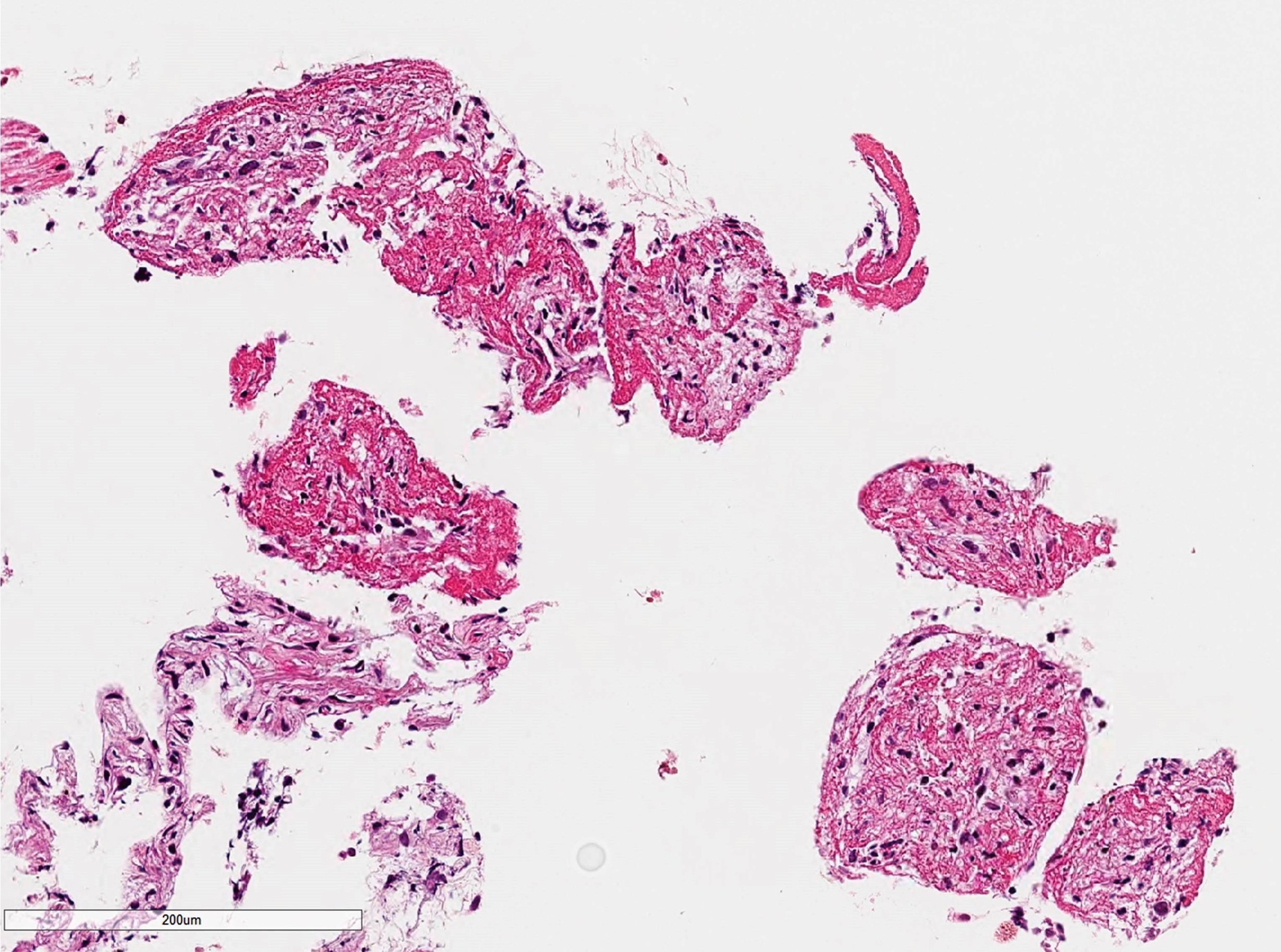
High power
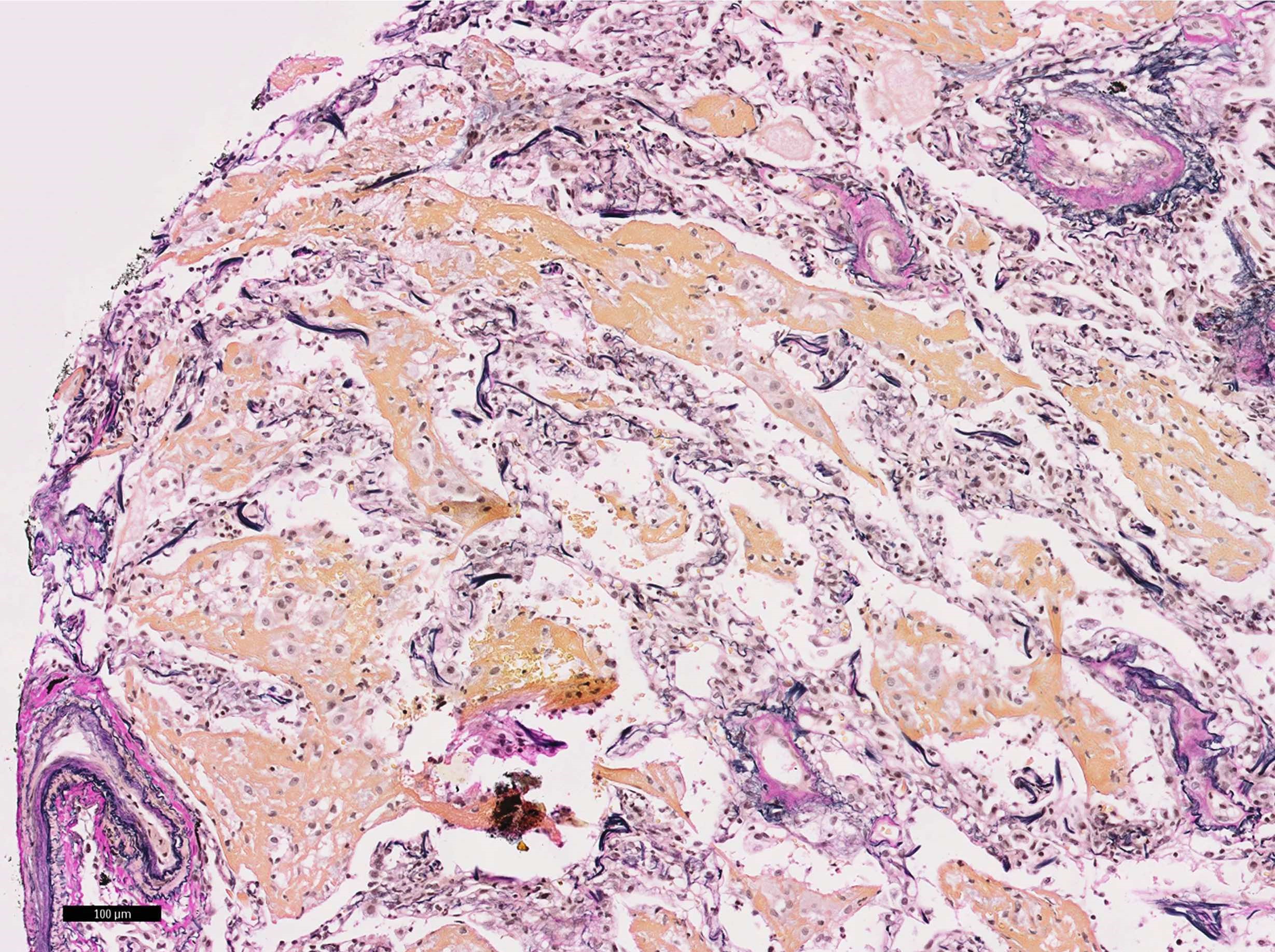
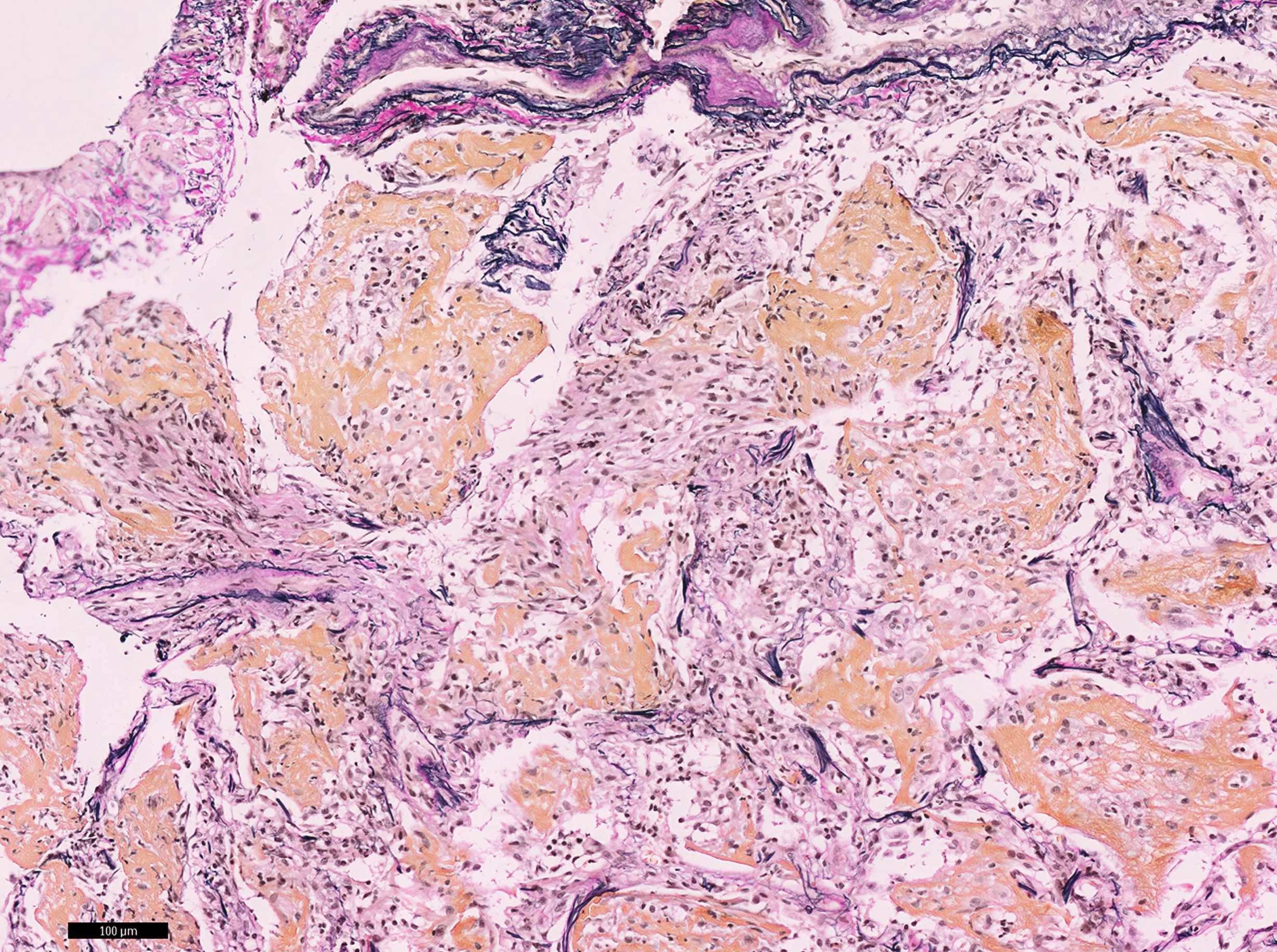
Elastica van Gieson staining
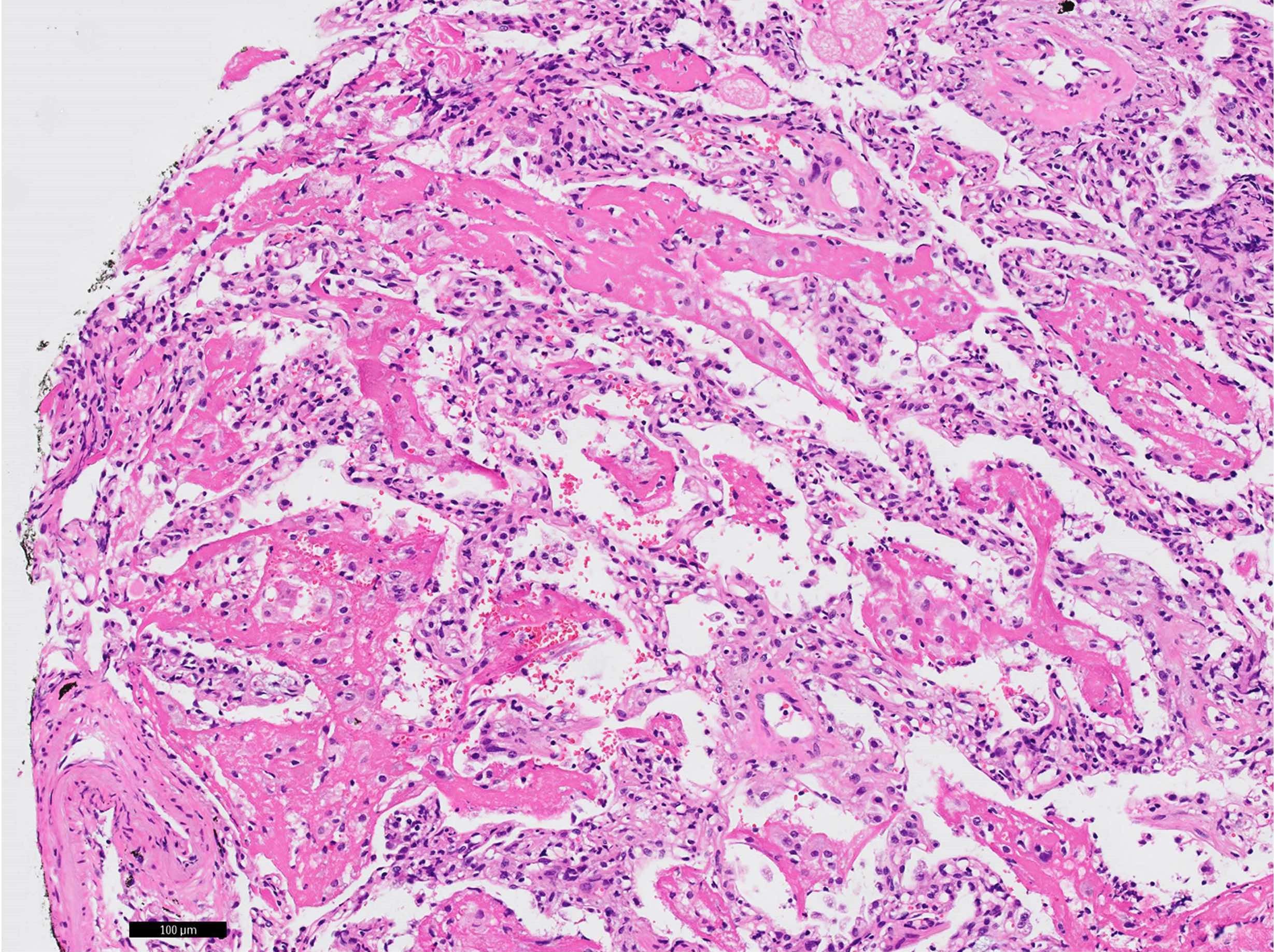
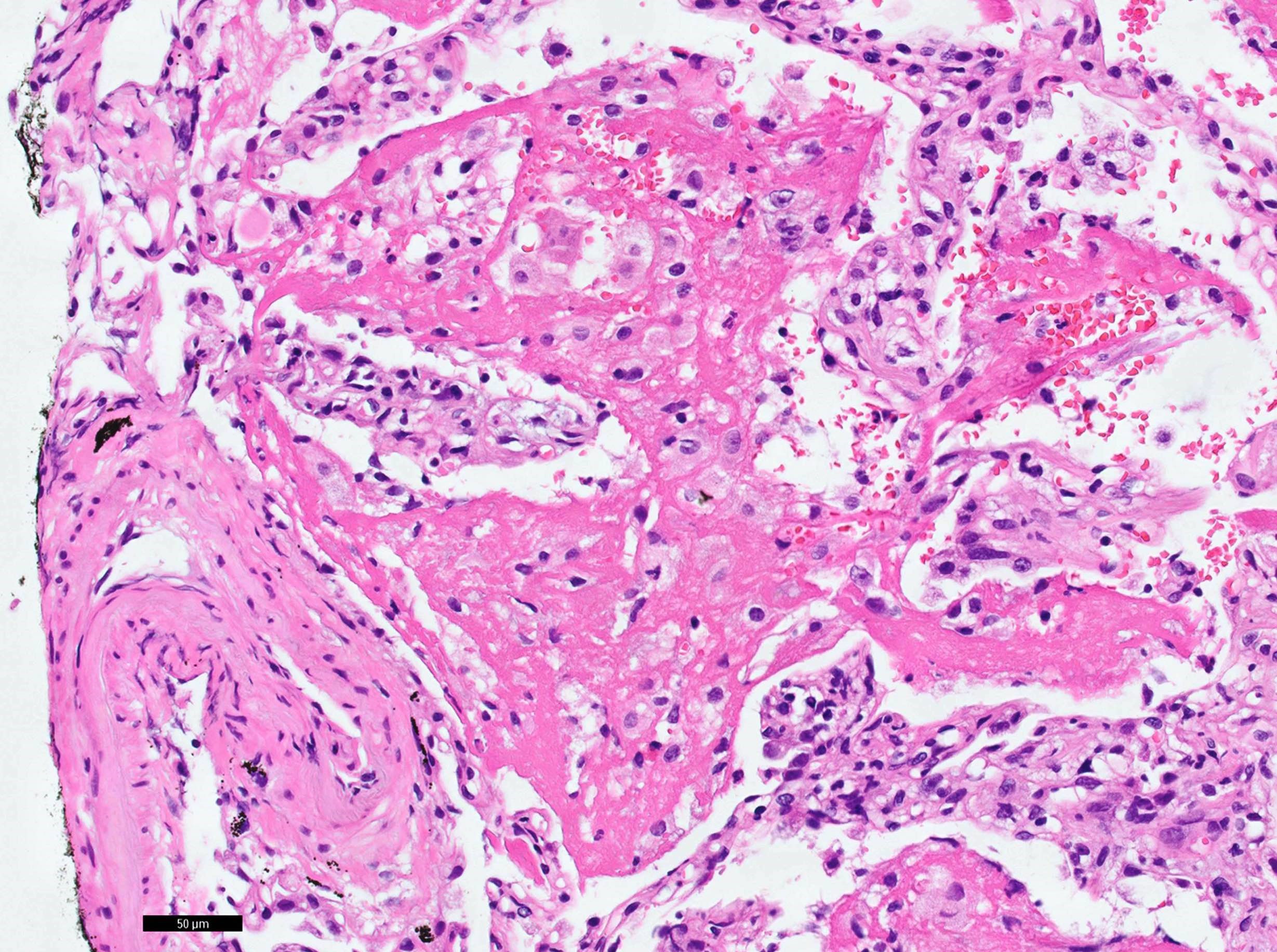
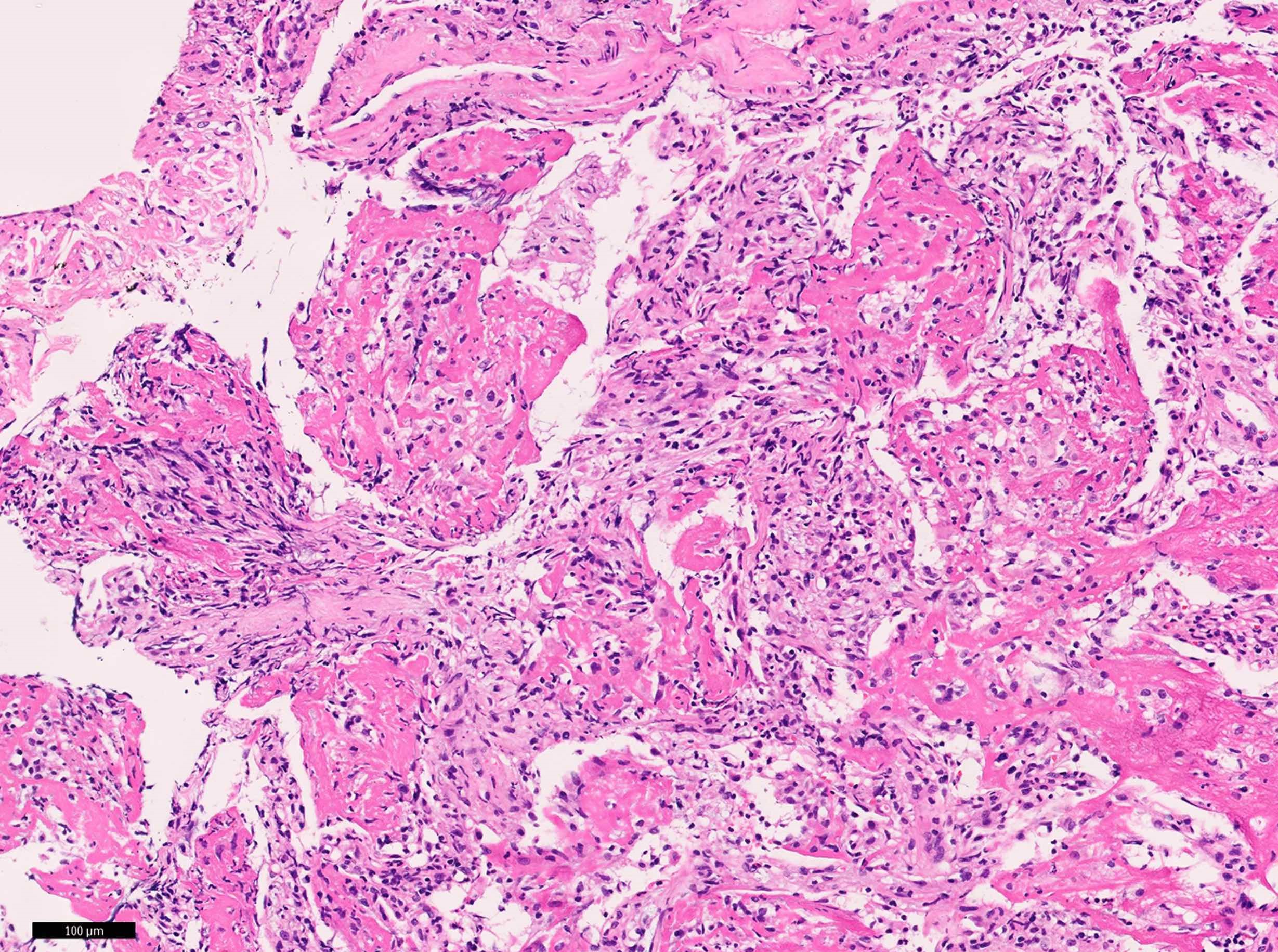
Fibrin balls
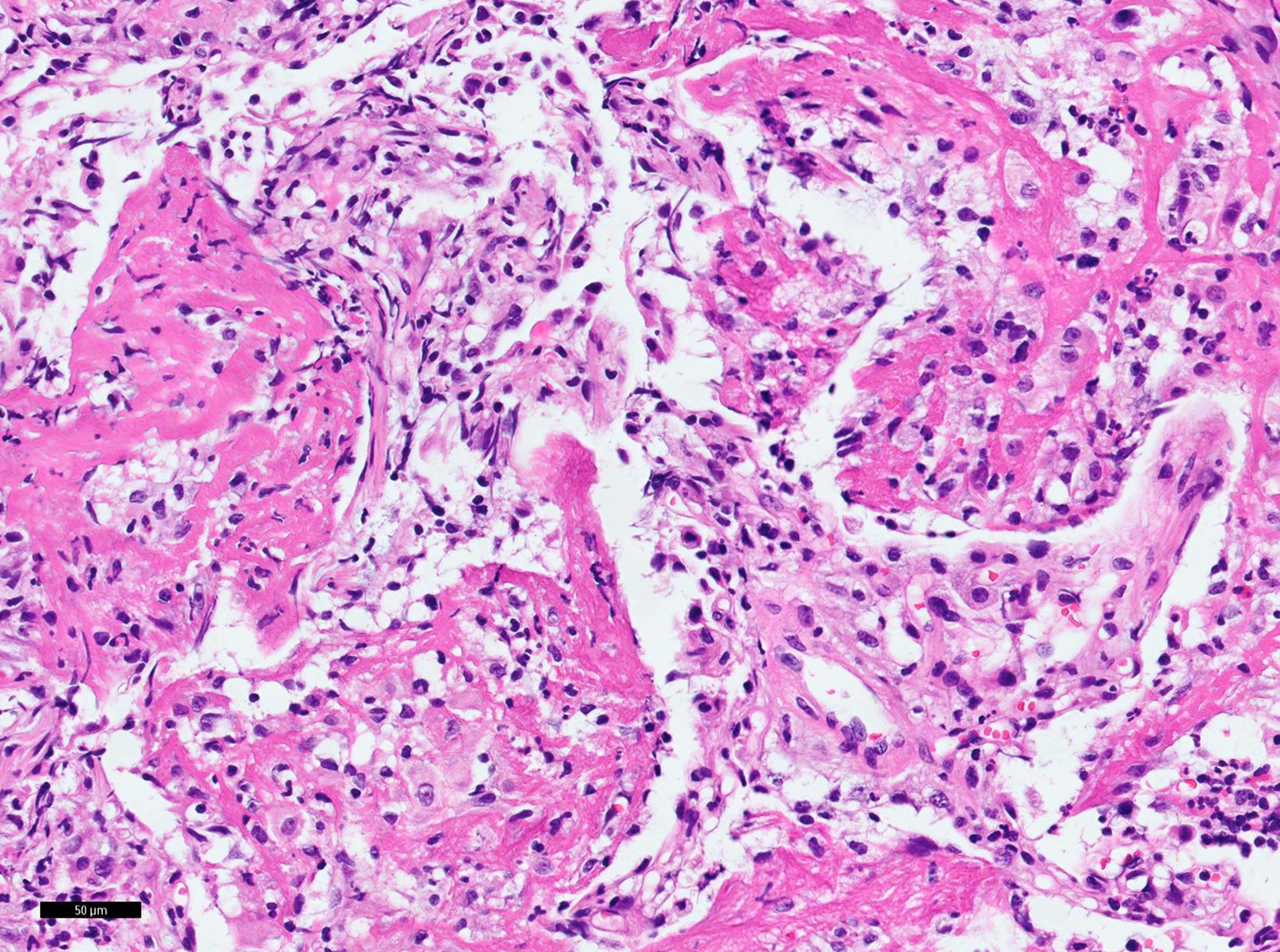
Fibrin balls
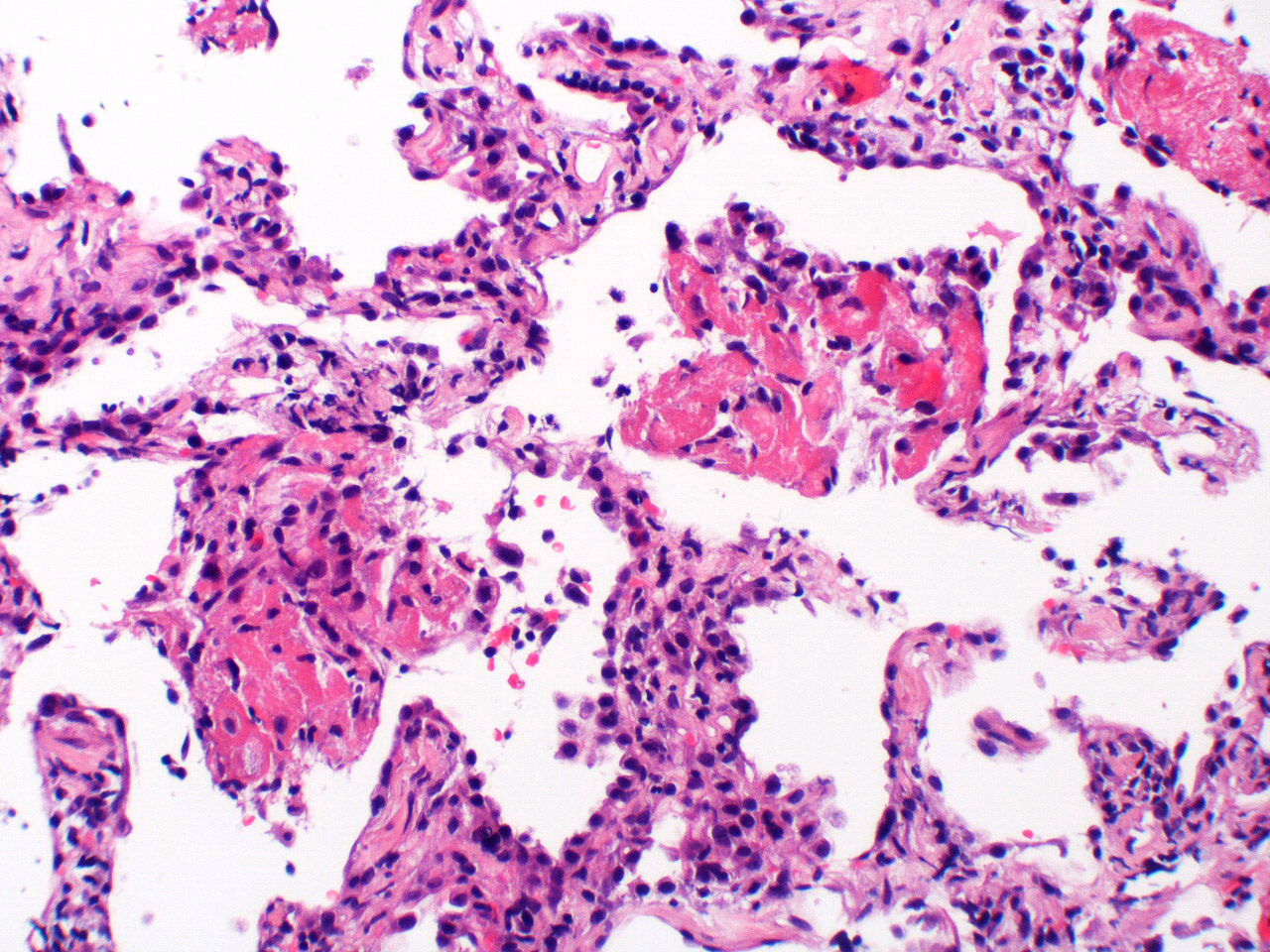
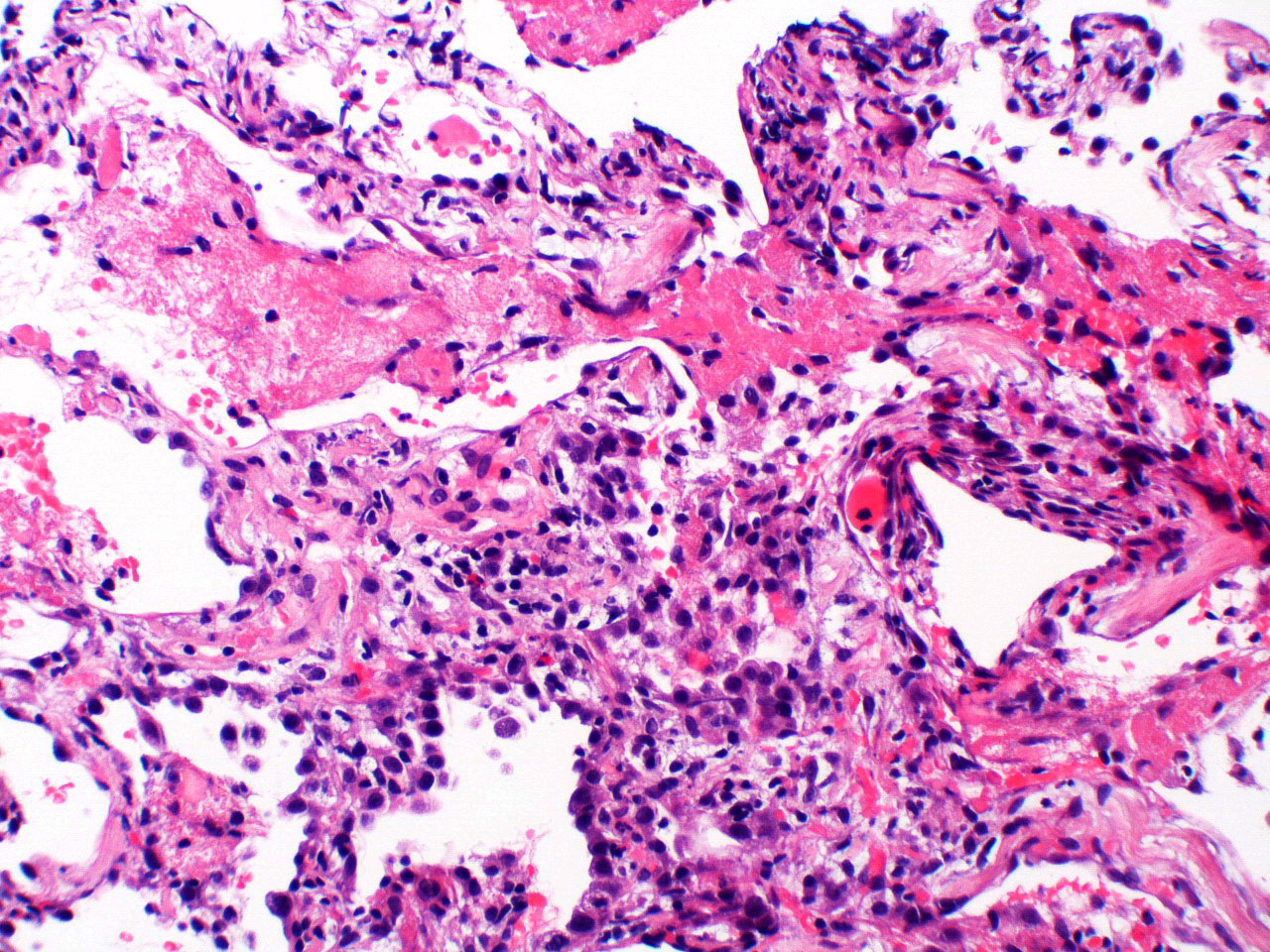
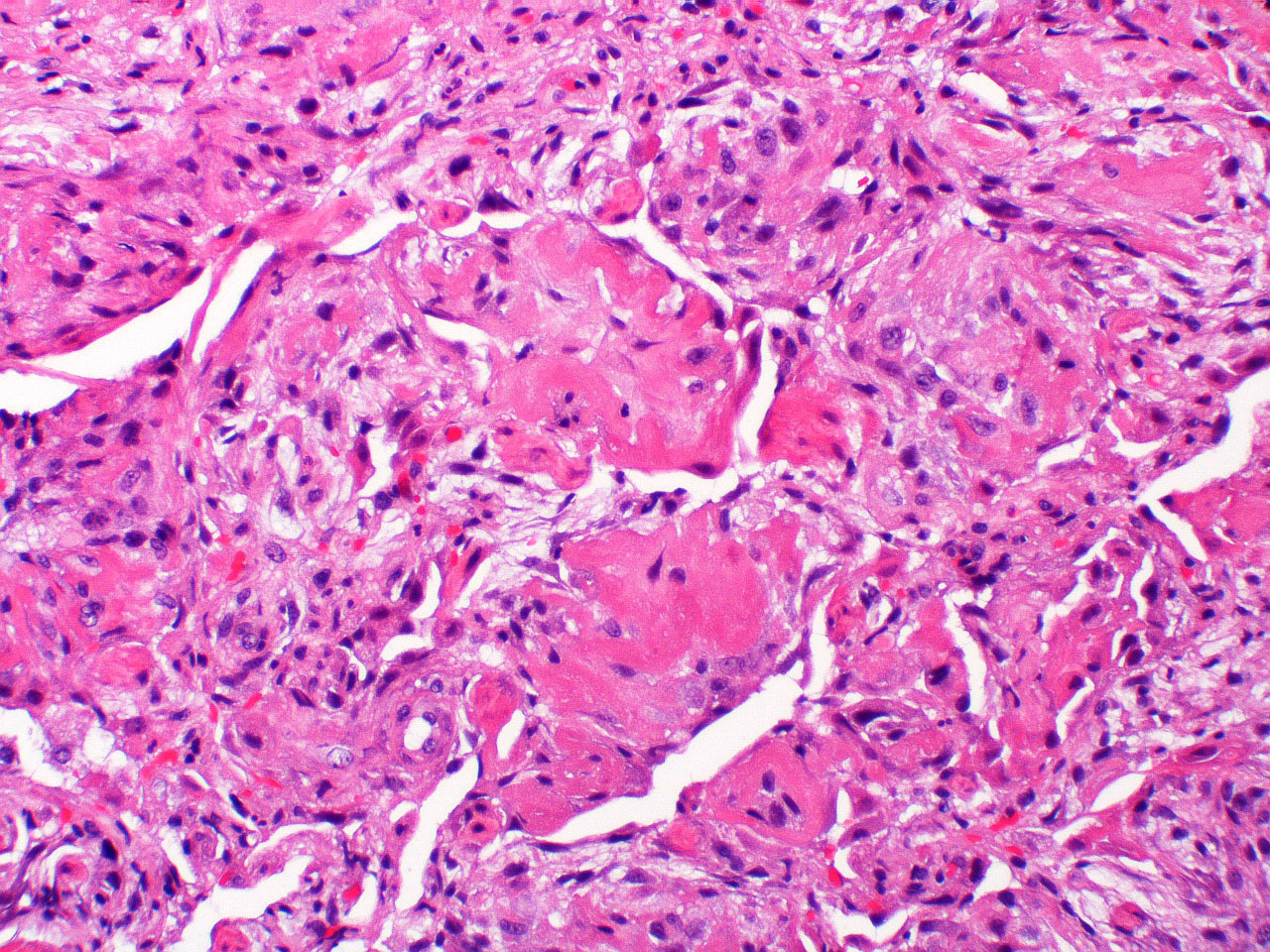
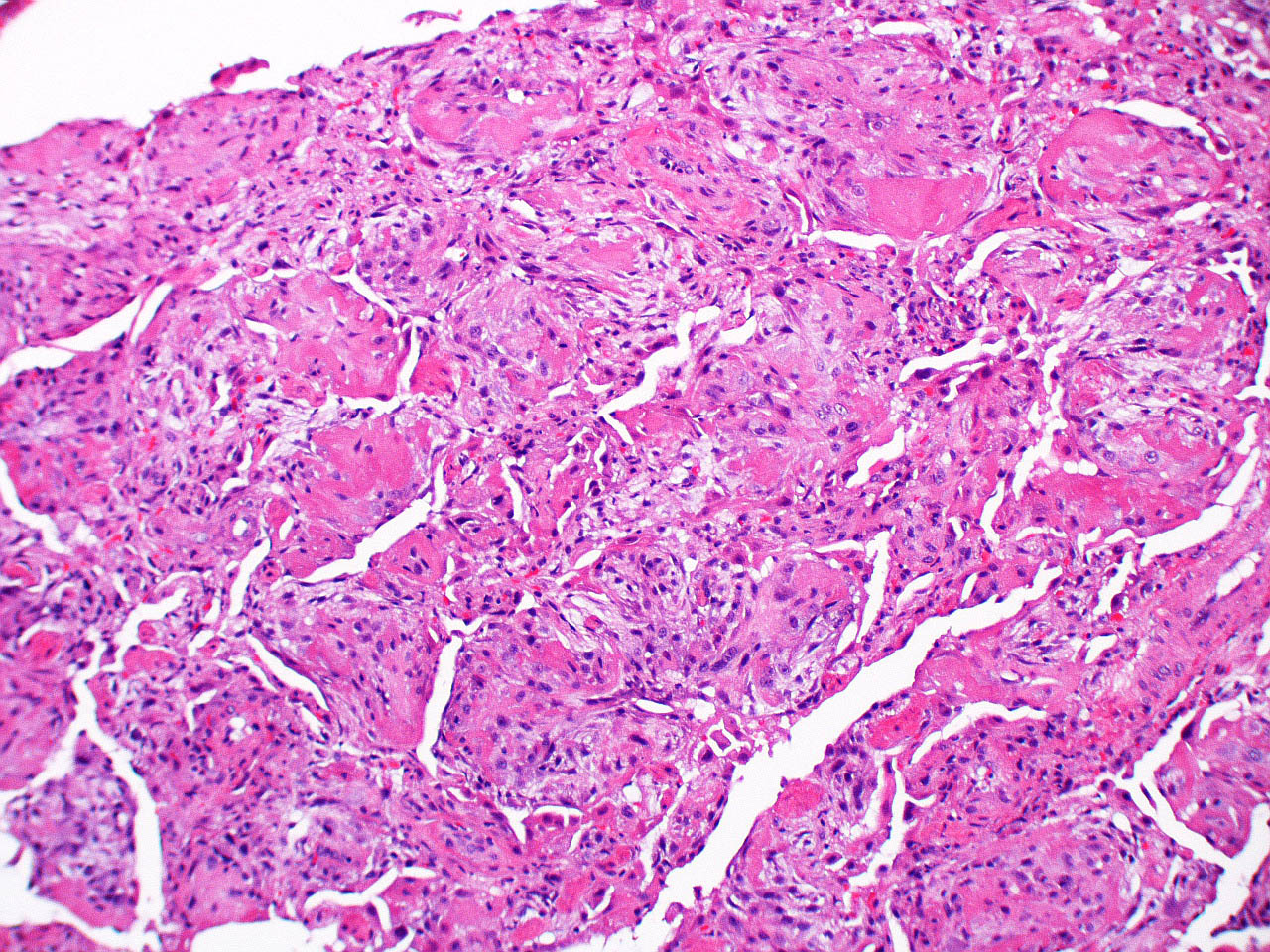
Acute fibrinous and organizing pneumonia
Images hosted on other servers:





Fibrin balls in air spaces


Fibrin balls in air spaces

AFOP
Positive stains
- Elastica van Gieson stains fibrin yellow
- Martius scarlet blue trichrome and picro Mallory staining are positive for fibrin
Negative stains
- Organizing pneumonia foci are free from elastic fiber and collagen fiber, easily confirmed by elastica van Gieson staining
- Giemsa, Grocott and Ziehl-Neelsen stains are usually mandatory to rule out infectious diseases
Differential diagnosis
- Acute exacerbation of chronic lung disease, especially hypersensitivity pneumonitis (Hum Pathol 2012;43:660)
- Cryptogenic organizing pneumonia: scanty or absent fibrin deposition
- Diffuse alveolar damage (acute interstitial pneumonia / acute respiratory distress syndrome): hyaline membranes, architectural destruction and myofibroblastic aggregation
- Eosinophilic pneumonia: prominent eosinophilic infiltrate, pink macrophages (not foamy)
- Granulomatosis with polyangiitis: geographic necrosis, alveolar hemorrhage, capillaritis, granuloma, eosinophils
- Infection: especially, fungal infection is often challenging to differentiate
- Microscopic polyangiitis: small vessel vasculitis and capillaritis with neutrophils, extravasation of neutrophils in alveolar space, alveolar hemorrhage
Additional references
Board review style question #1
Which two of the following findings are against the histological diagnosis of acute fibrinous and organizing pneumonia?
- Eosinophilic infiltration
- Hyaline membranes
- Lymphocytic infiltration
- Organizing pneumonia
- Type 2 pneumocyte hyperplasia
Board review style answer #1
A and B. Eosinophilic infiltration suggests eosinophilic pneumonia. Hyaline membranes suggest diffuse alveolar damage.
Comment Here
Reference: Acute fibrinous and organizing pneumonia
Comment Here
Reference: Acute fibrinous and organizing pneumonia
