

Soft tissue
So called fibrohistiocytic
Plexiform fibrohistiocytic tumor
Author: Vijay Shankar, M.D.

Last author update: 1 August 2012
Last staff update: 27 March 2024 (update in progress)
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Plexiform fibrohistiocytic tumor soft tissue
Table of Contents
Definition / general | Terminology | Epidemiology | Clinical features | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Differential diagnosis | Additional referencesCite this page: Shankar V. Plexiform fibrohistiocytic tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissueplexiformfh.html. Accessed May 18th, 2024.
Definition / general
- Dermal or subcutaneous, plexiform or multinodular proliferation of fibrohistiocytic cells and osteoclast-like giant cells with chronic inflammatory infiltrate
Terminology
- First described in 1988 (Am J Surg Pathol 1988;12:818)
- Also called plexiform fibrous histiocytoma
- May have common histogenesis with cellular neurothekeoma (Am J Surg Pathol 2009;33:905)
Epidemiology
- Usually children and young adults, 80% female
Clinical features
- Small, slow growing dermal or subcutaneous mass, upper extremity (65%) or lower extremity (27%), rarely head and neck (Dermatol Sinica 2010;28:117 (pdf))
Case reports
- 3 year old child whose tumor lacked osteoclast-like giant cells (Am J Dermatopathol 2002;24:399)
- 6 year old boy with small perioral tumor (Eur J Dermatol 2004;14:118)
- 17 year old girl with nasal tumor and nodal metastasis (Dermatol Sinica 2010;28:117)
- 21 year old woman with mass on back (Indian J Pathol Microbiol 2008;51:245)
- 24 year old woman with supraclavicular myxoid tumor without giant cells (Arch Pathol Lab Med 2004;128:931)
- 29 year old woman with occipital mass (Case of the Week #180)
- 39 year old woman with recurrent tumor (Univ Pittsburgh Case #316)
Treatment
- Low grade malignant behavior
- After excision, recurs locally, rarely has nodal or pulmonary metastases (Am J Surg Pathol 1999;23:662)
Gross description
- Multinodular, poorly circumscribed, firm, dermal or subcutaneous, 3 cm or less
Microscopic (histologic) description
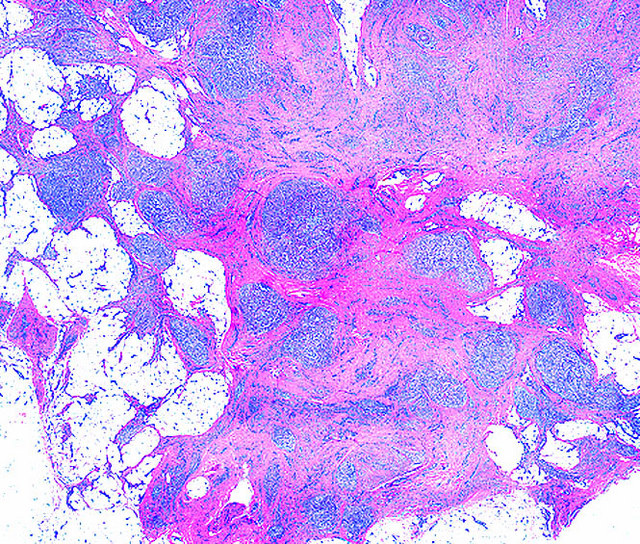
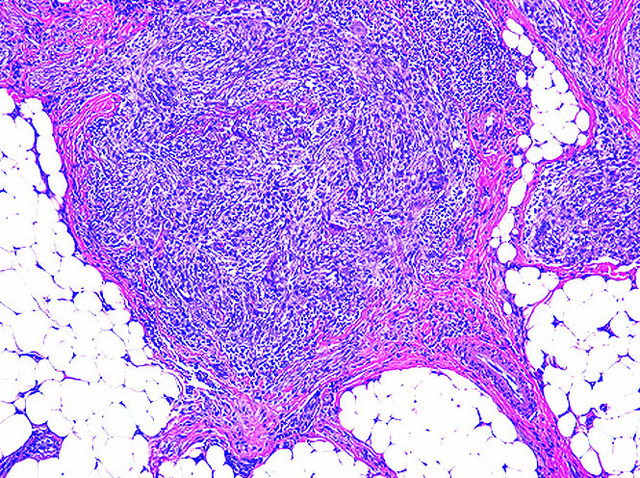
- Deep dermal or subcutaneous tumor with ray like extension into skeletal muscle or adipose tissue
- Overlying epidermis and dermis are usually normal
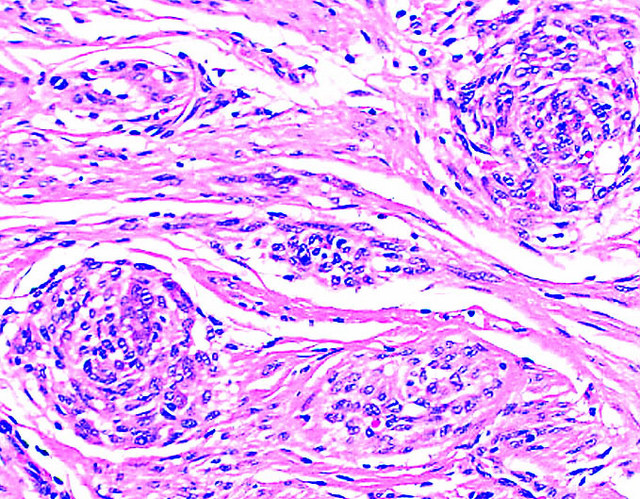
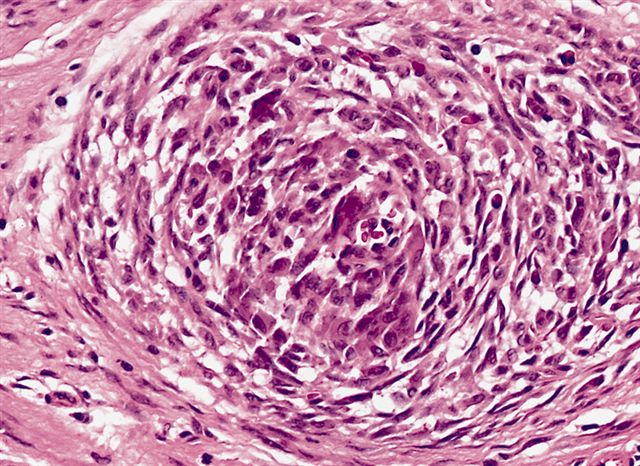
- Plexiform or multinodular proliferation of fibrohistiocytic cells with minimal atypia plus osteoclast-like giant cells and chronic inflammatory infiltrate
- Nodules or clusters are interconnected in characteristic plexiform arrangement
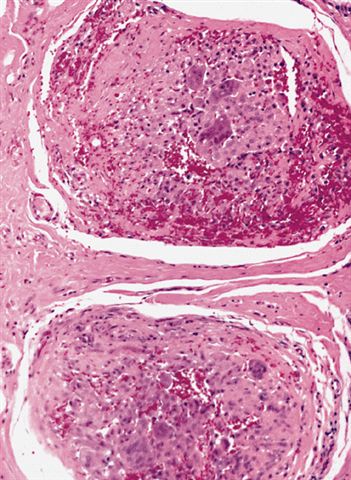
- Prominent dilated vessels; more sclerotic than MFH
- Often hemorrhage and hemosiderin
- Vascular invasion in 10 - 20%
- Usually 0 - 2 MF / 10 HPF, no necrosis
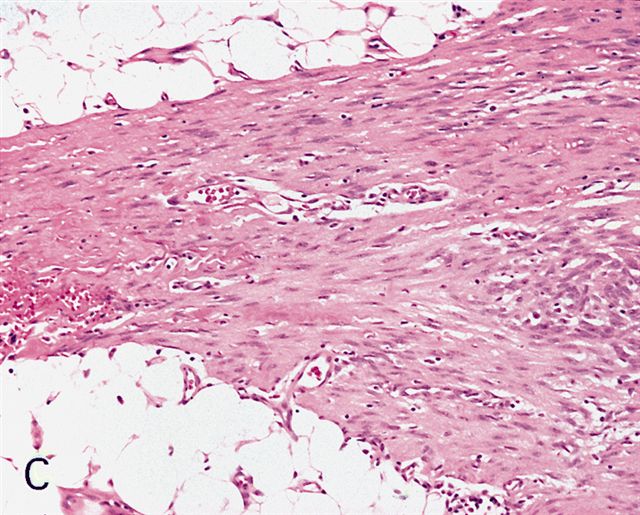
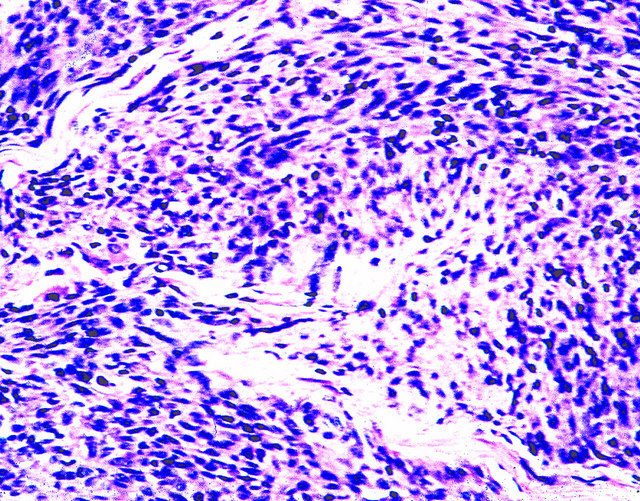
- Subtypes are fibrohistiocytic (histiocyte-like cells and giant cells), fibroblastic (fibroblast-like cells) and mixed
Microscopic (histologic) images
Contributed by David Cohen, M.D. (Case #180), Mark R. Wick, M.D. and AFIP
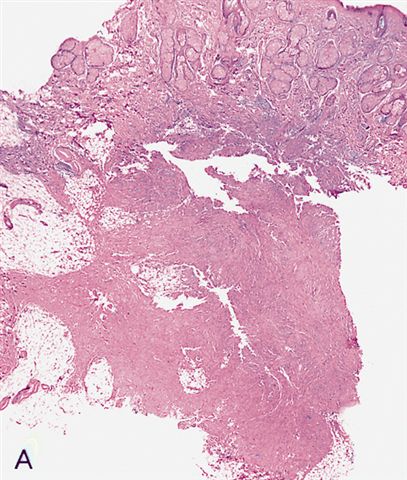
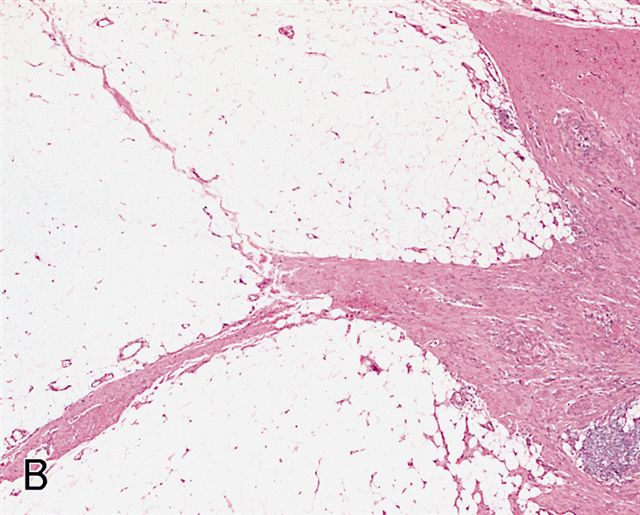
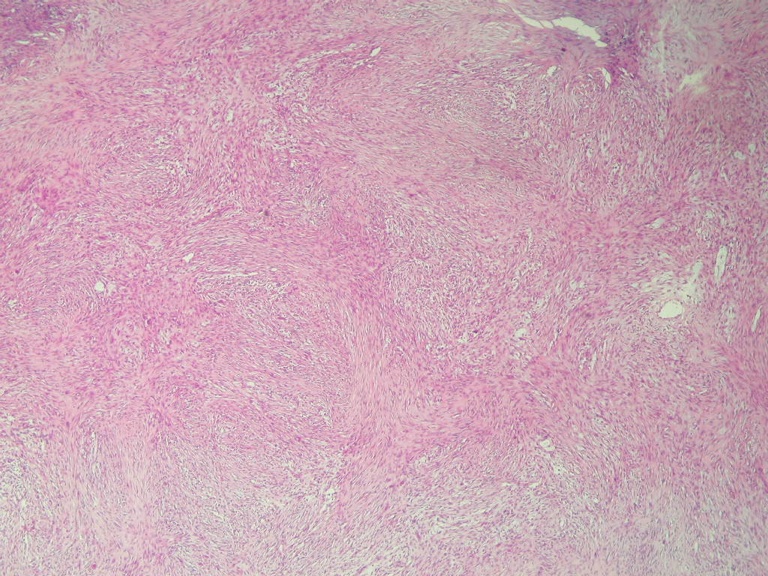
Subcutaneous proliferation of bland fibrous tissue
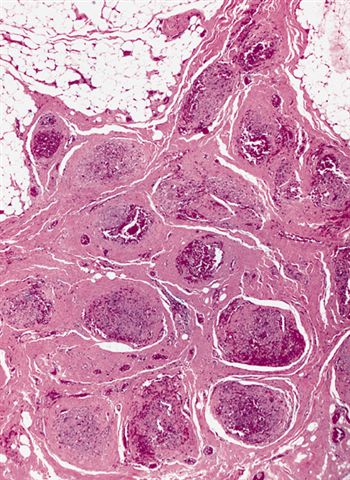
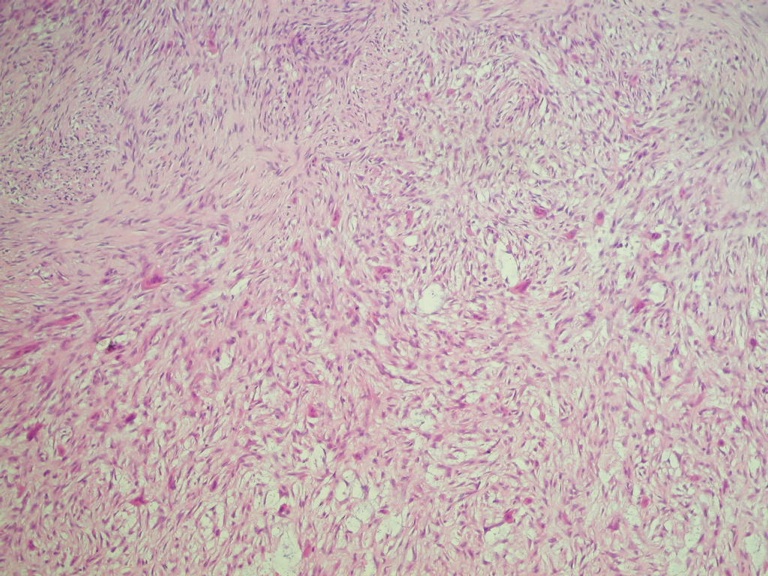
Nodules of histiocyte-like cells
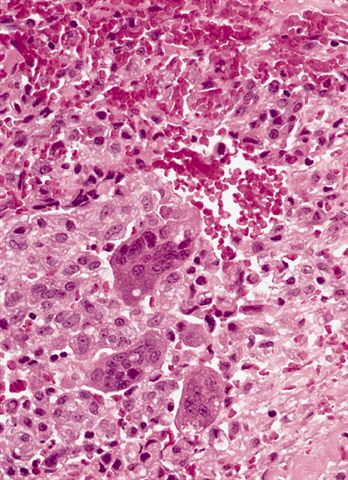
Histiocyte-like cells

Various images
Cells with elongated nuclei
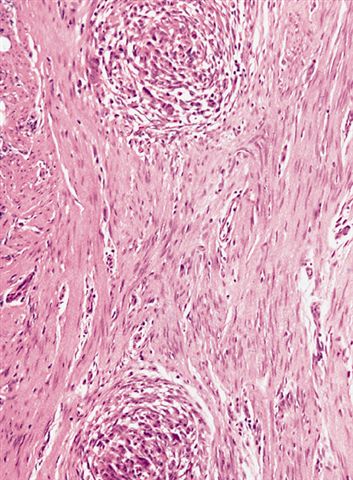
Tumor with nodules and fibrous tissue
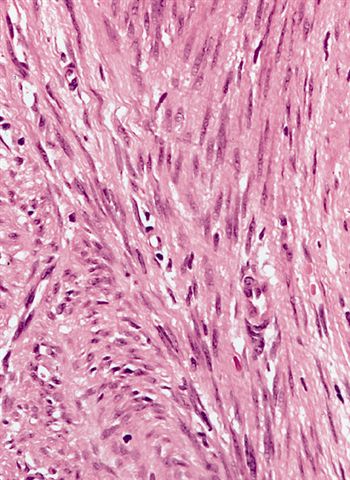
Resemblance to desmoid fibromatosis

Various images




Various images
Images hosted on other servers:


Various images



12 year old girl with upper arm lesion
Cytology description
- Plump fibroblastic cells and histiocyte-like cells within a finely granular myxoid background
- Also osteoclast-like giant cells (Acta Cytol 1999;43:867)
Positive stains
- Vimentin, CD68 (giant cells and mononuclear histiocyte-like cells), smooth muscle actin (fibroblast-like cells, Histopathology 1991;19:503)
- Rarely alpha-1-antitrypsin and alpha-1-antichymotrypsin
Negative stains
- S100, keratin, CD45, Factor VIII, desmin
Electron microscopy description
- Resembles myofibroblasts, fibroblasts and undifferentiated cells
Differential diagnosis
- Benign fibrous histiocytoma:
- Older patients, prominent foam cells, no plexiform extensions of fibrous tissue, no nodules of histiocyte-like cells, no multinucleated giant cells
- Cellular neurothekeoma:
- Uniform population of epithelioid cells, no distinct nodules of histiocytoid cells or osteoclast-like giant cells (Am J Surg Pathol 2007;31:329), podoplanin+ (Am J Dermatopathol 2009;31:137)
- Fibromatosis:
- Centered in muscle, diffusely infiltrative, no nodules
- Fibrous hamartoma of infancy:
- Immature cells present, also myxoid stroma
- Giant cell tumor of soft tissue:
- Infiltrative nodules of mixed giant cells and spindle cells, frequent mitotic figures
- Neurofibroma:
- No distinct nodules, S100+
