Breast
Fibrocystic changes
Adenosis
Author: Julie M. Jorns, M.D.
Editorial Board Member: Gary Tozbikian, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 7 December 2020
Last staff update: 19 February 2025
Copyright 2002-2025, PathologyOutlines.com, Inc.
PubMed Search Adenosis breast pathology [TIAB]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Positive stains | Videos | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Jorns JM. Adenosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastadenosisgeneral.html. Accessed September 15th, 2025.
Definition / general
- Any hyperplastic process (see subtypes below) displaying increase in glands, typically within terminal duct lobular units
- Common, often accompanied by fibrocystic changes
Essential features
- Proliferation of glands, typically lobulocentric (expanding terminal duct lobular unit)
Terminology
- Simple adenosis
- Special subtypes:
- Adenomyoepithelial adenosis
- Apocrine adenosis
- Sclerosing adenosis
- Tubular adenosis (tubular adenoma)
- Nodular adenosis / adenosis tumor
- Blunt duct adenosis (now classified as columnar cell change)
ICD coding
Epidemiology
- Wide age range, highest in third and fourth decades, paralleling fibrocystic changes
- Premenopausal: lesions with predominant epithelial component (proliferation of acini and ducts); nodular adenosis
- Postmenopausal: lesions with more sclerosis (sclerosing adenosis)
Sites
- Terminal duct lobular unit; otherwise, no specific location within the breast
Clinical features
- Considered a part of the spectrum of fibrocystic changes
- Can present as a palpable mass if nodular adenosis / adenosis tumor
Diagnosis
- Histologic examination of tissue with or without immunohistochemistry
Radiology description
- Not visualized on imaging if focal (incidental finding when there is another indication for tissue evaluation)
- Increased mammographic breast density (Breast Cancer Res 2017;19:134)
- Architectural distortion, calcifications and asymmetry may prompt biopsy (Medicine (Baltimore) 2019;98:e17061)
- Mass can be seen with nodular adenosis / adenosis tumor; may mimic invasive carcinoma (Breast Cancer Res Treat 2020;181:127)
Prognostic factors
- With some subtypes (e.g. sclerosing adenosis), the risk of subsequent breast cancer is 1.5 - 2 times higher, as seen with proliferative fibrocystic changes
- 2 times higher risk of breast cancer with increased Ki67 proliferation index in sclerosing adenosis or associated normal background breast tissue (Breast Cancer Res Treat 2015;151:89)
Case reports
- 35 year old woman with heterogeneous echogenicity who underwent excisional biopsy revealing adenomyoepithelial adenosis (Int J Clin Exp Med 2014;7:1166)
- 51 year old woman with nodular adenosis detected an enhancing mass (Radiol Case Rep 2020;15:1211)
- 63 year old woman with adenosis tumor evaluated on cytology with surgical pathology correlation (Diagn Cytopathol 2008;36:496)
Treatment
- Does not require treatment unless there is cytologic atypia (rare)
Gross description
- Variable - may be indistinguishable from surrounding benign breast tissue, ill defined fibrosis or fibrotic mass with relatively well defined borders
- See separate adenosis topics for specific subtypes
Microscopic (histologic) description
- Simple adenosis: proliferation of acini, with 2 layers (inner epithelial and outer myoepithelial), surrounded by basement membrane, without distortion of lobular architecture
- Adenomyoepithelial adenosis: adenosis, with proliferation of glands (2 layers) with prominent myoepithelial cells
- Apocrine adenosis: adenosis, with proliferation of glands (2 layers) with predominant apocrine cytology
- Sclerosing adenosis: adenosis, with proliferation of glands (2 layers) with glandular compression and (mild to marked) distortion due to stromal fibrosis / sclerosis; entrapped secretions frequently become calcified
- Tubular adenosis: adenosis with haphazard proliferation of branching tubules (2 layers)
- Nodular adenosis / adenosis tumor: adenosis that is mass forming
- Cytologic atypia is uncommon
- See also separate topics for specific subtypes
Microscopic (histologic) images
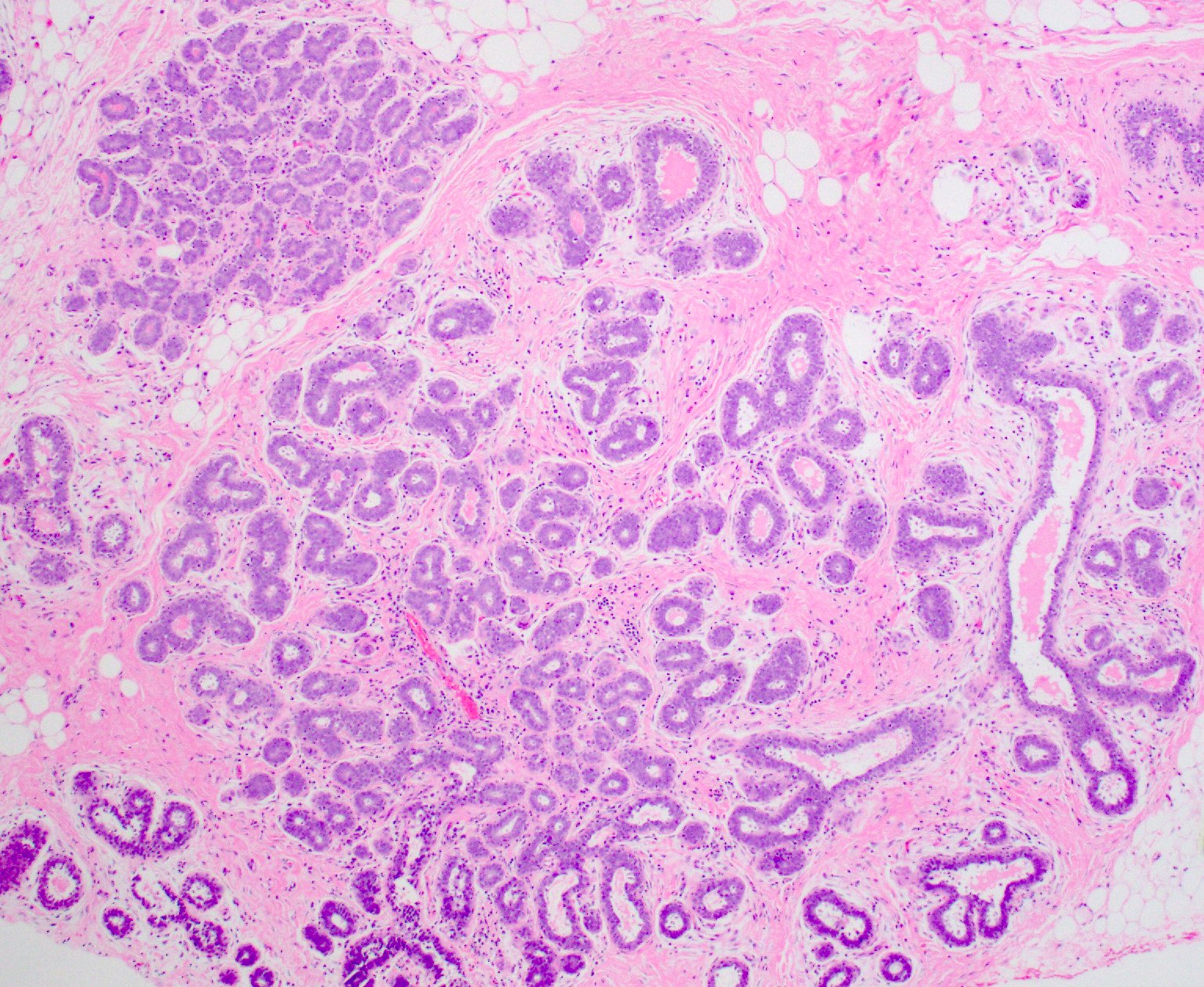
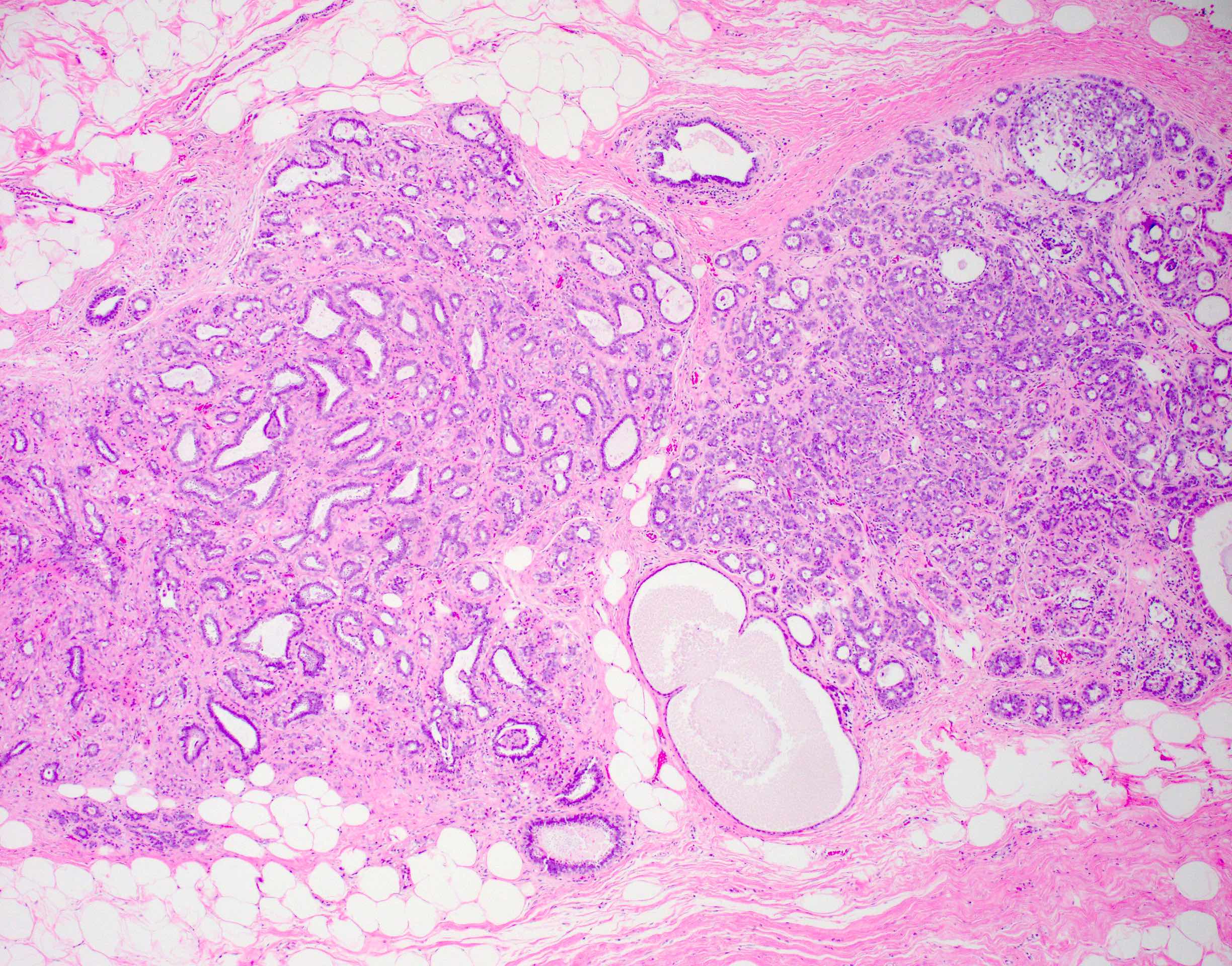
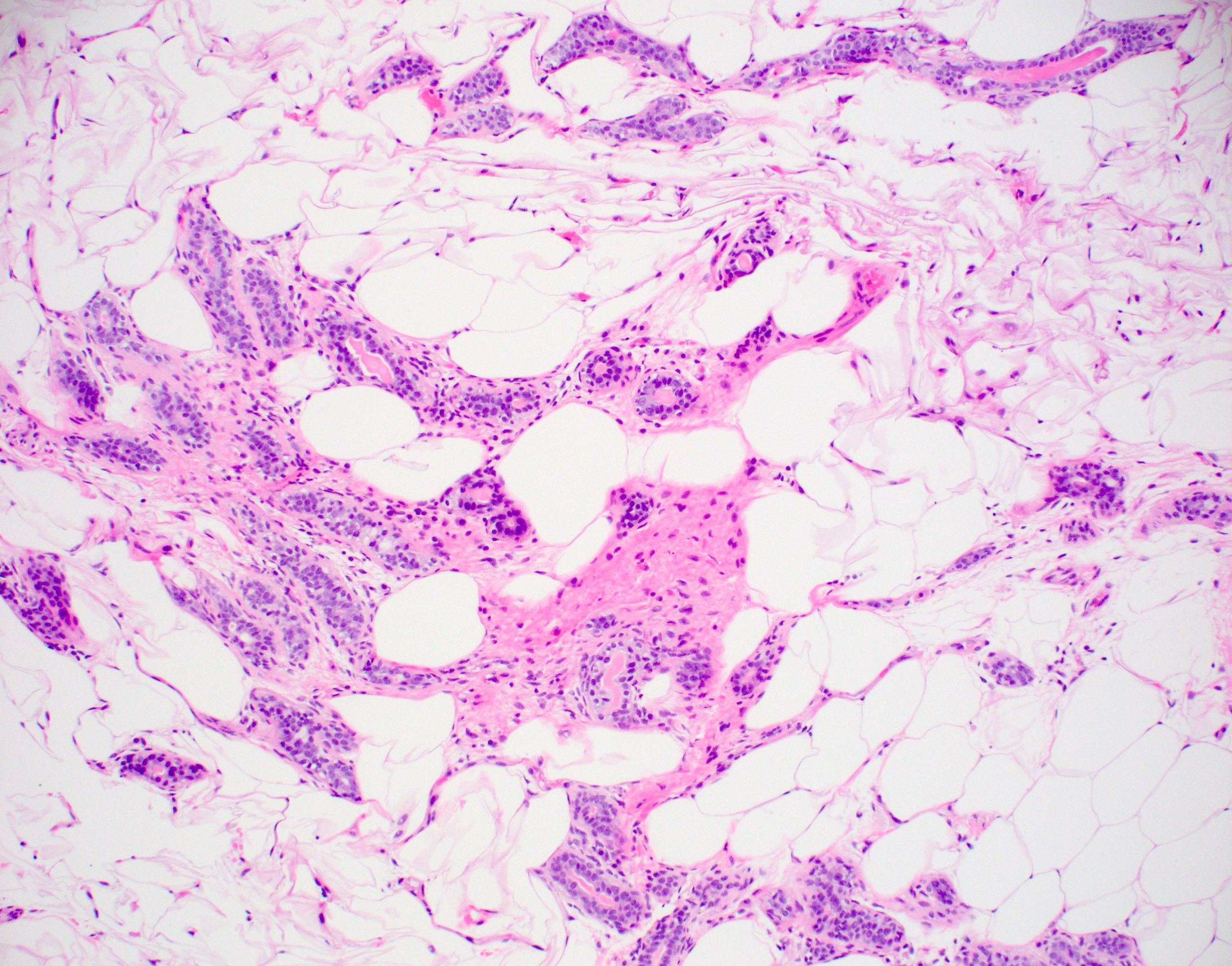
Contributed by Julie M. Jorns, M.D.
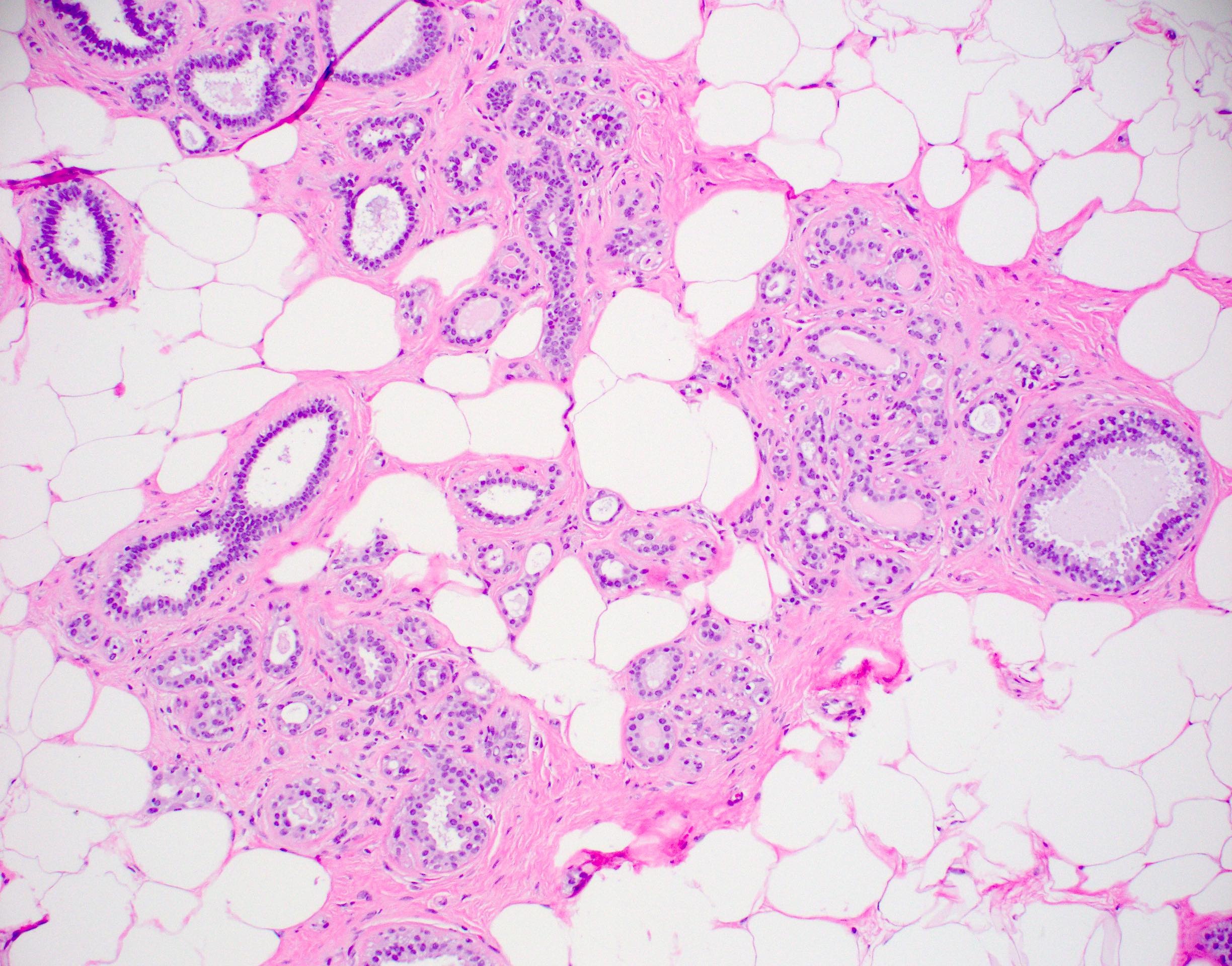
Simple adenosis
Nodular adenosis
Tubular adenosis
Virtual slides
Images hosted on other servers:

Breast, adenosis

Breast, adenosis (myosin / smooth muscle stain)
Cytology description
- Cellular with small groups of benign epithelial cells with variable architecture, including sheets and individual cells and dense hyalinized stroma (Acta Cytol 2001;45:353)
Positive stains
Videos
What is adenosis?
Sample pathology report
- Left breast, core biopsy:
- Nodular adenosis with microcalcifications
Differential diagnosis
Additional references
Practice question #1
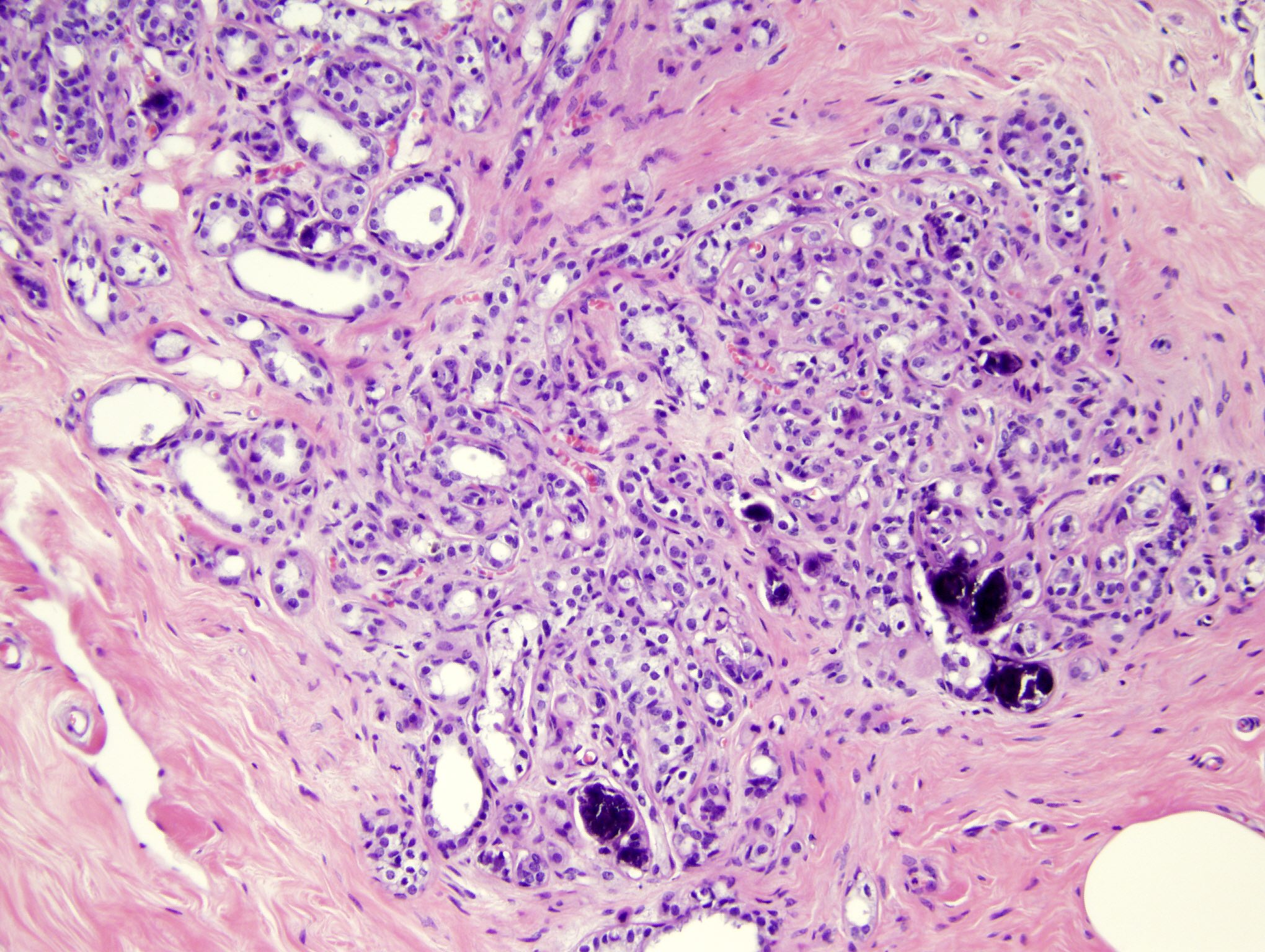
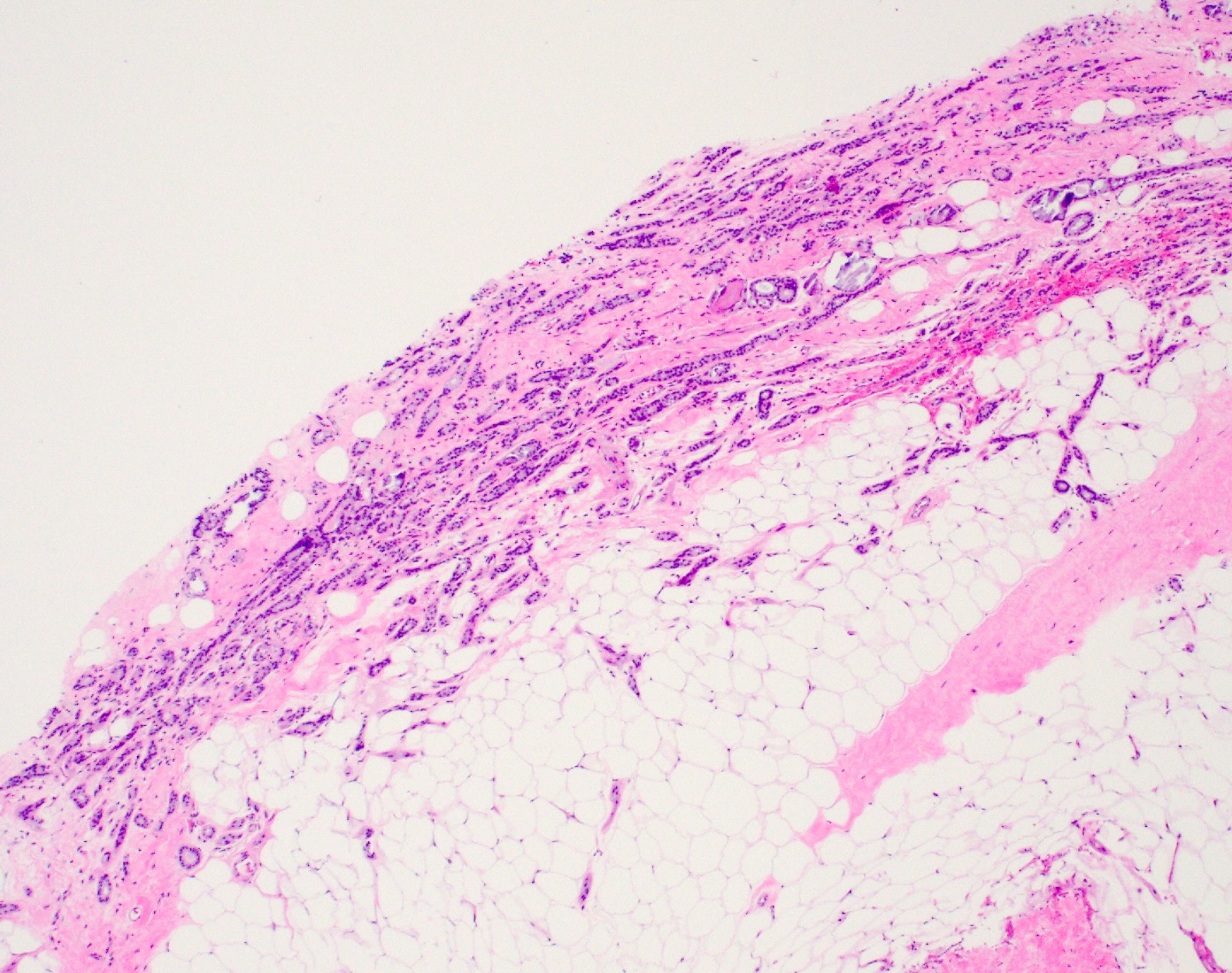
A 48 year old woman had calcifications detected on a screening mammogram, which showed the pictured lesion. What should be done next?
- Biopsy adjacent breast tissue
- Excision of the lesion
- Mammography per routine screening
- Neoadjuvant chemotherapy
- Perform breast MRI
Practice answer #1
C. Mammography per routine screening. The pictured lesion is sclerosing adenosis, which is a benign lobular proliferation with distortion of glands by fibrosis. Microcalcifications (as seen above as dark purple intraluminal material) are frequently seen in sclerosing adenosis and are a result of calcification of entrapped secretions, making this biopsy benign and concordant with imaging findings. Therefore, no treatment or additional imaging is needed outside of routine screening.
Comment Here
Reference: Breast adenosis
Comment Here
Reference: Breast adenosis
Practice question #2
Which of the following is usually true regarding simple adenosis of the breast?
- Clinically palpable
- Displays cytologic atypia
- Involves terminal duct lobular units
- Lacks myoepithelium
- Requires immunohistochemistry for diagnosis
Practice answer #2
C. Involves terminal duct lobular units. Simple adenosis of the breast is a proliferation of glands with normal 2 cell layer (inner epithelial and outer myoepithelial) configuration involving terminal duct lobular units. It rarely harbors atypia and does not show distortion by fibrosis as seen in other forms of adenosis (e.g. sclerosing, tubular), making diagnosis relatively easy via H&E staining alone. It is often incidental or may less frequently show distortion or calcifications on imaging. This contrasts with nodular adenosis / adenosis tumor, which is mass forming and may be clinically palpable.
Comment Here
Reference: Breast adenosis
Comment Here
Reference: Breast adenosis
