Breast
Other invasive carcinoma subtypes, WHO classified
Apocrine
Author: Jonathan Marotti, M.D.
Editorial Board Member: Julie M. Jorns, M.D.
Deputy Editor-in-Chief: Gary Tozbikian, M.D.

Last author update: 6 April 2023
Last staff update: 6 April 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Apocrine carcinoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1Cite this page: Marotti J. Apocrine . PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastmalignantapocrine.html. Accessed August 25th, 2025.
Definition / general
- Invasive breast carcinoma comprised of large cells with abundant eosinophilic and granular cytoplasm, enlarged nuclei and prominent nucleoli
- Apocrine morphology in > 90% of tumor cells
Essential features
- Apocrine morphology in > 90% of tumor cells
- Estrogen receptor (ER) negative, progesterone receptor (PR) negative and androgen receptor (AR) positive
Terminology
- Carcinoma with apocrine differentiation
- Invasive apocrine carcinoma
- Apocrine carcinoma
ICD coding
- ICD-O: 8401/3 - apocrine adenocarcinoma
- ICD-11: 2C61 & XH4GA3 - invasive carcinoma of breast & adenocarcinoma with apocrine metaplasia
Epidemiology
- Rare subtype of invasive breast carcinoma, representing ~1% of invasive carcinomas
- Mean age of diagnosis is typically older than invasive breast carcinoma, NST
Sites
- Breast
- Can occur in axilla
Etiology
- Most carcinomas with apocrine differentiation are sporadic
- Some carcinomas in patients with germline PTEN mutation (Cowden syndrome) display apocrine morphology (Breast Cancer Res 2010;12:R63)
Clinical features
- Similar to those of invasive breast cancer of no special type (NST)
- Typically a firm, poorly circumscribed mass
Diagnosis
- Histologic examination of involved tissue
Radiology description
- Imaging findings are similar to invasive breast cancer of no special type (NST)
Radiology images
Contributed by Jonathan Marotti, M.D.

Mammogram
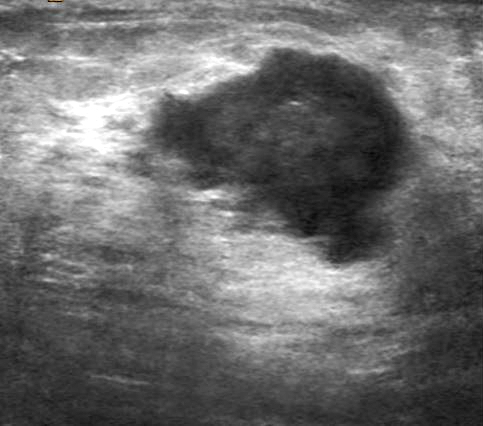
Ultrasound
Prognostic factors
- Prognosis is based on conventional factors such as grade, tumor size and nodal status
- Studies evaluating clinical outcomes have contradictory results (Clin Breast Cancer 2022;22:e576)
Case reports
- 61 year old woman with abnormal screening mammography (Iran J Radiol 2016;13:e35298)
- 70 year old woman with right breast mass (J Cytol 2014;31:96)
- 75 year old woman with axillary lymphadenopathy (Cureus 2021;13:e18523)
Treatment
- Surgical excision
- Chemotherapy and radiation are dependent on stage
- Neoadjuvant therapy may be considered
- Anti-HER2 therapy for HER2+ tumors
- Single agent anti-AR therapy has shown limited therapeutic benefit; clinical trials are ongoing (Clin Breast Cancer 2022;22:e576)
Gross description
Microscopic (histologic) description
- Infiltrating tumor cells with apocrine morphology: abundant eosinophilic and granular cytoplasm, well defined cell borders, enlarged round nuclei and prominent nucleoli
- Apocrine morphology in > 90% of tumor cells
- Typically high grade / poorly differentiated
- Often associated with ductal carcinoma in situ (DCIS) with apocrine features
Microscopic (histologic) images
Contributed by Jonathan Marotti, M.D.

Large atypical epithelial cells
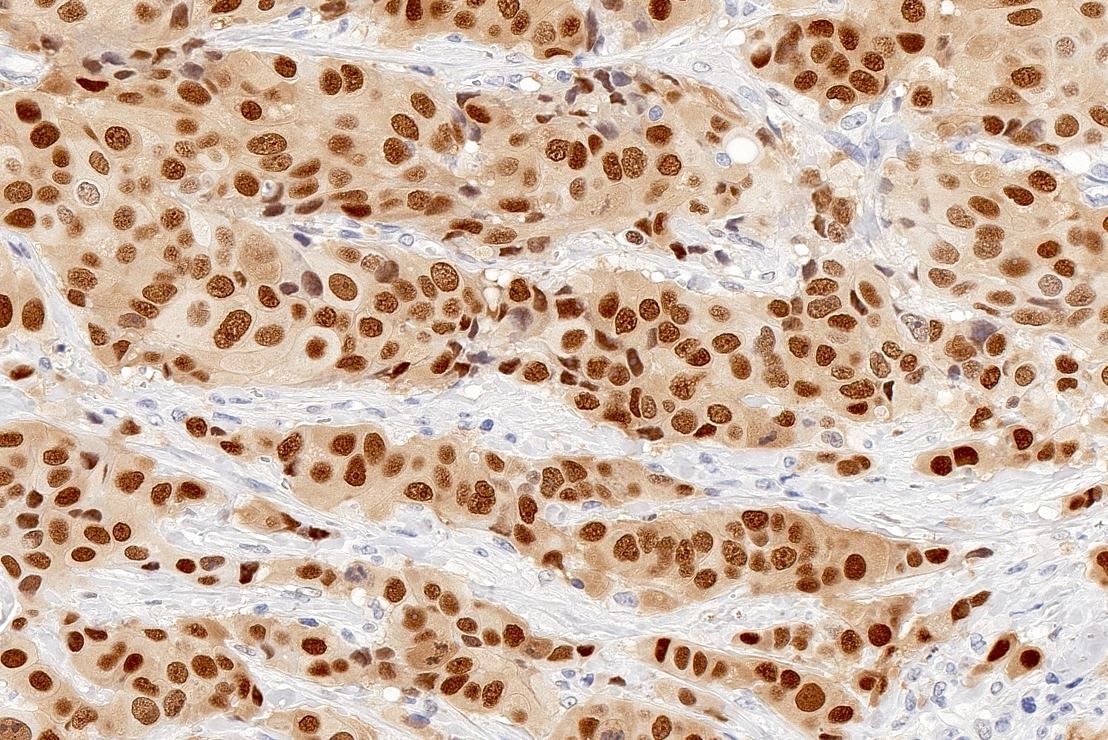
AR positive
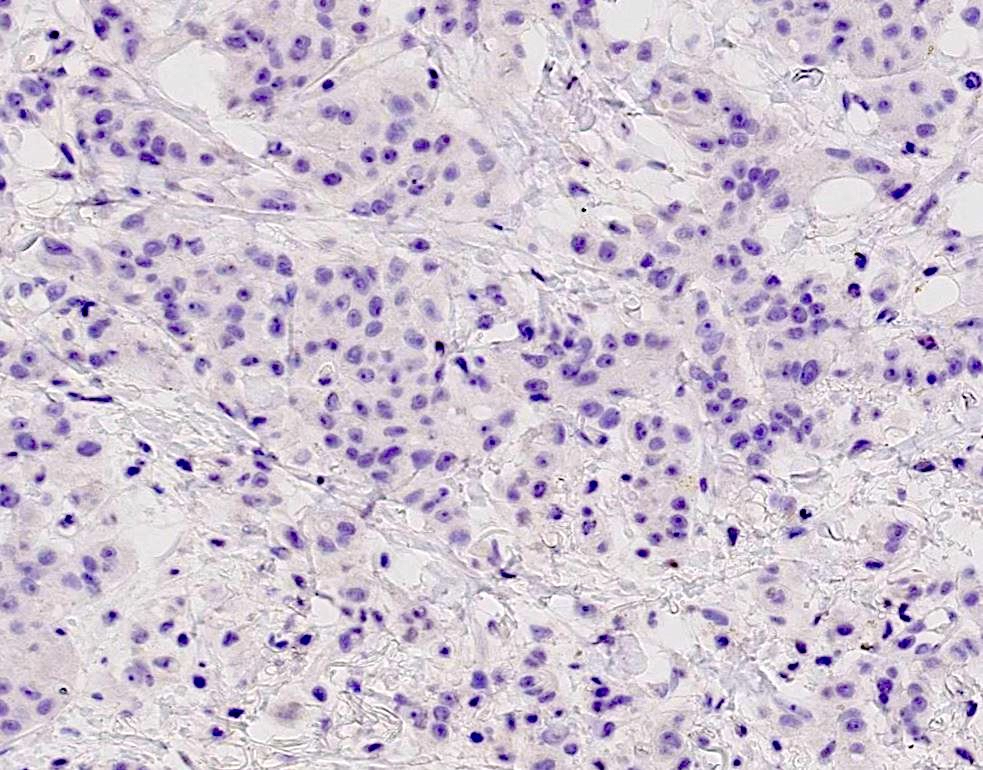
ER negative
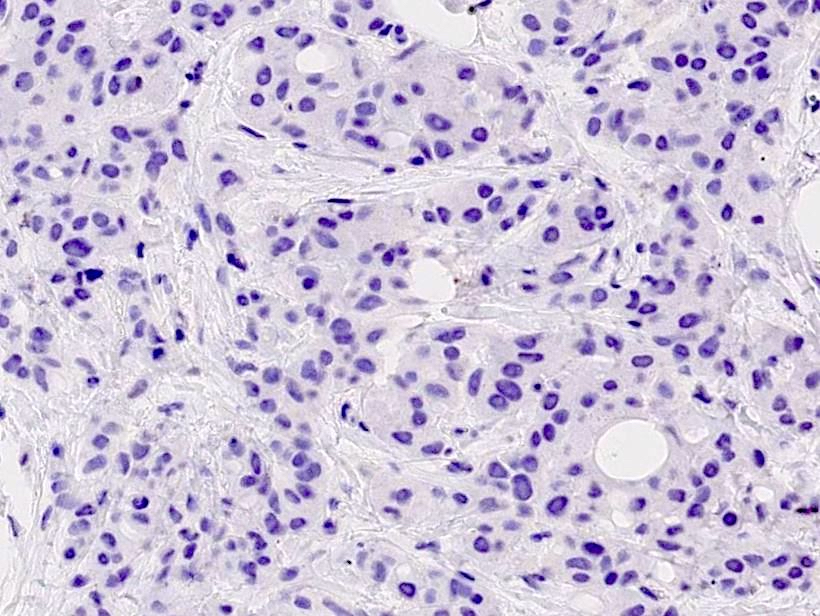
PR negative
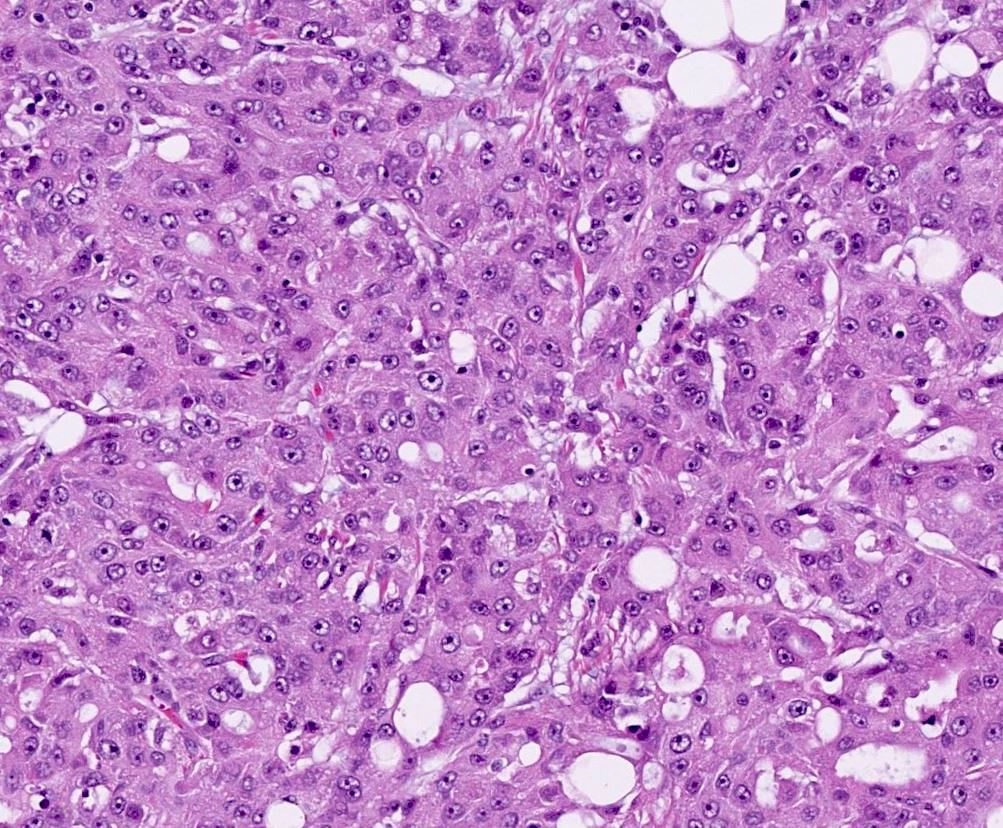
Large atypical epithelial cells
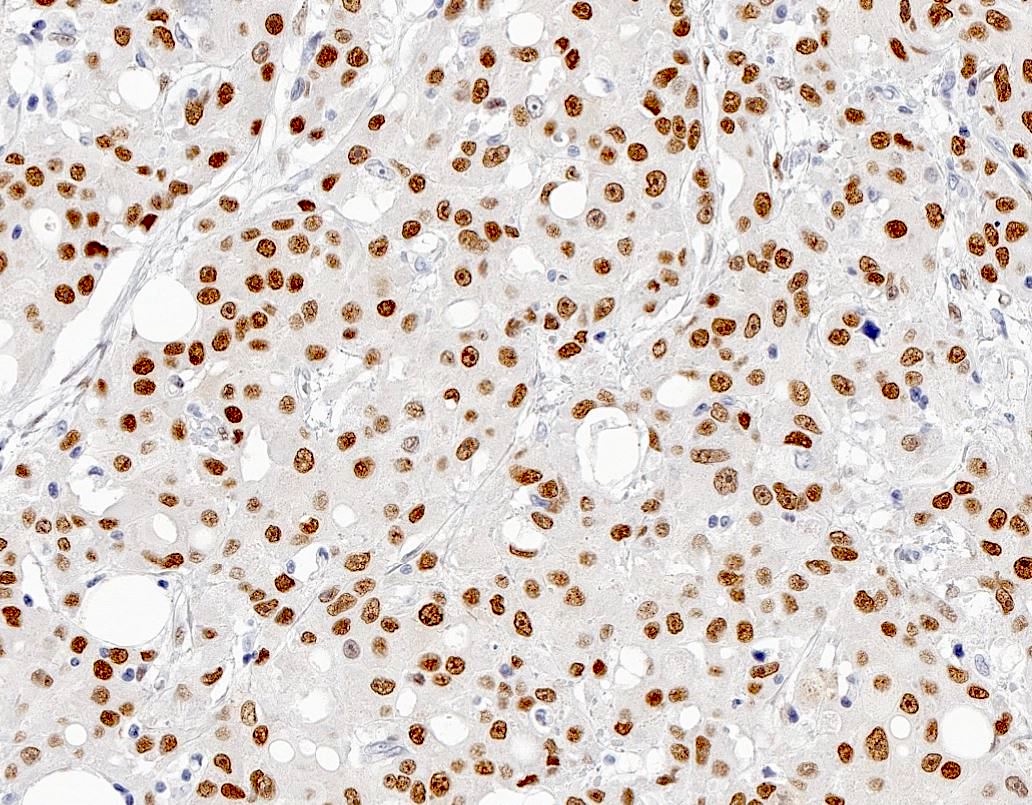
AR positive
Cytology description
- Highly cellular
- Sheets, clusters and single cells with abundant eosinophilic cytoplasm, large nuclei with variable pleomorphism and prominent nucleoli (Acta Cytol 1996;40:247)
- Binucleate and multinucleate forms; often many bare nuclei
- Difficult to differentiate from benign apocrine metaplastic lesions on cytologic preparations (Diagn Cytopathol 2017;45:1156)
Positive stains
Electron microscopy description
- Extensive rough endoplasmic reticulum and numerous osmophilic membrane bound granules (Am J Pathol 1986;123:532)
- Large mitochondria with incomplete cristae (Histol Histopathol 2013;28:13935)
Electron microscopy images
Images hosted on other servers:

Cytoplasm rich in organelles

Electron dense granules
Molecular / cytogenetics description
- Most genetic alterations found in carcinoma with apocrine differentiation are also found in invasive breast carcinoma, NST
- Frequent mutations of TP53 and PIK3CA / PTEN / AKT genes (Mod Pathol 2020;33:2473)
- Gene expression profiling has defined a molecular apocrine / luminal AR signature (with or without HER2 activation)
- Molecular apocrine / luminal AR signature does not always correlate with apocrine morphology
Sample pathology report
- Left breast, partial mastectomy:
- Carcinoma with apocrine differentiation (see synoptic report and comment)
- Comment: Sections show an infiltrating tumor comprised entirely of large epithelial cells with abundant eosinophilic and granular cytoplasm, well defined cell borders, enlarged nuclei and prominent nucleoli. The tumor cells are diffusely and strongly positive for AR and AMACR; they are negative for ER, PR and HER2. The combined cytomorphologic and immunohistochemical findings are consistent with a carcinoma with apocrine differentiation.
Differential diagnosis
- Invasive breast carcinoma, NST with focal apocrine differentiation:
- Focal apocrine differentiation may be present in up to 60% of invasive ductal carcinoma, NST (J Clin Pathol 2007;60:1313)
- Carcinoma with apocrine differentiation must have > 90% apocrine morphology
- Invasive breast carcinoma, NST with oncocytic carcinoma pattern:
- Tumor cells with abundant eosinophilic and granular cytoplasm with well defined cell borders and round, centrally located nuclei with prominent nucleoli
- Positive for mitochondrial immunostains
- Mostly positive for ER
- Often display chromosomal gains of 11q13.1-q13.2 and 19p13
- Granular cell tumor:
- Apocrine DCIS:
- DCIS with apocrine cytology
- Myoepithelial cell layer present
- Apocrine adenosis / atypical apocrine adenosis:
- Lobulocentric proliferation with apocrine cytology and distortion by stromal fibrosis / sclerosis
- Myoepithelial cell layer present
- Histiocytic proliferations:
- Pale to foamy cytoplasm without nuclear atypia
- CD68 positive
Additional references
Practice question #1
A 3.3 cm irregular mass was detected within the right breast of a 78 year old woman. Lumpectomy showed a tumor with histology as represented in the image throughout the tumor. What biomarker profile is concordant with this subtype of breast cancer?
- AR+, ER+, PR-, HER2-
- AR+, ER+, PR+, HER2-
- AR+, ER-, PR-, HER2-
- AR-, ER-, PR-, HER2-
Practice answer #1
C. AR+, ER-, PR-, HER2-. Carcinomas with apocrine differentiation are comprised of tumor cells with apocrine cytology: large atypical epithelial cells with abundant eosinophilic and granular cytoplasm, enlarged nuclei and prominent nucleoli. Apocrine morphology must be present in > 90% of the tumor. Carcinomas with apocrine differentiation are usually triple negative (ER-, PR- and HER2-); however, HER2 amplification / overexpression has been reported in 30 to 60% of tumors. Carcinomas with apocrine differentiation demonstrate diffuse and strong AR immunoreactivity. It should be noted that focal apocrine morphology and AR immunoreactivity may be seen in up to 60% of invasive breast carcinomas, NST. Additionally, AMACR, a marker of apocrine differentiation, is positive in the majority of carcinomas with apocrine differentiation.
Comment Here
Reference: Apocrine carcinoma
Comment Here
Reference: Apocrine carcinoma
