Cervix
Benign / nonneoplastic epithelial lesions
Tunnel clusters
Author: Gulisa Turashvili, M.D., Ph.D.
Editorial Board Member: Carlos Parra-Herran, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 2 April 2020
Last staff update: 30 September 2024
Copyright: 2007-2025, PathologyOutlines.com, Inc.
PubMed search: Tunnel clusters
Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Turashvili G. Tunnel clusters. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixtunnelclusters.html. Accessed September 18th, 2025.
Definition / general
- Lobular aggregates of benign endocervical glands in the cervical wall
Essential features
- Incidental finding
- Benign proliferation of endocervical glands with lobular configuration
- 2 types (A and B) have been described:
- Type A tunnel clusters are composed of small noncystic glands and may show gastric metaplasia in up to 15% of cases
- Type B tunnel clusters are composed of cystically dilated glands
Terminology
- No synonyms
Epidemiology
- Common incidental finding in cone biopsies or hysterectomy specimens (Am J Surg Pathol 1990;14:895)
- More prevalent in older, multiparous and pregnant women
- Identified in 8% of adult women and 13% of postmenopausal women (Obstet Gynecol 1961;17:206)
Sites
- Endocervix
Pathophysiology
- May represent subinvolution of endocervical glandular hyperplasia, for example, due to prior pregnancies (Am J Surg Pathol 1990;14:895)
Etiology
- Unclear
Clinical features
- Typically asymptomatic
- May be associated with mucoid discharge
- Rarely visible on colposcopic examination
Diagnosis
- Histologic examination
Prognostic factors
- Excellent prognosis
- No risk of recurrence or malignant transformation
Treatment
- None
Gross description
- Tunnel A clusters are often grossly unremarkable
- Tunnel B clusters show a grossly visible, lobular mass lesion in 40% of cases and multiple lesions in 80% of cases
- Rarely cervical wall expansion
Microscopic (histologic) description
- Well demarcated, rounded, lobular proliferation of closely packed tubules of varying size lined by endocervical glandular epithelium
- No desmoplastic or inflammatory stromal response
- May be associated with Nabothian cysts
- Usually found close to endocervical surface epithelium
- Type A:
- Small elongated noncystic glands lined by columnar to low cuboidal cells with basally located nuclei and apical mucinous cytoplasm
- Mild cytologic atypia may be present with pseudostratification, nuclear enlargement, hyperchromasia, vesicular chromatin or prominent nucleoli (Am J Surg Pathol 1996;20:1312)
- Minimal or no mitotic activity
- Gastric metaplasia in up to 15% (Histopathology 2007;50:843)
- Type B (B for big):
- Cystically dilated glands containing inspissated mucin and lined by cuboidal or flattened epithelium
- The lining cells are cytologically bland with ovoid nuclei lacking mitotic activity
- Type A and type B tunnel clusters may be admixed
Microscopic (histologic) images
Contributed by Gulisa Turashvili, M.D., Ph.D.
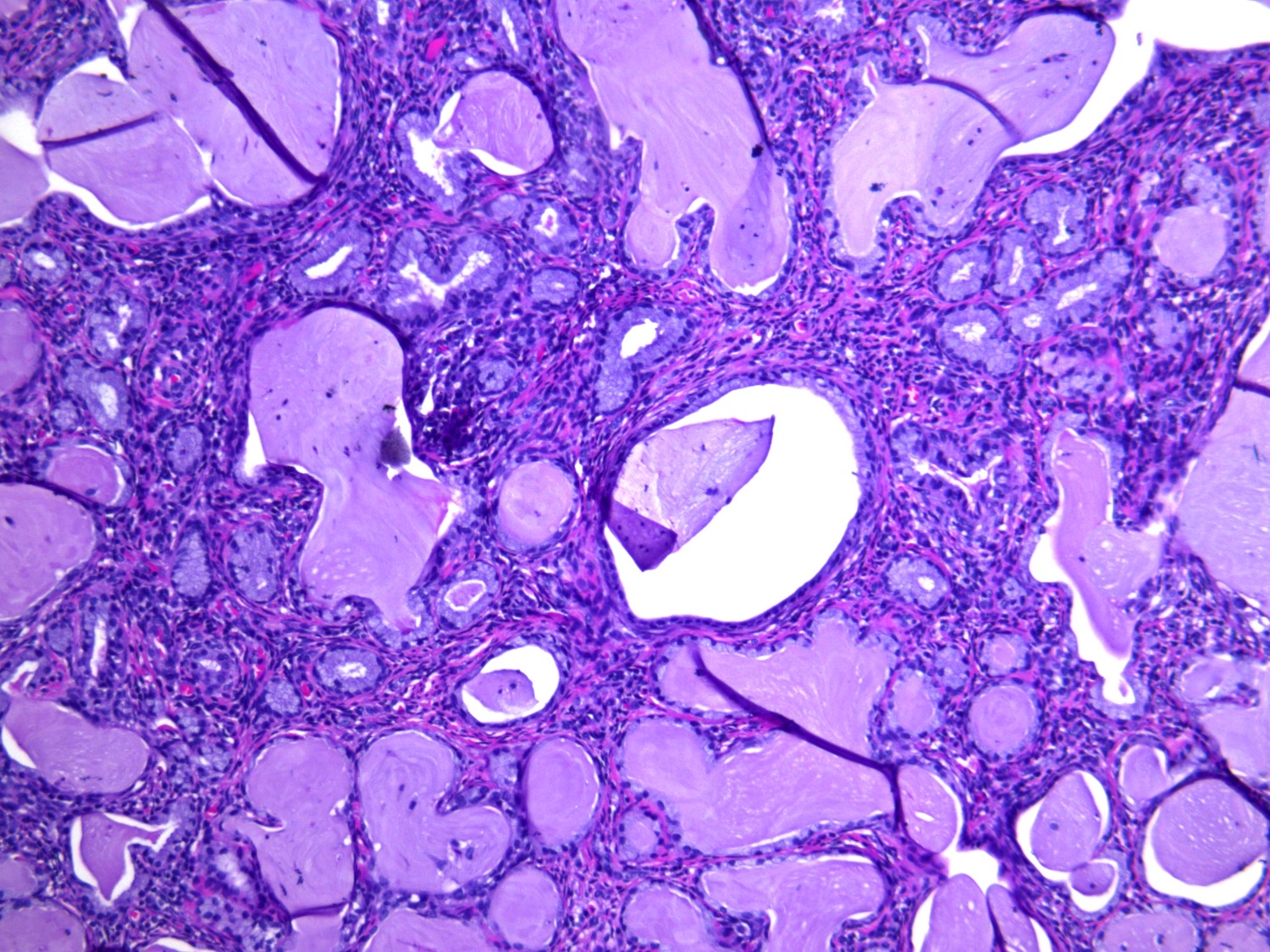
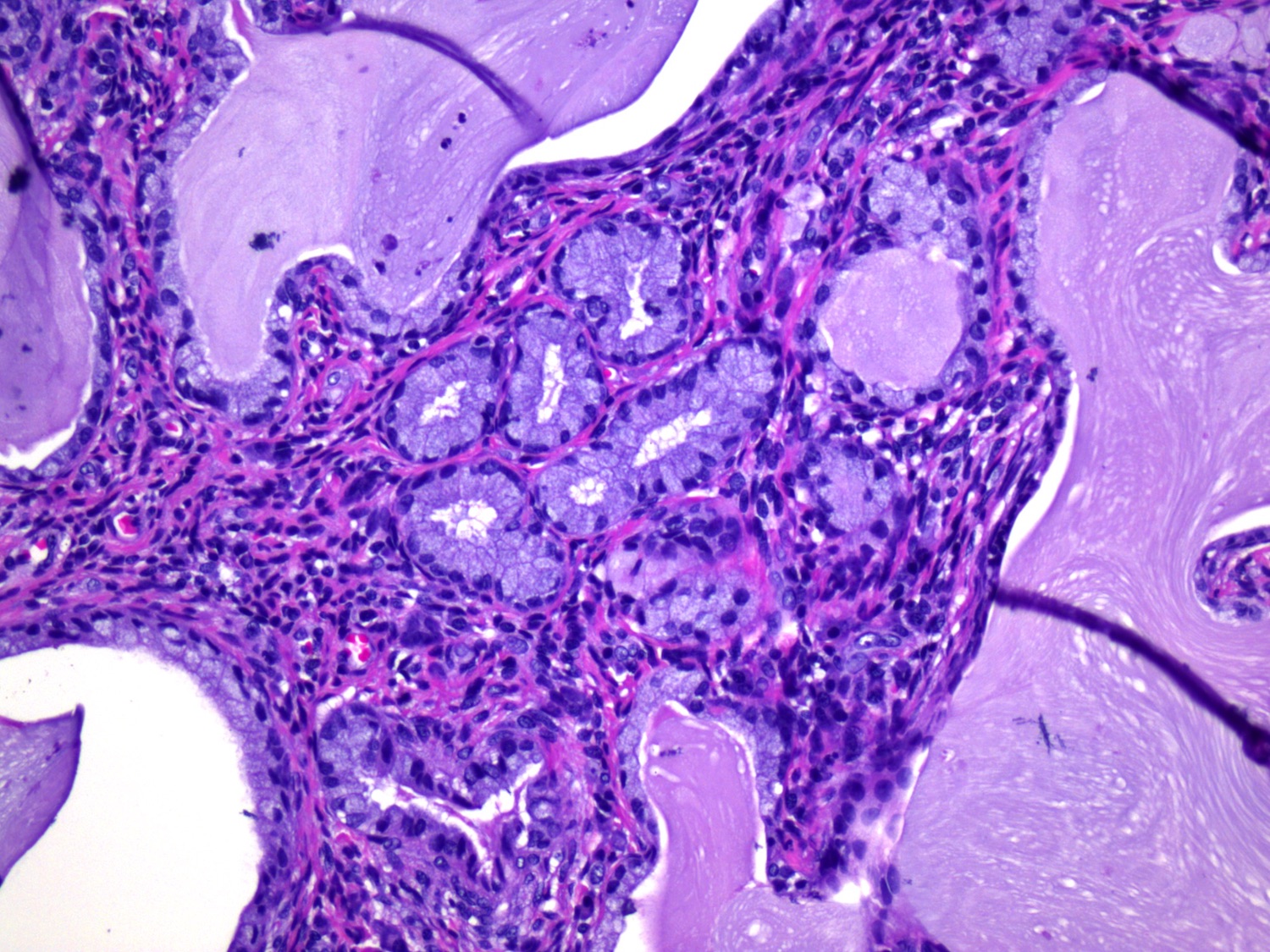
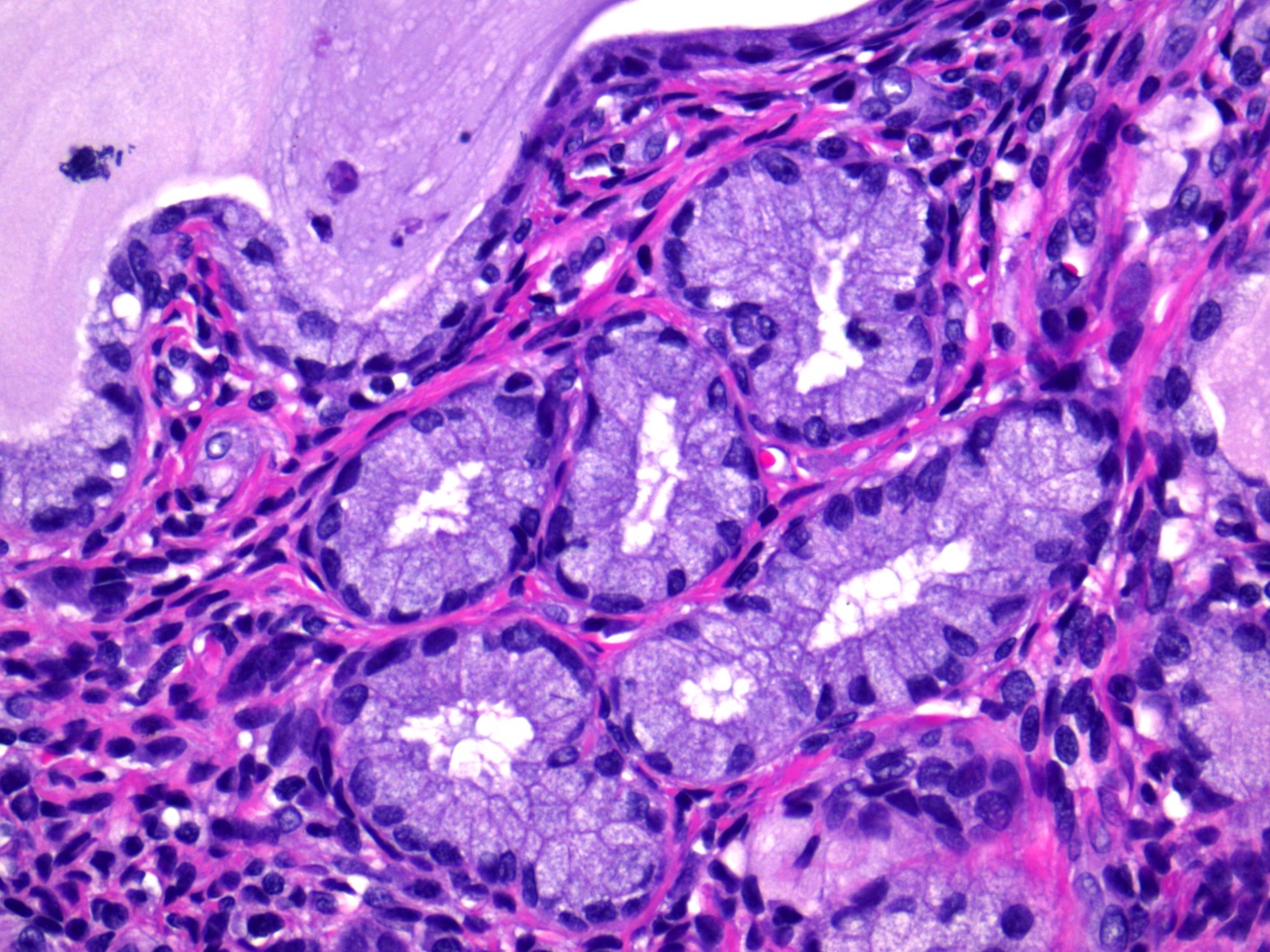
Type A tunnel clusters
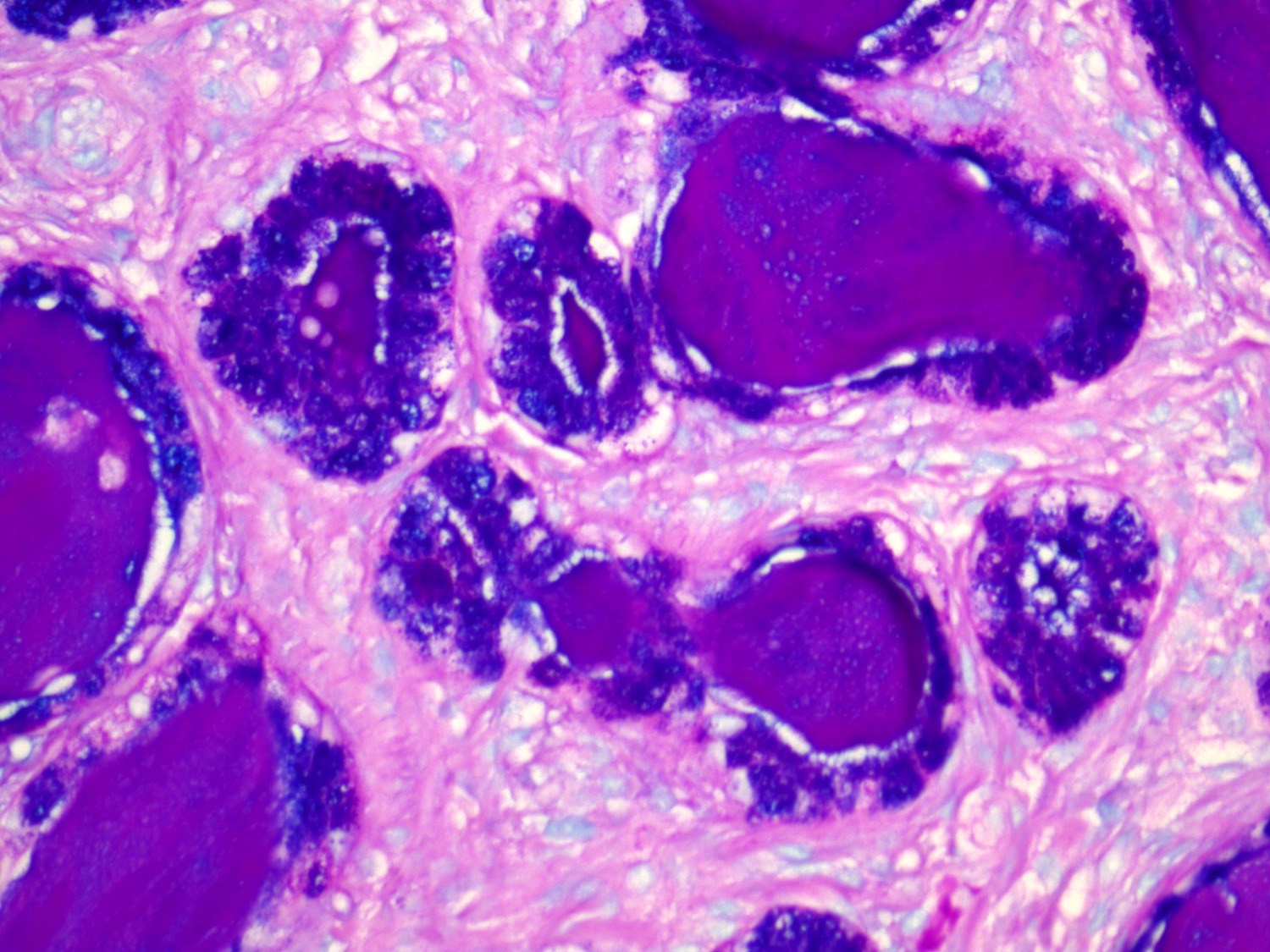
Alcian blue / PAS in type A tunnel clusters

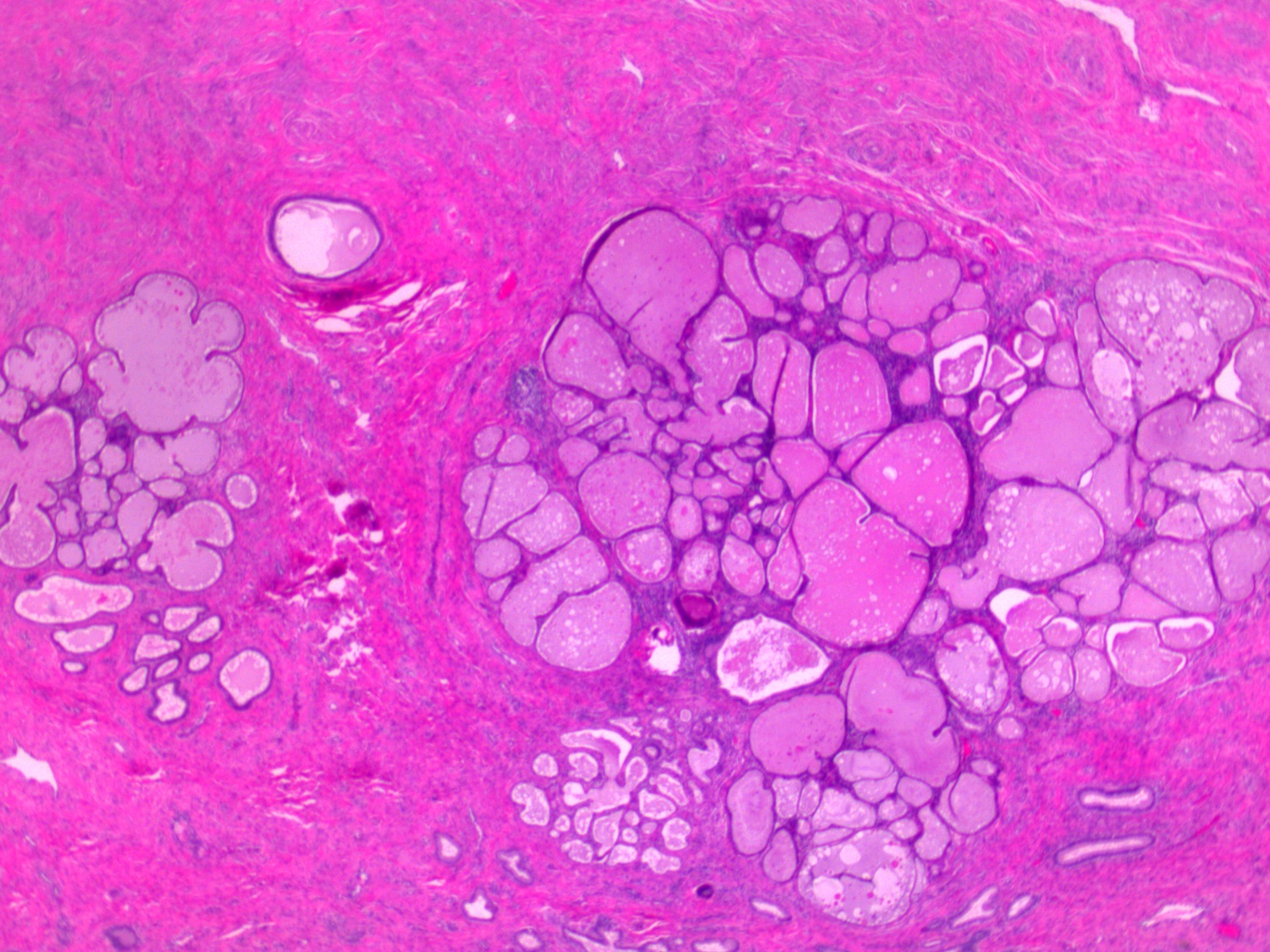

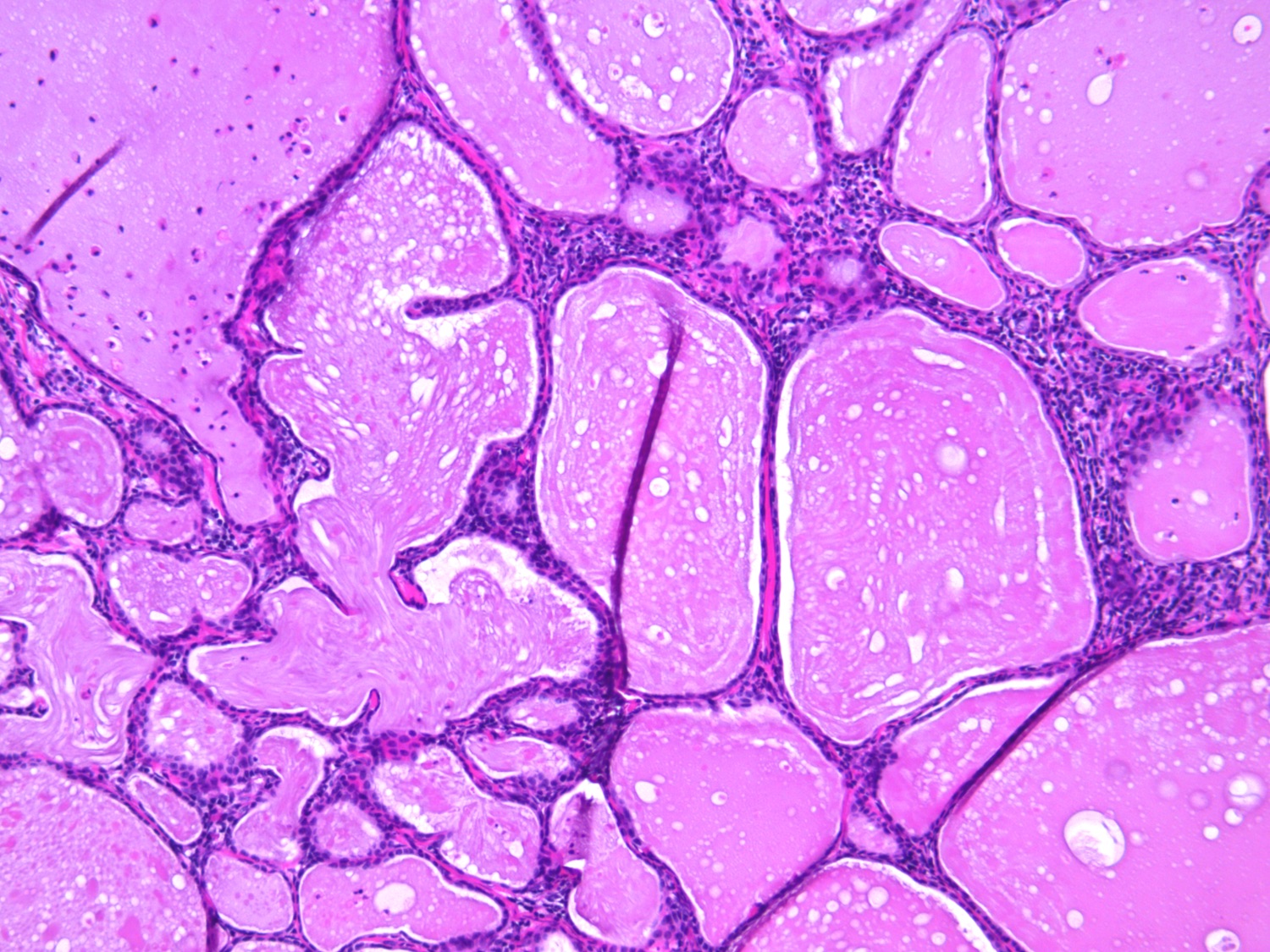
Type B tunnel clusters
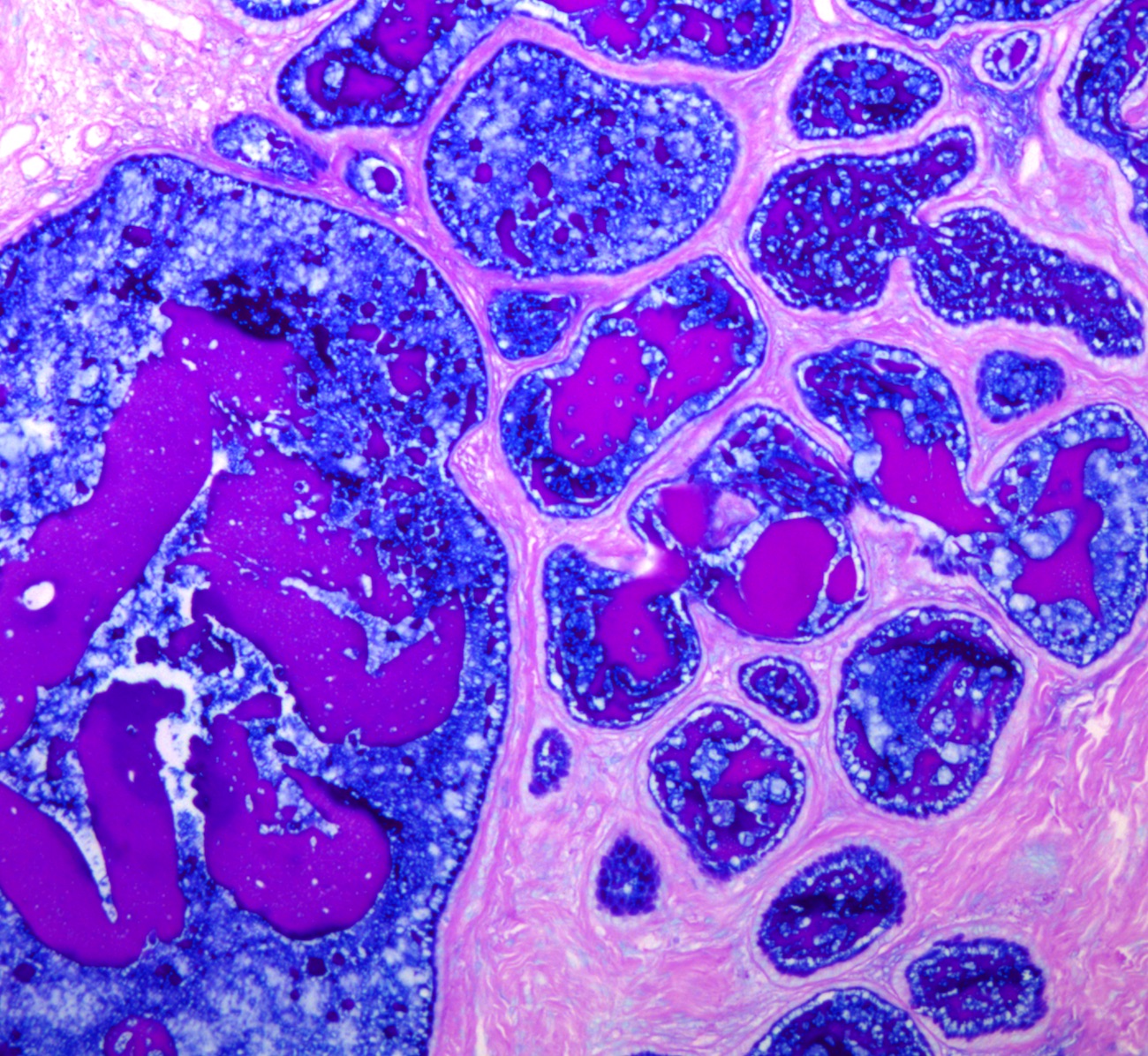
Alcian blue / PAS in type B tunnel clusters
Cytology description
- No specific cytologic features
- Benign endocervical glands
Positive stains
- PAX2 (Am J Surg Pathol 2010;34:137)
- HIK1083: positive in type A tunnel clusters if gastric metaplasia is present
- Alcian blue / periodic acid-Schiff: positive neutral mucin (red or magenta) in type A tunnel clusters if gastric metaplasia is present
Negative stains
- CEA: negative or focally positive (Am J Surg Pathol 1990;14:895)
- Ki67: negative or low
- p16: negative or patchy positive
Sample pathology report
- Tunnel clusters have no clinical relevance and do not need to be mentioned in the pathology report
Differential diagnosis
- Minimal deviation adenocarcinoma
- Lacks lobular configuration
- Composed of irregular branching glands often with deep extension in cervical wall
- At least focal stromal desmoplasia and cytologic atypia
- Negative for PAX2
- Usual type endocervical adenocarcinoma
- Shows infiltrative growth with cytologic atypia, apical mitotic figures and apoptotic bodies, often with stromal desmoplastic reaction
- Diffusely positive for p16
- Adenocarcinoma in situ
- Demonstrates cytologic atypia with pseudostratified hyperchromatic nuclei, apical mitotic figures and apoptotic bodies
- Diffusely positive for p16
- Nabothian cysts
- Shows large mucin filled cysts without lobular configuration
- Mesonephric remnants / hyperplasia
Additional references
Practice question #1
Which of the following immunoprofiles would be expected in type A tunnel clusters (pictured above)?
- Positive for PAX2, p16 and CEA, Ki67 > 10%
- Positive for PAX2, p16 and CEA, Ki67 > 10%, variable HIK1083
- Positive for PAX2, negative p16 and CEA, Ki67 < 1%, variable HIK1083
- Negative for PAX2, p16 and CEA, Ki67 < 1%
Practice answer #1
C. Positive for PAX2, negative p16 and CEA, Ki67 < 1%, variable HIK1083. Type A tunnel clusters are positive for PAX2 and negative or focally positive for p16 and CEA. The Ki67 labeling index is low. HIK1083 may also be positive if gastric metaplasia is present.
Comment Here
Reference: Tunnel clusters
Comment Here
Reference: Tunnel clusters
Practice question #2
Which of the following immunoprofiles would be expected in type B tunnel clusters (pictured above)?
- Positive for PAX2, p16 and CEA, negative for HIK1083, Ki67 > 10%
- Positive for PAX2 and HIK1083, negative for p16 and CEA, Ki67 > 10%
- Positive for HIK1083, negative for PAX2, p16 and CEA, Ki67 < 1%
- Positive for PAX2, negative for p16, CEA and HIK1083, Ki67 < 1%
Practice answer #2
D. Positive for PAX2, negative for p16, CEA and HIK1083, Ki67 < 1%. Type B tunnel clusters are positive for PAX2 and negative or focally positive for p16 and CEA. The Ki67 labeling index is low. HIK1083 is negative.
Comment Here
Reference: Tunnel clusters
Comment Here
Reference: Tunnel clusters
