Skin nonmelanocytic tumor
Benign (nonmelanocytic) epidermal tumors or tumor-like lesions
Dermatosis papulosa nigra
Authors: Negin Farsi, M.D., Sara C. Shalin, M.D., Ph.D.
Editorial Board Member: Viktoryia Kozlouskaya, M.D., Ph.D.


Last author update: 28 October 2022
Last staff update: 27 February 2023
Copyright: 2022-2025, PathologyOutlines.com, Inc.
PubMed Search: Dermatosis papulosa nigra
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Farsi N, Shalin SC. Dermatosis papulosa nigra. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnonmelanocyticdermatosispapulosanigra.html. Accessed September 16th, 2025.
Definition / general
- Benign epidermal growth presented as hyperpigmented or skin colored papules on face and neck, most commonly found on patients with darker phototypes (Fitzpatrick type IV, V or VI)
- Likely a variant of seborrheic keratosis
Essential features
- Small (several millimeters) hyperpigmented or flesh colored papules seen most commonly in patients with skin of color, particularly darker phototypes (Fitzpatrick type IV, V or VI)
- Increase in size and number of papules with aging
- Familial
- Clinical: filiform, verrucous or pedunculated pigmented papule
- Histology: acanthosis, papillomatosis, hyperkeratosis and hyperpigmentation
Terminology
- First described in 1925 by Dr. Aldo Castellani
- Seborrheic keratosis
ICD coding
- ICD-10: L82.1 - other seborrheic keratosis
Epidemiology
- Common in patients with skin of color, particularly darker phototypes (Fitzpatrick type IV, V or VI), affecting 10 - 75% of the population (Clin Dermatol 2017;35:491)
- Onset often late in adolescence, increasing numbers with age, common in adulthood and age > 60 years
- Familial in majority of cases (Int J Dermatol 2017;56:957)
- F:M = 2:1
Sites
- Mainly in photoexposed areas: head, neck and upper trunk
Pathophysiology
- Not entirely known
- Frequent positive family history and possible genetic predisposition
- Somatic activation mutation in FGFR3 has been rarely reported (Br J Dermatol 2010;162:508)
- Cumulative ultraviolet (UV) exposure may play a role
Etiology
- Not entirely known
- Aging
- UV exposure
Clinical features
- Round, 1 - 5 mm, skin colored to hyperpigmented fleshy papules mimicking skin tags, warts or seborrheic keratoses
- Filiform to sessile, smooth surface to wrinkled papules in a symmetric distribution
- Distribution is typically head and neck, upper chest
- Generally asymptomatic papules without crusting, scaling or ulceration
- No spontaneous resolution (Int J Dermatol 2017;56:957)
Diagnosis
- Diagnosis is usually clinical
- Dermatoscopy: fissures and ridges in a cerebriform pattern in 59% of cases, comedo-like openings in 27% and milia-like cysts (Int J Dermatol 2017;56:957)
- Biopsy often performed if concerned for malignancy
- Histologic findings are confirmatory
Prognostic factors
- No risk for transforming to malignancy
- Never regresses spontaneously
Case reports
- 3 year old boy with dermatosis papulosa (Pediatr Dermatol 1993;10:356)
- 9 year old girl with early onset dermatosis papulosa nigra (Br J Dermatol 2016;174:1148)
- 32 year old woman with superimposed segmental dermatosis papulosa nigra (Clin Exp Dermatol 2020;45:521)
- 42 year old black woman with eruptive dermatosis papulosa nigra as a possible sign of internal malignancy (Int J Dermatol 2007;46:186)
Treatment
- Not necessary; for cosmetic purposes
- Caution in choosing treatment option due to tendency of darker skin to dyspigmentation
- Snip excision with scissors
- Light curettage with or without anesthesia
- Electrodesiccation (Dermatol Surg 2009;35:1079)
- Cryotherapy
- Potassium titanyl phosphate (KTP), pulse dye laser (PDL), Nd:YAG and carbon dioxide lasers (Indian J Dermatol 2015;60:321, Dermatol Surg 2010;36:1968)
Clinical images
Contributed by Sara C. Shalin, M.D., Ph.D.

Well circumscribed filiform lesions

Flat topped papules
Gross description
- Round to filiform, skin colored or hyperpigmented polyp / papule ranging from 1 - 5 mm
Microscopic (histologic) description
- Irregular acanthosis of epidermis, hyperkeratosis and papillomatosis
- Elongated and interconnected rete ridges with hyperpigmentation of basal layer
- No increase in melanocyte number
- Keratin filled invagination of epidermis
- Prominent and well developed fibrous stroma within papillomatous acanthotic structures
- Similar features to reticulate and acanthotic types of seborrheic keratosis (Int J Dermatol 2017;56:957)
Microscopic (histologic) images
Contributed by Sara C. Shalin, M.D., Ph.D.

Hyperkeratotic papule with papillomatosis
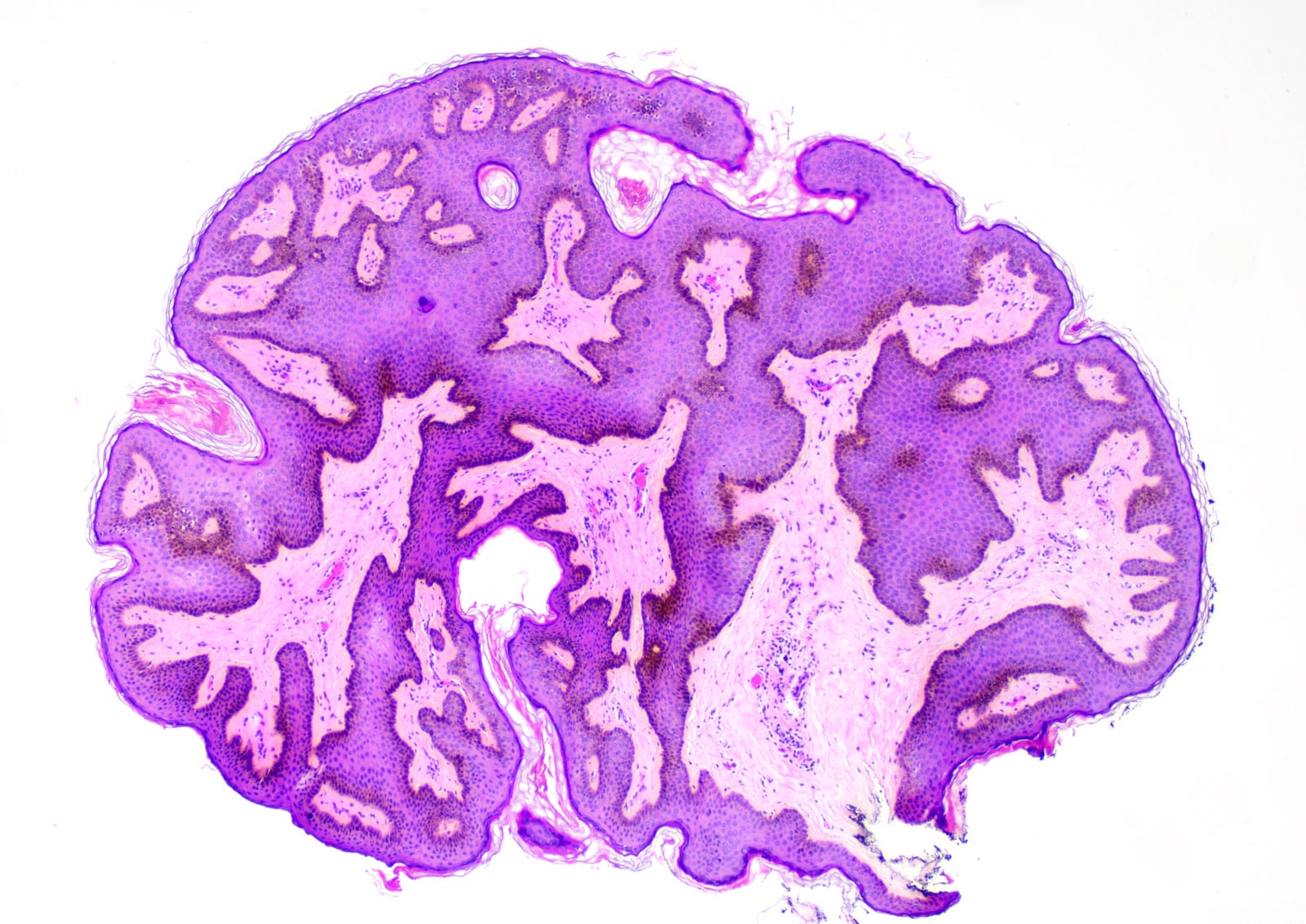
Pedunculated papule
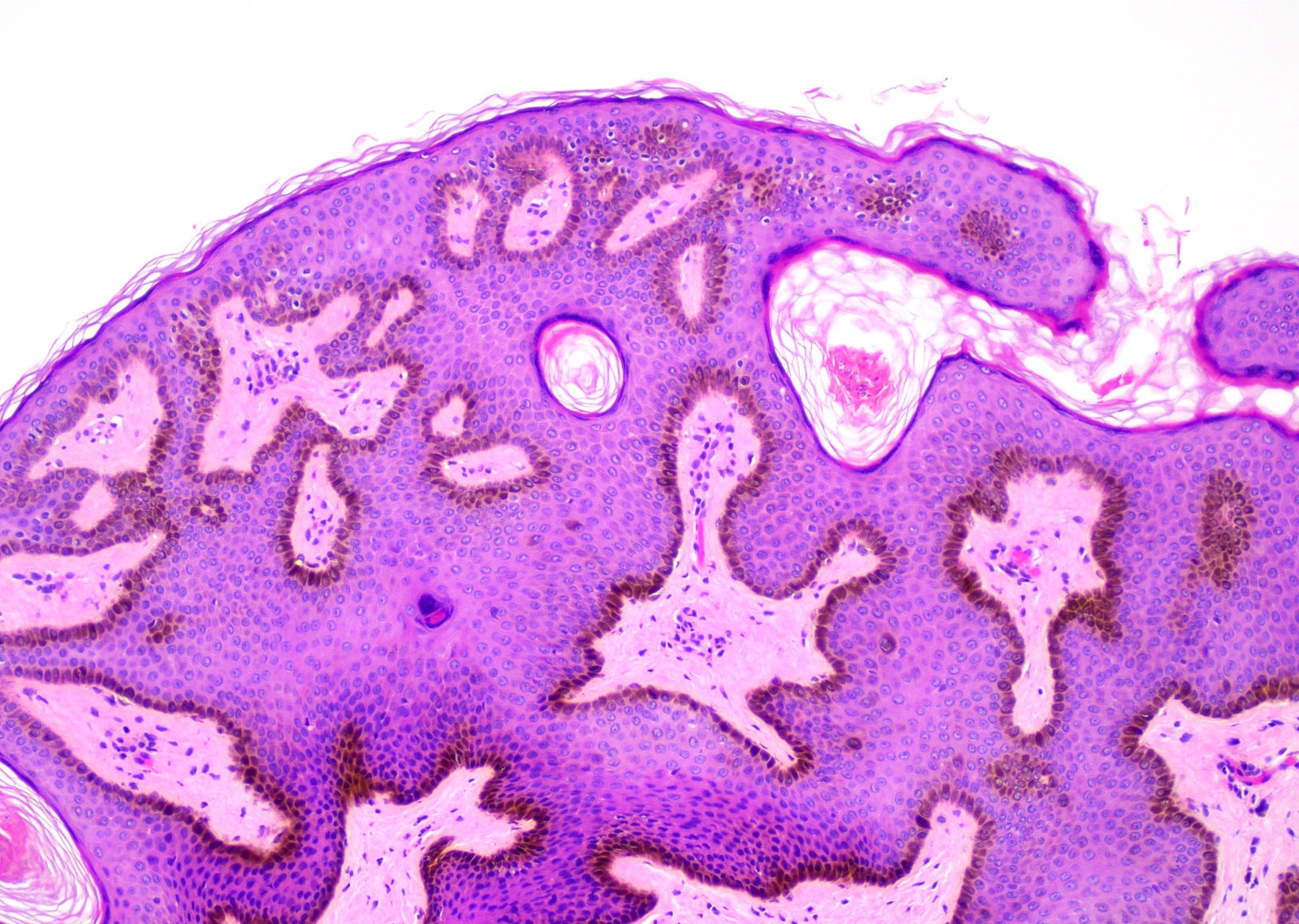
Basal hyperpigmentation
Positive stains
- No stains are required to make the diagnosis
- Pancytokeratin and high molecular weight cytokeratin positive
Negative stains
Sample pathology report
- Skin, right shoulder, shave biopsy:
- Dermatosis papulosa nigra
Differential diagnosis
- Seborrheic keratosis:
- Essentially identical histopathologic features
- Distinguishing features are predominantly clinical
- Not all clinicians agree with dermatosis papulosa nigra being a variant of seborrheic keratosis
- Affects all skin types, including lighter skin phototypes (Fitzpatrick skin type I to II) (Int J Dermatol 2007:46:45)
- Not limited to sun exposed areas
- Can be larger in size (up to several cm)
- Verruca vulgaris:
- Papillomatosis, tiers of parakeratosis, valleys of hypergranulosis and dilated papillary dermal blood vessels
- Acrochordon / fibroepithelial polyp / skin tag:
- Polypoid fragment of skin lined by unremarkable (not significantly acanthotic) epidermis with abundant loose fibrocollagenous stroma, abundant vessels and no adnexal structures
- Melanocytic nevi:
- Nest of melanocytes in dermoepidermal junction or within dermis
- Actinic keratosis:
- Proliferation of atypical keratinocytes at basal layer, loss of granular layer, parakeratosis, solar elastosis in dermis
Additional references
Practice question #1
(Disclaimer: this question has not been reviewed or approved by Dr. Shalin)
65 year old woman with darkly pigmented skin (Fitzpatrick type V) presented with multiple pigmented lesions on her cheek with the microscopic features shown above. What is the best diagnosis?
- Actinic keratosis
- Cutaneous fibroepithelial polyp
- Dermatosis papulosa nigra
- Verruca vulgaris
Practice answer #1
C. Dermatosis papulosa nigra. This is a dermatosis papulosa nigra showing irregular acanthosis, hyperpigmentation of basal layer and papillomatosis.
Comment Here
Reference: Dermatosis papulosa nigra
Comment Here
Reference: Dermatosis papulosa nigra
Practice question #2
(Disclaimer: this question has not been reviewed or approved by Dr. Shalin)
What are the most important histology findings of dermatosis papulosa nigra?
What are the most important histology findings of dermatosis papulosa nigra?
- Increased melanocyte proliferation in epidermis
- Papillomatosis, acanthosis and hyperkeratosis
- Papillomatosis, parakeratosis, valleys of hypergranulosis and dilated papillary dermal blood vessels
- Parakeratosis, proliferation of atypical keratinocytes at basal layer and loss of granular layer
Practice answer #2
B. Papillomatosis, acanthosis and hyperkeratosis. Microscopic findings of dermatosis papulosa nigra are hyperkeratosis, papillomatosis, elongated and interconnected rete ridges with hyperpigmentation of basal layer and irregular acanthosis.
Comment Here
Reference: Dermatosis papulosa nigra
Comment Here
Reference: Dermatosis papulosa nigra
