Testis & paratestis
Development
Cryptorchidism
Authors: Christopher Dall, M.D., Debra L. Zynger, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.


Last author update: 7 December 2021
Last staff update: 4 June 2025
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Cryptorchidism [TI] testis and epididymis
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Dall C, Zynger DL. Cryptorchidism. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/testiscryptorchidism.html. Accessed July 31st, 2025.
Definition / general
- Absence of one or both testes in the scrotum
- Most common congenital abnormality of the genitourinary tract (Transl Pediatr 2016;5:233)
- Associated with infertility and subfertility, testicular germ cell tumor, testicular torsion and inguinal hernia
Essential features
- Absence of one or both testes in the scrotum most commonly due to failure of descent into the scrotum during fetal development
- Increased risk of reduced fertility and testicular germ cell tumor
Terminology
- Cryptorchidism: absence of one or both testes in the scrotum
- Anorchia or vanishing testis syndrome: absence of one or both testes
- Orchiopexy or orchidopexy: procedure that tethers the testicle into the scrotum
- Ectopic testis: testis is situated away from normal path of descent; differs from undescended testicle
ICD coding
Epidemiology
- 1 - 4% in full term newborns of normal weight; decreases to 1% by the first year (Transl Pediatr 2016;5:233, Int J Urol 2021;28:882)
- Incidence varies by region with increased rates in United Kingdom, Denmark and Lithuania (Hum Reprod Update 2008;14:49)
Sites
- Undescended testicle may be located in the abdomen or inguinoscrotal region
Pathophysiology
- Testicular descent from initial position on abdominal wall is divided into 2 stages with abnormalities of migration thought to be associated with undescended testicle (Endocr Rev 2008;29:560)
- Transabdominal descent: the gubernaculum, a caudal ligament connecting the testicle to the internal ring, holds testicle near internal ring as abdominal cavity develops; insulin-like factor 3 (INSL3) and anti-Müllerian hormone dependent
- Inguinoscrotal descent: the gubernaculum shortens, pulling testicle through inguinal canal to position within scrotum; androgen dependent
- May be a component of testicular dysgenesis syndrome, which includes increased levels of testicular malignancy, poor semen quality and hypospadias
Etiology
- Numerous genes implicated; lack of a clear association in human studies suggests multifactorial causes
- More common in preterm (30%) and low birth weight infants (Transl Pediatr 2016;5:233, J Urol 1999;161:1606)
- Concordance in sibling studies (Fertil Steril 2010;93:124)
- Associated with and increased risk in certain chromosomal abnormalities and genetic syndromes, such as Klinefelter and Prader-Willi syndrome (Lancet 2004;364:273)
- Environmental factors likely play a role: diethylstilbestrol and pesticide exposure have been associated with increased rates; maternal and paternal smoking may increase risk (Mol Cell Endocrinol 2012;355:208, Pediatr Int 2020;62:1256, Med Sci Monit 2005;11:CR274)
Clinical features
- 80% of undescended testicles palpated within inguinal canal or high scrotal area
- 20% of undescended testicles not palpated
- 50% lie in abdomen, 50% are atrophic (Am Fam Physician 2000;62:2047)
- Associated with increased risk of testicular germ cell tumor
- Increasing risk of malignancy with delayed treatment (J Urol 2009;181:452)
- Relative risk of malignancy is 2 - 8x; higher risks associated with delayed repair, bilateral cryptorchidism, additional endocrinopathies, abnormal karyotype and intra-abdominal testes
- Seminoma is most common malignancy
Diagnosis
- Laparoscopy is gold standard in diagnosing a nonpalpable testis
- Ultrasound and other radiologic imaging are not sensitive in diagnosing a nonpalpable testis (Pediatrics 2011;127:119, Pediatrics 2013;131:e1908)
- Must exclude retractile testis, a testis that has descended into the scrotum but has been pulled superiorly by cremaster muscle
- In bilateral cryptorchidism, must exclude congenital adrenal hyperplasia and persistent Müllerian duct syndrome
Laboratory
- In cases of bilateral undescended testicles, hormonal studies (LH, FSH, Müllerian inhibiting substance [MIS] and testosterone) may support diagnosis of gonadal dysgenesis with abnormal hCG stimulation test (Am Fam Physician 2000;62:2037)
Radiology description
- Diagnostic imaging is not recommended in most cases (J Pediatr Surg 2011;46:2406)
Prognostic factors
- Delayed repair reduces fertility, which is worse with bilateral cryptorchidism
- Relative risk for testicular germ cell tumor is 2.2x with prepubertal repair versus 5.4x with postpubertal repair (N Engl J Med 2007;356:1835)
Case reports
- 1 year old boy with swelling of abdominal wall (Am J Case Rep 2020;21:e927495)
- 1 year old boy with persistent Müllerian duct syndrome and transverse testicular ectopia (BMJ Case Rep 2018;2018:bcr2017223994)
- 46 year old man with yolk sac tumor in cryptorchid testis (BMJ Case Rep 2019;12:e229541)
Treatment
- Orchiopexy may be performed at 6 - 18 months as it is unlikely that testicle will spontaneously descend after this time (J Pediatr Urol 2021;17:239)
- American Urological Association does not recommend hormonal therapy (hCG) to promote the descent of the undescended testicle due to low response rates (AUA: Evaluation and Treatment of Cryptorchidism [Accessed 19 November 2021])
Clinical images
Images hosted on other servers:

Intra-abdominal mass

Abdominal testis

Mass with right gonadal vein

Scrotum with cryptorchidism

Abdominal wall ectopic testis
Gross description
- Smaller and atrophic compared to descended testis
Gross images
Contributed by Debra L. Zynger, M.D.
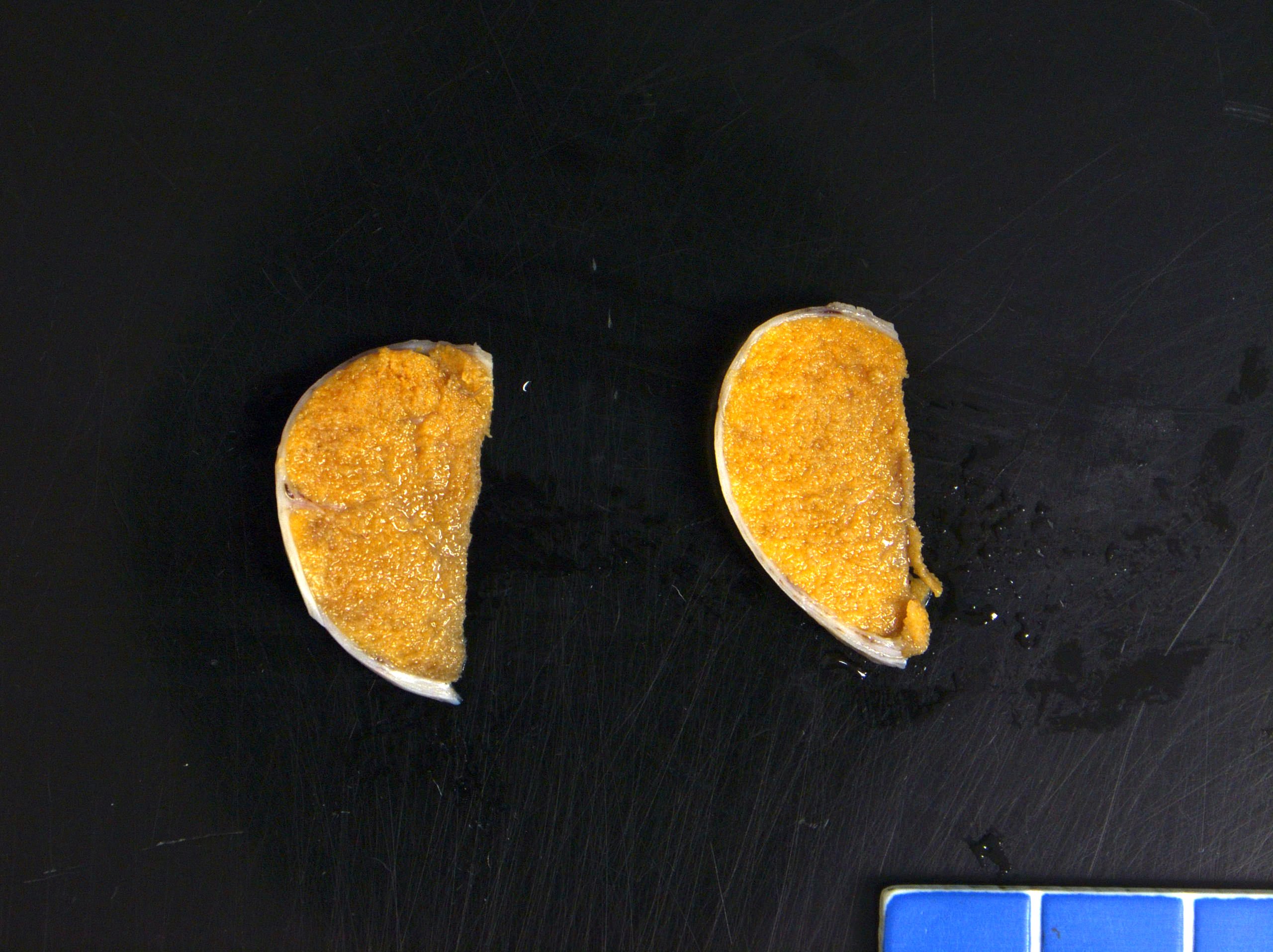
Cryptorchid testicle
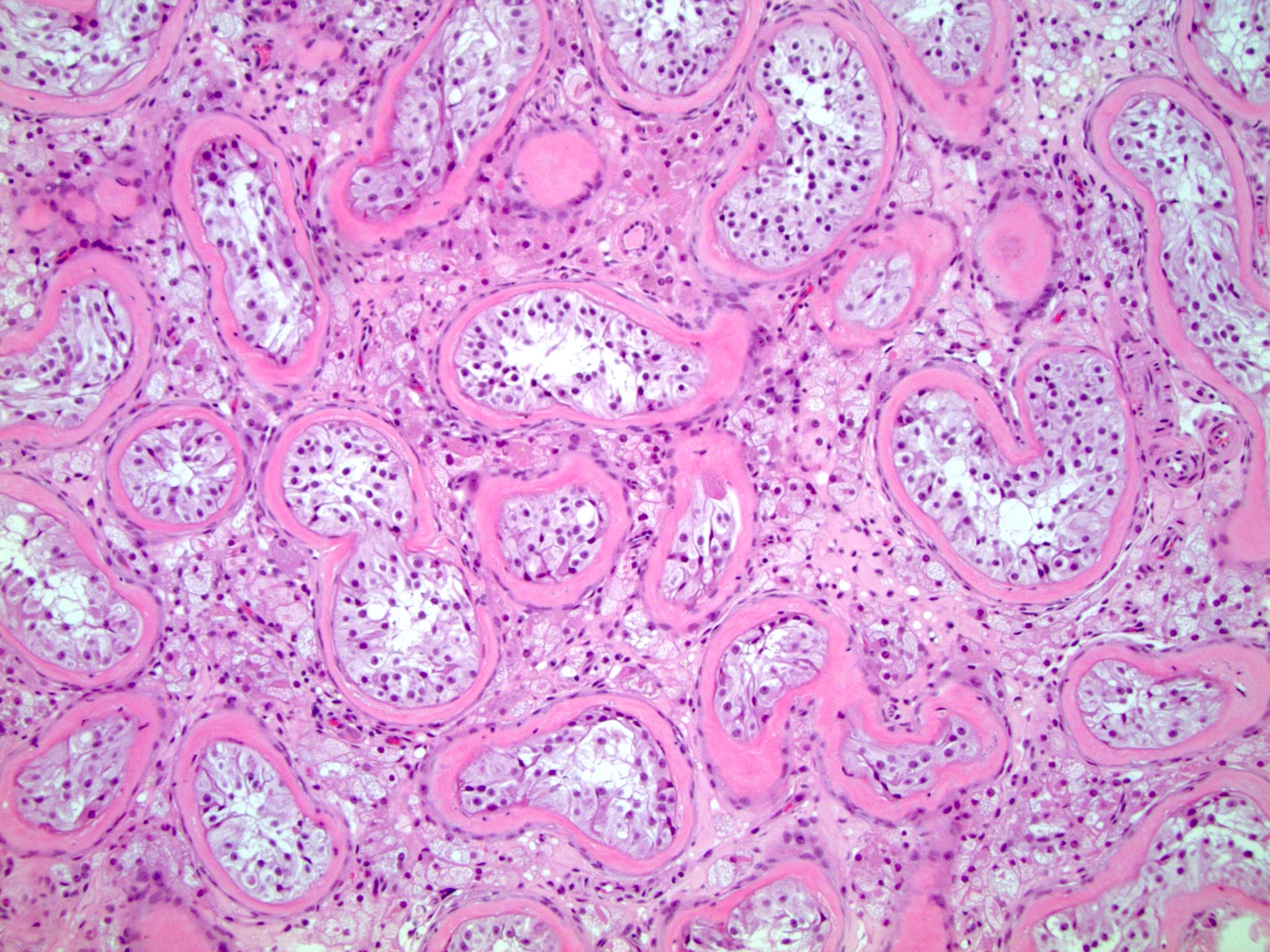
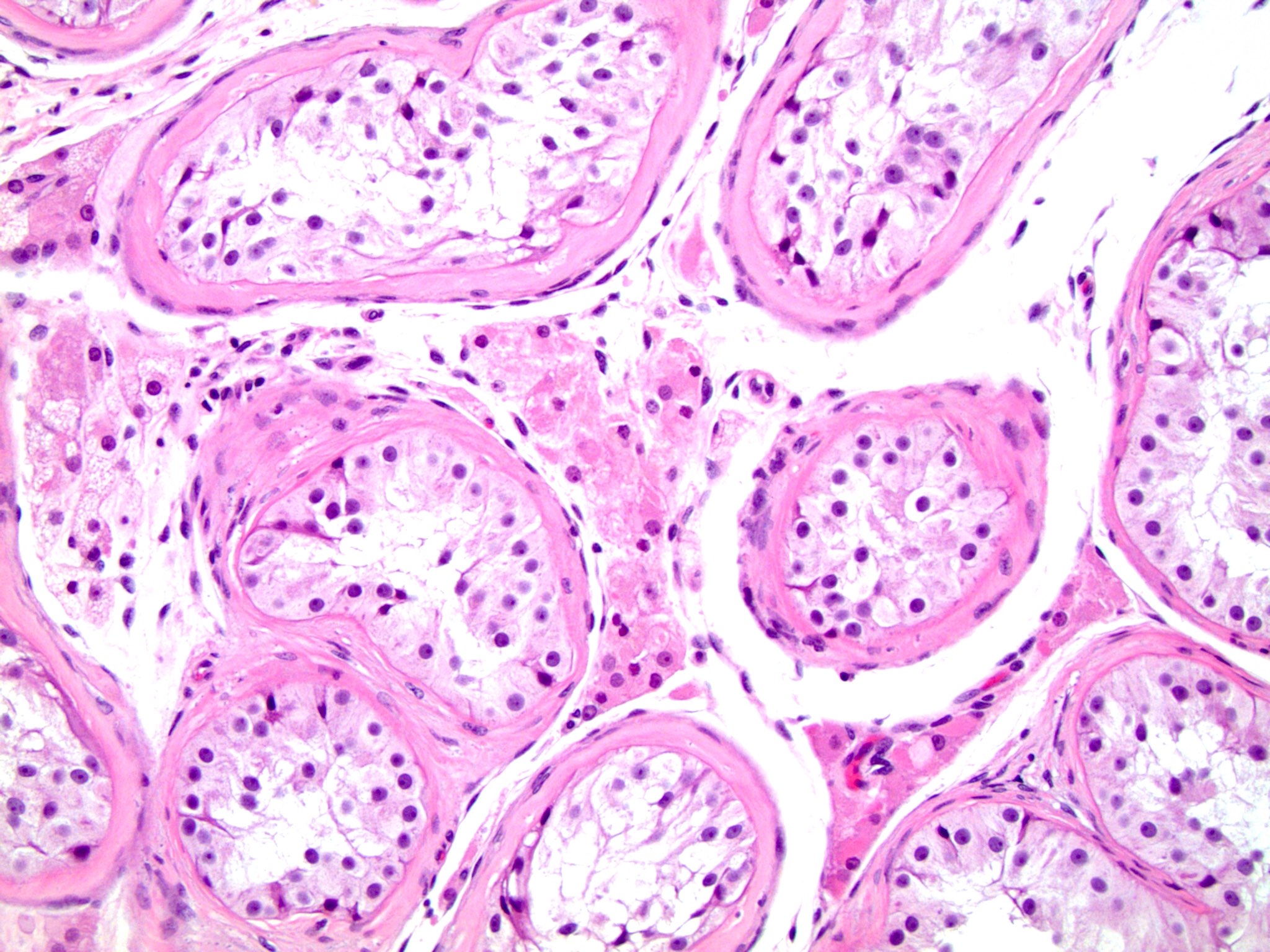
Microscopic (histologic) description
- Histopathologic differences become much more pronounced after 2 years of life and are increased with delayed orchiopexy (J Urol 2009;182:704)
- Peritubular fibrosis
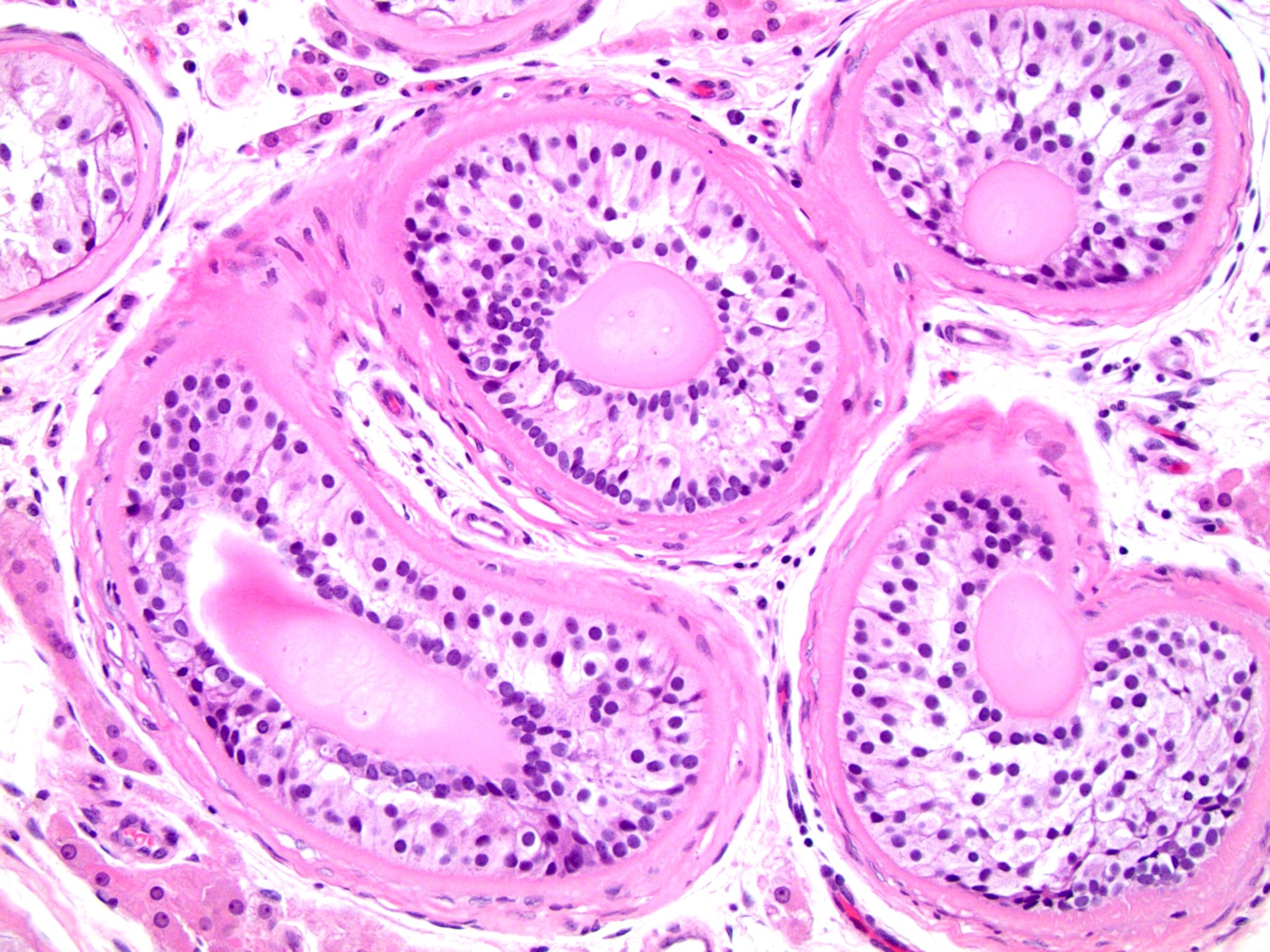
- Seminiferous tubule atrophy
- Decreased / absent spermatogenesis
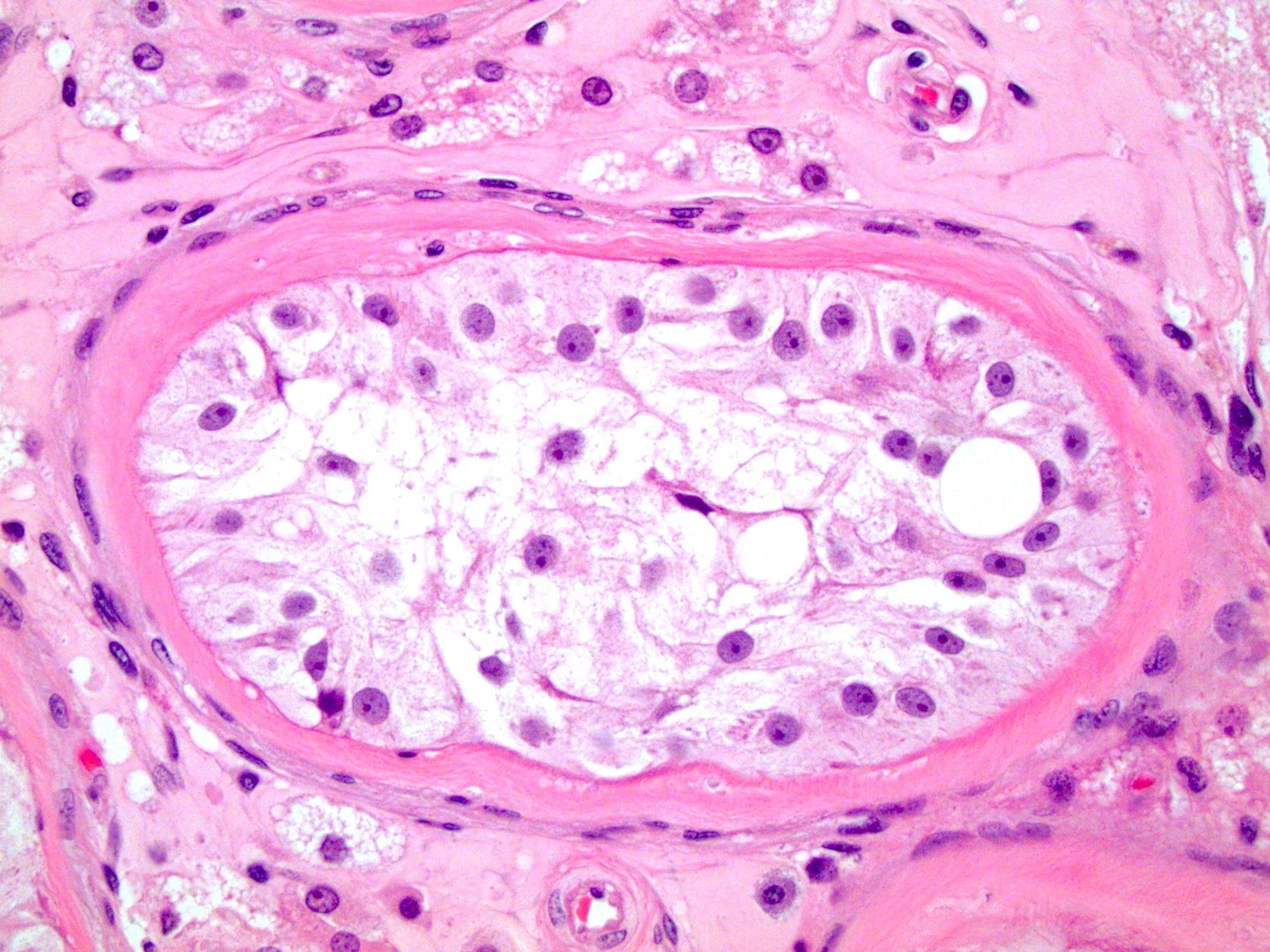
- Sertoli cells may demonstrate granular cell change with eosinophilic granular cytoplasmic lysosomes
- Sertoli cell only seminiferous tubules: tubules with only bland, monotonous pale cells with granular cytoplasm attached to the basement membrane; absent germ cells and no spermatogenesis
- Sertoli cell nodule: nodules composed of immature elongated Sertoli cells (Pick adenoma) may be present; can have central microliths
- Increased microliths within seminiferous tubules
- Retained Leydig cells give appearance of hyperplasia
- Evaluate for germ cell neoplasia in situ (GCNIS): large, pleomorphic, basally located cells within the seminiferous tubules may be present; use immunostains for confirmation
Microscopic (histologic) images
Contributed by Debra L. Zynger, M.D.
Sertoli cell only tubules
Absent spermatogenesis

Peritubular fibrosis
Sertoli cell nodule
Retained Leydig cells

Granular cell change within Sertoli cells
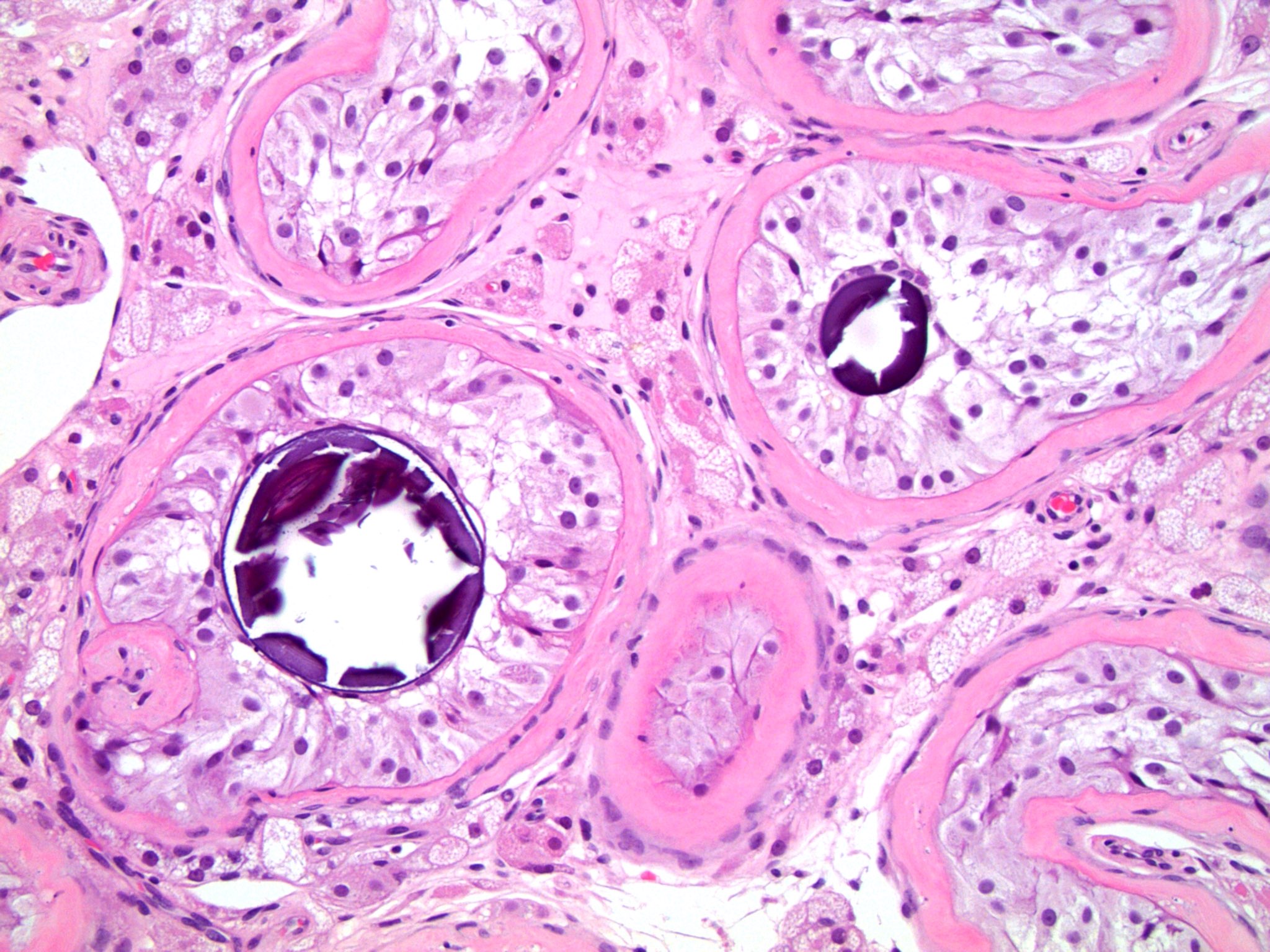
Microliths
Cytology description
- Not used to evaluate a cryptorchid testis
Positive stains
- Germ cell neoplasia in situ (GCNIS) is positive for CD117 (KIT), PLAP, D2-40 and OCT 3/4 but these stains may be falsely positive in boys < 2 years old with cryptorchidism (J Urol 2014;191:1084)
Sample pathology report
- Ectopic testis, removal:
- Seminiferous tubules with Sertoli only tubules, peritubular fibrosis, no spermatogenesis and microliths consistent with cryptorchid testis
Differential diagnosis
Practice question #1
A 24 year old man with a history of untreated cryptorchidism presents with a painful abdominal mass. Pathology is most likely to be consistent with which of the following?
- Dermoid cyst
- Germ cell neoplasia in situ
- Mixed germ cell tumor
- Seminoma
- Sertoli cell tumor
Practice answer #1
D. Seminoma is the most common malignancy in the setting of cryptorchidism.
Comment Here
Reference: Cryptorchidism
Comment Here
Reference: Cryptorchidism
Practice question #2
What histological changes are most likely to be observed in a nonneoplastic cryptorchid testis?
- Atrophic seminiferous tubules, peritubular fibrosis and nodules of cells containing dark nucleoli and eosinophilic granular cytoplasm
- Bland appearing cysts lined with cuboidal epithelium and ciliated cells
- Cysts lined by squamous cells filled with keratin
- Glycogen rich cells with large, irregular nuclei arranged in sheets
- Rod-like cytoplasmic inclusions with a diffuse growth pattern and rare mitotic cells
Practice answer #2
A. Atrophic seminiferous tubules, peritubular fibrosis and nodules of cells containing dark nucleoli and eosinophilic granular cytoplasm are findings consistent with an undescended testicle. B is incorrect because these might be the findings associated with benign glands, such as those seen in endometriosis or endosalpingiosis. C is incorrect because this histology may be associated with teratoma. D is incorrect because these might be the findings of a seminoma, which are more common in undescended testicles. E is incorrect because Leydig cell tumors often contain Reinke crystals, described in this answer choice.
Comment Here
Reference: Cryptorchidism
Comment Here
Reference: Cryptorchidism
