Thyroid & parathyroid
Cytology
Bethesda system
Follicular neoplasm (oncocytic follicular neoplasm)
Author: Ayana Suzuki, Ph.D.
Editorial Board Member: Marc Pusztaszeri, M.D.
Deputy Editor-in-Chief: Andrey Bychkov, M.D., Ph.D.

Last author update: 12 June 2025
Last staff update: 12 June 2025
Copyright: 2020-2025, PathologyOutlines.com, Inc.
PubMed Search: Follicular neoplasm (oncocytic follicular neoplasm)
Table of Contents
Definition / general | Essential features | Terminology | Sites | Pathophysiology | Clinical features | Diagnosis | Case reports | Treatment | Cytology description | Cytology images | Molecular / cytogenetics description | Videos | Sample cytology reports | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Suzuki A. Follicular neoplasm (oncocytic follicular neoplasm). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidhurthlecellneoplasm.html. Accessed September 10th, 2025.
Definition / general
- Oncocytic carcinomas are uncommon; they represent 15 - 20% of all follicular carcinomas (Rosai: Tumors of the Thyroid and Parathyroid Glands, Series 4, 2015)
- Oncocytes are thyroid follicular cells with oncocytic appearance characterized by large hyperchromatic nuclei with prominent nucleoli and abundant granular eosinophilic cytoplasm
- Cases cytologically suspected for oncocytic adenoma and oncocytic carcinoma are included
- Final diagnosis is made histologically because capsular or vascular invasion are the essential criteria of oncocytic carcinoma
- Bethesda category IV - follicular neoplasm (oncocytic follicular neoplasm) is used for cases with a cellular aspirate that consists exclusively of oncocytes (Ali: The Bethesda System for Reporting Thyroid Cytopathology, 3rd Edition, 2023)
- WHO histological classification also has a separate chapter for oncocytic tumors
Essential features
- Includes cases with most of the follicular cells showing abundant fine granular cytoplasm (oncocytes)
- Frequency: 1.2 - 8.75%
- Resection rate: 30.1%
- Risk of malignancy: 25 - 50%
- 16 - 25% of cases in this category prove not to be neoplasms but rather hyperplastic proliferations
Terminology
- Oncocytes are also known as oxyphilic, Hürthle or Askanazy cells (Oncologist 2011;16:1380)
- In the Bethesda System for Reporting Thyroid Cytopathology, FNA specimens that are suspicious for an oncocytic follicular neoplasm are distinguished from those suspicious for a nononcocytic follicular neoplasm (Ali: The Bethesda System for Reporting Thyroid Cytopathology, 3rd Edition, 2023)
Sites
- Thyroid and parathyroid
Pathophysiology
- Oncocytic appearance is due to accumulation of dysfunctional mitochondria
Clinical features
- Frequency: 1.2 - 8.75% (J Clin Diagn Res 2013;7:1051, Int J Surg 2013;11:898)
- Resection rate: 30.1% (Int J Surg 2013;11:898)
- Rate of neoplastic lesion after resection: 75 - 84% (Eur J Endocrinol 2013;169:649)
- Risk of malignancy: 25 - 50% (Ali: The Bethesda System for Reporting Thyroid Cytopathology, 3rd Edition, 2023)
- Most common histopathological diagnosis is oncocytic adenoma and oncocytic carcinoma (77.3%), followed by follicular nodular disease (13.3%) and Hashimoto thyroiditis (6.6%) (Eur J Endocrinol 2013;169:649)
- Distinction between oncocytic adenoma and oncocytic carcinoma is based upon histologic evidence of transcapsular or vascular invasion (World J Surg 2010;34:836)
- Oncocytic carcinomas represent 15 - 20% of all follicular carcinomas (Rosai: Tumors of the Thyroid and Parathyroid Glands, Series 4, 2015)
Diagnosis
- Aspirates are at least moderately cellular and are composed exclusively of oncocytes
- Aspirates composed entirely of oncocytes with abundant fine granular cytoplasm should be diagnosed as follicular neoplasm / oncocytic follicular neoplasm (FN / OFN) (Cancer Cytopathol 2025;133:e70016)
- Excluded from this category
- Sparsely cellular aspirates composed entirely of oncocytes that could be interpreted as atypia of undetermined significance
- Moderately or markedly cellular aspirates composed entirely of nonatypical oncocytes with abundant colloid; it is acceptable to interpret the sample as benign
- Specimen with partial or minimal oncocytic differentiation should be diagnosed as follicular neoplasm rather than FN / OFN
- Aspirates with oncocytes showing nuclear features of papillary carcinoma should be classified as malignant
Case reports
- 36 year old woman with medullary carcinoma of thyroid mimicking oncocytic neoplasm on cytology (Diagn Cytopathol 2019;47:943)
- 55 year old man with a novel nonsense EIF1AX mutation identified in an oncocytic carcinoma (Endocrine 2018;62:492)
- 71 year old woman with EIF1AX mutation in an oncocytic carcinoma (Endocr Pathol 2018;29:27)
- Woman in her 70s with synchronous oncocytic and medullary thyroid carcinomas (BMJ Case Rep 2022;15:e248879)
- 90 year old woman with subcutaneous implantation of oncocytic thyroid cell aggregates 9 years later from thyroidectomy (Int J Surg Case Rep 2022;93:106935)
Treatment
- Diagnostic lobectomy (Thyroid 2016;26:1)
- Molecular testing with available gene panels is generally not helpful in identifying oncocytic carcinomas or distinguishing them from adenomas (Cancer Cytopathol 2018;126:654)
- Patients with FN / OFN who have benign Afirma gene expression classifier (GEC) result may be spared an unnecessary lobectomy (Endocr Pract 2018;24:622)
Cytology description
- Abundant finely granular cytoplasm
- Blue or gray-pink (Romanowsky), green (Papanicolaou), pink (H&E)
- Nuclei
- Round
- Enlarged, central or eccentrically located
- Prominent nucleolus
- Binucleation (common)
- Small cells with high N:C ratio (small cell dysplasia) (Cancer 2002;96:261)
- Large cells with > 2 times anisonucleosis (large cell dysplasia) (Cancer 2002;96:261)
- Predominantly isolated cells but sometimes arranged in crowded, syncytial-like clusters
- Little or no colloid
- No lymphocytes or plasma cells
- Transgressing vessels (capillaries passing through clusters of Hürthle cells), seen occasionally (Arch Pathol Lab Med 2001;125:1031)
- Sometimes intracytoplasmic colloid inclusions (Arch Pathol Lab Med 2001;125:1031)
Cytology images
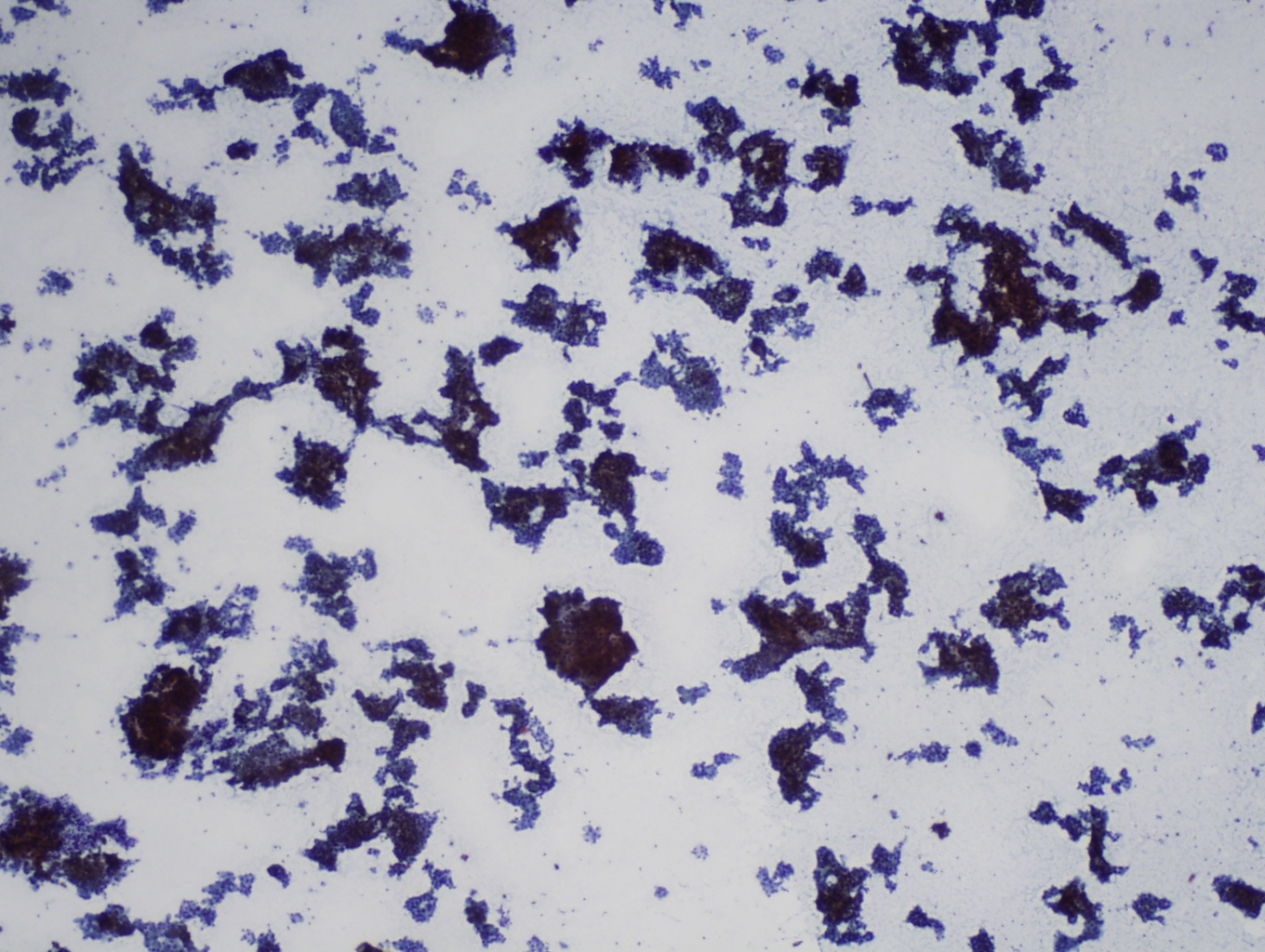
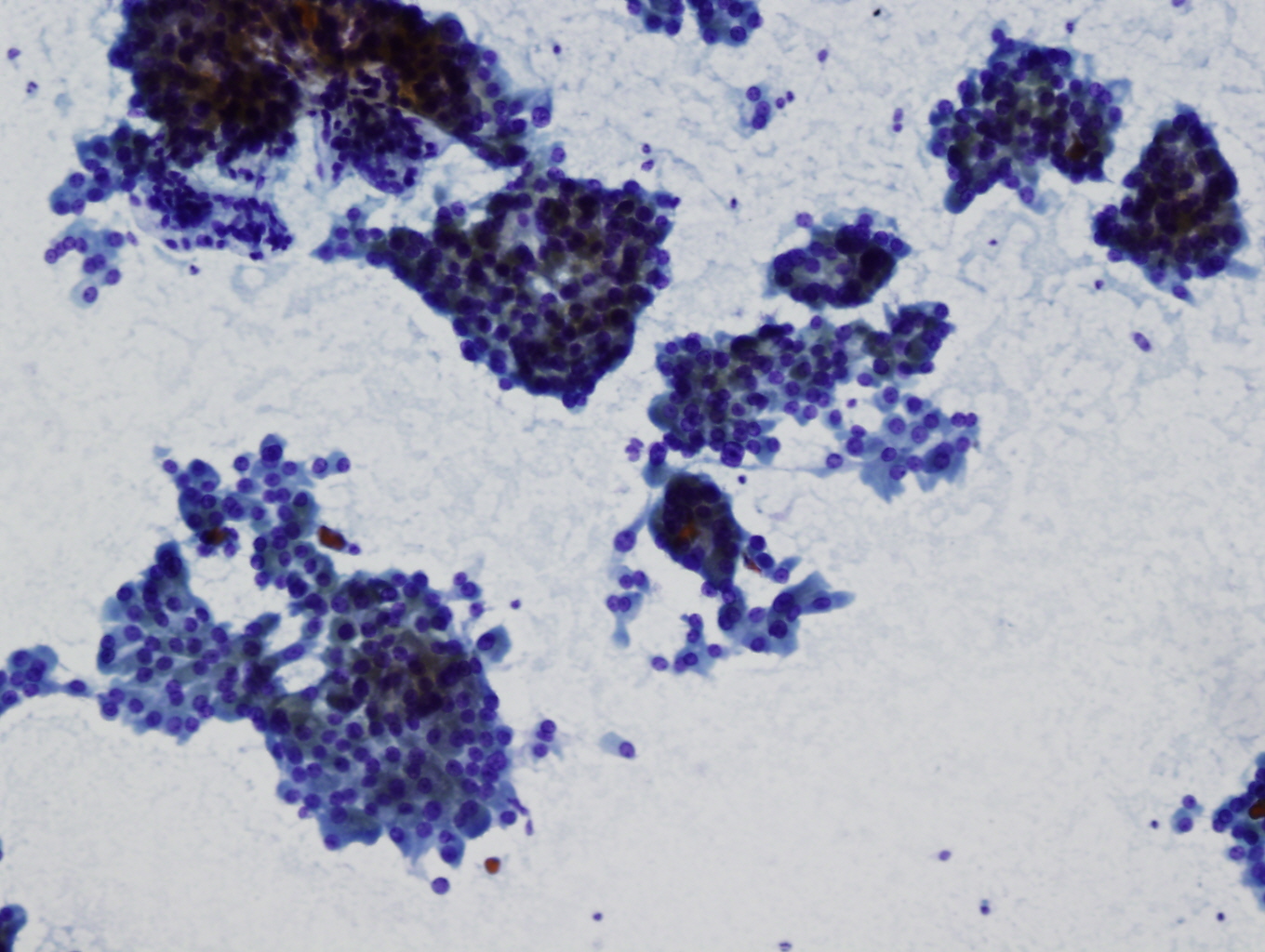
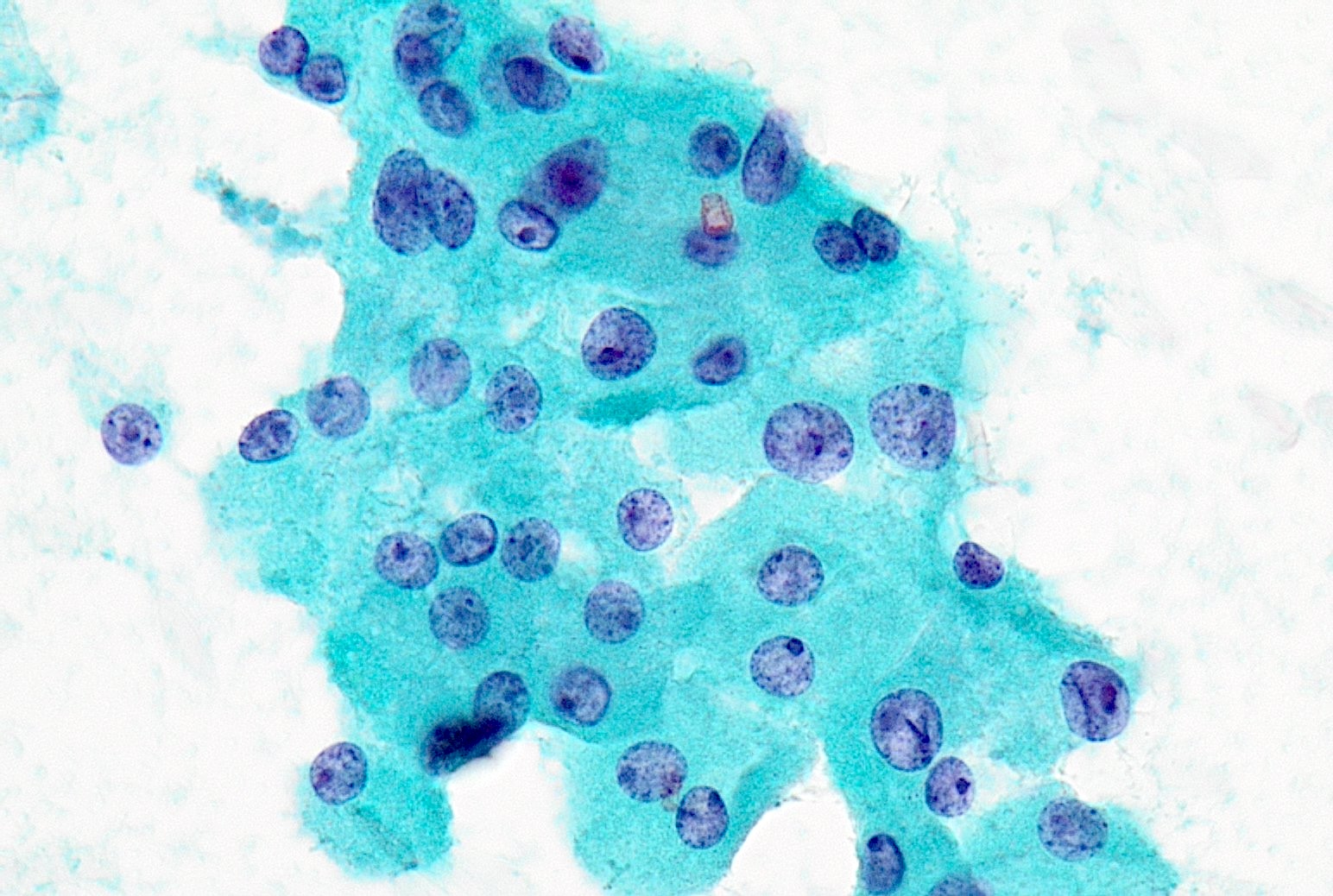
Contributed by Ayana Suzuki, Ph.D. and Grace C.H. Yang, M.D.
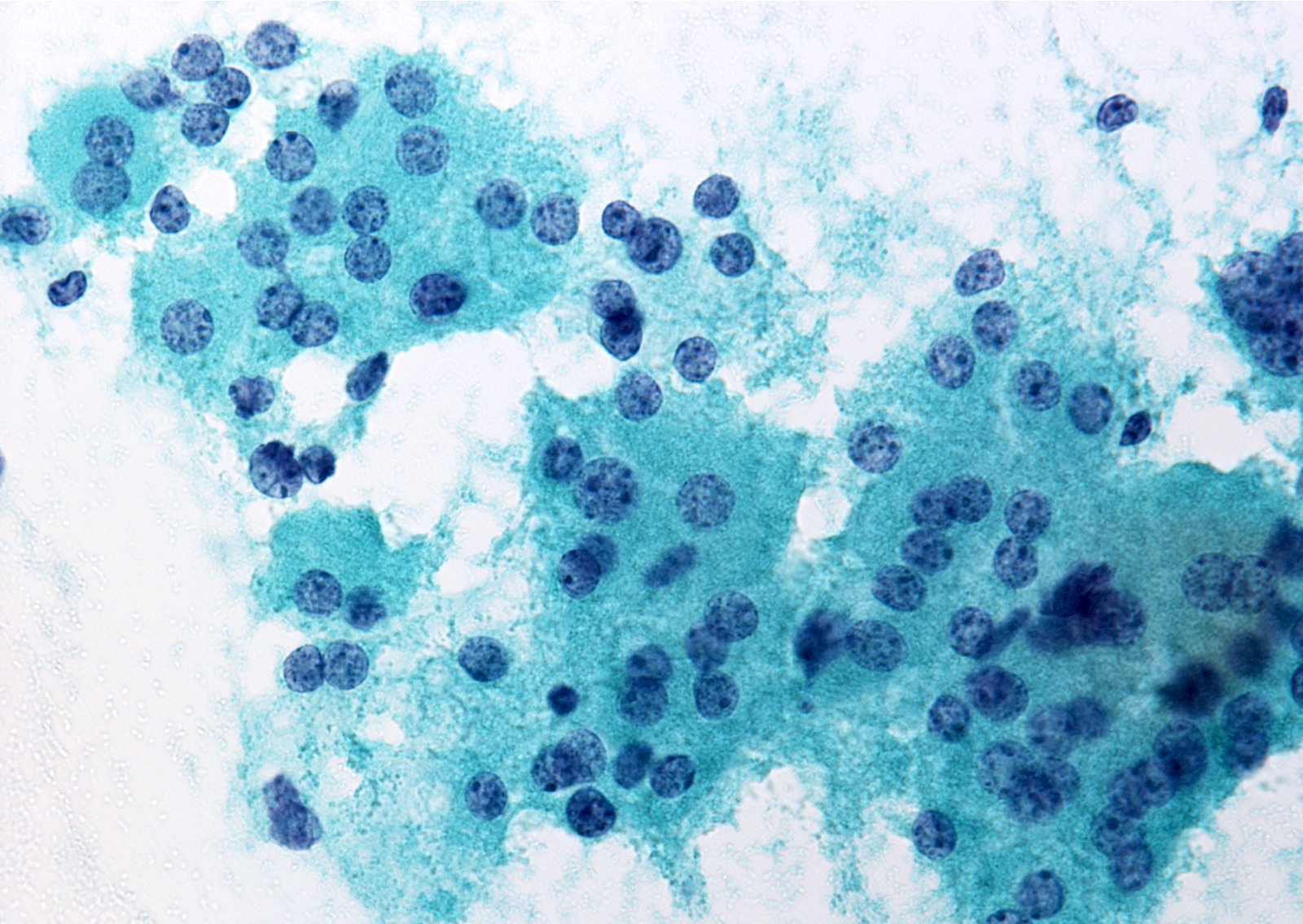
Oncocytes with nuclear enlargement
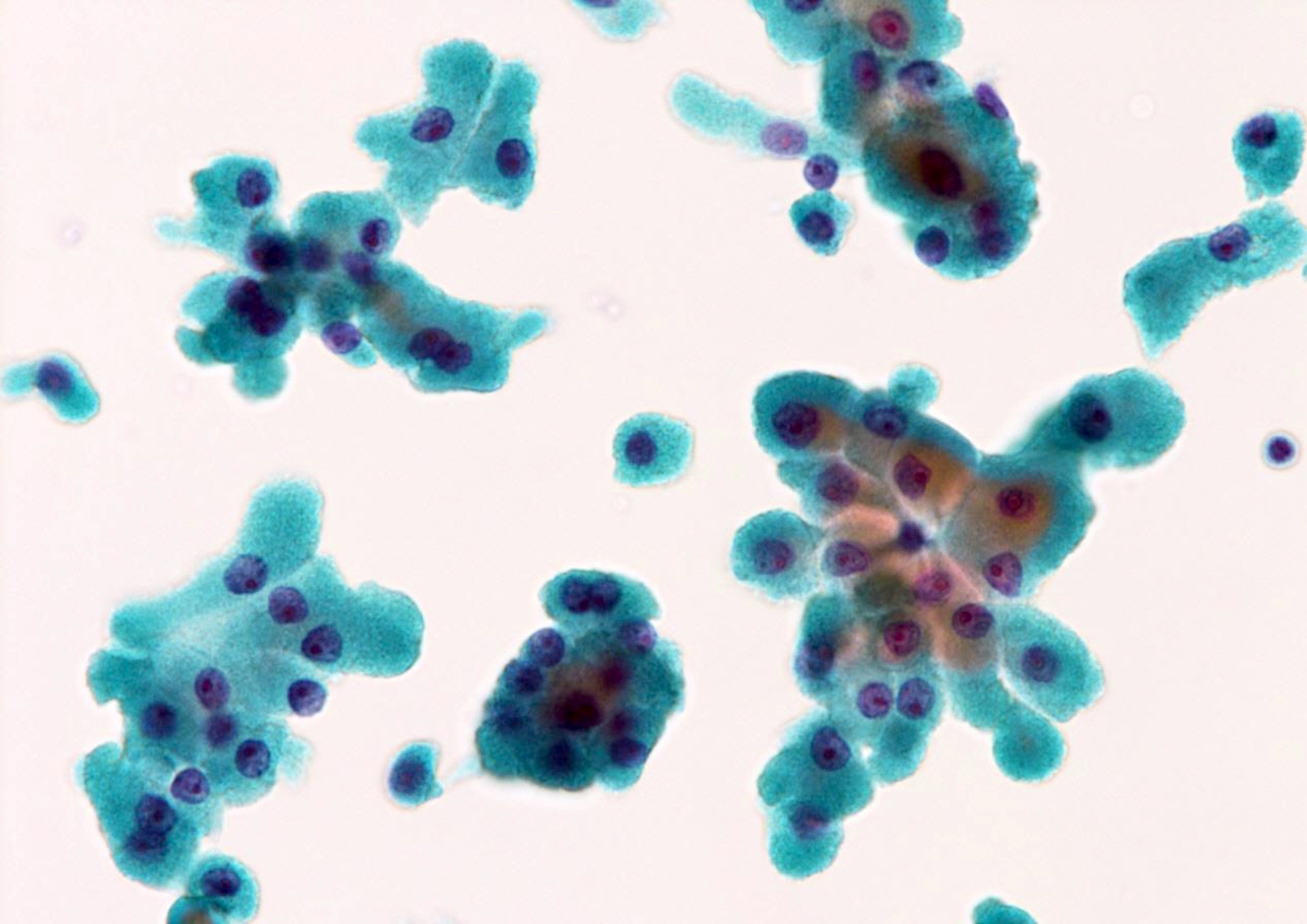
Oncocytic clusters
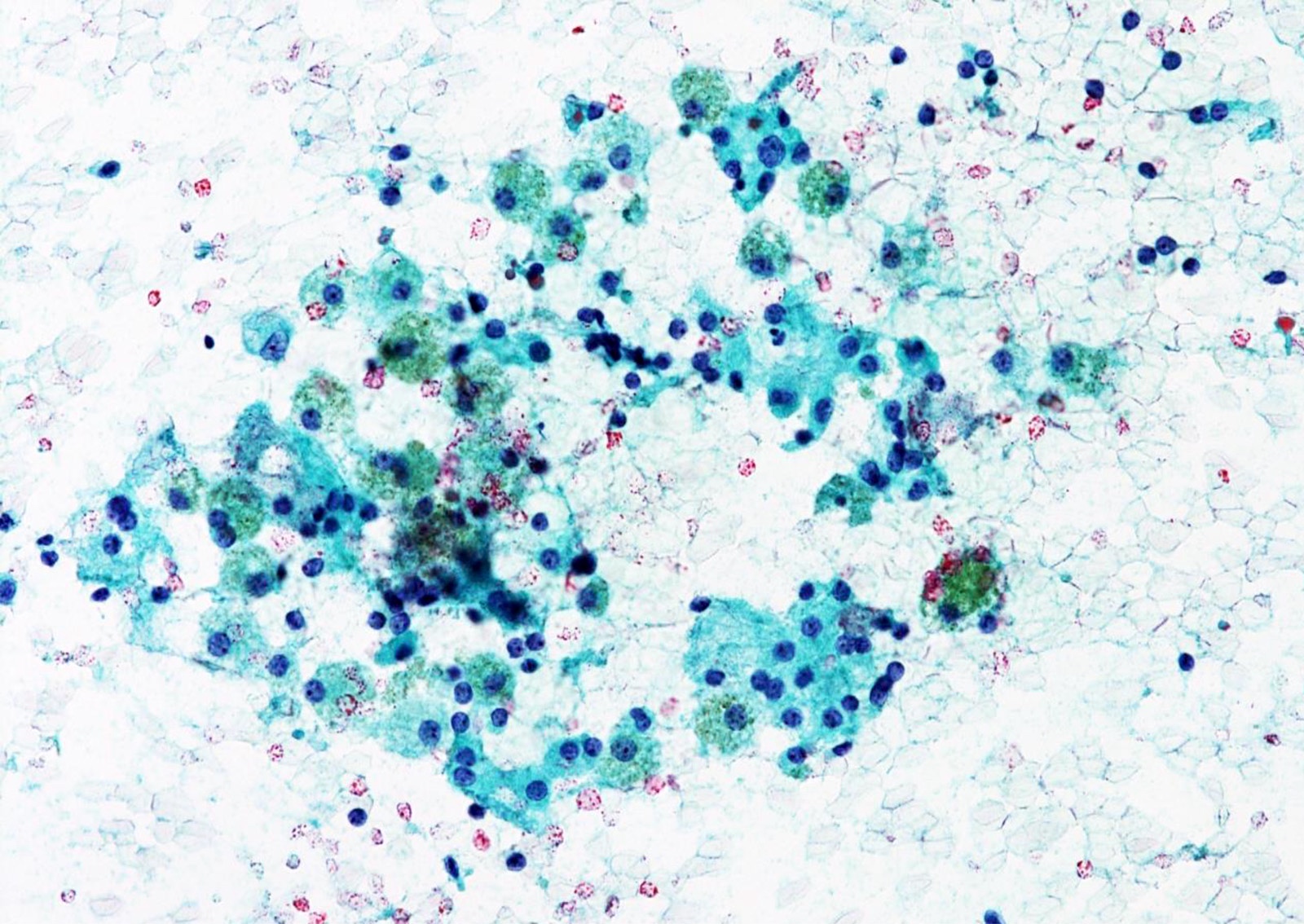
Oncocytes and histiocytes
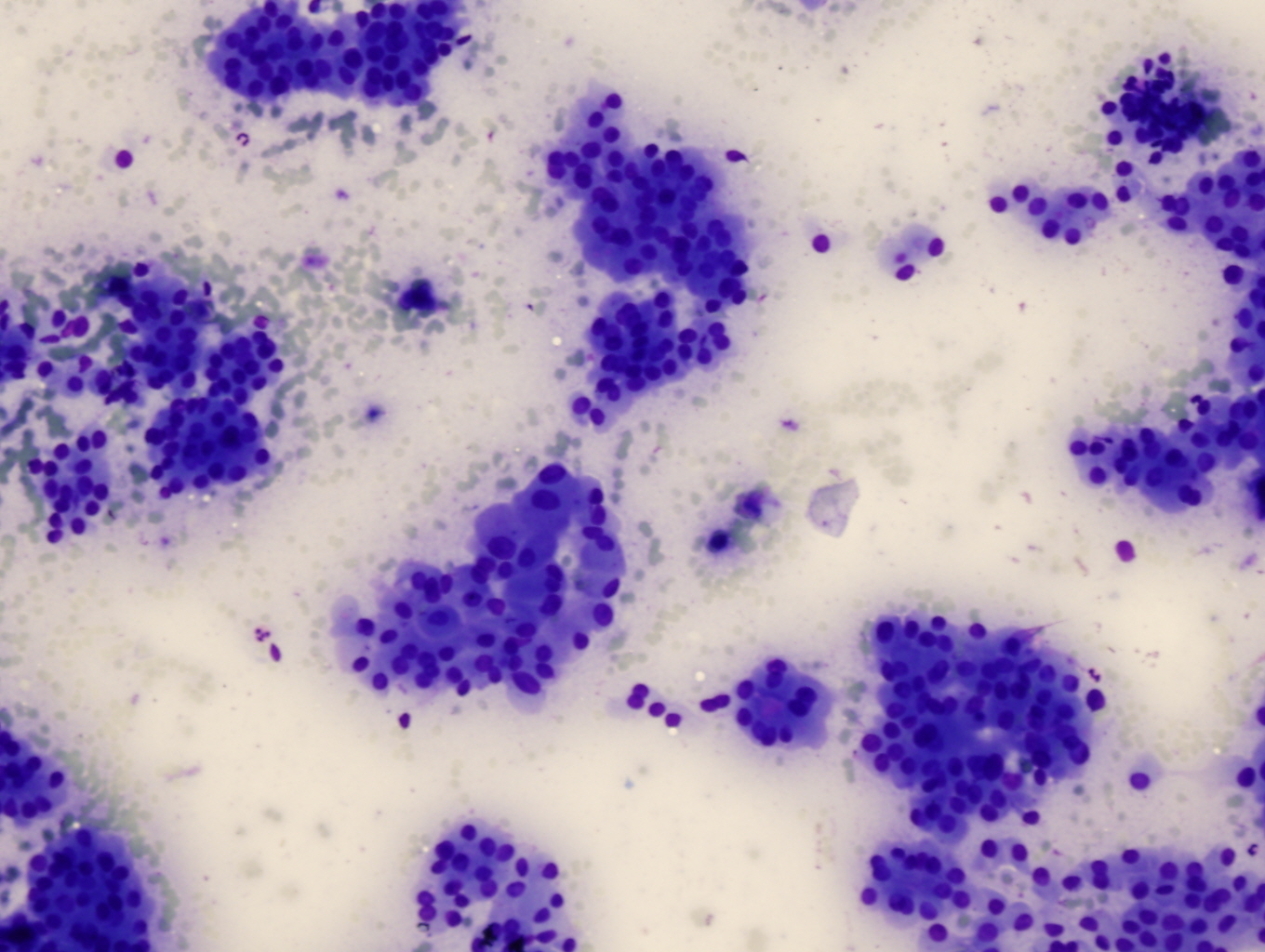
Oncocytic adenoma
(Diff-Quik)
Oncocytic adenoma (Pap stain)
Molecular / cytogenetics description
- Striking morphologic difference between the cytologic patterns of follicular and oncocytic follicular neoplasms
- Follicular and oncocytic carcinomas are genetically different neoplasms (Onco Targets Ther 2016;9:6873)
- Follicular neoplasm: RAS, PAX8::PPARγ rearrangement
- Oncocytic neoplasm: mitochondrial DNA mutation
Videos
Atypical thyroid FNA by Dr. Cibas
Interesting cases by
Dr. Teresa M. Alasio
Oncocytic lesions by Z. Baloch
How to observe thyroid FNA
Sample cytology reports
- Thyroid, ultrasound guided FNA:
- Follicular neoplasm (oncocytic follicular neoplasm) (see comment)
- Comment: Cellular aspirate consisting of abundant isolated oncocytes in the absence of colloid.
- Thyroid, ultrasound guided FNA:
- Suspicious for a follicular neoplasm (oncocytic follicular neoplasm) (see comment)
- Comment: Cellular aspirate of follicular cells with oncocytic features; in addition, occasional nuclear grooves and focal papillary architecture are seen. The findings raise the possibility of a Hürthle cell neoplasm with mild nuclear irregularity but a papillary carcinoma cannot be excluded.
- Thyroid, ultrasound guided FNA:
- Suspicious for a follicular neoplasm (oncocytic follicular neoplasm) (see comment)
- Comment: Cellular aspirate composed of cells with abundant granular cytoplasm. The findings raise the possibility of an oncocytic neoplasm but a parathyroid tumor cannot be excluded. Correlation with clinical findings, imaging and biochemistry might be helpful.
Differential diagnosis
- Follicular nodular disease:
- Flat, cohesive sheets of oncocytes admixed with normal follicular cells and a moderate to abundant amount of colloid (Cancer Cytopathol 2014;122:241)
- Chronic thyroiditis:
- Lymphocytes predominate over oncocytes
- Data suggest that the criteria for FN / OFN have a lower predictive value for malignancy in the setting of chronic thyroiditis (Am J Clin Pathol 2011;135:139)
- Oncocytic variant of papillary carcinoma:
- Nuclear features specific for papillary carcinoma (i.e., nuclear enlargement, pale chromatin, grooves and intranuclear pseudoinclusions)
- A few oncocytic neoplasms exhibit some of the architectural and nuclear features of papillary carcinoma (diagnosed either as FN / OFN or suspicious for malignancy) (Malays J Pathol 2015;37:49)
- Medullary carcinoma:
- Presence of salt and pepper chromatin, intranuclear pseudoinclusions but absence of prominent nucleolus; metachromasia on Romanowsky stains
- Positive for calcitonin and chromogranin, negative for thyroglobulin (Endocr J 2017;64:1099)
- Calcitonin measurement using needle washout fluid is helpful (Endocr J 2017;64:1099)
- Parathyroid adenoma:
- Monomorphous cytoplasm with round nuclei and salt and pepper chromatin
- Positive for GATA3, chromogranin, synaptophysin and parathyroid hormone, negative for thyroglobulin and TTF1 (Endocr J 2016;63:621)
- Parathyroid hormone measurement using needle washout fluid is helpful
- GEC can recognize the expression profile of parathyroid lesions (Diagn Cytopathol 2017;45:526)
- Granular cell tumor (very rare):
Additional references
Practice question #1
Which finding is helpful in distinguishing parathyroid adenoma from an oncocytic neoplasm?
- Calcitonin immunostaining
- Calcitonin measurement using needle washout fluid
- Metachromasia in Romanowsky stain
- Parathyroid hormone (PTH) value measurement using needle washout fluid
- Thyroglobulin measurement using needle washout fluid
Practice answer #1
D. Parathyroid hormone (PTH) value measurement using needle washout fluid is useful when parathyroid lesions are suspected clinically or cytologically. Answers A, B and C are incorrect because these are useful in differentiating oncocytic neoplasm from medullary carcinoma. Answer E is incorrect because thyroglobulin measurement using needle washout fluid is useful to identify if it is a metastasis of follicular cell derived thyroid cancer when aspirated from a nonthyroid nodule.
Comment Here
Reference: Follicular neoplasm (oncocytic follicular neoplasm)
Comment Here
Reference: Follicular neoplasm (oncocytic follicular neoplasm)
Practice question #2
A thyroid FNA shows abundant granular cytoplasm, large round cells and prominent nucleoli. Which of the following is the most likely diagnosis?
- Chronic thyroiditis
- Follicular nodular disease
- Medullary carcinoma
- Oncocytic neoplasm
- Parathyroid adenoma
Practice answer #2
D. Oncocytic neoplasm. The round cells with prominent nucleoli, anisonucleosis and granular cytoplasm are typical features of oncocytic neoplasms, making this the most likely diagnosis in this case. Answer A is incorrect because chronic thyroiditis (e.g., Hashimoto thyroiditis) typically presents with abundant lymphocytes. Answer B is incorrect because follicular nodular disease usually involves a mix of follicular cells with some variation in size but their background has abundant colloid or foamy histiocytes. Answer C is incorrect because medullary carcinoma shows salt and pepper chromatin and does not typically show prominent nucleoli seen in oncocytic neoplasms. Answer E is incorrect because parathyroid adenomas usually present with a uniform population without anisonucleosis.
Comment Here
Reference: Follicular neoplasm (oncocytic follicular neoplasm)
Comment Here
Reference: Follicular neoplasm (oncocytic follicular neoplasm)
