

Bone & joints
Other chondrogenic tumors
Chondroblastoma
Resident / Fellow Advisory Board: Josephine K. Dermawan, M.D., Ph.D.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 18 October 2021
Last staff update: 19 September 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Chondroblastoma
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Patton A, Wakely PE. Chondroblastoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bonechondroblastoma.html. Accessed May 14th, 2024.
Definition / general
- Benign neoplasm; rare (< 1% of primary bone neoplasms), arising in second to third decades of life, with slight male predilection
- Treatment with surgical curettage is generally curative; recurrence varies with location
Essential features
- Rare (< 1% of primary bone neoplasms)
- Peaks in second decade of life, with slight male predilection
- Common location includes epiphysis of long bones > metaphysis; may involve skull in older patients
- Sheets of chondroblasts admixed with osteoclast-like giant cells and eosinophilic chondroid matrix; pericellular chicken wire type calcification may be present
- K36M mutations commonly identified
ICD coding
Epidemiology
- Rare (< 1% of primary bone neoplasms) (Arch Pathol Lab Med 2017;141:867)
- Peaks in second and third decades of life (10 - 25 years of age) (Hum Pathol 1993;24:944)
- Slight male predominance (M:F = 2:1)
Sites
- 75% of cases involve long bones; generally confined to a single bone (Skeletal Radiol 1985;14:1, J Bone Joint Surg Am 1985;67:748)
- Common locations: epiphysis of proximal and distal femur, proximal humerus, proximal tibia; rarely involves the metaphysis (Skeletal Radiol 1985;14:1)
- Other locations: pelvis, ribs, scapula, navicular, carpal bones, patella and skull (Hum Pathol 1993;24:944, Virchows Arch A Pathol Anat Histopathol 1992;421:355)
Pathophysiology
- May arise from cartilage germ cells, epiphyseal cartilage cells or possibly multipotent mesenchymal cell or tendon sheath synovial cell (Eur J Radiol 2007;63:63, Skeletal Radiol 1995;24:220)
Clinical features
- Pain in the affected area (Arch Pathol Lab Med 2017;141:867)
- Joint effusions can occur if involving articular cartilage or synovium
Diagnosis
- Xray (anterior posterior, lateral and oblique views) or MRI; CT scan less common (Acta Orthop Belg 2016;82:68)
- Open surgical biopsy / surgical curettage is frequently performed (Acta Orthop Belg 2016;82:68)
- Fine needle aspiration (FNA) biopsies are less common
Radiology description
- Xray: well defined lucent lesion with a thin sclerotic rim, with or without matrix calcifications, commonly arising eccentrically within the epiphysis of long bones; extension to the metaphysis can be seen (AJR Am J Roentgenol 1977;128:613)
- CT scan: can show matrix calcification and solid periosteal reaction (J Comput Assist Tomogr 1984;8:907)
- MRI: associated with bone marrow edema, periosteal and soft tissue reactions, varying signal intensity on T2 weighted sequences (Skeletal Radiol 2002;31:88)
Radiology images
Contributed by Mark R. Wick, M.D., Borislav A. Alexiev, M.D. and AFIP

Femur Xray

Foot talus Xray

Humerus Xray
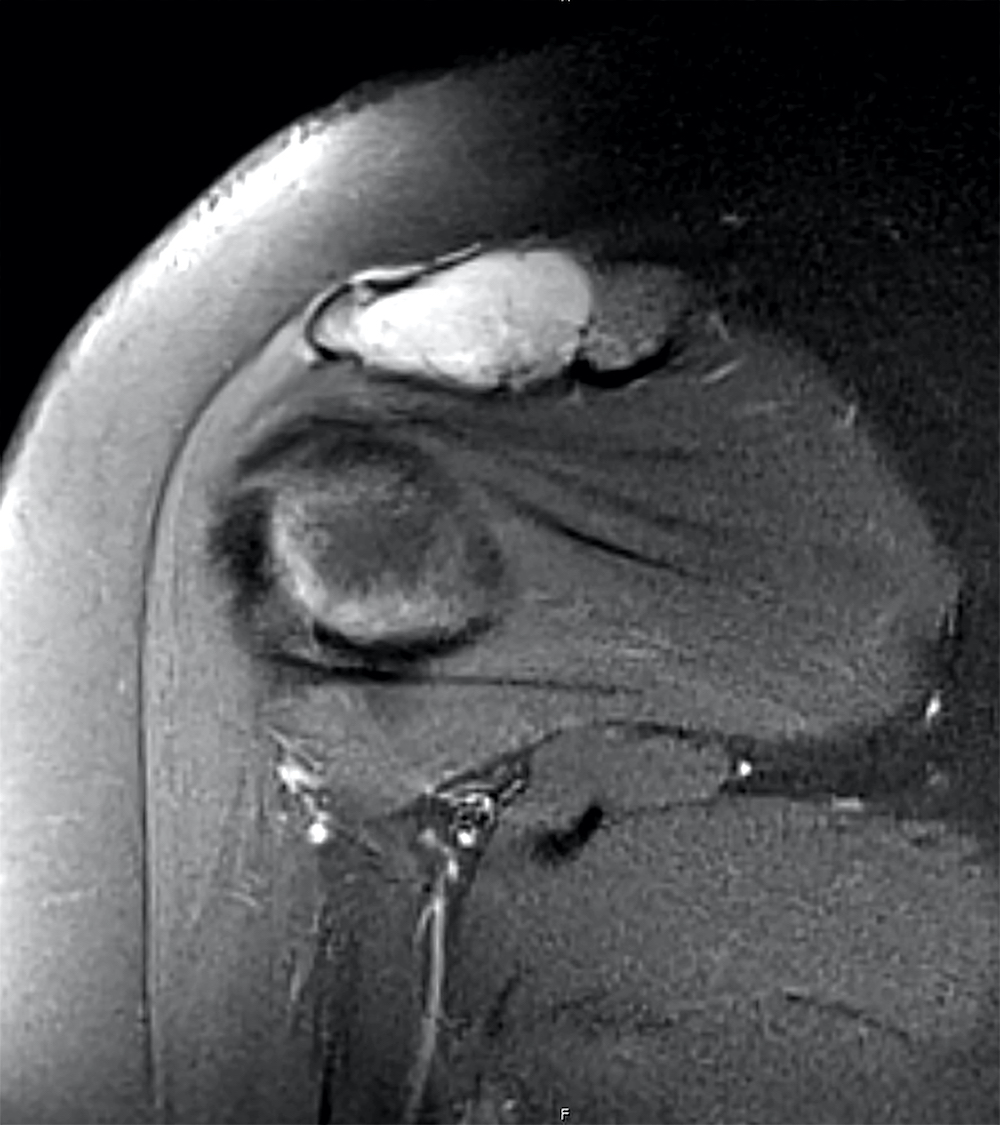
Left acromion lesion

Radiograph of tibia
Prognostic factors
- Can be locally aggressive (Mod Pathol 2020;33:2295)
- Rare lung metastases have been identified (J Pediatr Orthop 2020;40:e894, Pathol Res Pract 1987;182:113)
- Local recurrences vary, depending on location (Acta Orthop Traumatol Turc 2018;52:415)
Case reports
- 11 year old girl with chondroblastoma of distal femur (J Orthop Sports Phys Ther 2020;50:275)
- 17 year old boy with recurrent chondroblastoma of sacrum (World J Clin Cases 2021;9:5709)
- 30 year old man with chondroblastoma of patella with secondary aneurysmal bone cyst (BMC Musculoskelet Disord 2021;22:381)
Treatment
- Excision or curettage, with or without bone grafting, is the mainstay of treatment (Acta Orthop Belg 2016;82:68)
- En bloc resection or amputation is reserved for advanced cases
Gross description
- When resected with bone: usually 3 - 6 cm, well circumscribed, white-blue-gray, firm
- When resected as curetted material: reddish, friable material (Arch Pathol Lab Med 2017;141:867)
- Variable calcification, necrosis, cystic areas
Microscopic (histologic) description
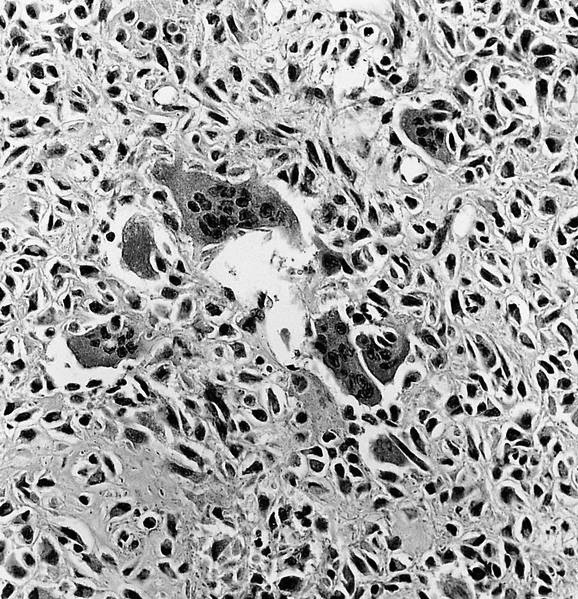
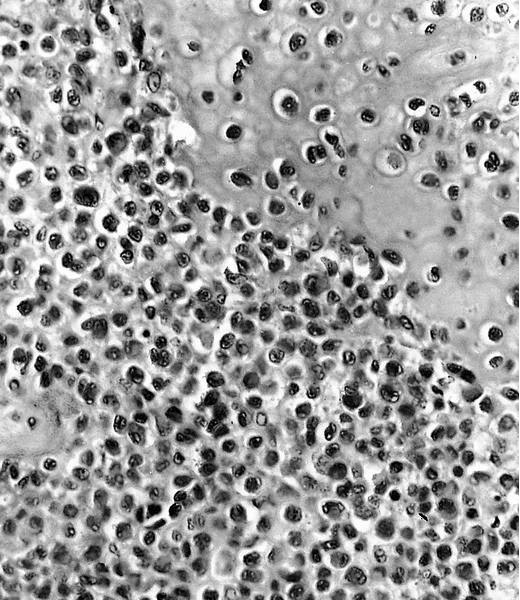
- Composed of round or polyhedral chondroblasts with abundant eosinophilic cytoplasm and well defined cell borders; spindle shaped cells may be focal (Ann Diagn Pathol 2003;7:205, Cancer 1972;30:401)
- Nuclei are oval, hyperlobulated with grooves
- Pericellular lace-like or chicken wire type calcification among degenerative chondroblasts
- Chondroid matrix almost always present (pink rather than blue matrix)
- May have marked cellularity, intracytoplasmic glycogen granules, mitotic figures, necrosis and osteoclast type giant cells
- No significant nuclear atypia as compared with malignant chondroblastoma (Mod Pathol 2020;33:2295)
- Aneurysmal bone cyst-like change is common (Skeletal Radiol 2010;39:583)
Microscopic (histologic) images
Contributed by Ashley Patton, D.O., Ph.D., Nasir Ud Din, M.B.B.S. AFIP and @JMGardnerMD on Twitter
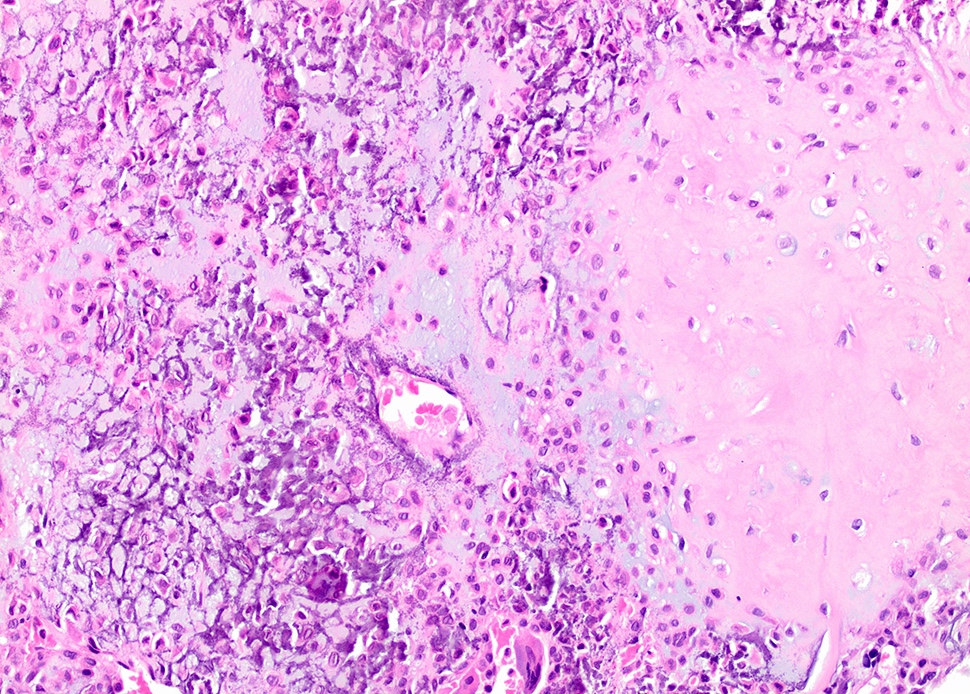
Chicken wire calcification and mature cartilage formation

Osteoclast-like giant cell

Sheets of chondroblasts
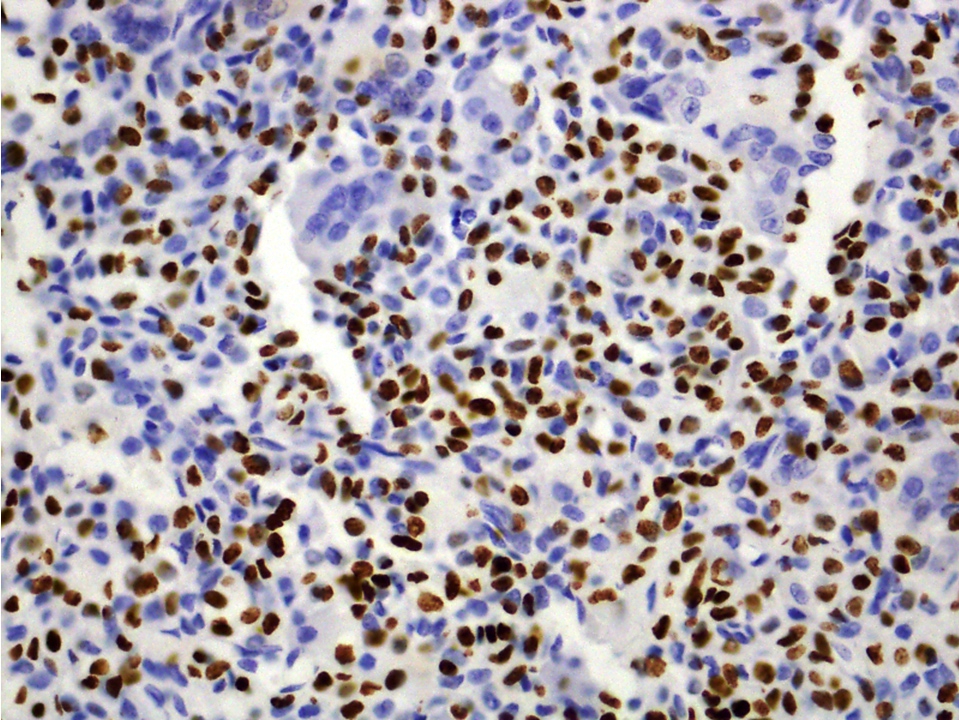
H3K36M antibody
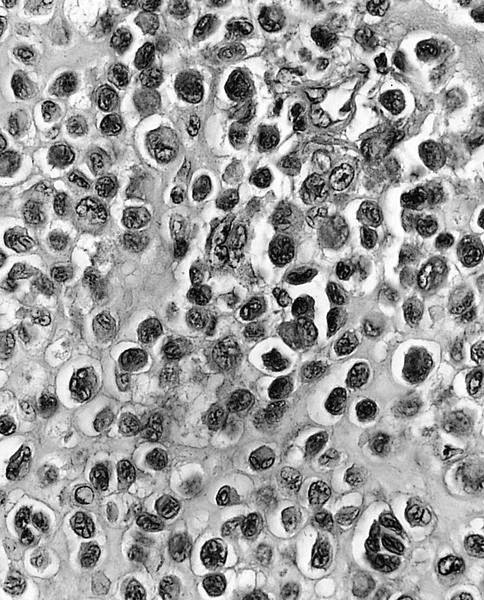
Nuclei vary in size
Neoplastic cells with ovoid to spindled nuclei
Well formed chondroid matrix
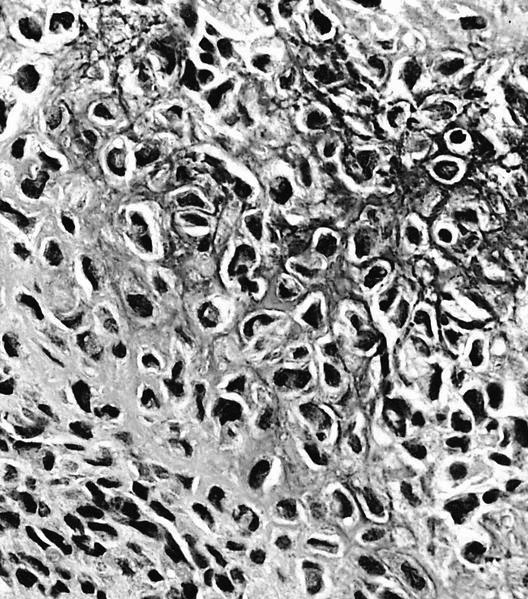
Chicken wire appearance
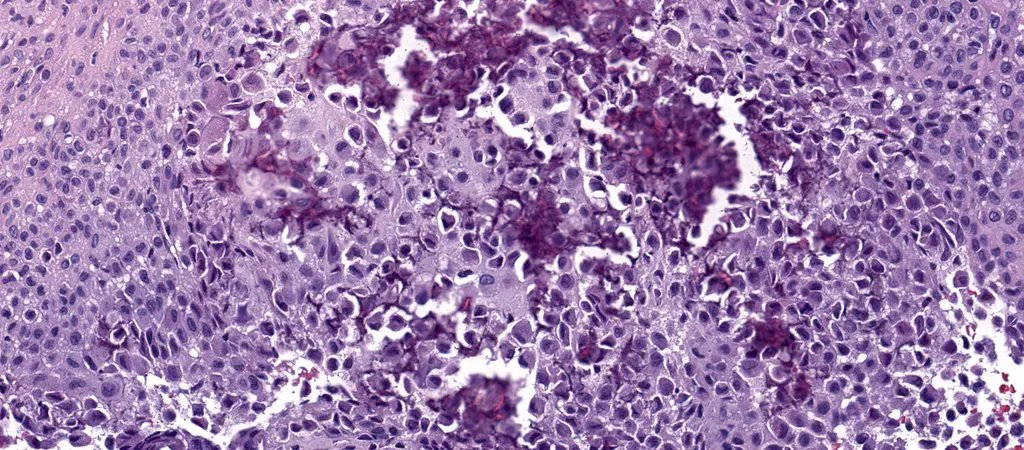
Chondroblastoma
Cytology description
- FNA demonstrates clusters of uniformly round to oval cells with loose matrix and scattered multinucleated giant cells (Cancer Cytopathol 2018;126:552)
Cytology images
Contributed by Borislav A. Alexiev, M.D.
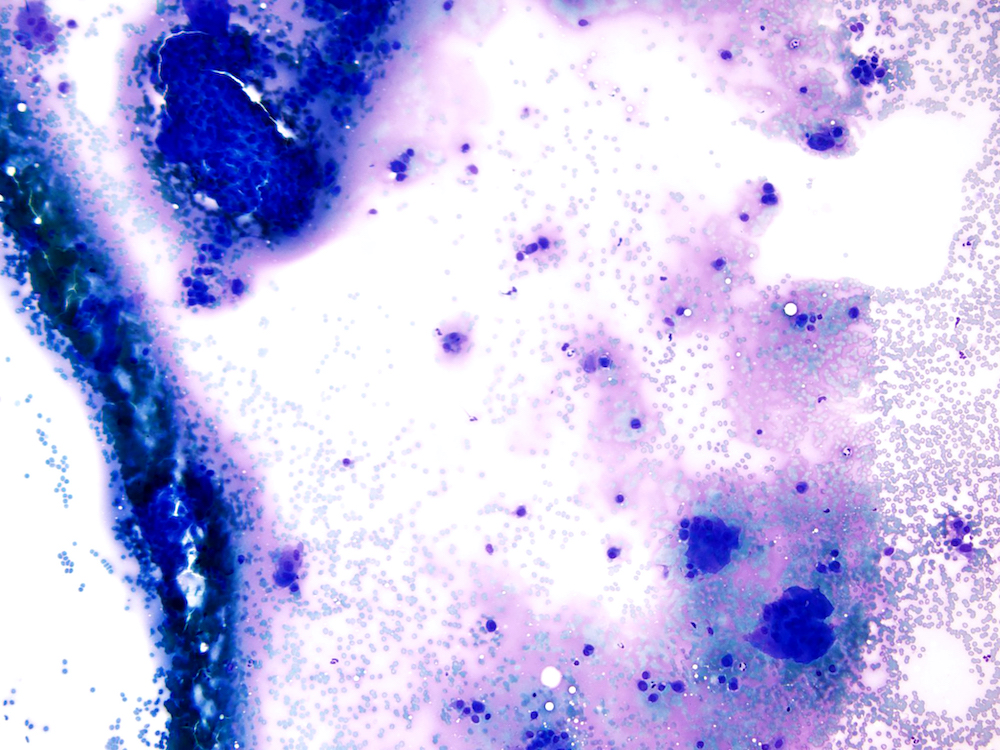
Giant cell rich lesion
Positive stains
- H3.3B (H3F3B) p.Lys36Met (K36M): diffuse nuclear staining may be helpful to distinguish from aneurysmal bone cyst (Cancer Cytopathol 2018;126:552)
- S100, DOG1 (Ann Diagn Pathol 2020;44:151440)
- SOX9 (Hum Pathol 2010;41:208)
Electron microscopy description
- Resembles tissue culture epiphyseal cartilage cells with prominent fibrous lamina that causes microscopic well defined cell borders (Cancer 1972;30:401)
Molecular / cytogenetics description
- K36M mutations commonly identified within H3F3B and rarely in H3F3A (Am J Surg Pathol 2015;39:1576)
Videos
Histological overview of chondrosarcoma
Sample pathology report
- Left femur, resection:
- Chondroblastoma
Differential diagnosis
- Chondromyxoid fibroma:
- Metaphyseal, myxoid with pseudolobular pattern with pleomorphic stellate cells
- Negative for K36M
- Giant cell tumor:
- Metaphyseal or epiphyseal in patients with closed epiphysis (third decade of life), clustered giant cells that are larger and more numerous and uniformly distributed than chondroblastoma, no chondroid matrix or chicken wire matrix
- Negative for K36M
- Aneurysmal bone cyst:
- Primary: multiloculated, blood filled, destructive, cystic lesion; USP6 gene rearrangements
- Secondary: can be associated with chondroblastoma, giant cell tumor, osteoblastoma and osteosarcoma (Clin Imaging 2020;62:23)
- Chondroblastoma-like osteosarcoma:
- Histologically, chondroblastoma-like osteosarcoma is characterized by monotonous, minimally to moderately atypical rounded cells with ovoid nuclei resembling chondroblastoma and abnormal osteoid deposition with destruction of the bone (Arch Pathol Lab Med 2020;144:15, Orthopedics 1999;22:337)
- Negative for H3K36M
Additional references
Board review style question #1
An 18 year old man presents with a 3 cm, well defined lucent lesion within the epiphysis of the distal femur. Microscopic features of the surgical curettage specimen are represented by the H&E images. The best diagnosis is
- Chondroblastoma
- Chondroblastoma-like osteosarcoma
- Chondromyxoid fibroma
- Giant cell tumor of bone
Board review style answer #1
A. Chondroblastoma. Chondroblastomas commonly present in the second decade of life as a singular, well defined lucent lesion within skeletally immature long bones. Characteristic histopathological features include sheets of chondroblasts admixed with osteoclast-like giant cells in a chondroid matrix and focal chicken wire type calcification. Chondroid fibromas typically lack chicken wire type calcification. Chondroblastoma-like osteosarcomas generally display an infiltrative growth pattern with marked cytologic atypia. Chondroid matrix is not commonly seen in giant cell tumor of bone.
Comment Here
Reference: Chondroblastoma
Comment Here
Reference: Chondroblastoma
Board review style question #2
Which of the following is a feature of chondroblastoma?
- Aggressive lesion with an infiltrative growth pattern
- Commonly arises in the epiphysis and metaphysis of long bones
- Generally shows a high degree of cytologic atypia
- Lacks a pericellular chicken wire calcification
Board review style answer #2
B. Commonly arises in the epiphysis and metaphysis of long bones. Chondroblastomas show pericellular chicken wire calcification and generally display well demarcated borders and a lesser degree cytologic atypia when compared with chondroblastoma-like osteosarcoma.
Comment Here
Reference: Chondroblastoma
Comment Here
Reference: Chondroblastoma
