Bladder & urothelial tract
Urothelial neoplasms - noninvasive
Noninvasive papillary urothelial carcinoma high grade
Editorial Board Members: Maria Tretiakova, M.D., Ph.D., Bonnie Choy, M.D.


Last author update: 9 August 2021
Last staff update: 9 August 2021
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: High grade papillary urothelial carcinoma [TIAB]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Yu YHS, Downes MR. Noninvasive papillary urothelial carcinoma high grade. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bladderhgpap.html. Accessed September 14th, 2025.
Definition / general
- Neoplastic proliferation of the urothelium with a papillary configuration and no invasion beyond the basement membrane
- Moderate to marked architectural and cytologic atypia
Essential features
- Noninvasive papillary urothelial neoplasm with moderate to marked cytoarchitectural abnormality
- Complex solid to fused papillary architecture, nuclear atypia, pleomorphism (may be focal), crowded and overlapping cells, brisk mitotic activity
- Immunohistochemistry not required for diagnosis
- Commonly presents with hematuria
- High rate of progression to invasion
Terminology
- Current 2016 WHO Classification: high grade
- Prior / older terminology - 1973 WHO classification: grade 2 and 3
- Overlap between WHO 1973 (grade 1, 2 and 3) and 2004 (low / high grade) nomenclatures
ICD coding
- ICD-O: 8130/2 - papillary transitional cell carcinoma, noninvasive
Epidemiology
- M:F = 6 - 8:1
- Median age: 70 years
Sites
- Most commonly found in posterior and lateral walls of bladder but may be found anywhere within urothelium
- 85% of urothelial neoplasms of renal pelvis are papillary and 66% of them are high grade (Mod Pathol 2005;18:11)
Pathophysiology
- Normal urothelium develops hyperplasia, dysplasia or carcinoma in situ as it acquires further genetic alterations: loss of chromosome 9, activating mutations in FGFR3 or RAS (Int J Clin Oncol 2008;13:287)
- Other mutations: PIK3CA, loss of 11p, CCND1, p53
Etiology
- Smoking (Int J Epidemiol 2016;45:857)
- Occupational exposure to chlorinated hydrocarbons, polycyclic aromatic hydrocarbons and aromatic amines (Eur Urol 2014;66:59)
- Arsenic exposure (Cancer Epidemiol Biomarkers Prev 2014;23:1529)
Clinical features
- Painless, intermittent hematuria
- Gross hematuria associated with more advanced pathologic stage (BJU Int 2016;117:783)
- Pure high grade carcinomas more aggressive than mixed high and low grade
- High rate of progression to invasive disease
Diagnosis
- Cystoscopy: exophytic lesion, solitary or multiple, with varying size
- Imaging: CT urography or ultrasound
- Urine cytology
Radiology description
- CT urography shows hydronephrosis and filling defects (Abdom Radiol (NY) 2018;43:663)
- Ultrasound can detect hydronephrosis and any intraluminal bladder masses
Prognostic factors
- WHO / ISUP histologic grade
- Nuclear anaplasia: decreased time to recurrence and progression
- Concomitant urothelial carcinoma in situ: higher recurrence rate
- Multifocal disease: higher disease associated mortality and progression
- High Ki67 poor prognosis (Int J Mol Sci 2018;19:2548)
- PTEN deletions: increased recurrence rate (Virchows Arch 2018;472:969)
- TP53 and RB alternations: adverse histopathological parameters (Anticancer Res 2018;38:3985)
Case reports
- 64 year old woman with high grade noninvasive papillary urothelial carcinoma develops Poncet disease (rare, nondestructive parainfective symmetric polyarthritis) after intravesical Bacillus Calmette-Guérin treatment (BMC Res Notes 2017;10:416)
- 69 year old woman with high grade noninvasive urothelial carcinoma of bladder later metastatic to uterus (Int J Gynecol Pathol 2017;36:493)
- 24 cases of noninvasive urothelial carcinoma of bladder with glandular differentiation (Am J Surg Pathol 2009;33:1241)
Treatment
- Surgical: transurethral resection of tumor
- Adjuvant therapy:
- Intravesical immunotherapy with Bacillus Calmette-Guérin
- Intravesical chemotherapy with thiotepa or mitomycin C
Gross description
- Exophytic single or multiple lesions with variation in size
- More likely nontranslucent and hyperemic than low grade lesions
Frozen section description
- Papillary architecture with nuclear pleomorphism, dyscohesion and mitotic activity
Microscopic (histologic) description
- Fibrovascular cores lined by neoplastic urothelium
- Complex, solid to fused papillae common
- Architectural disorder; nuclear pleomorphism readily visible at low and intermediate power
- Crowded overlapping cells, dyscohesion common and partial denudation
- Nucleomegaly present, irregular and clumped chromatin
- Frequent prominent nucleoli and mitoses (brisk and maybe atypical)
- Concomitant low grade carcinoma may be present
- Inverted growth pattern may coexist (both exophytic and endophytic growth)
- Reference: Mod Pathol 2009;22:S60
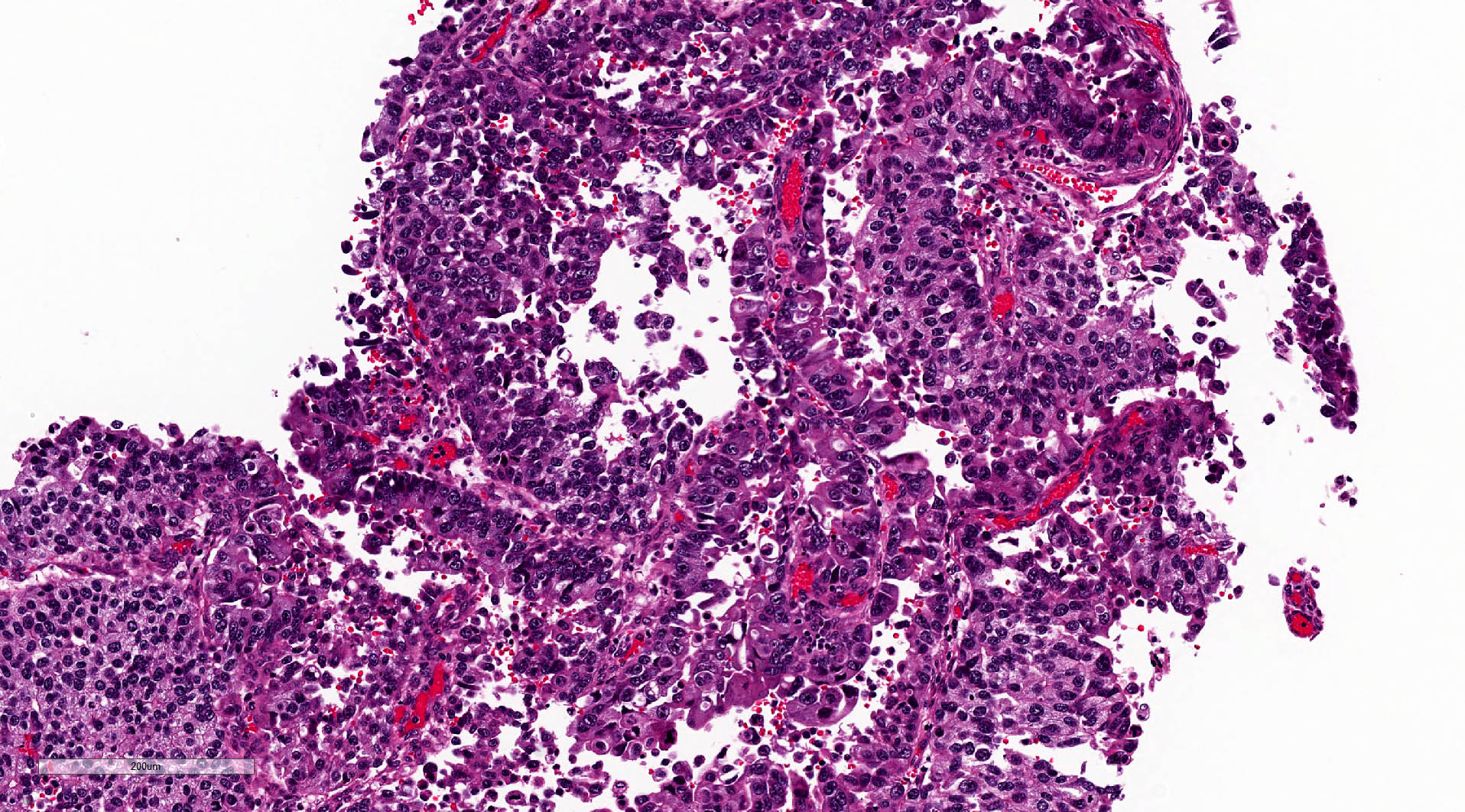
Microscopic (histologic) images
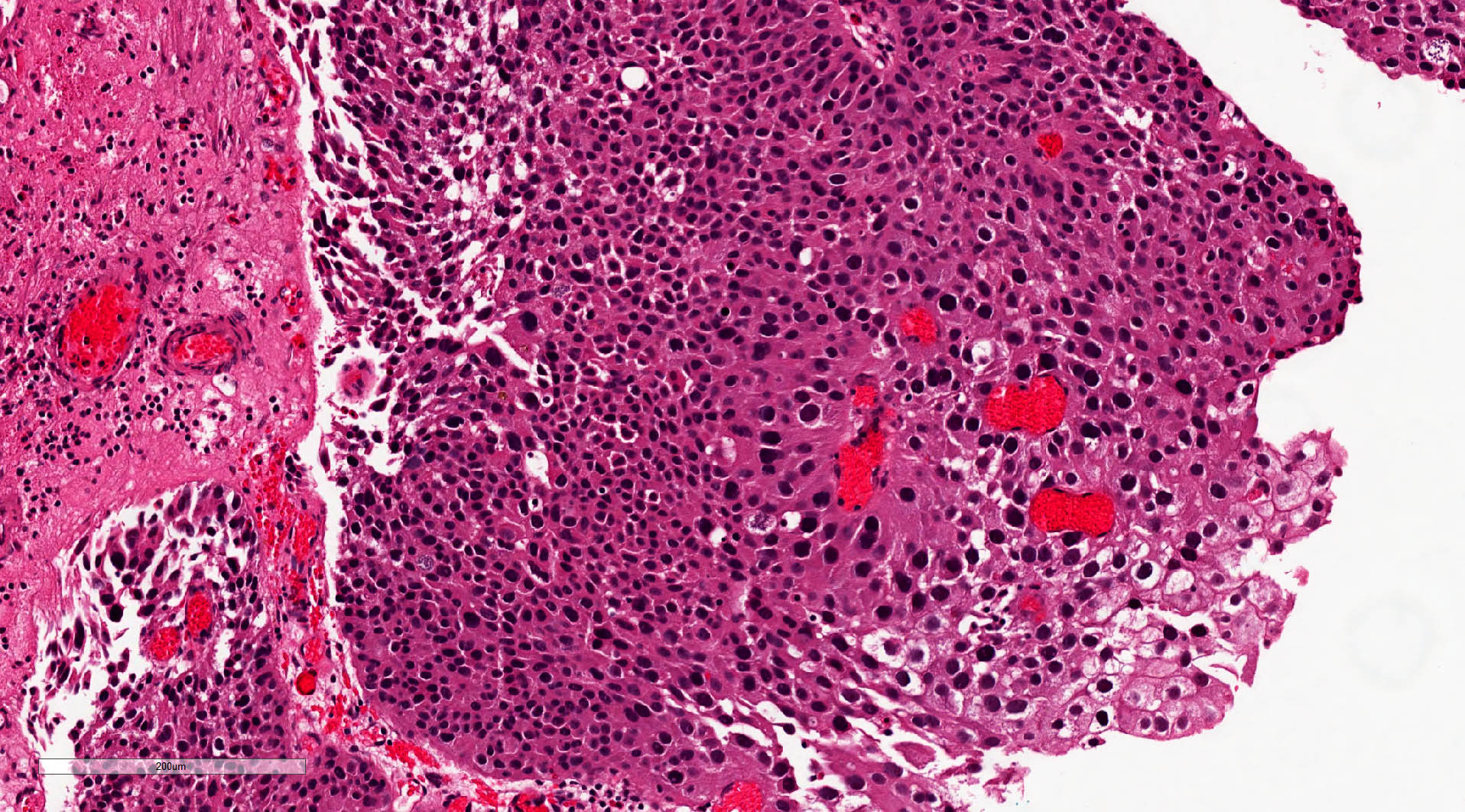
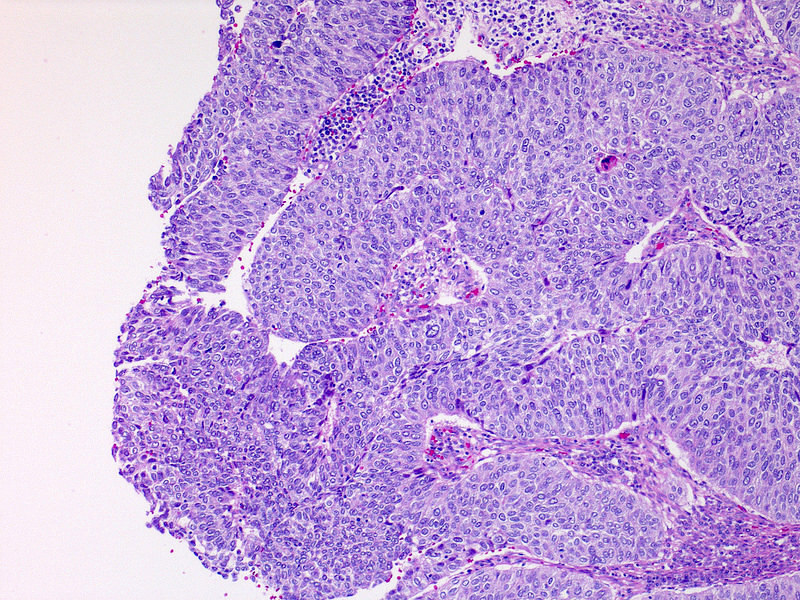
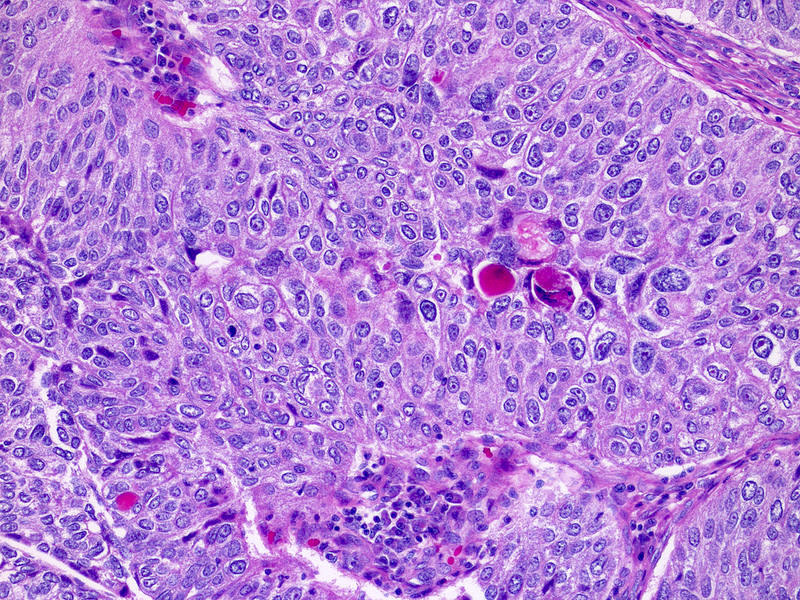
Contributed by Michelle R. Downes, M.D., Nicole K. Andeen, M.D. and Maria Tretiakova, M.D.
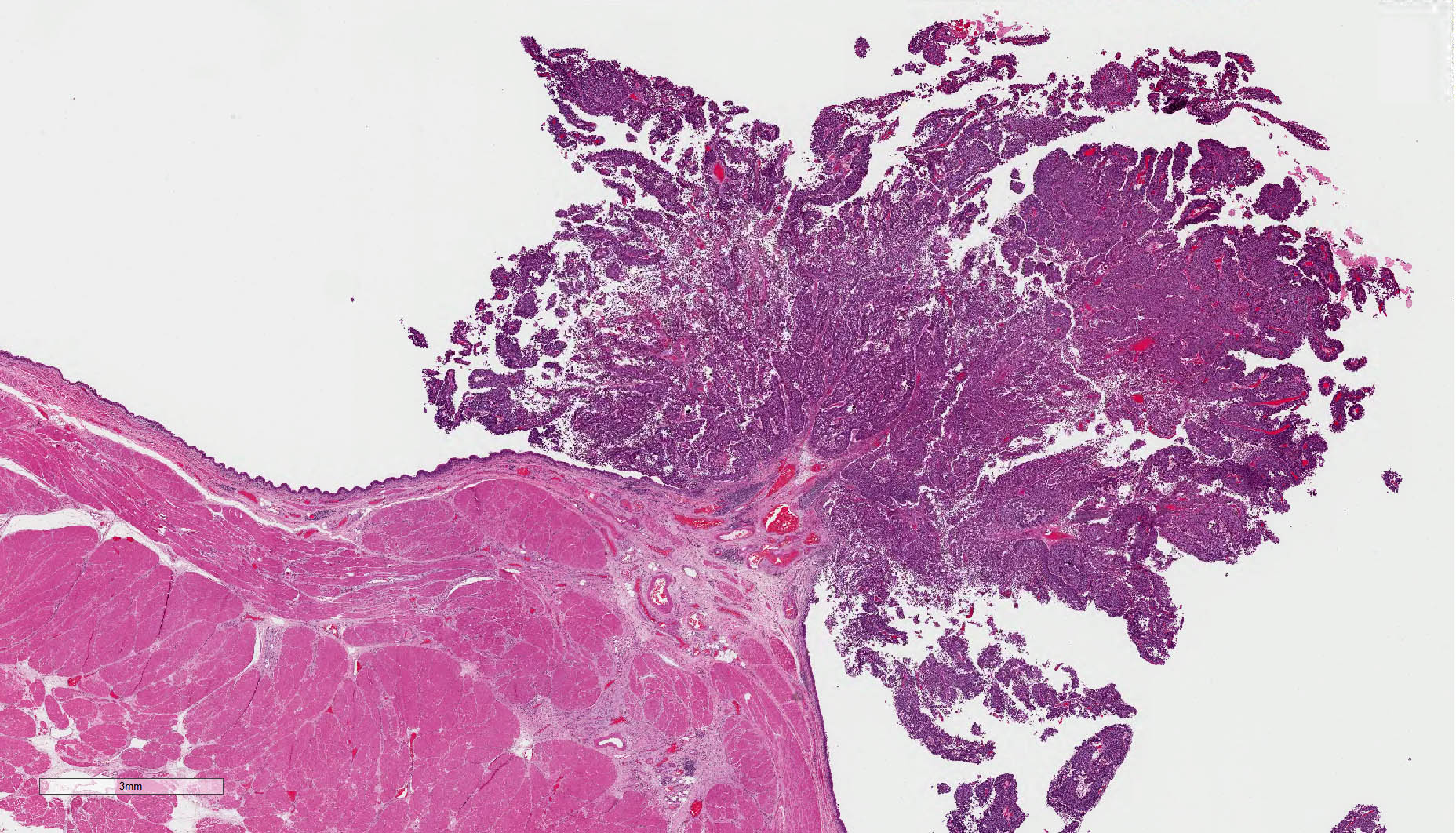
Cystectomy section
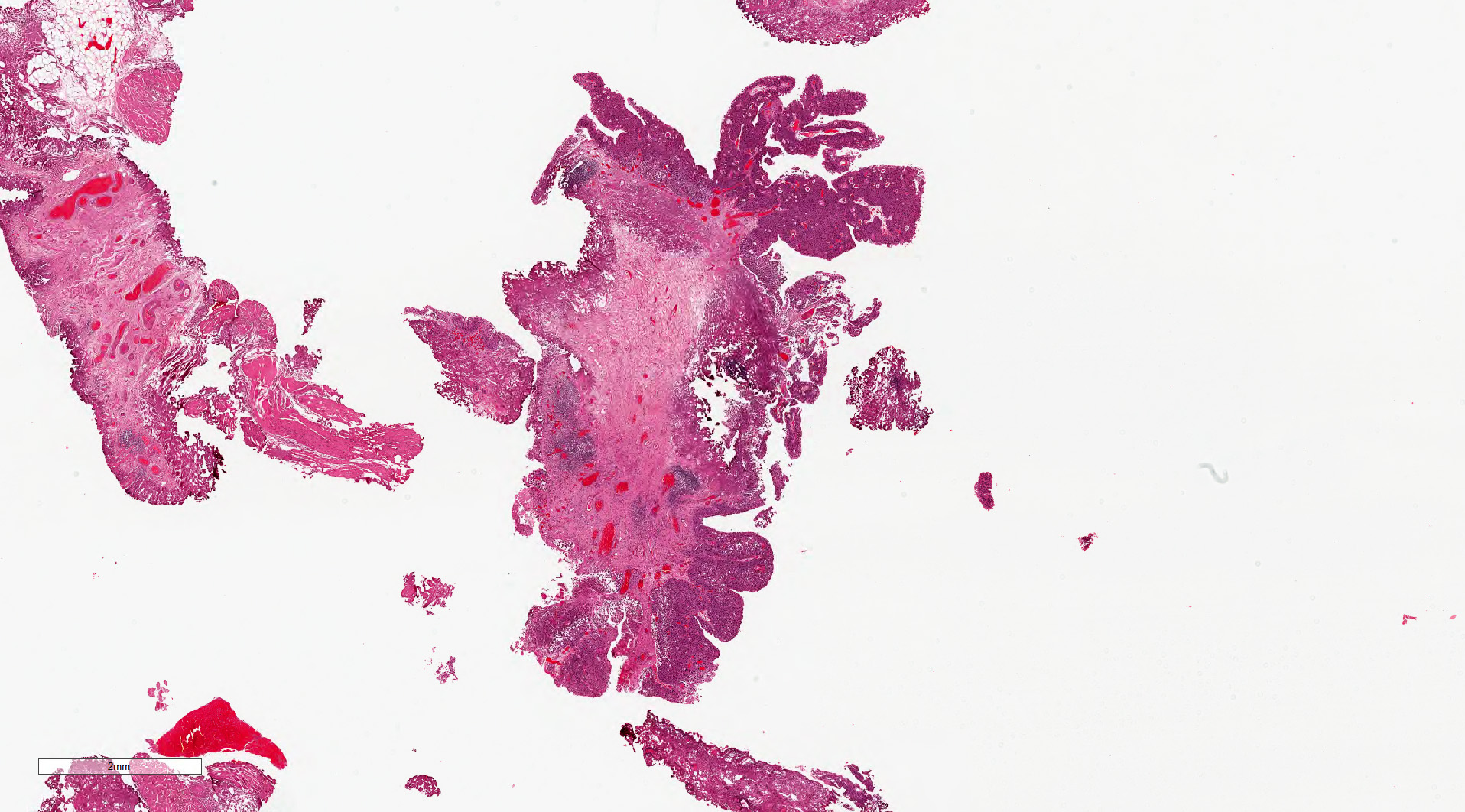
Transurethral bladder resection
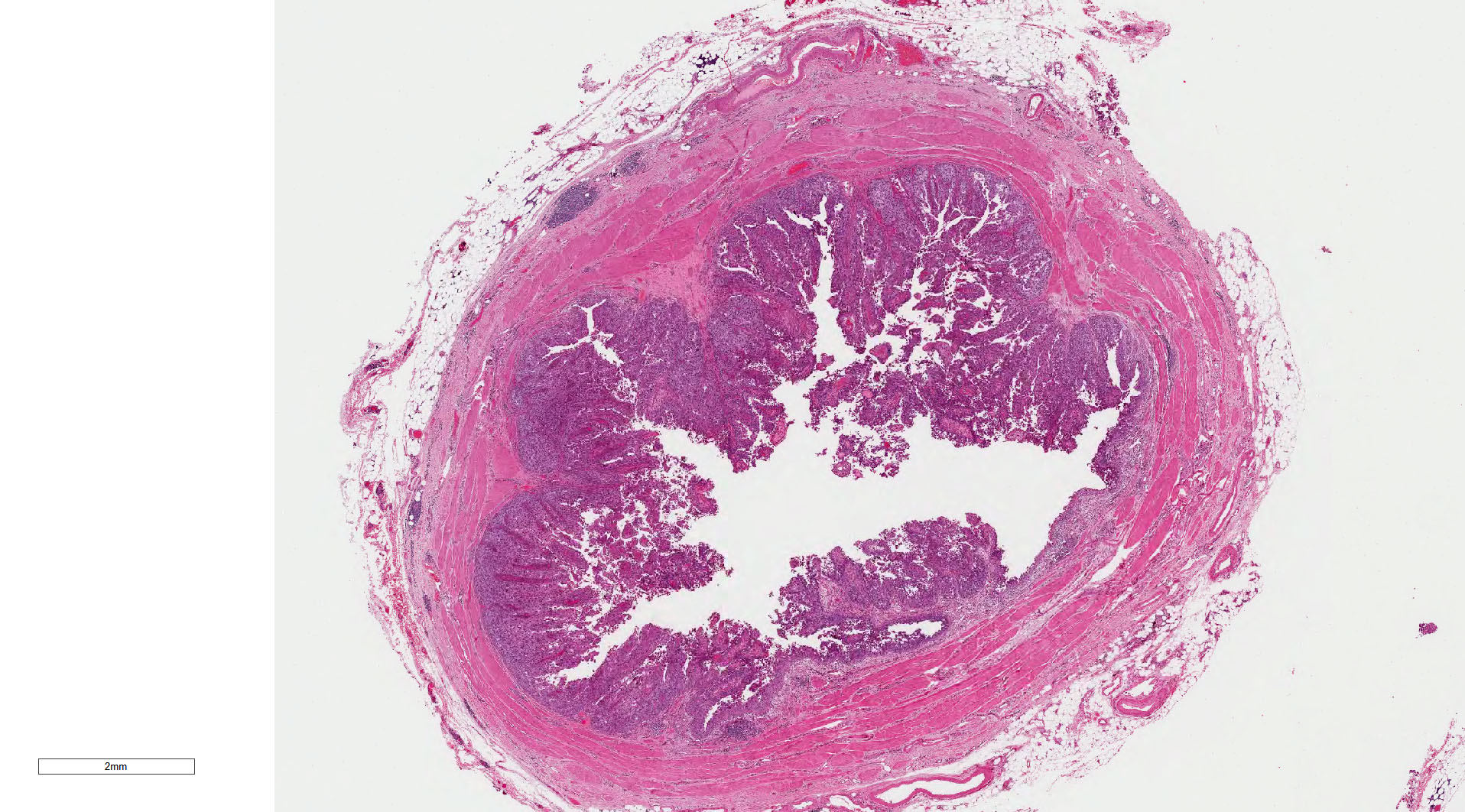
Cross section of ureter
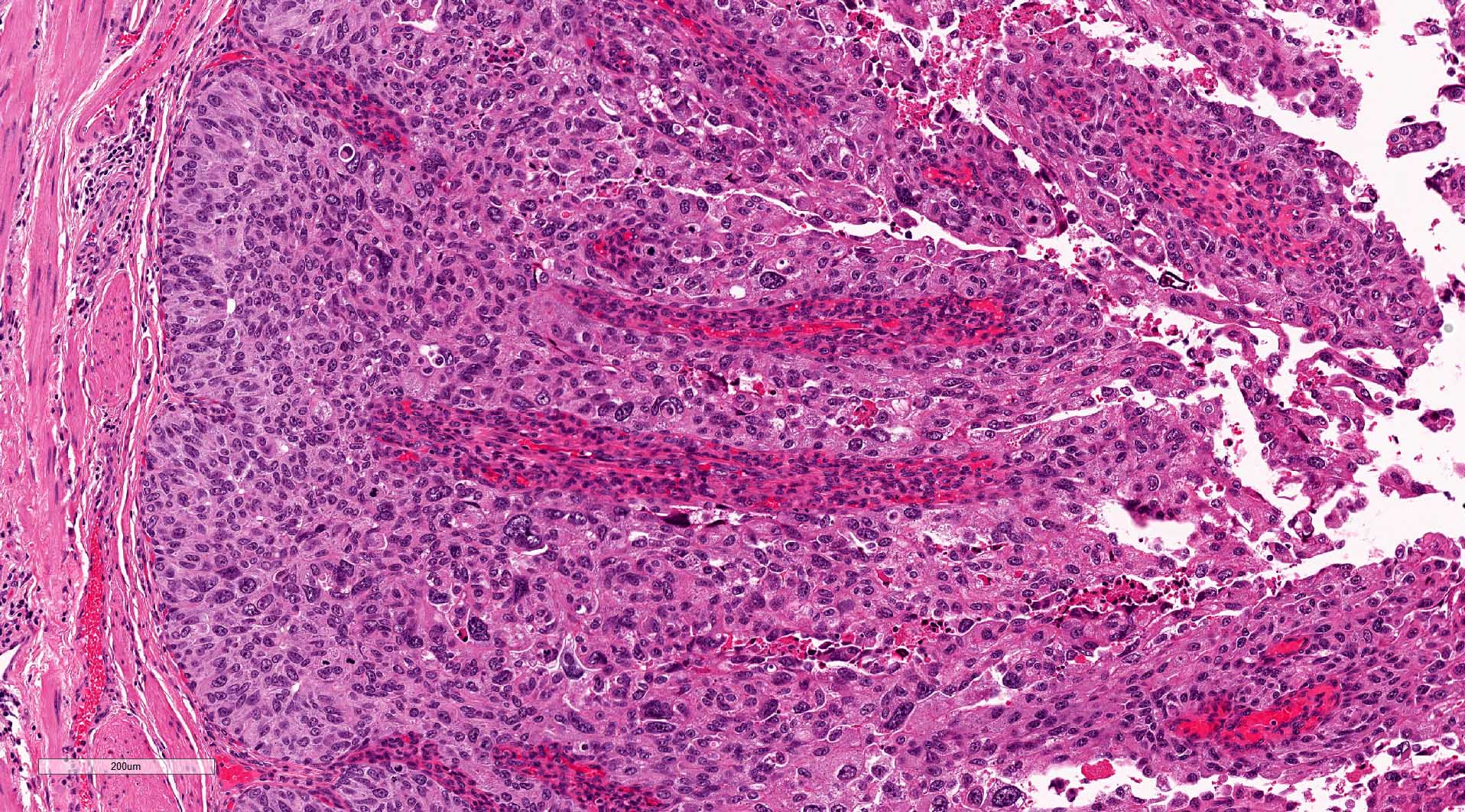
Architecture and cytology
Cytologic features
Noninvasive papillary urothelial carcinoma, high grade (pTa)
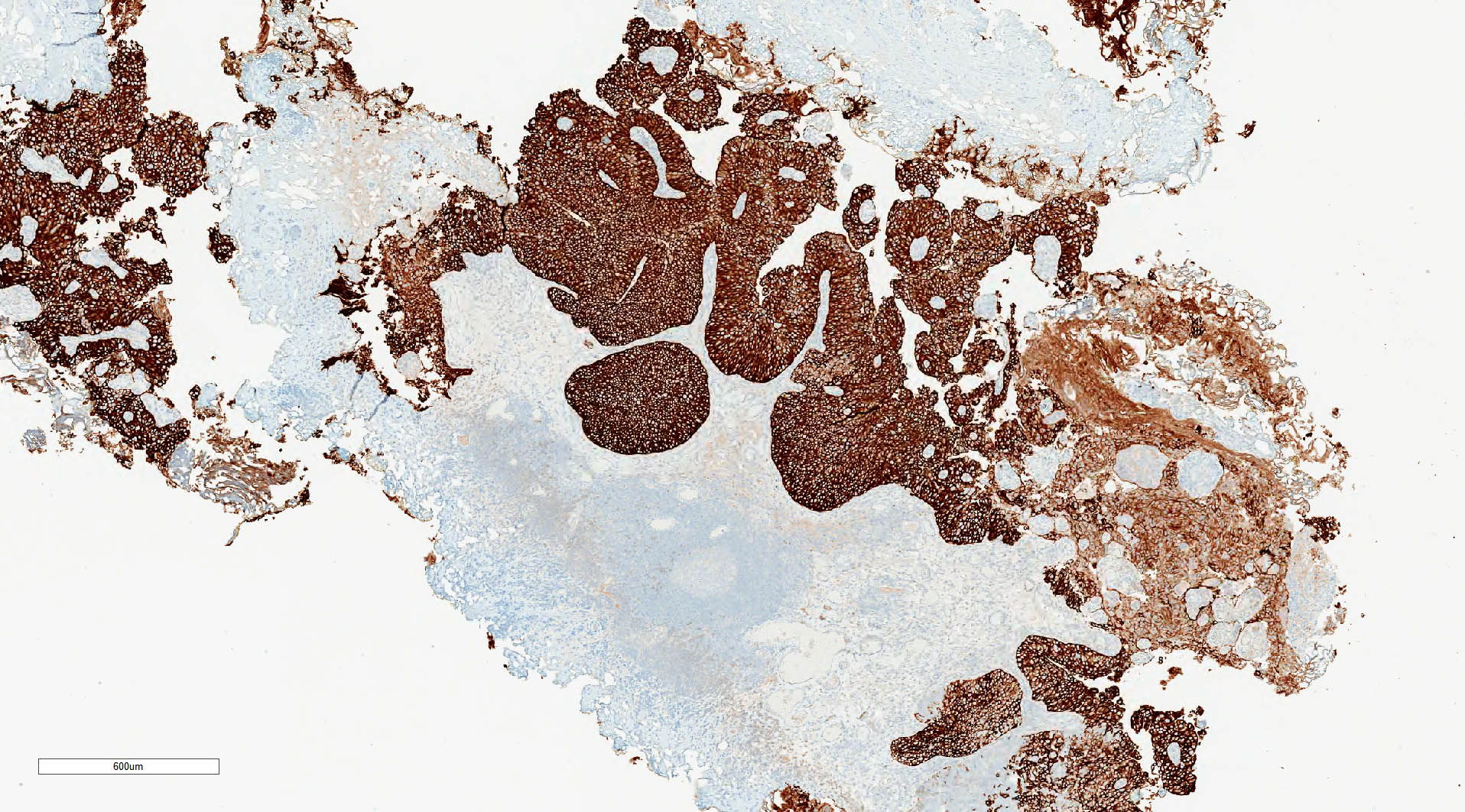
CK7 expression
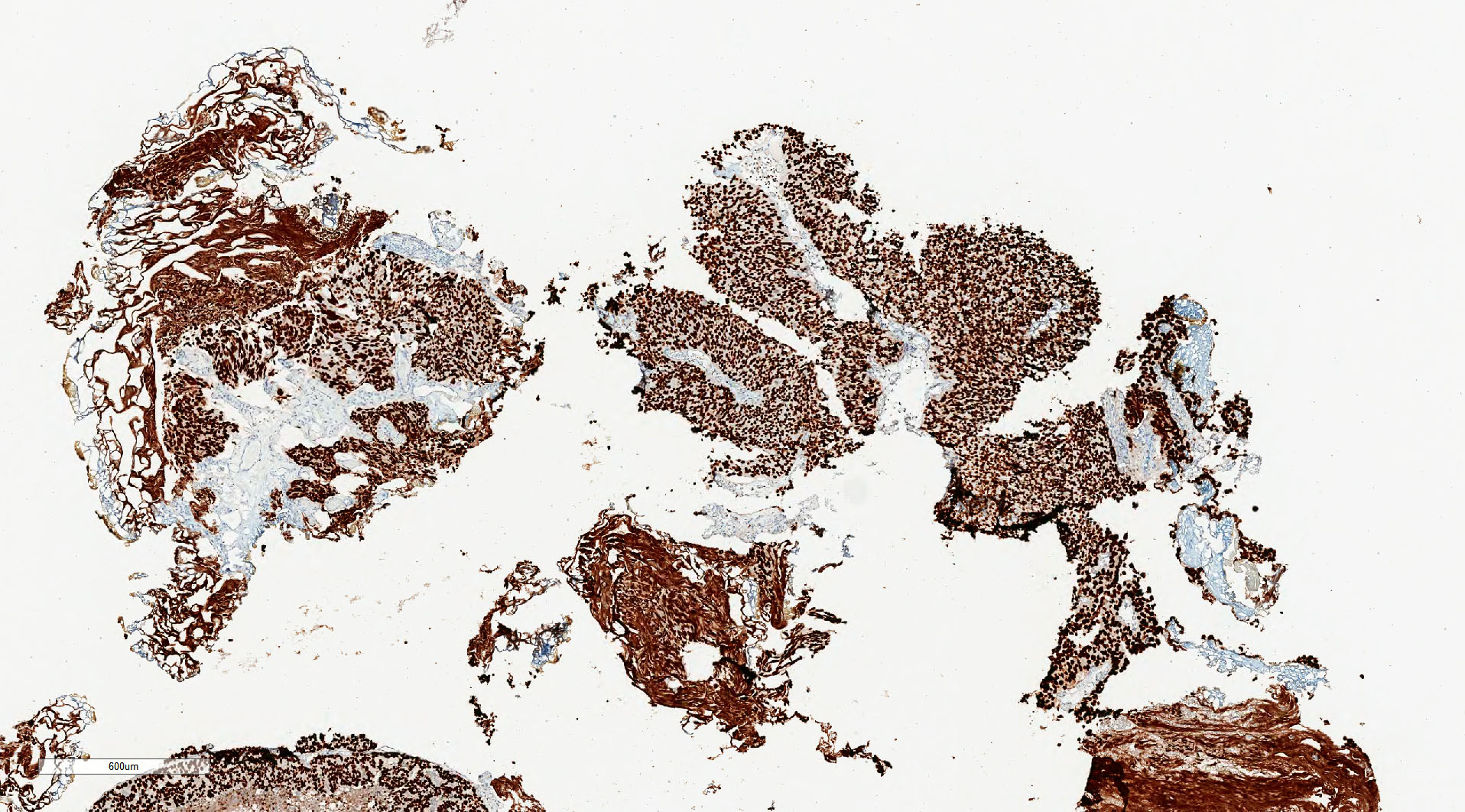
GATA3 expression
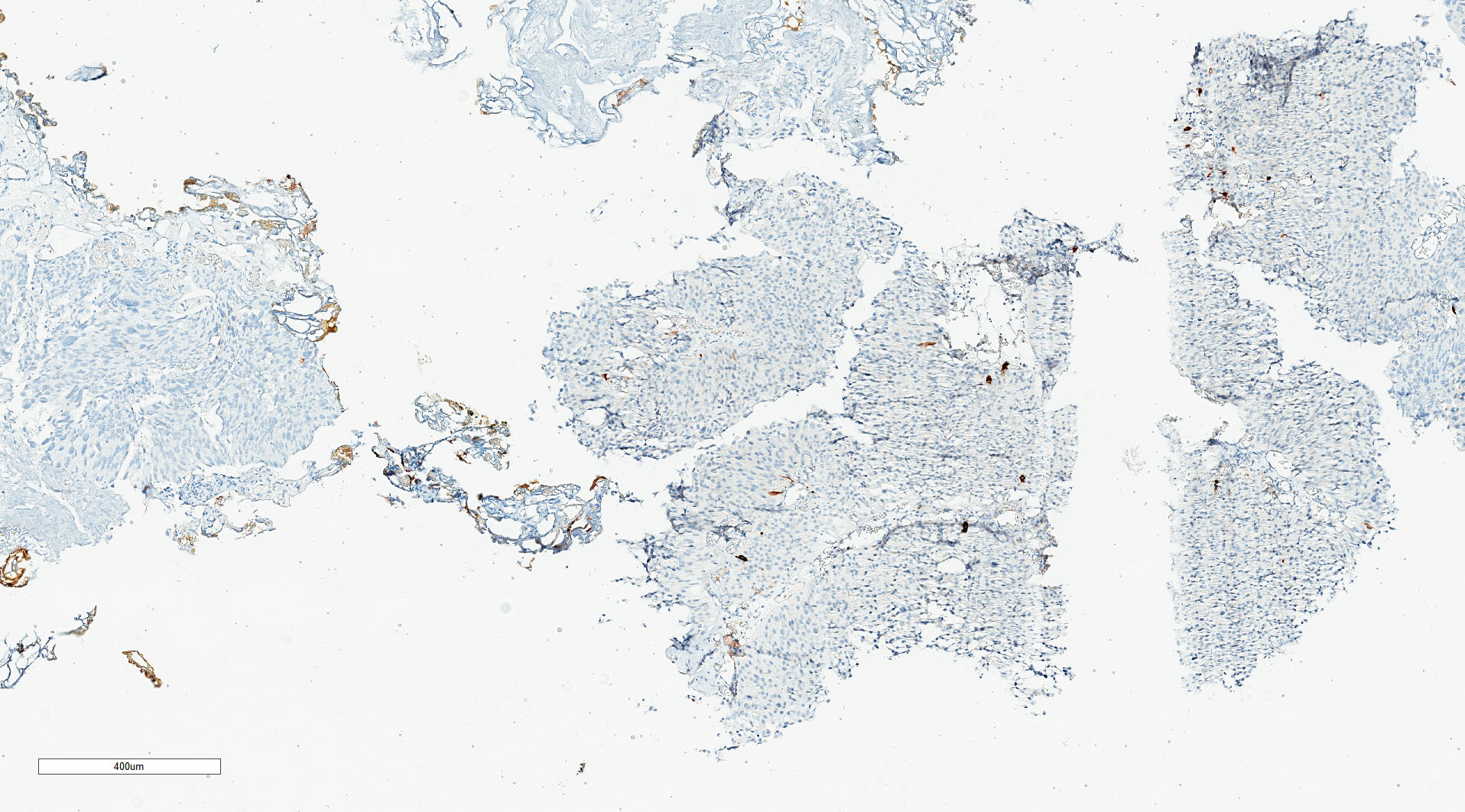
CK5/6 loss
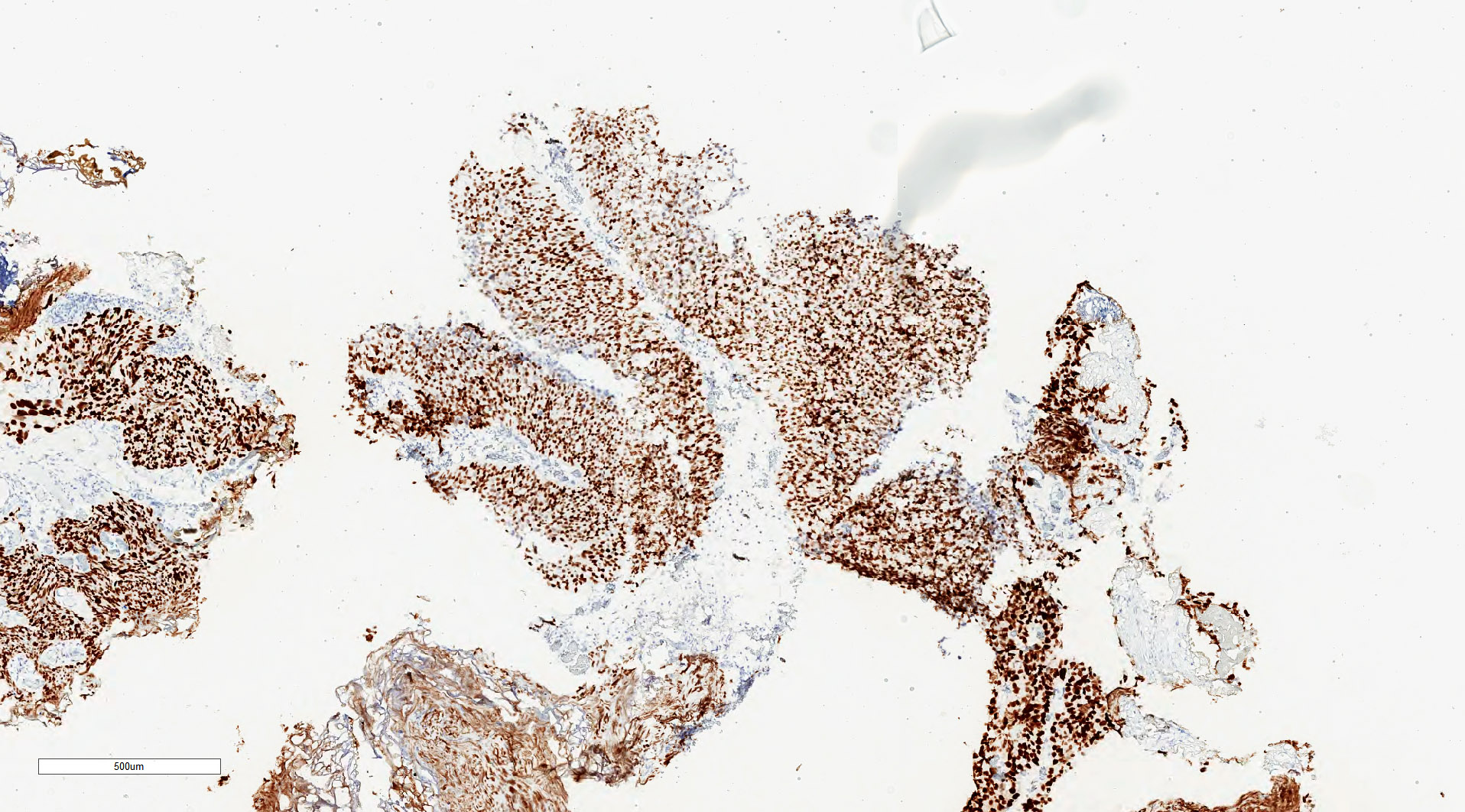
p53
Cytology description
- Moderate / severe nuclear hyperchromasia, irregular nuclear membrane, coarse chromatin, nuclear/cytoplasmic ratio ≥ 0.7; mitoses and necrotic debris may be present
- Cytology cannot distinguish invasive from noninvasive high grade or carcinoma in situ
- Shows high sensitivity (up to 84%) for high grade tumors (Urol Oncol 2015;33:66.e25)
- Use of 2016 Paris Working Group Reporting system recommended (Acta Cytol 2016;60:185)
Cytology images
Contributed by Zeina Ghorab, M.D. and Bonnie Choy, M.D.

High grade cytology
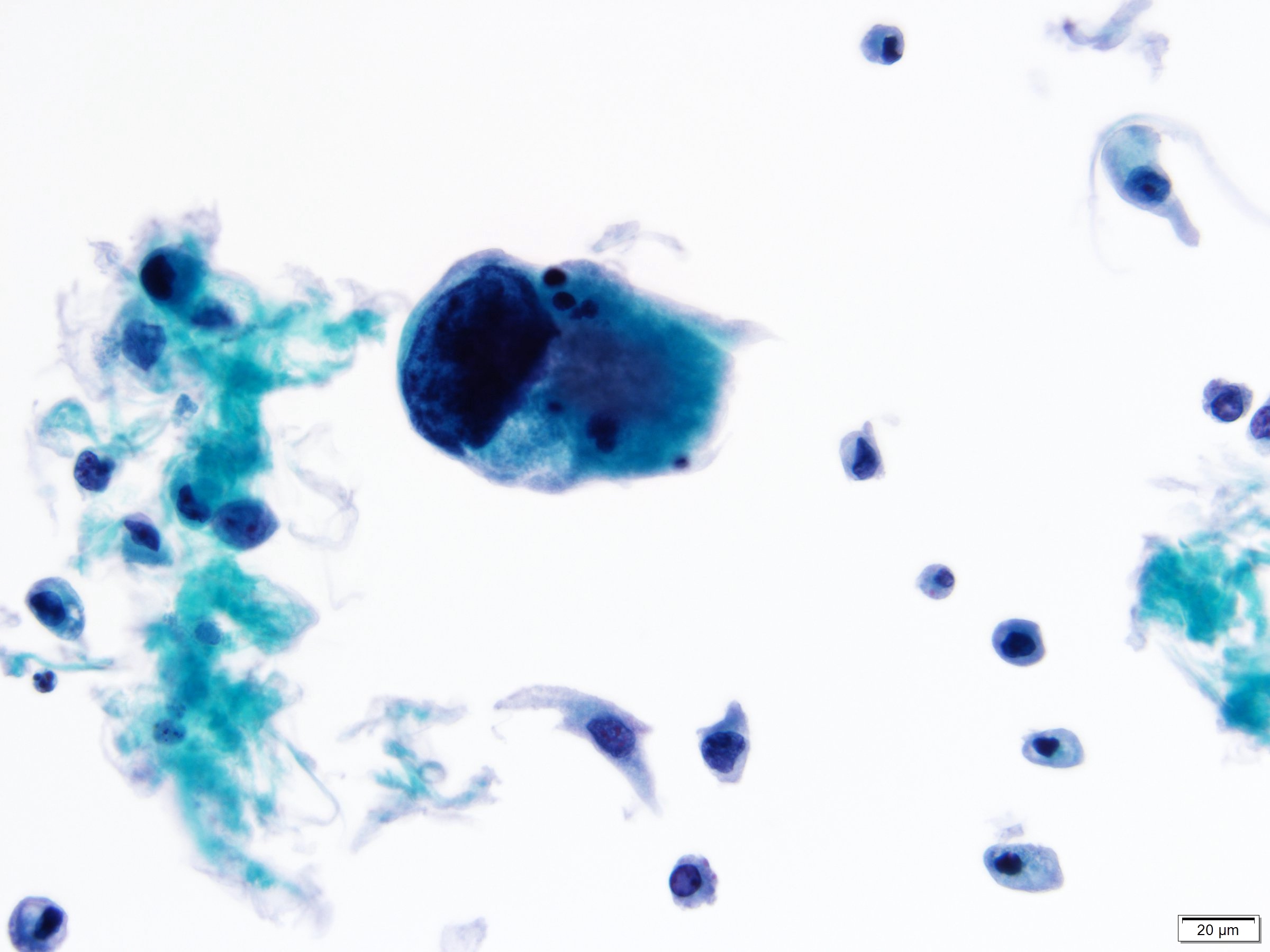
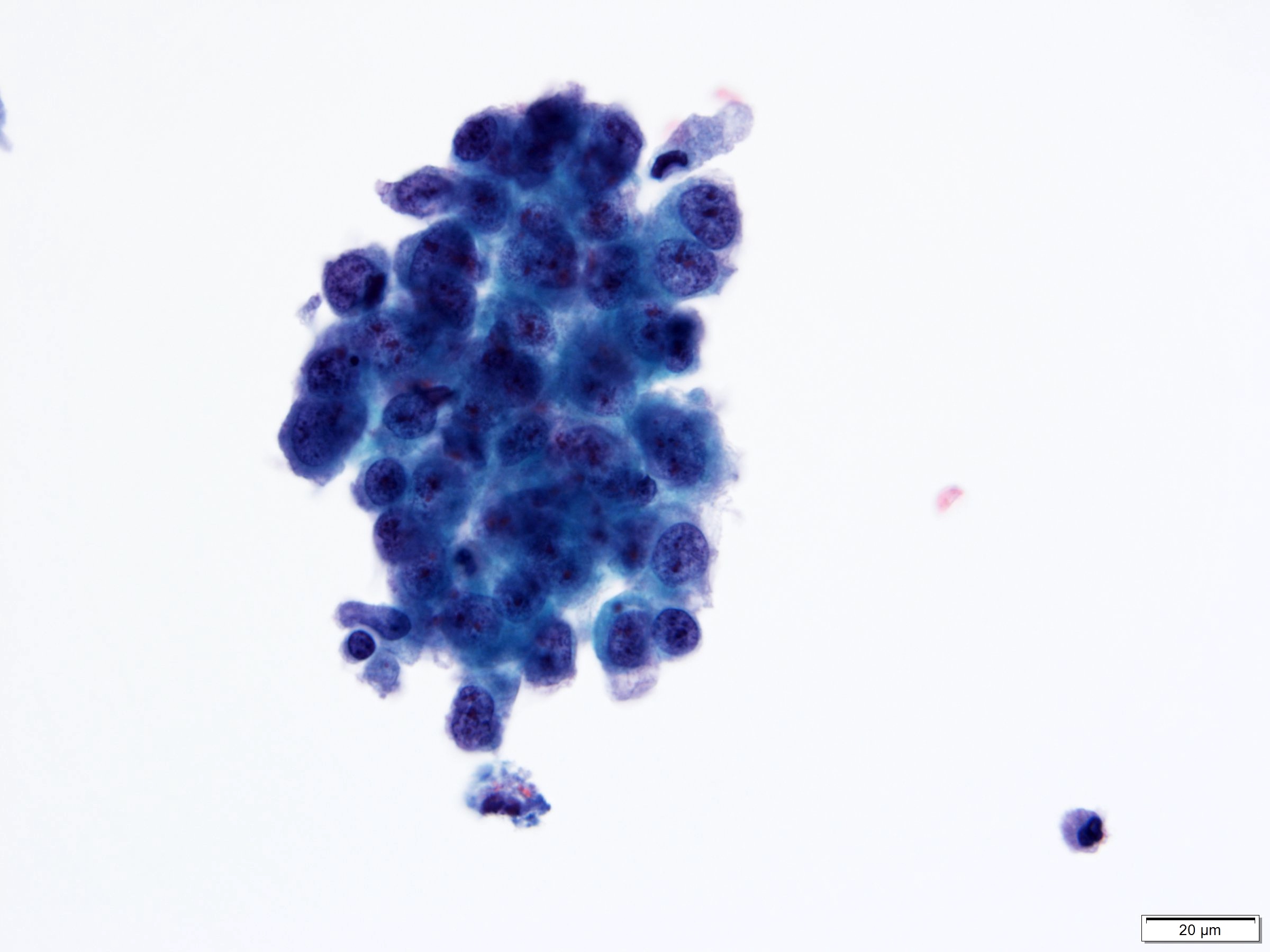

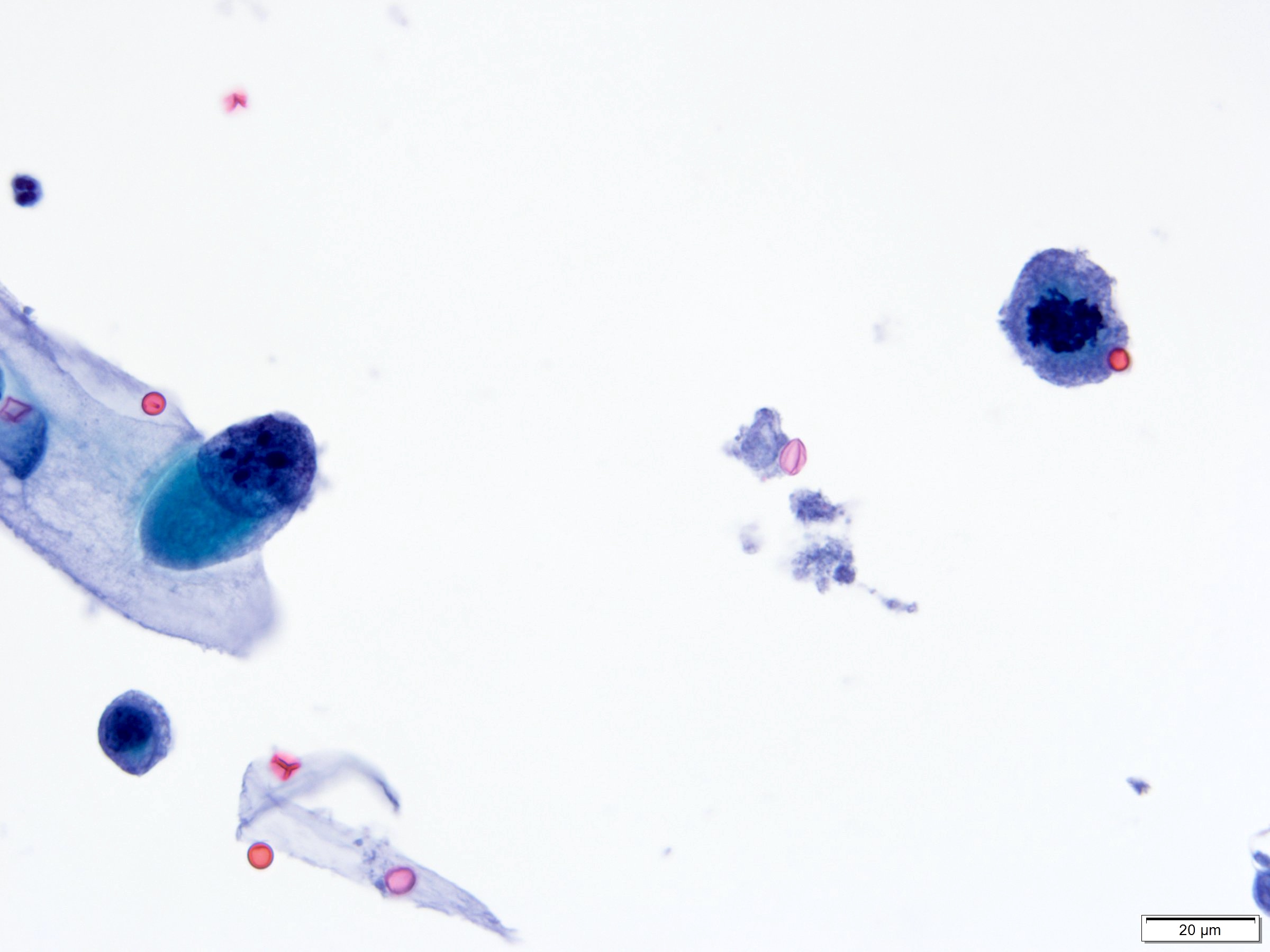
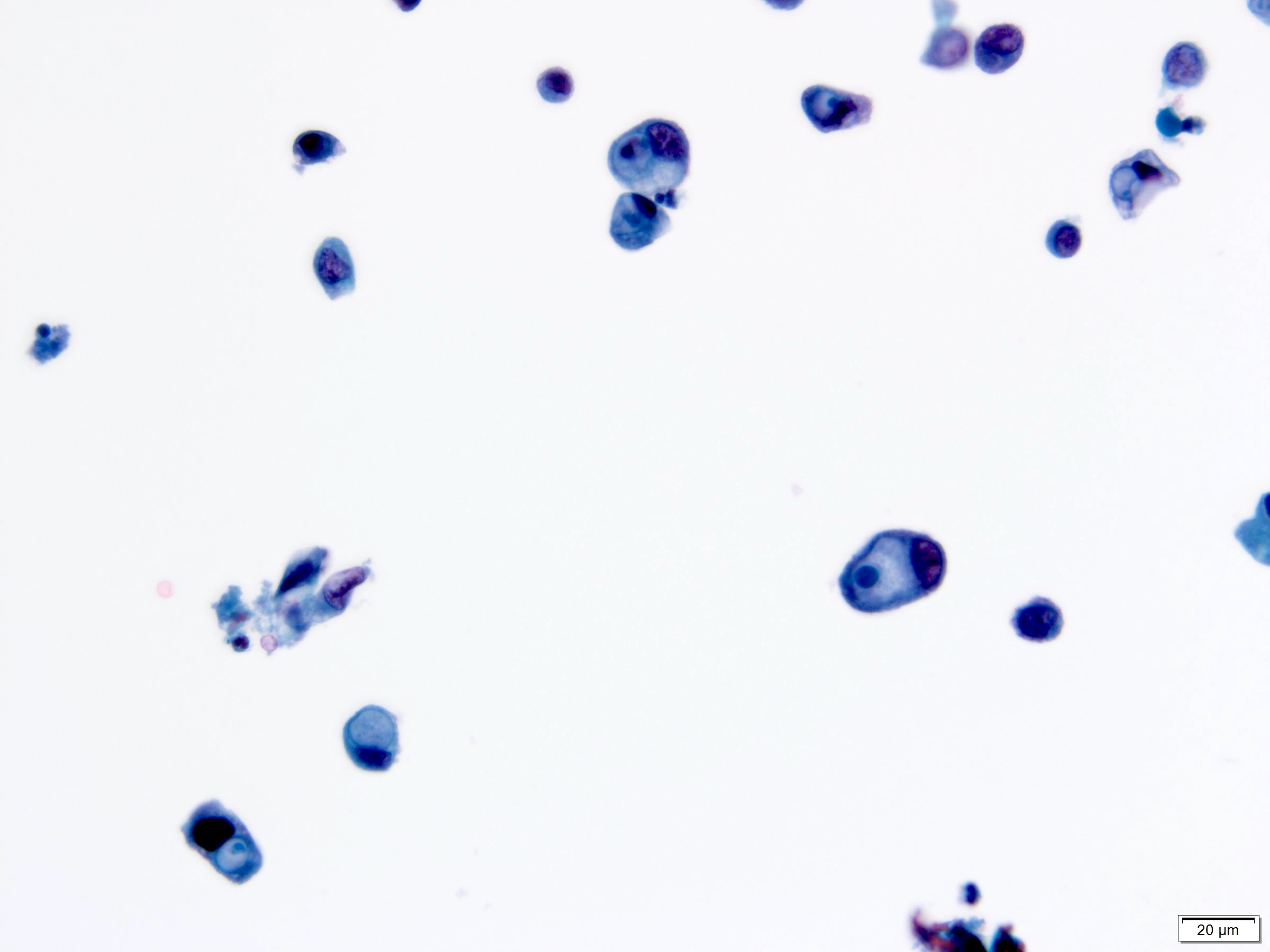
High grade urothelial carcinoma
Positive stains
- GATA3, CK20, p63, CK5/6, high molecular weight cytokeratin, CK7
- Increased p53 and Ki67 expression more frequent than in low grade
- Reference: Am J Surg Pathol 2014;38:e20
Negative stains
- CK5/6 loss in subset (Int J Mol Sci 2019;20:570)
Electron microscopy description
- High grade papillary urothelial carcinoma shows focal loss of zonula occludens (tight junctions) and macula adherens (desmosomes) (Cancer 1971;27:71)
Molecular / cytogenetics description
- Genetic or epigenetic changes in TP53 gene or TP53 regulatory gene (CDKN2A or p16)
- Somatic mutations in TERT in 70 - 80% noninvasive urothelial carcinomas
- Mutations in PIK3CA (25% of cases), TSC1, HRAS, APC
- Epigenetic silencing of tumor suppressor genes via promoter hypermethylation): RUNX3, CDKN2A, MLH1, MGMT, VHL, DAPK, TBX2, TBX3, GATA2, ZIC4, GSTP1, CDH1 (Eur Urol 2012;61:1245, Nat Rev Urol 2013;10:327)
- MicroRNA alterations (J Pak Med Assoc 2018;68:759)
- Loss of chromosome 9
Videos
Urothelial carcinoma, papillary and invasive
Sample pathology report
- Bladder lesion, transurethral resection:
- Papillary urothelial carcinoma, high grade (grade 3/3 - WHO 1973)
- Noninvasive, pTa
- Muscularis propria sampled
- No lymphovascular invasion
- Negative for urothelial carcinoma in situ
Differential diagnosis
- Low grade urothelial carcinoma:
- Cells more uniform and appear orderly on low power
- Chromatin evenly distributed
- Mitoses may be present but usually confined to lower half of urothelium
- Prominent umbrella cells present
- Papillary polypoid cystitis:
- Broad based papillary fronds with edematous or fibrous stroma
- No complex branching papillary structures
- Reactive urothelial atypia may be present
- Papillary nephrogenic adenoma:
- Prostatic type polyp:
Additional references
Practice question #1
Which of the following is true about the noninvasive papillary bladder lesion in the above image?
- Immunohistochemistry is helpful for diagnosis
- Progression to invasive disease is rare
- Common presentation include dysuria, urgency, frequency
- Neoplastic cells dyscohesion and partial denudation of urothelium is rare
- Cytologic atypia, nuclear pleomorphism and loss of polarity are common
Practice answer #1
E. Cytologic atypia, nuclear pleomorphism and loss of polarity are common
Comment Here
Reference: Noninvasive papillary urothelial carcinoma high grade
Comment Here
Reference: Noninvasive papillary urothelial carcinoma high grade
Practice question #2
Which of the following molecular changes has been described in high grade noninvasive papillary urothelial carcinoma?
- TP53
- FGFR3
- STAG3
- Chromosome 11 point mutations
- Germline mutations in TERT promoter
Practice answer #2
