Colon
Carcinoma
Adenocarcinoma
Author: Raul S. Gonzalez, M.D.
Editorial Board Member: Catherine E. Hagen, M.D.

Last author update: 10 May 2021
Last staff update: 2 September 2025 (update in progress)
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Adenocarcinoma colon

Table of Contents
Definition / general | Essential features | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Gonzalez RS. Adenocarcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colontumoradenocarcinoma.html. Accessed September 11th, 2025.
Definition / general
- Glandular neoplasm of the colorectum, representing 98% of colonic cancers (therefore, most details in the general colon carcinoma section pertain to adenocarcinomas)
- 9 WHO recognized subtypes: adenoma-like, adenosquamous, carcinoma with sarcomatoid components, medullary, micropapillary, mucinous, serrated, signet ring cell, undifferentiated
- Uncommon subtypes are clear cell adenocarcinoma, low grade tubuloglandular adenocarcinoma and villous / adenoma-like adenocarcinoma (Am J Surg Pathol 2006;30:1022, Histopathology 2016;68:183)
Essential features
- Most common primary colon carcinoma
- Typically arises through chromosomal instability pathway (70 - 80%) or microsatellite instability pathway (10 - 15%)
- Stage is most important prognostic factor
Clinical features
- Increased carcinoma risk in patients with polyposis syndromes, Lynch syndrome and inflammatory bowel disease
- Right sided tumors cause anemia, weakness and fatigue
- Left sided tumors cause change in bowel habits (diarrhea or constipation)
- Superficial tumors only rarely cause lymph node metastases due to distribution of lymphatics in colon
Diagnosis
- Generally discovered on colonoscopy and confirmed on biopsy
Prognostic factors
- Good prognostic factors:
- Microsatellite instability (Medicine (Baltimore) 2018;97:e0019)
- Increased tumor infiltrating lymphocytes (Am J Surg Pathol 2020;44:536)
- Poor prognostic factors:
- Advanced stage, higher grade, lymphovascular and perineural invasion (Surg Pathol Clin 2020;13:503)
- Positive margins
- High tumor budding (Mod Pathol 2012;25:1315)
- CDX2 loss (World J Gastroenterol 2015;21:1457)
- High stromal content (Histopathology 2018;73:197)
Case reports
- 29 year old man with colonic adenocarcinoma metastasizing as a germ cell neoplasm (Arch Pathol Lab Med 2001;125:558)
Treatment
- Surgical resection is generally required unless tumor is small and confined to a polyp
- Adjuvant therapy given for patients with lymph node metastases
- Neoadjuvant therapy often given for rectal carcinomas
Gross description
- Usually single, polypoid or ulcerated mass
- May cause serosal puckering if muscularis propria is involved
- Right colon tumors tend to be polypoid and exophytic, while left colon tumors tend to be annular, encircling lesions
Gross images
Images hosted on other servers:

Early, flat tumor

Flat, small adenocarcinoma

Invasive mucinous adenocarcinoma


Exophytic lesion
Microscopic (histologic) description
- Usually well or moderately differentiated gland forming carcinoma with marked desmoplasia, particularly at edge of tumor
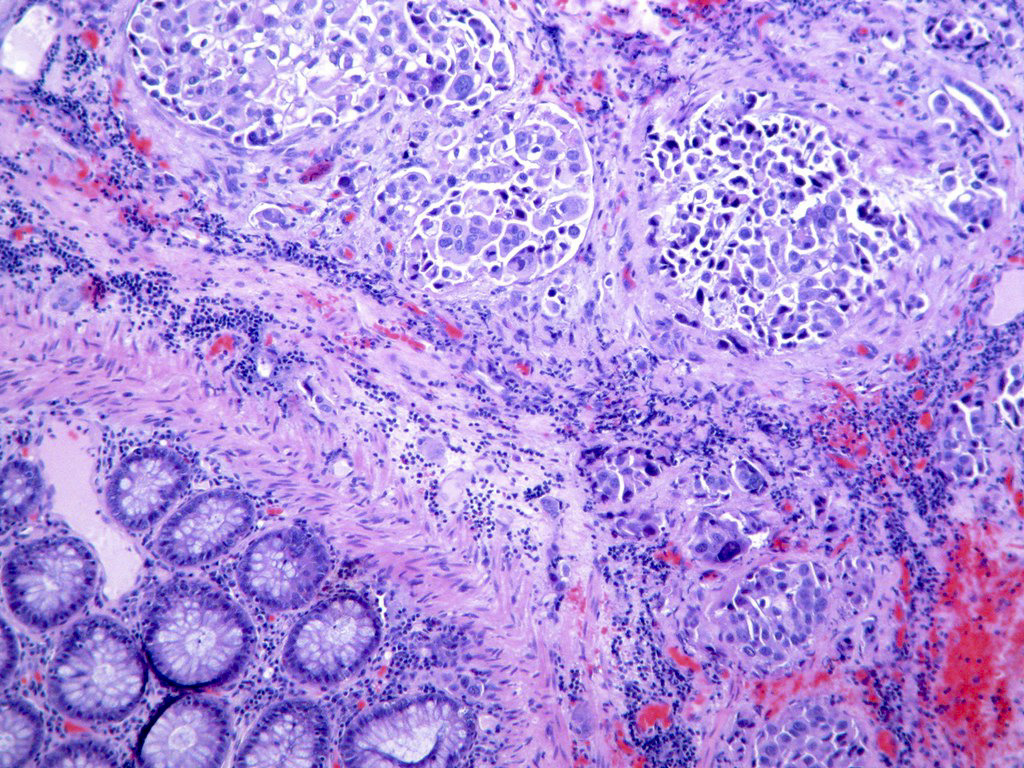
- Glands often cribriform and filled with necrotic debris (dirty necrosis), in both primary and metastatic sites
- Inflammatory cells and scattered neuroendocrine cells are common (Pol J Pathol 2005;56:89)
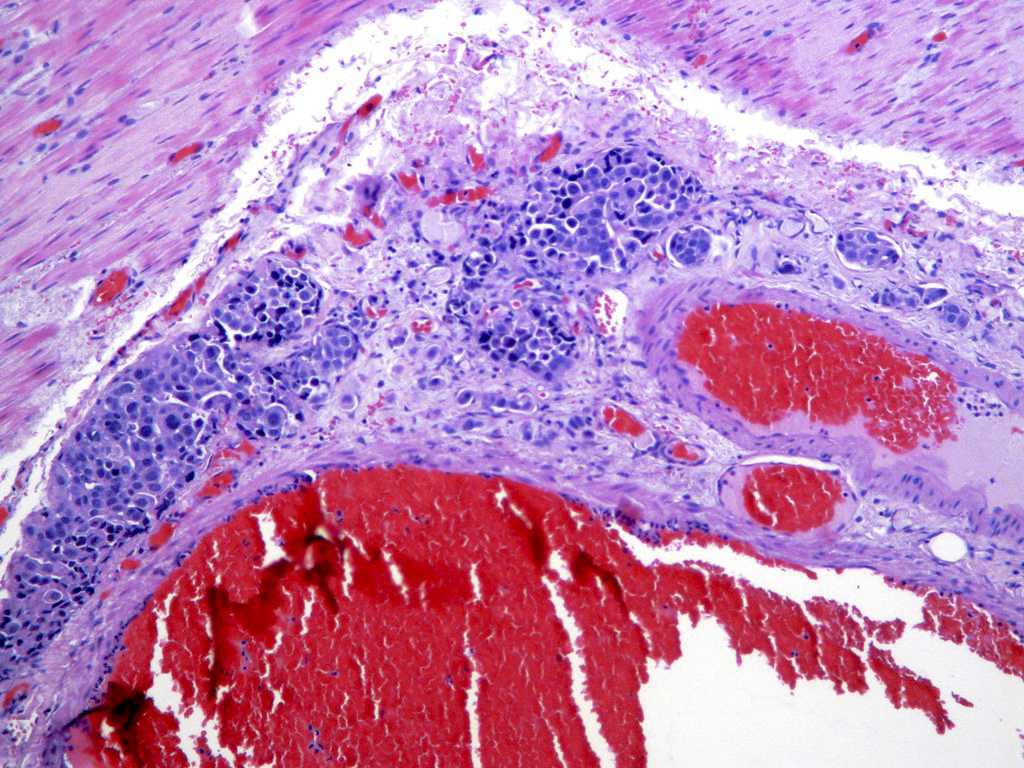
- Intramural venous invasion may be easier to identify using an elastin stain (J Clin Pathol 2002;55:17)
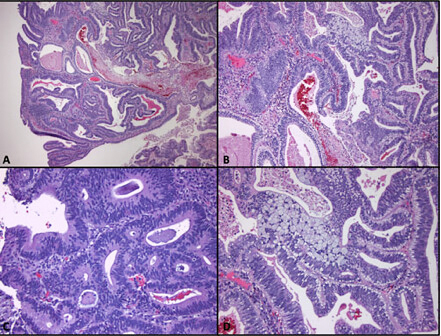
- Well differentiated:
- 15 - 20% of all carcinomas
- Well formed glands or simple tubules with uniform, basally oriented nuclei
- Somewhat resembles adenomatous epithelium
- Moderately differentiated:
- 60 - 70% of all carcinomas
- Tubules may be simple, complex or slightly irregular
- Nuclear polarity lost
- Poorly differentiated:
- 15 - 20% all of carcinomas
- Less than 50% gland formation
- Majority of tumor (excluding advancing edge) consists of sheets of cells without gland formation
- Usually right sided (Hepatogastroenterology 2004;51:1698)
- Note: preoperative histologic grading is not accurate (J Med Assoc Thai 2005;88:1535)
Microscopic (histologic) images
Contributed by Raul S. Gonzalez, M.D.
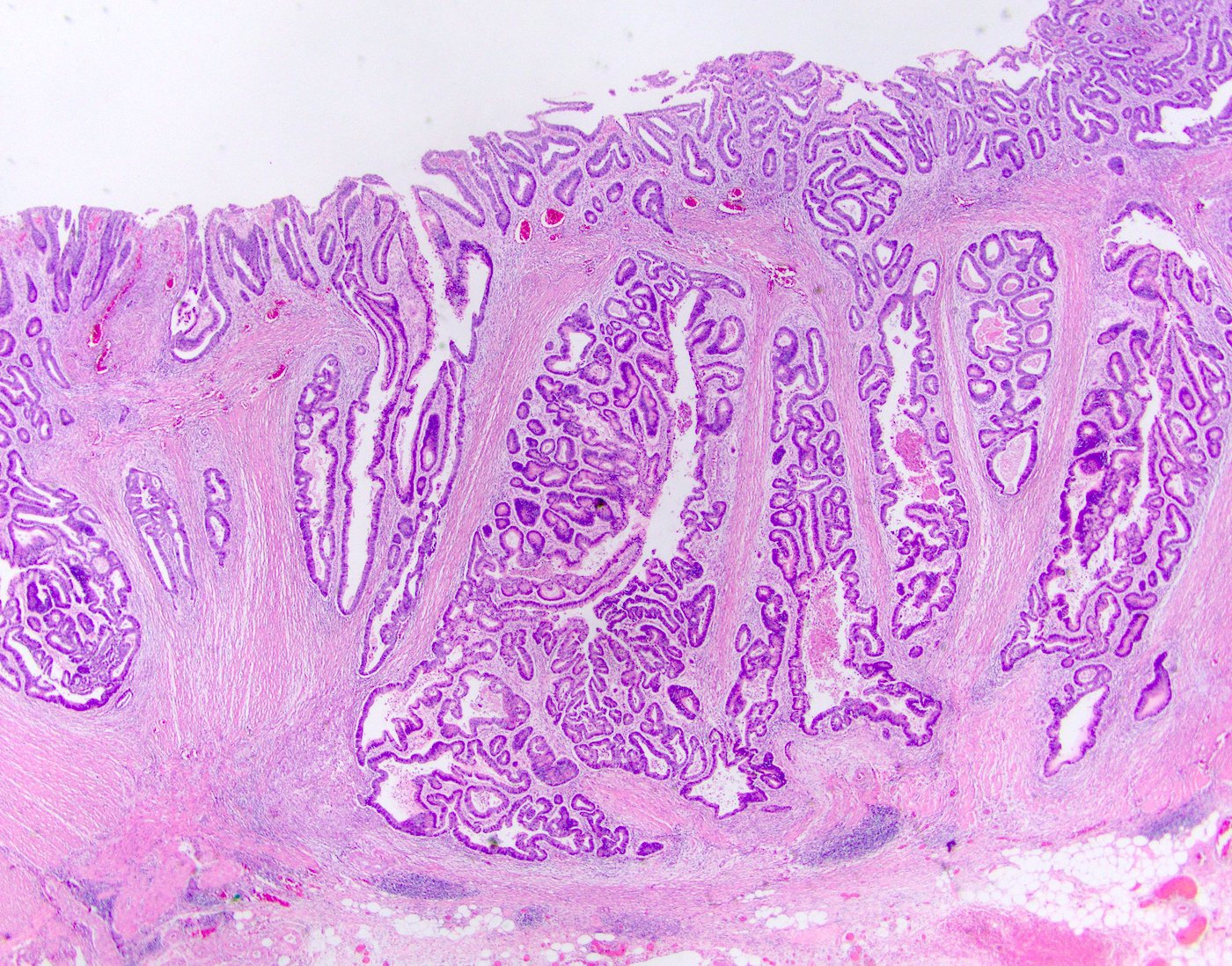
Low power
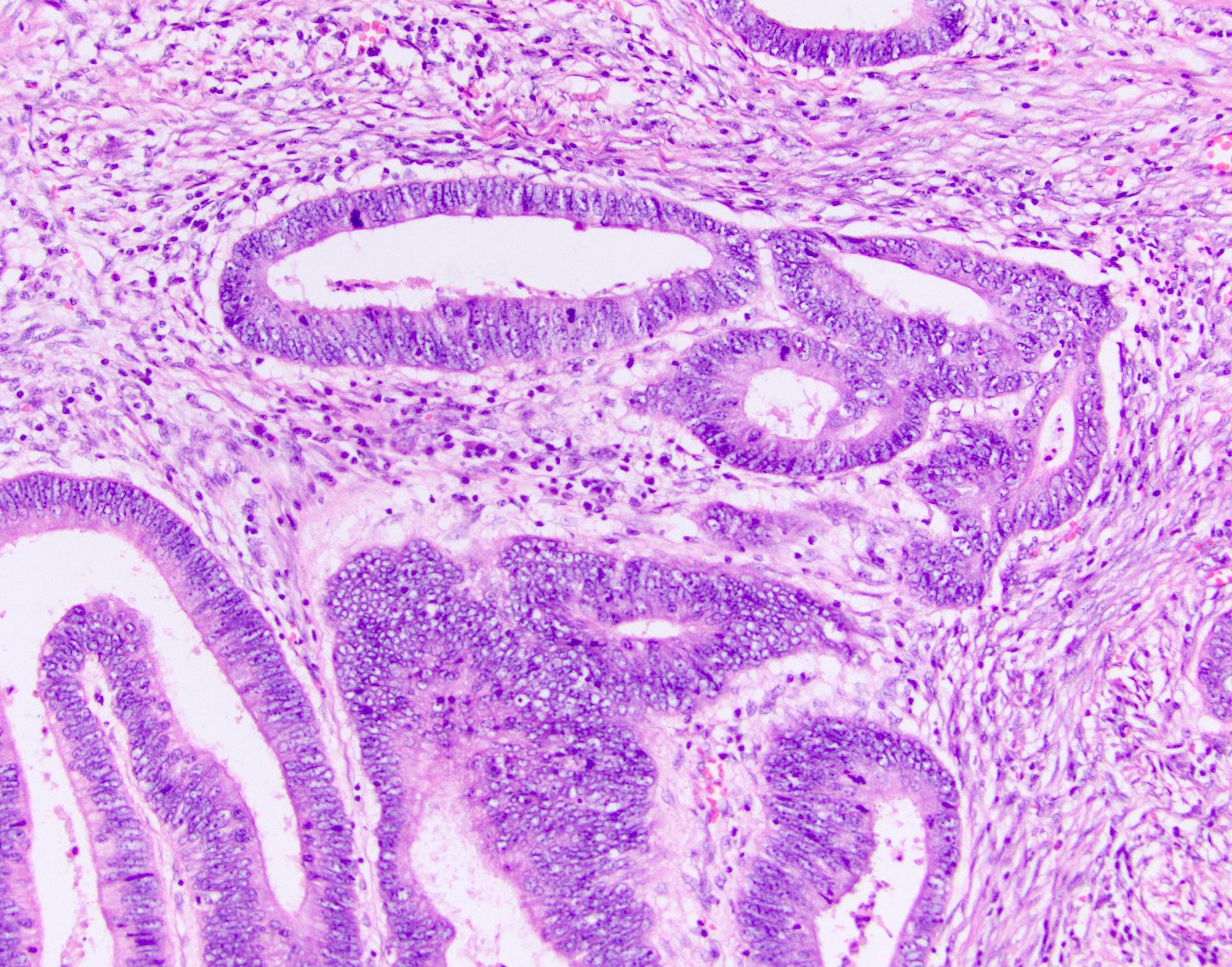
High power

Dirty necrosis
Cribriforming
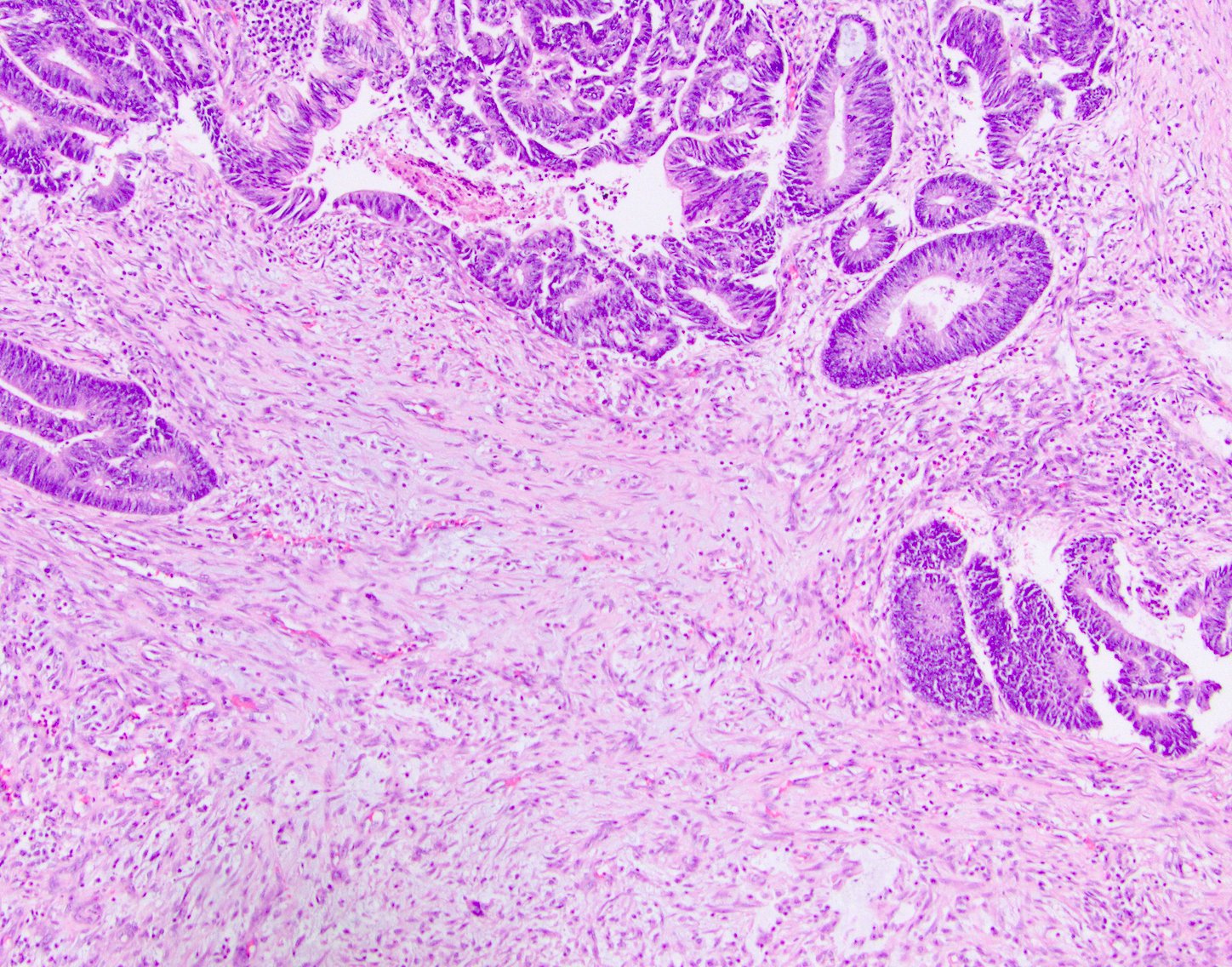
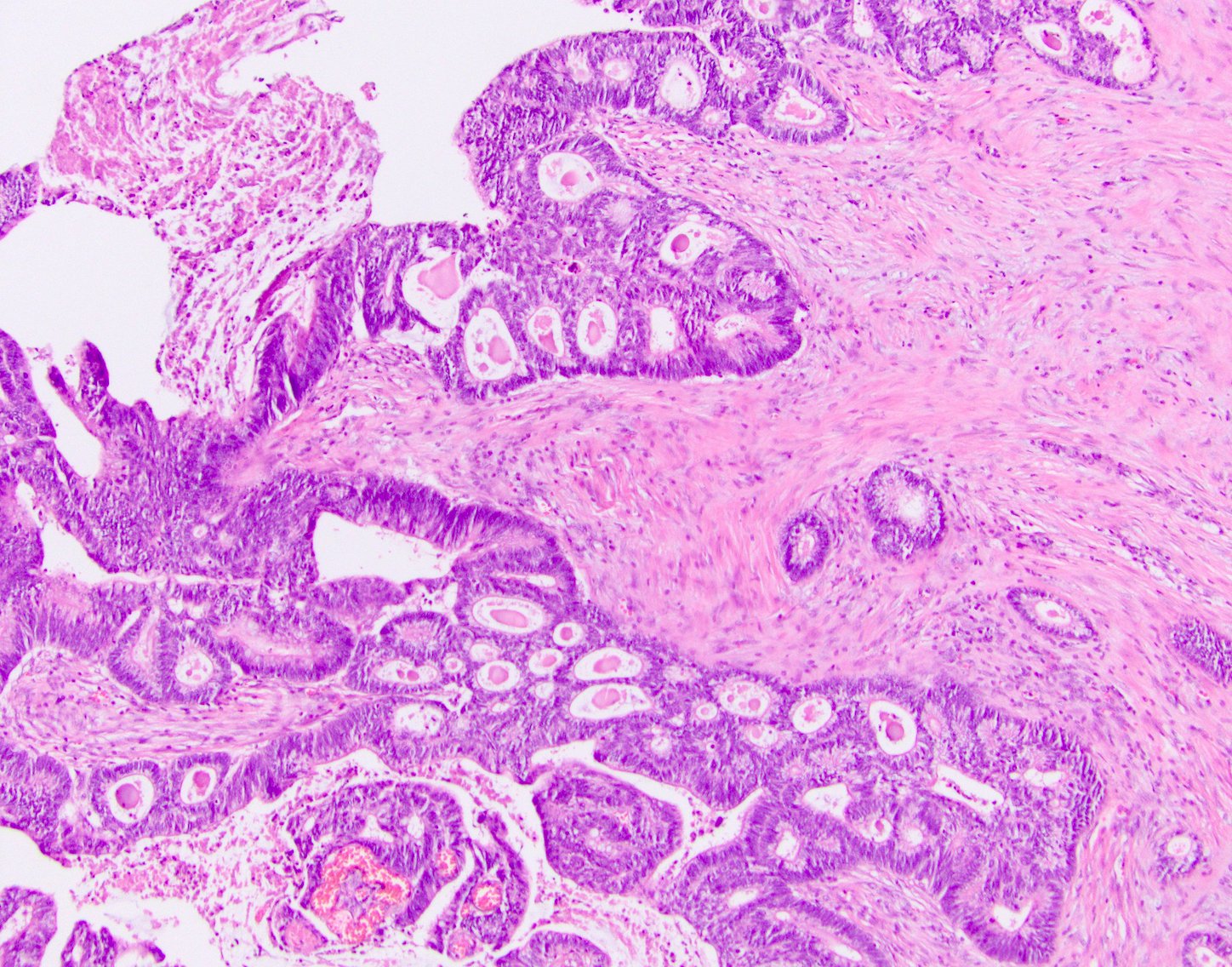
Desmoplasia
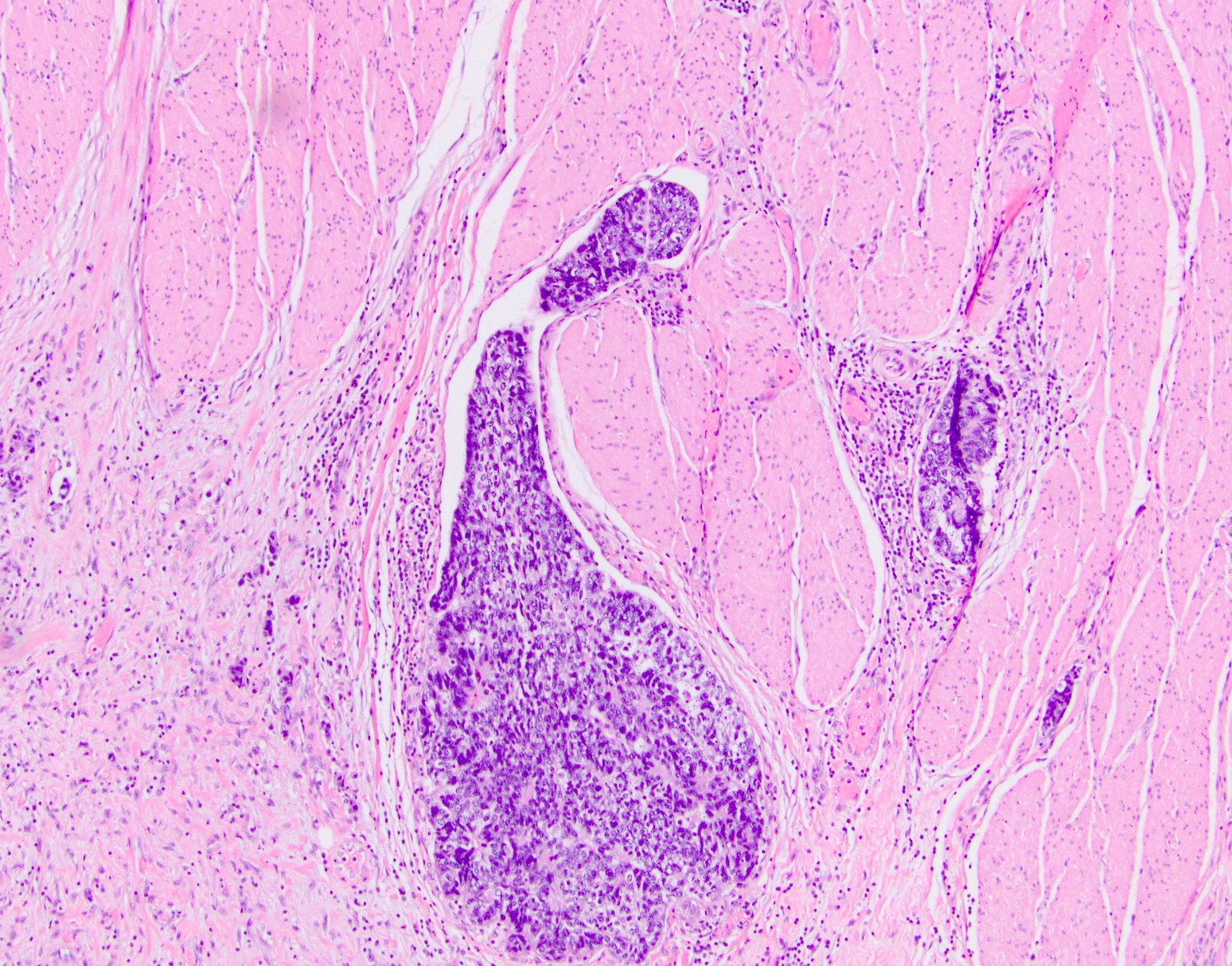
Lymphovascular invasion
Contributed by Semir Vranic, M.D., Ph.D. and Beverly Wang, M.D.
Poorly differentiated adenocarcinoma
Adenocarcinoma
Images hosted on other servers:

Whole mount scan

Moderately differentiated

Dirty necrosis in gland lumens

Venous invasion

Serosal penetration

Detached carcinoma cells

Signet ring morphology

Lymph node metastasis
Positive stains
- CK20 (Mod Pathol 2000;13:962)
- CDX2 (superior to villin: Am J Surg Pathol 2003;27:303)
- Also: AMACR (Am J Surg Pathol 2002;26:926)
- Sometimes estrogen receptor (Hum Pathol 2001;32:940)
- CD10 in stromal cells (Hum Pathol 2002;33:806)
- SATB2
Negative stains
- CK7, except in rectal adenocarcinomas (Appl Immunohistochem Mol Morphol 2009;17:196)
Molecular / cytogenetics description
- Most commonly mutated genes include APC, TP53 and KRAS
- Molecular classification of carcinomas has been proposed (Histopathology 2007;50:113)
- Tumors can be screened for microsatellite instability via immunohistochemistry for MLH1, MSH2, MSH6 and PMS2
Videos
Histopathology colon adenocarcinoma
Sample pathology report
- Sigmoid colon, resection:
- Adenocarcinoma, moderately differentiated (see synoptic report)
Differential diagnosis
Additional references
Practice question #1
- Which of the following is an official WHO recognized subtype of colorectal adenocarcinoma (per the 2019 classification)?
- Adenosquamous carcinoma
- Clear cell carcinoma
- Cribriform comedo carcinoma
- Low grade tubuloglandular adenocarcinoma
Practice answer #1
Practice question #2
- Which of the following is true about colon cancer?
- Commonly mutated genes include APC, TP53 and KRAS
- Most cases are poorly differentiated
- Most cases are positive for CK7 and negative for CK20 and CDX2
- Superficial / early tumors metastasize often
Practice answer #2
