Kidney tumor
Childhood tumors
TFE3 rearranged renal cell carcinoma
Resident / Fellow Advisory Board: Alcino Pires Gama, M.D.
Editorial Board Member: Michelle R. Downes, M.D.


Last author update: 17 December 2024
Last staff update: 17 December 2024
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: TFE3 rearranged renal cell carcinoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | IHC panels | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Rizkalla C, Tretiakova M. TFE3 rearranged renal cell carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumormalignantASPLTFE3.html. Accessed August 15th, 2025.
Definition / general
- MiT family translocation renal cell carcinomas (MiT RCC) comprise a distinct group of kidney tumors characterized by genetic alterations involving the TFE3 or TFEB genes
- They are more common in younger patients and may present with various architectural patterns, necessitating specific molecular and immunohistochemical techniques for accurate diagnosis
Essential features
- TFE3 rearranged renal cell carcinoma (TFE3 rRCC) is the most common subtype of renal cell carcinoma within the MiT translocation family
- Characterized by various translocations on chromosome Xp11.2, leading to gene fusions involving the TFE3 gene, which can be detected by immunohistochemistry showing diffuse strong nuclear expression of TFE3 protein (by break apart fluorescence in situ hybridization [FISH] or by RNA sequencing)
- Although the majority of TFE3 rRCC cases have a unique morphology of predominantly clear cells, papillary architecture and psammoma bodies, they often show substantial morphologic overlap with clear cell renal cell carcinoma (ccRCC) and papillary renal cell carcinoma (pRCC)
Terminology
- MiT family comprises a group of transcription factors (including TFE3 and TFEB, among others) that are associated with TFE3 rRCC, TFEB rearranged RCC (TFEB rRCC) and TFEB amplified RCC (Histol Histopathol 2022;37:311)
- TFE3 rRCC was previously referred to as Xp11 translocation renal cell carcinoma or renal cell carcinoma associated with Xp11.2 translocations / TFE3 gene fusions
ICD coding
Epidemiology
- TFE3 rRCC constitutes up to 50% of pediatric renal cancers, ∼15% of RCC cases in adults under the age of 45 and 1 - 2% of all RCC cases (Int J Mol Sci 2022;23:7649, Adv Anat Pathol 2022;29:131)
- Since RCC overall is much more common in adults, TFE3 rRCC in adults vastly outnumbers pediatric cases (Histol Histopathol 2022;37:311, Genes Chromosomes Cancer 2022;61:219)
- Higher occurrence of this condition in female patients (F:M = 2:1) can be partly explained by oncogenic fusions involving the inactive X chromosome; this process also partially reactivates some silenced genes on the rearranged X chromosome (Int J Mol Sci 2022;23:7649, bioRxiv 2023 Aug 6 [Preprint])
- Average age of onset is 40, with the most frequent decade age group being 20 - 29 (Int J Mol Sci 2022;23:7649)
Sites
- Kidney
Etiology
- Prior cytotoxic therapy is the only known risk factor predisposing to the development of TFE3 rRCC cases and accounts for 15% of patients (J Clin Oncol 2006;24:1529)
Clinical features
- As with other RCCs, ~33% of all tumors are asymptomatic at the time of diagnosis and are often incidentally discovered (Int J Mol Sci 2022;23:7649)
- ~33% of patients present with nodal involvement at presentation (Int J Mol Sci 2022;23:7649)
- Of the symptomatic patients, the most common clinical features include abdominal pain and gross hematuria (Front Oncol 2023;13:1252282, Front Pediatr 2023;11:1141223)
Diagnosis
- Usually asymptomatic and incidentally discovered by imaging
Prognostic factors
- Favorable prognostic factors
- Patients with lymph node involvement (N+) but without metastatic spread (M0) maintained a favorable prognosis following surgery (Int J Mol Sci 2022;23:7649)
- Poor prognostic factors
- Distant metastasis and older age at diagnosis independently predicted death (Genes Chromosomes Cancer 2022;61:219)
- Large tumor size and the presence of necrosis (but not nucleolar grade) are associated with more aggressive tumor behavior (Pathology 2020;52:297)
- Large series of consecutively treated RCC patients showed that cancer specific survival for patients with TFE3 rRCC was significantly worse than for patients with TFE3 rearranged negative pRCC (P < 0.001) but not different from patients with TFE3 rearranged negative ccRCC (Am J Surg Pathol 2012;36:663)
Case reports
- 16 year old girl presented with hematuria lasting for 5 days (Open Med (Wars) 2024;19:20240985)
- 28 year old woman presented with hematuria for 1 day at 29 weeks of gestation (Front Oncol 2024;14:1388880)
- 48 year old man who developed papillary RCC in transplanted kidney and TFE3 rearranged RCC in native kidney (J Korean Soc Radiol 2024;85:437)
- 71 year old woman with end stage kidney disease who was found to have a multiloculated cystic renal neoplasm on imaging (Adv Anat Pathol 2024;31:34)
Treatment
- For localized tumors, including patients with positive regional lymph nodes, surgery is the treatment of choice
- Therapies targeting vascular endothelial growth factor (VEGF) receptor, immunotherapy, mTOR inhibitors and target therapies for the MET signaling pathway are possible options for hematogenous metastases (J Immunother Cancer 2018;6:159, Int J Mol Sci 2022;23:7649)
Gross description
- No specific gross appearance; can closely resemble ccRCC (Semin Diagn Pathol 2015;32:103)
- Tumor mass located at the renal cortex
- Usually well circumscribed with a pseudocapsule
- Can have infiltrative edges that may extend beyond the kidney
- Yellow or tan cut surfaces
- May have papillary excrescences
Gross images
Contributed by Maria Tretiakova, M.D., Ph.D. and Debra L. Zynger, M.D.
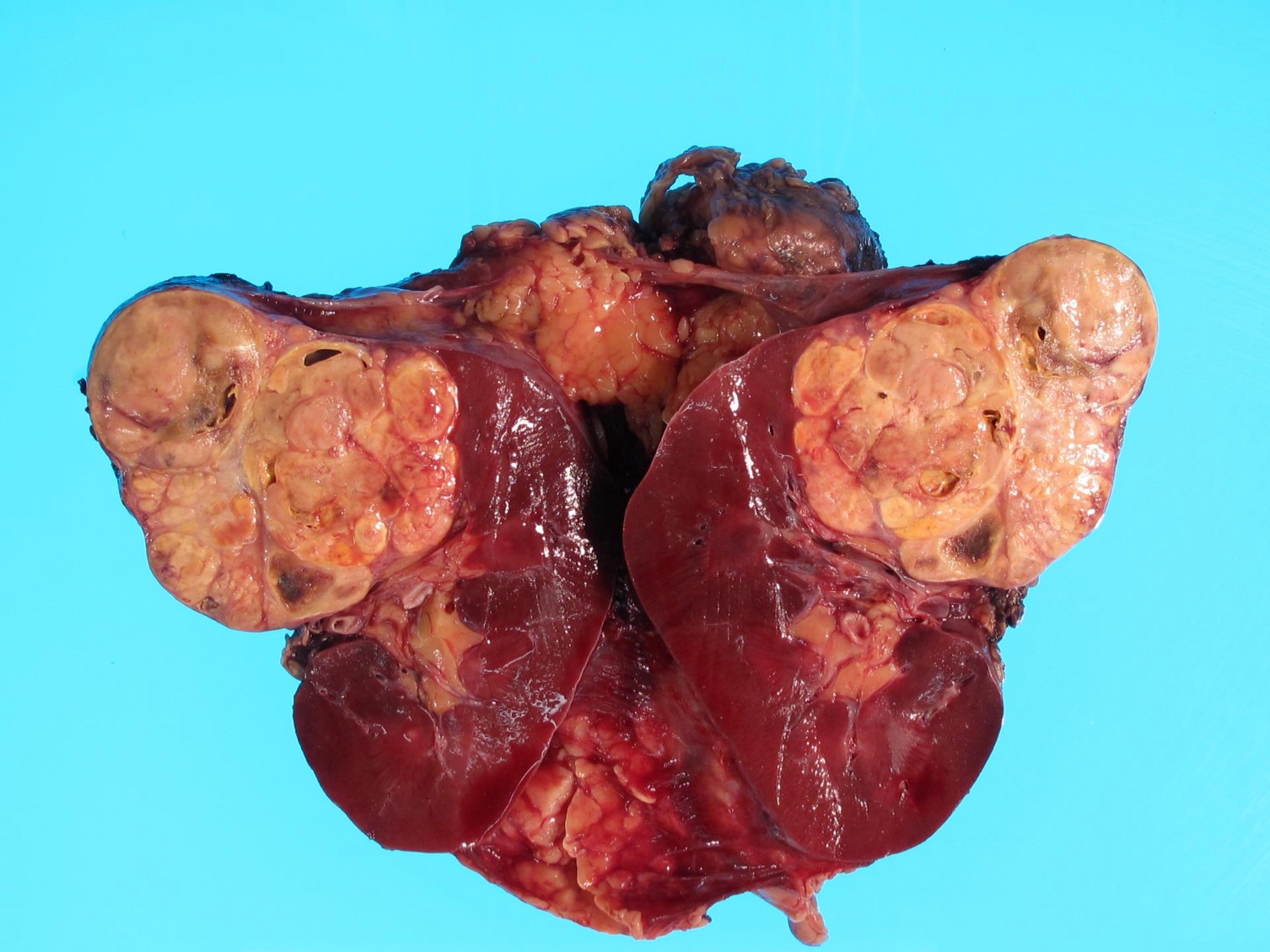
Solid tumor

Cystic tumor
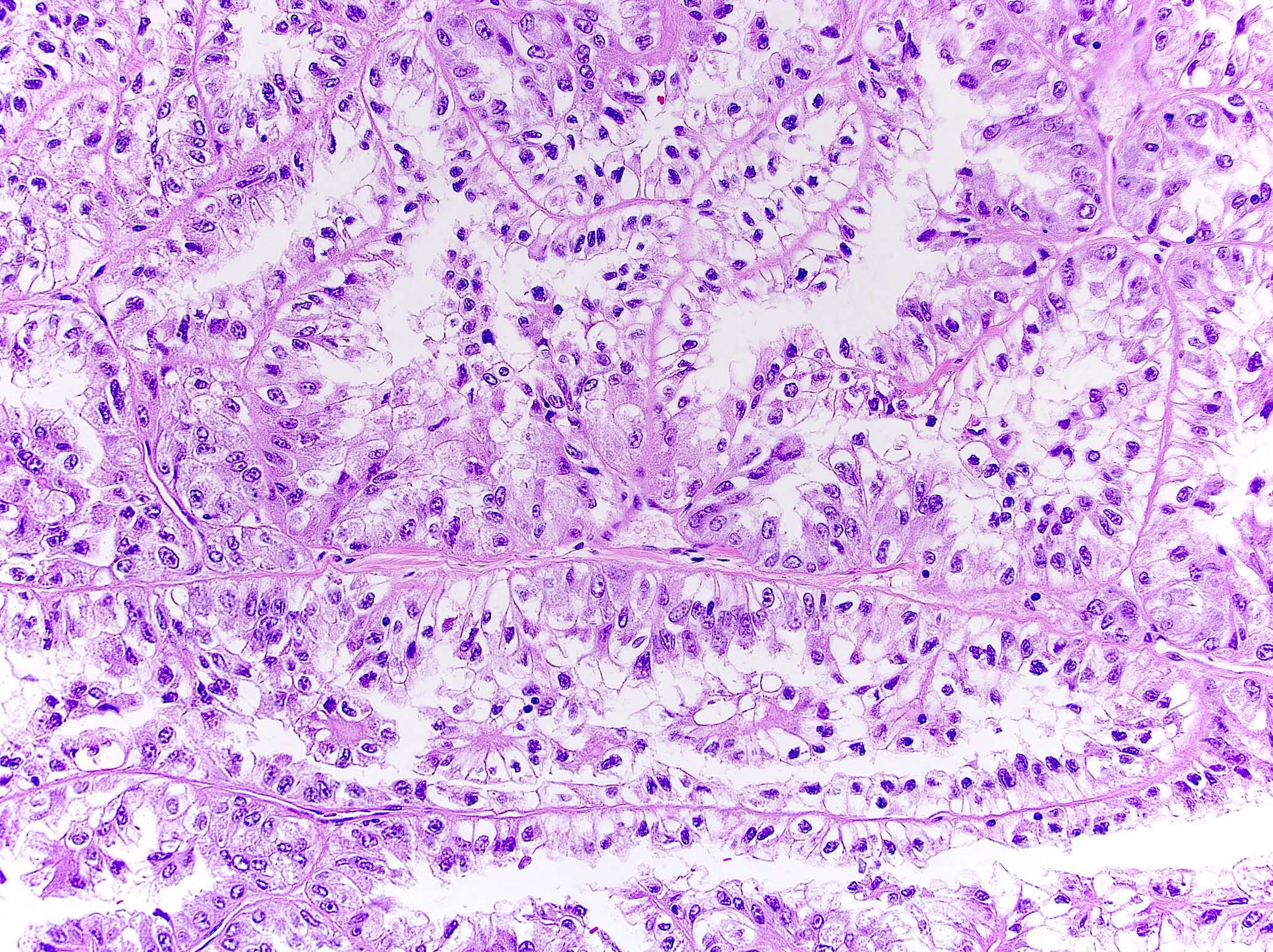
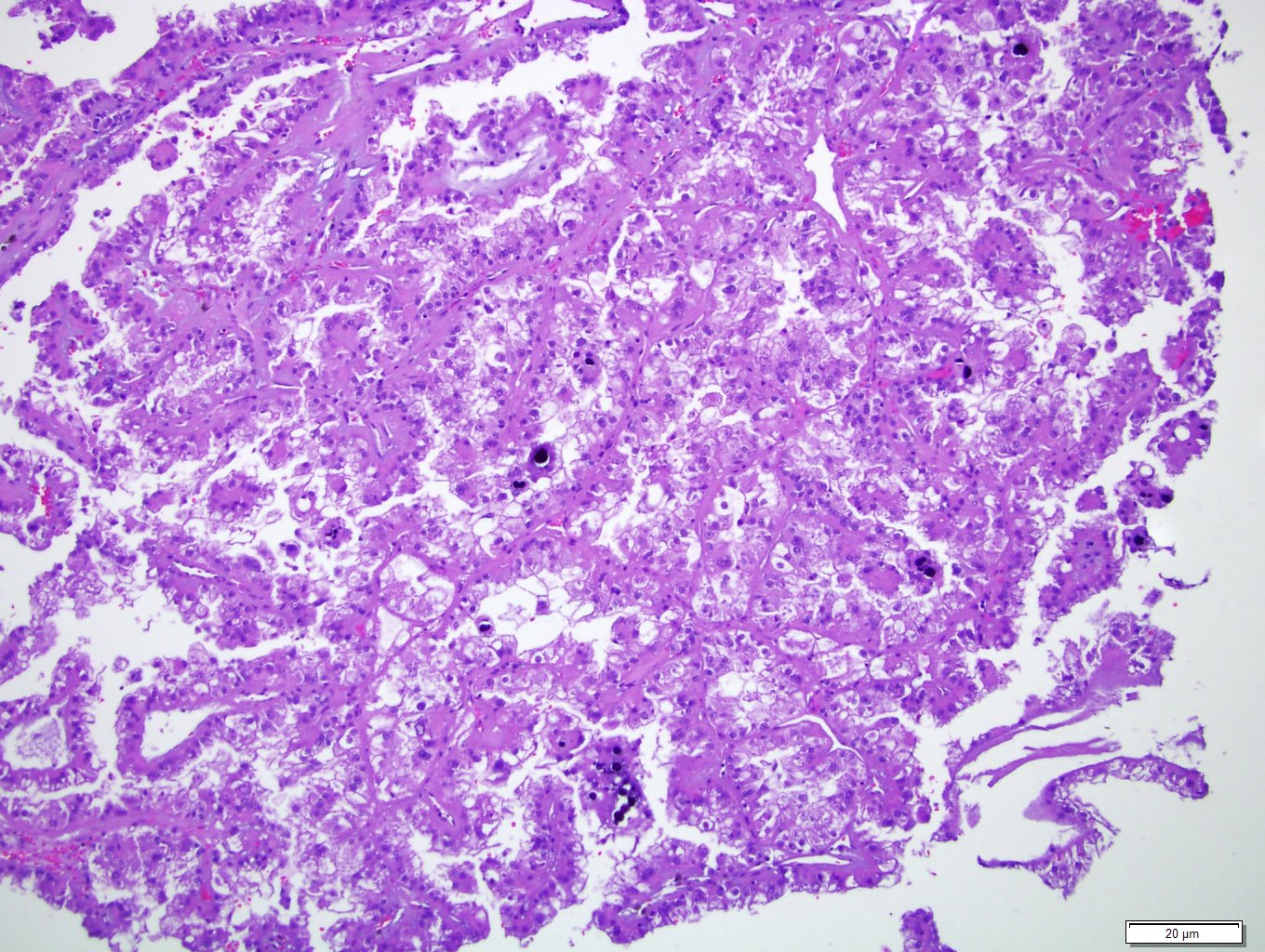
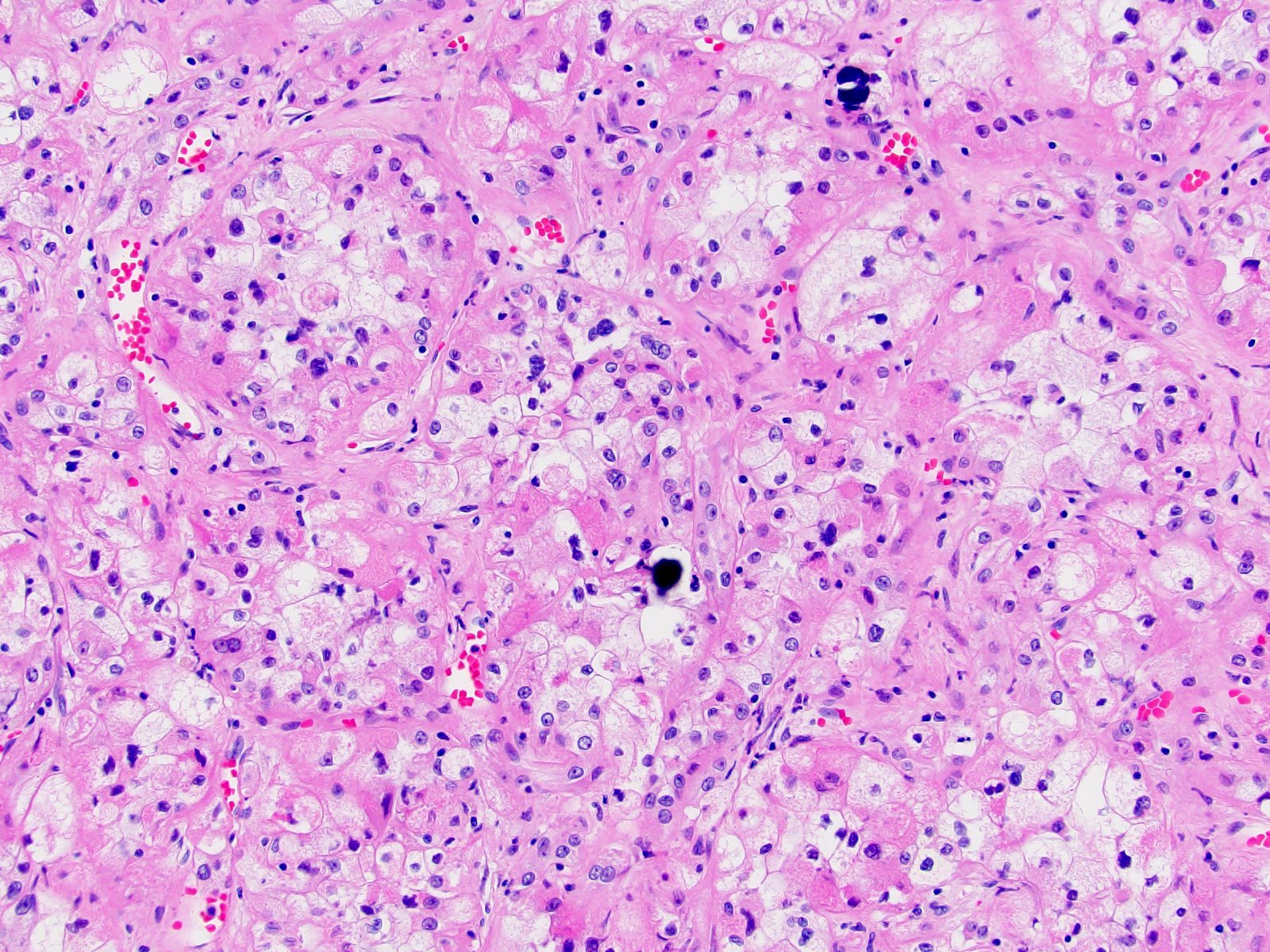
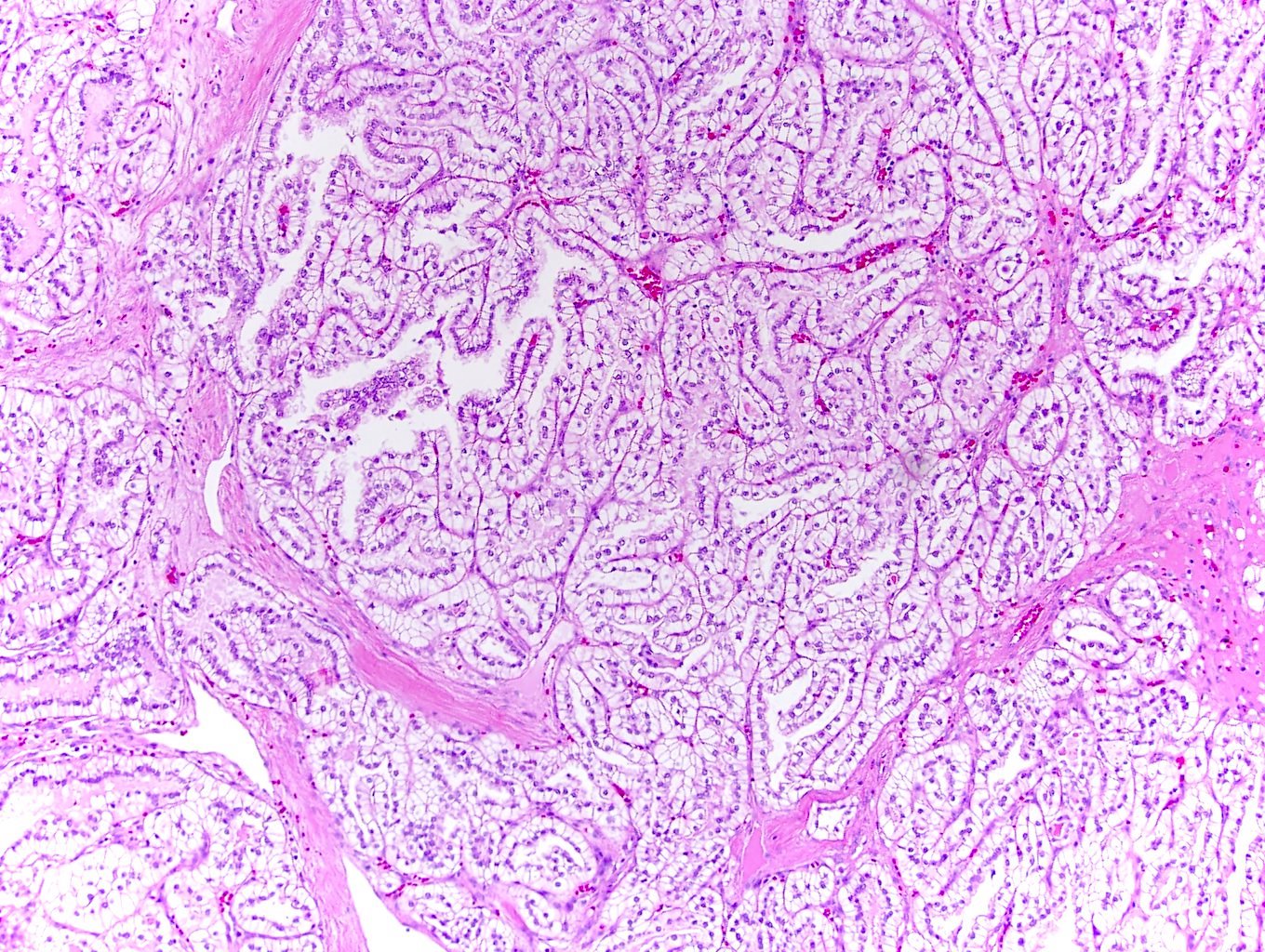
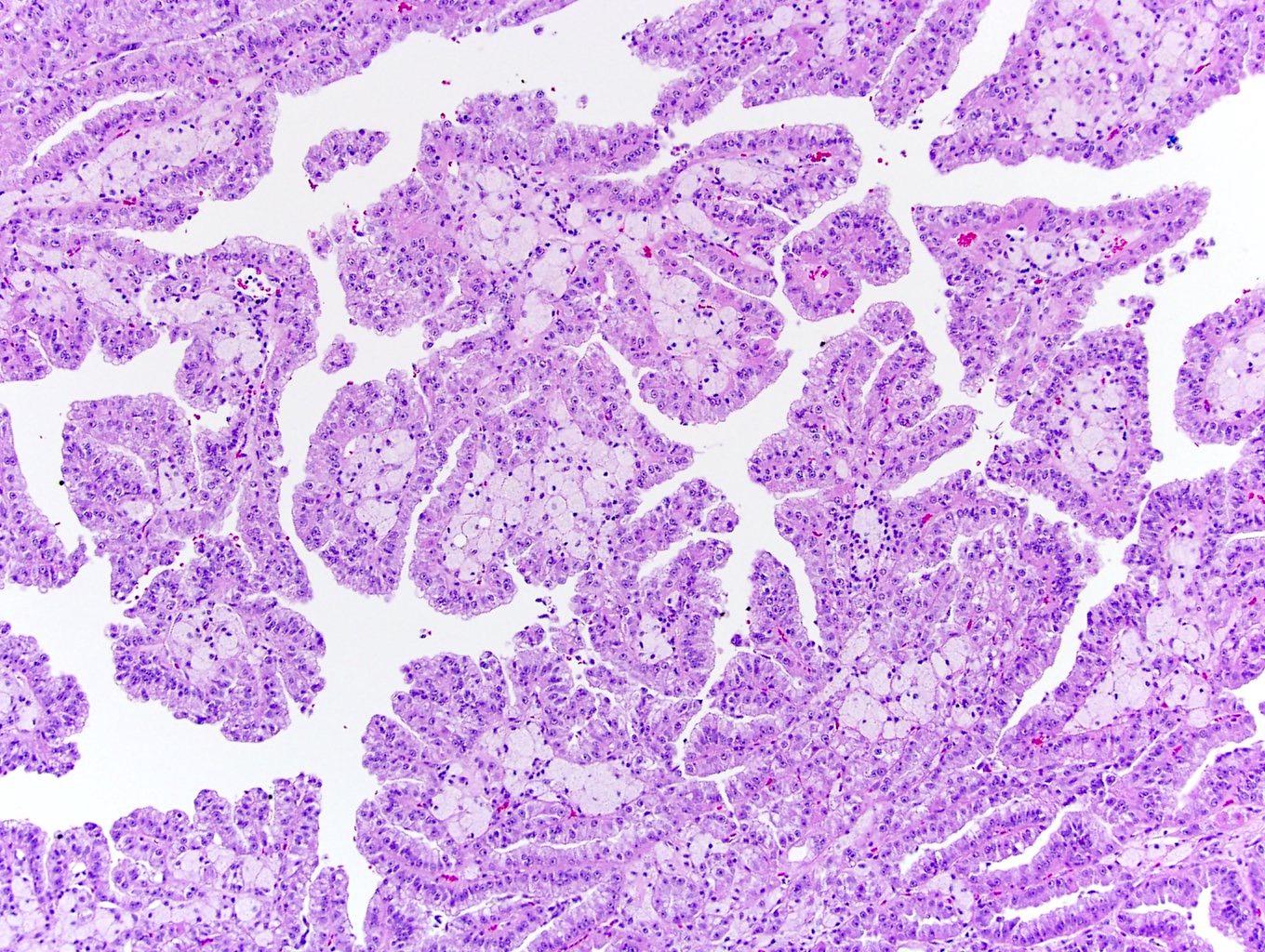
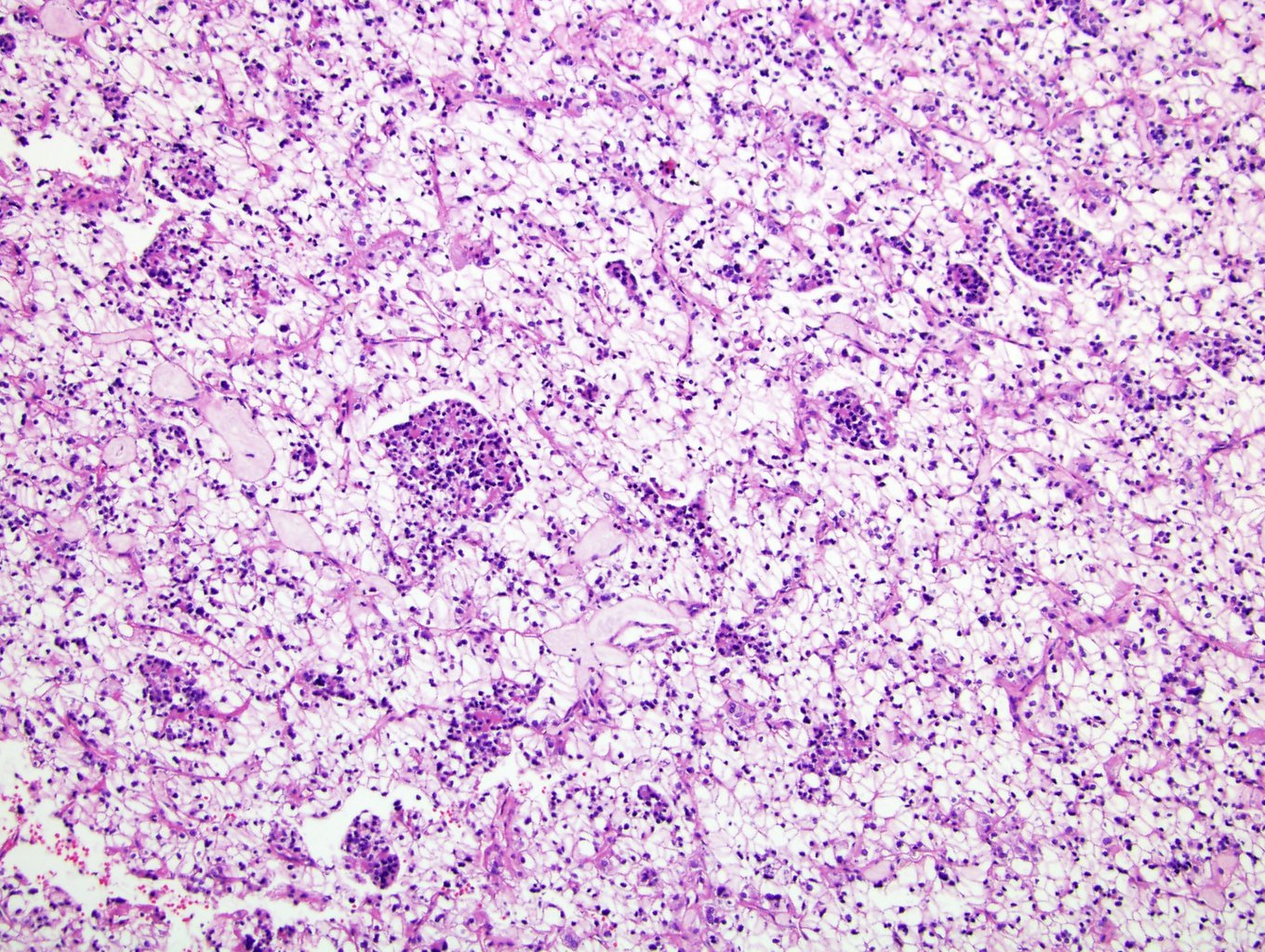
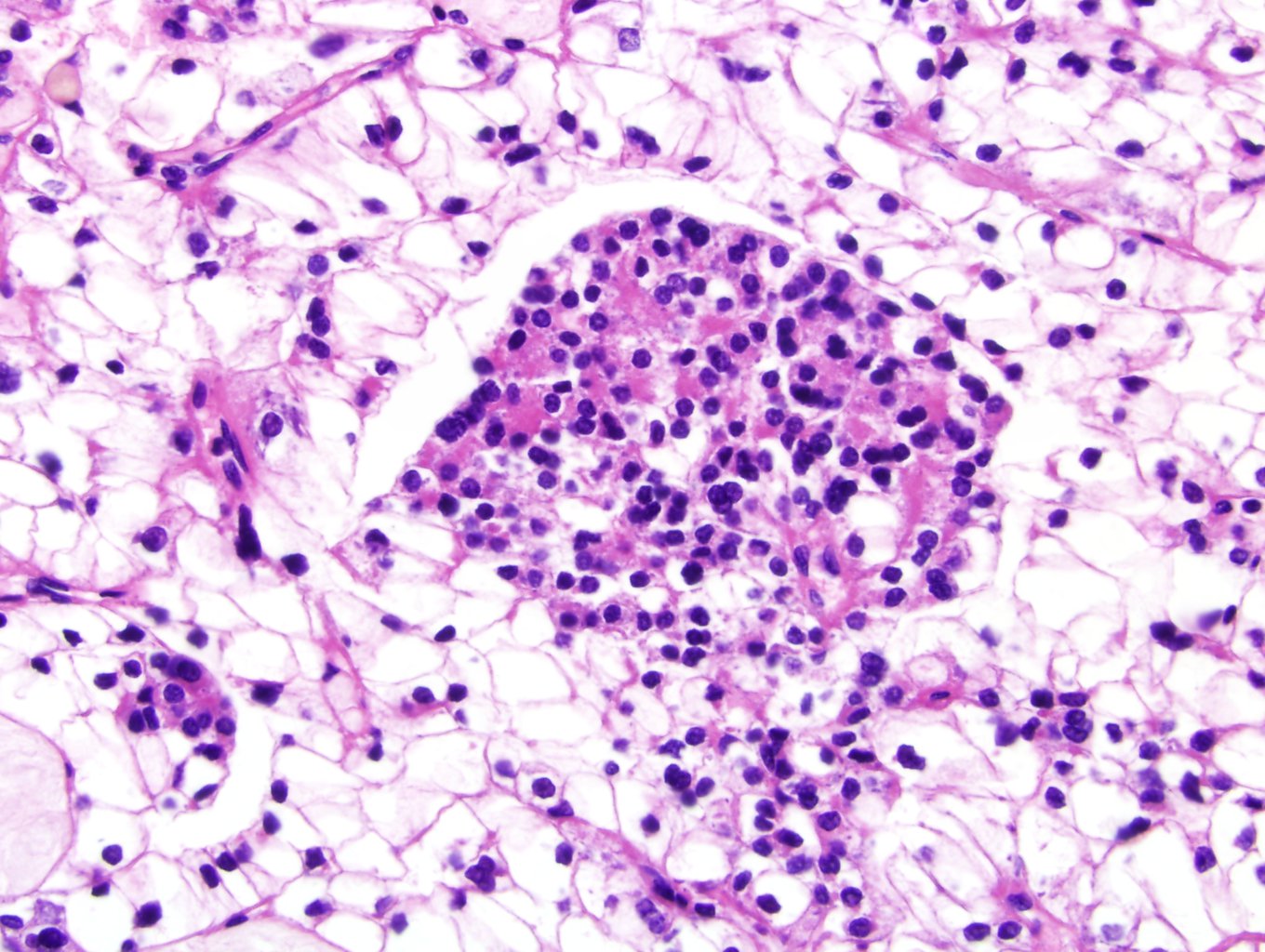
Microscopic (histologic) description
- Classic triad is present in ~66% of cases (Adv Anat Pathol 2022;29:131)
- Papillary architecture
- Large pale or clear cells with prominent nucleoli
- Psammoma bodies
- Cells are characteristically large with voluminous cytoplasm, discrete cell border and discohesion resulting in free floating cell clusters
- Other architectures can be appreciated: nested, alveolar, solid, cystic, tubular, hyalinized stroma
Microscopic (histologic) images
Contributed by Maria Tretiakova, M.D., Ph.D.
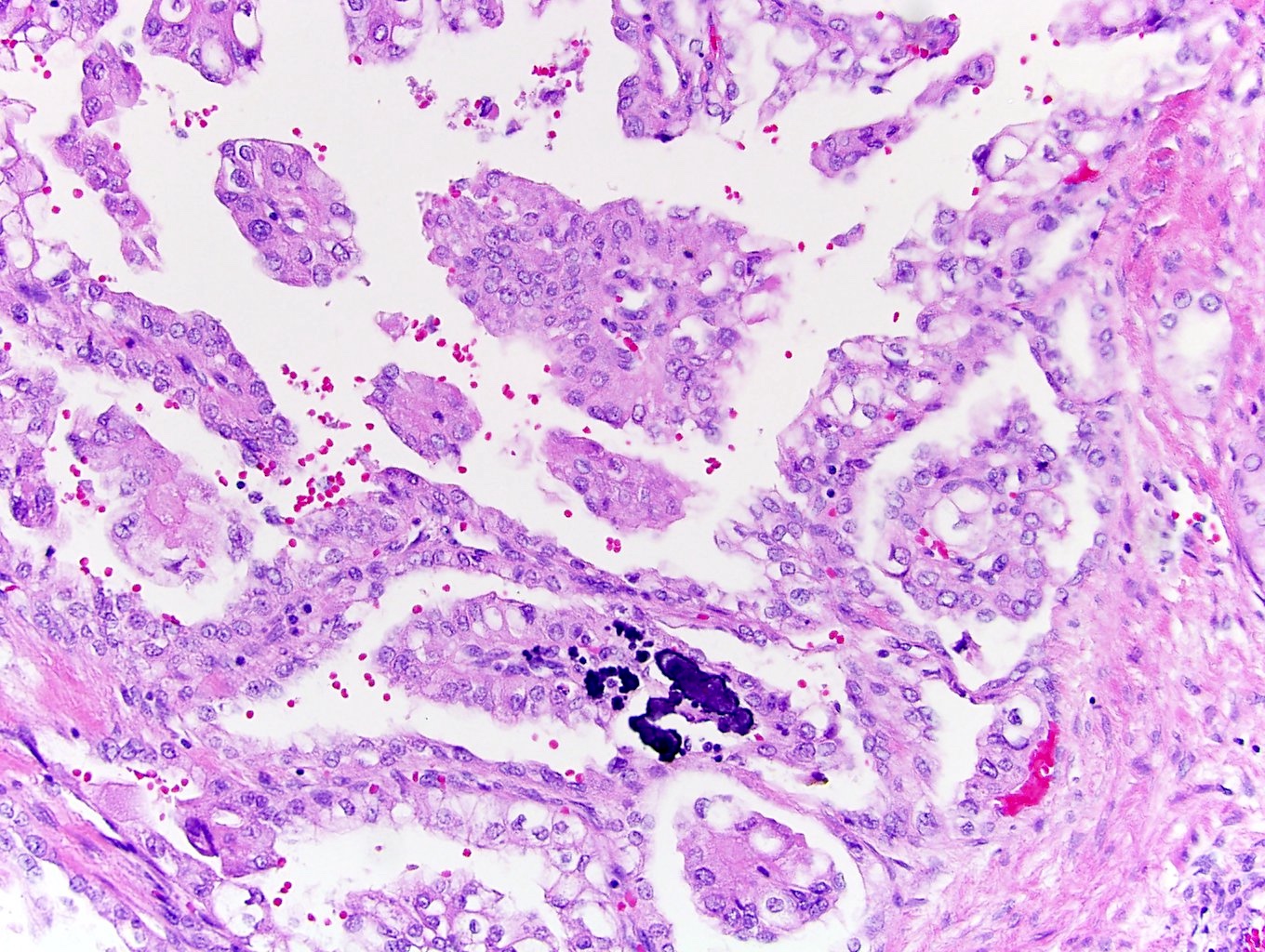
Classic triad
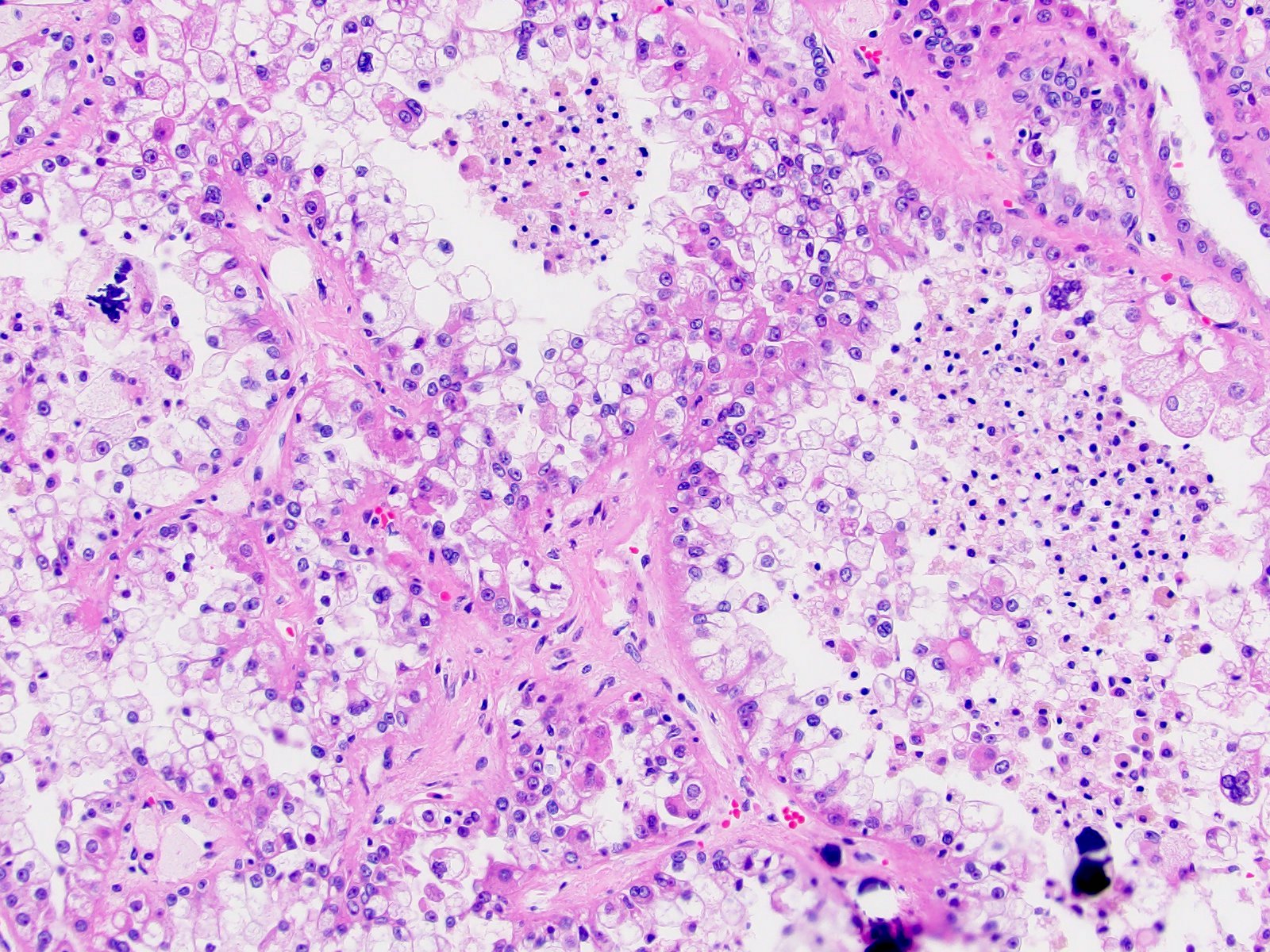
Cell blistering
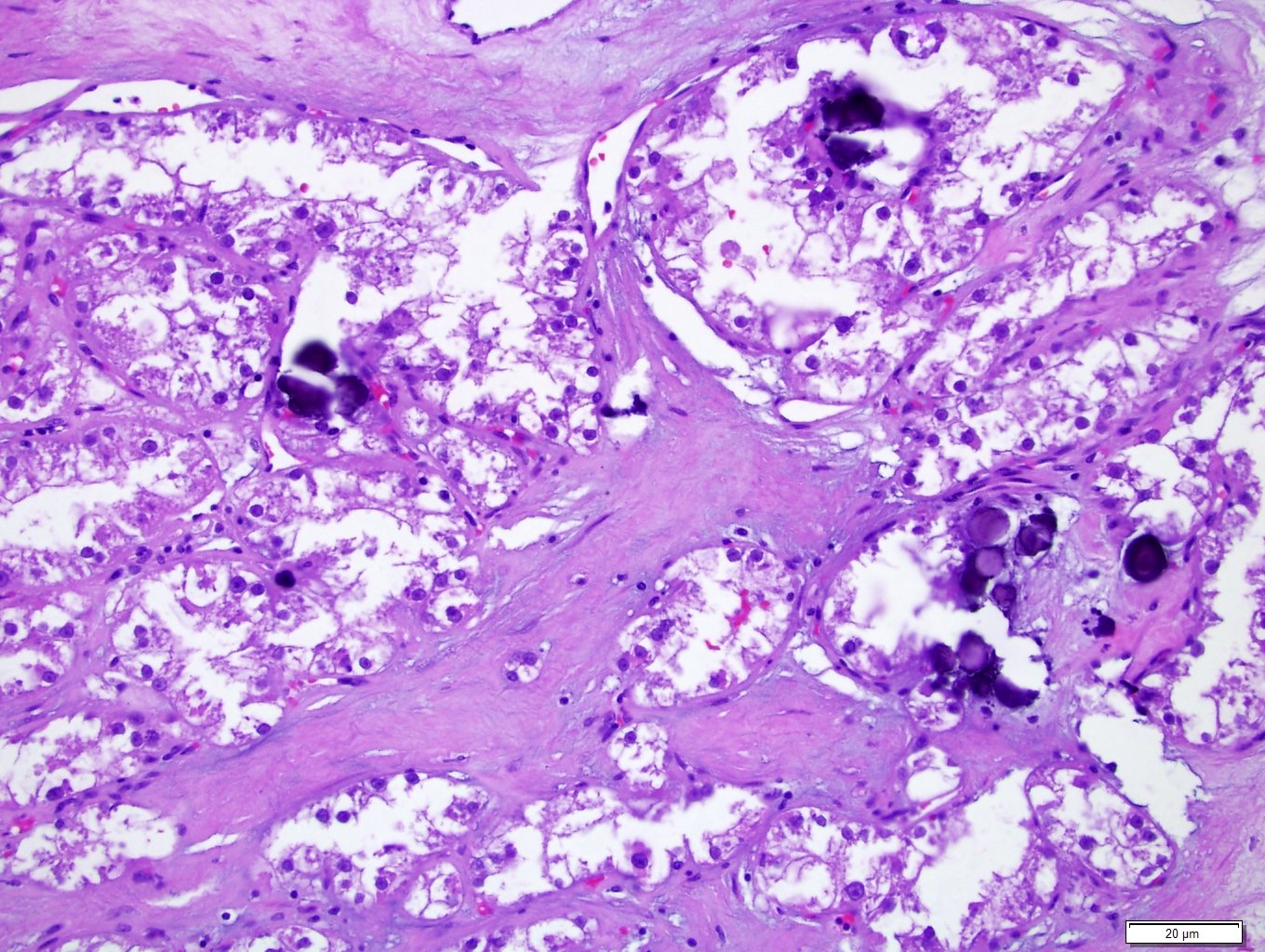
Psamomma bodies
TFE3 rRCC mimicking CCPRCT
Papillary and alveolar growth pattern
CCPRCT
pRCC
TFEB renal cell carcinoma
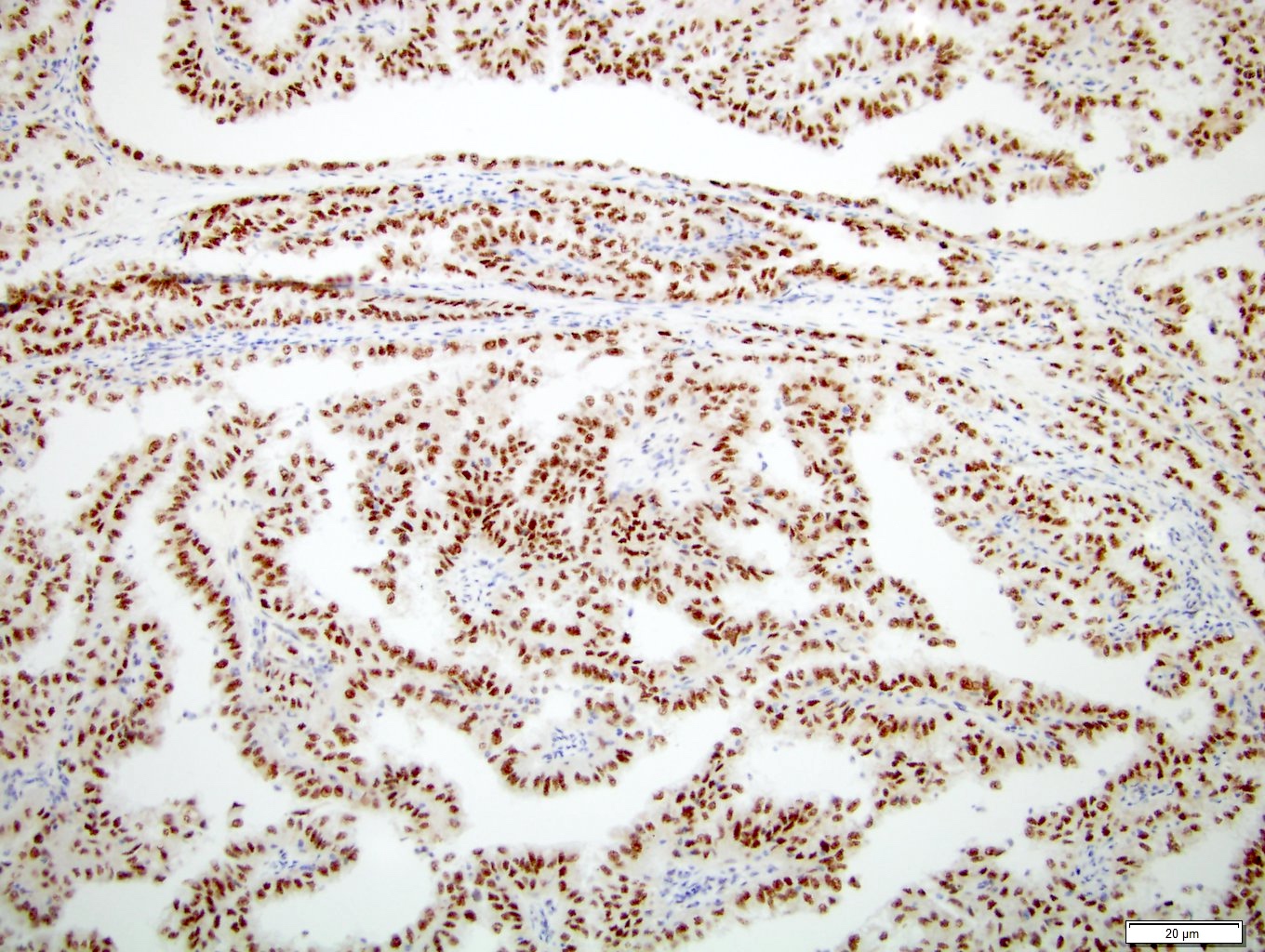
TFE3 positive IHC
Cytology description
- Touch preparations show tumor cells arranged in follicular, papillary or solid clusters with abundant vacuolated to granular cytoplasm and variably conspicuous nucleoli
- Psammoma bodies and hyaline globules are characteristic but nonspecific
- Reference: Diagn Cytopathol 2022;50:E382
Positive stains
- PAX8 (100%)
- TFE3 (95%)
- Very high sensitivity; positive in 95% of cases
- Should be used with cautious interpretation given that it can be overexpressed in other tumor types that do not harbor a TFE3 rearrangement, including epithelioid angiomyolipoma (AML), paragangliomas, adrenocortical carcinomas, melanomas and others (Adv Anat Pathol 2022;29:131)
- CD10 (89%)
- RCC (87%)
- AMACR / P504 (82%)
- GPNMB (glycoprotein nonmetastatic B) (J Pathol 2022;257:158)
- Sensitive screening tool for translocation RCC and TSC1 / TSC2 / MTOR alteration associated renal tumors (examples include eosinophilic solid and cystic carcinoma, eosinophilic vacuolated tumor and low grade oncocytic tumor)
- Helpful in distinguishing these tumors from more common RCC subtypes (ccRCC, pRCC, chromophobe RCC, oncocytoma)
- TRIM63 in situ hybridization (ISH): a positive result is highly specific to MiT RCC and results are highly concordant with TFE3 / TFEB FISH results (Mod Pathol 2021;34:1596)
- PDL1: positive in ~50% of rearranged renal cell carcinomas (Mod Pathol 2024;37:100404)
Negative stains
- Vimentin (40%)
- Cathepsin K (35%)
- Limited sensitivity
- Its expression is highly dependent on fusion subtype (ranging from 16 - 60%); highest rates of positivity are in PRCC::TFE3 and lowest in SPSCR1::TFE3 (Adv Anat Pathol 2022;29:131, Genes Chromosomes Cancer 2022;61:219)
- EMA (32%)
- AE1 / AE3 (28%)
- CAM 5.2 (23%)
- CAIX (3%)
- CK7 (10%)
- Melanocytic markers (HMB45 [17%], MelanA [19%])
- Largely negative, in contrast to TFEB rRCC
- Reference: Adv Anat Pathol 2022;29:131
IHC panels
| Hale | KIT | CK7 | S100A1 | VIM | CAIX | AMACR | SDH | TFE3 | |
| Chromophobe RCC | +++ | +++ | +++ | - | - | - | - | +++ | - |
| Clear cell RCC | - | - | - | - | +++ | +++ | - | +++ | - |
| Oncocytoma | - | +++ | Rare | +++ | - | - | - | +++ | - |
| Papillary RCC | - | - | +++ | - | +++ | - | +++ | +++ | - |
| Translocation RCC | - | - | - | - | - | - | ++ | +++ | +++ |
| SDH deficient RCC | - | - | - | - | - | - | - | - | - |
References: Pathol Res Pract 2015;211:303, Ann Diagn Pathol 2020;44:151448, Am J Surg Pathol 2014;38:e6, Arch Pathol Lab Med 2019;143:1455, Transl Androl Urol 2019;8:S123, Hum Pathol 2020;104:18
Molecular / cytogenetics description
- Background
- TFE3 rRCC occurs when transcription factor binding to IGHM enhancer 3 (TFE3) gene located on chromosome Xp11.2 and a partner gene on either chromosome X or an autosome fuse (Adv Anat Pathol 2022;29:131, bioRxiv 2023 Aug 6 [Preprint])
- Translocation of TFE3 forms oncogenic fusions with over 20 different partner genes in RCC, leading to the upregulation of over 300 genes involved in cell growth and invasion
- Fusion partners thus far include ASPL (ASPSCR1), EWSR1, CLTC, DVL2, FUBP1, GRIPAP1, KAT6A, KHDRBS2, KHSRP, LUC7L3, MED15, NEAT1, NONO, PARP14, PRCC, RBM10, SETD1B, SFPQ, ZC3H4, SRRM2 (Mod Pathol 2024;37:100404)
- Loss of specific chromosomes, such as 9p and 22q, is associated with poor survival and higher tumor stages; ASPSCR1::TFE3 fusions are particularly aggressive and often show a loss of 22q
- Most common TFE3 gene fusion subtypes include ASPSCR1::TFE3 and PRCC::TFE3
- ASPSCR1::TFE3 (Nat Commun 2021;12:5262)
- 23.7% frequency
- Poor outcomes with overall survival of 5 years
- Aggressive nature supported by a molecular signature that increases angiogenesis and proliferation, low levels of cytotoxic T cells and frequent copy number alterations with 22q loss
- PRCC::TFE3 (Nat Commun 2021;12:5262)
- 23.7% frequency
- Lower incidence of copy number alterations with a more favorable molecular signature
- ASPSCR1::TFE3 (Nat Commun 2021;12:5262)
- Notably, 90% ccRCC cases exhibit mutations or methylation of the VHL gene; other frequently mutated genes in ccRCC include PBRM1 (50%), SETD2 (20%) and BAP1 (15%)
- In contrast, renal cell carcinomas resulting from rearrangements rarely harbor these mutations, underscoring that these are distinct entities (Mod Pathol 2024;37:100404)
- Conversely, TERT promoter mutations are present in both ccRCC and rRCC but are more prevalent in rRCC (ccRCC: 9.2%, rRCC: 18.2%) (Mod Pathol 2024;37:100404)
- Detection techniques
- TFE3 break apart probe for FISH is currently the gold standard for diagnosing TFE3 rRCC
- Separate signals indicate that a rearrangement has occurred; however, this probe does not provide information about the specific gene fusion partner
- While fusion probes targeting the TFE3 gene and its fusion partners are available, their clinical utility is limited due to the rarity of these tumors and the maintenance required to keep these probes in a reference lab
- RNA sequencing is a confirmatory molecular test due to possible false negative FISH results in case of cryptic fusions and intrachromosomal inversions, which can be seen in up to 10% of tumors, especially with low grade morphology (Genes Chromosomes Cancer 2022;61:219)
Videos
MiT family translocation renal cell carcinoma by Rajal Shah, M.D.
Sample pathology report
- Left kidney, core biopsy:
- Renal cell carcinoma, favor TFE3 rearranged subtype (see comment)
- Comment: Molecular studies for TFE3 translocation (RNA sequencing or FISH) will be attempted to confirm diagnosis and reported in an addendum. RNA sequencing is a preferred molecular test due to possible false negative FISH results in case of cryptic fusions and intrachromosomal inversions, which can be seen in up to 10% of tumors, especially with low grade morphology.
Differential diagnosis
- Clear cell renal cell carcinoma:
- TFE3 rRCC can have substantial overlap with clear cell RCC due to solid nested architecture and clear cytoplasm (Genes Chromosomes Cancer 2022;61:219)
- ccRCC would be immunopositive for CAIX and epithelial markers while immunonegative for TFE3, TRIM63 ISH and cathepsin K
- Clues to TFE3 rRCC would be younger patient age, hyalinized blood vessels (contrast to endothelial cell rich capillary network of clear cell RCC) and presence of psammoma bodies
- Clear cell papillary renal cell tumor (CCPRCT):
- TFE3 rRCC can have substantial overlap with CCPRCT due to branching tubular architecture and prominent subnuclear vacuolization (Genes Chromosomes Cancer 2022;61:219)
- Diffuse CK7 and CAIX labeling of CCPRCT distinguish it from TFE3 rRCC
- TFEB rearranged renal cell carcinoma:
- Unique histologic features include a biphasic morphology with large clear cells and smaller cells with condensed chromatin arranged around basement membrane material
- However, these features can be focal, making this tumor diagnostically challenging due to morphologic overlap
- Papillary renal cell carcinoma:
- TFE3 rRCC and pRCC both can have foamy histiocytes in the papillary cores
- Diffuse CK7 IHC favors pRCC and is usually negative in TFE3 rRCC
- Multilocular cystic renal neoplasm of low malignant potential (MCNLMP):
- MED15::TFE3 RCC is extensively cystic and can mimic MCNLMP
- MCNLMP is less likely to have psammoma bodies
Additional references
Practice question #1
Which of the following statements about MiT family translocation renal cell carcinomas (MiT RCC) is true?
- Clear cell renal cell carcinoma (ccRCC) is more aggressive than TFE3 rearranged RCC
- Immunohistochemistry for TFE3 is not helpful in the diagnosis of TFE3 rearranged RCC due to its low sensitivity
- MiT RCC primarily affects older adults, with a mean age of onset of over 60 years
- Presence of psammoma bodies in clear cell tumors is a characteristic feature of TFE3 rearranged RCC
- TFE3 rearranged RCC is typically negative for PAX8 immunohistochemistry
Practice answer #1
D. Presence of psammoma bodies in clear cell tumors is a characteristic feature of TFE3 rearranged RCC. TFE3 rRCC often presents with psammoma bodies, although psammoma bodies could be also seen in other RCC subtypes (thus not unique to TFE3 rRCC). Other key histologic features include large voluminous clear cells with discrete cell borders and papillary architecture.
Answer C is incorrect because MiT RCC affects younger patients, with TFE3 rearranged RCC having an average age of onset of ~40 years and TFEB altered RCC ~34 years.
Answer E is incorrect because TFE3 rRCC is often positive for PAX8 immunohistochemistry.
Answer A is incorrect because ccRCC and TFE3 rRCC have similar cancer specific survival (Am J Surg Pathol 2012;36:663).
Answer B is incorrect because TFE3 immunohistochemistry is highly sensitive (positive in 95% of cases), though it should be interpreted with caution due to potential positivity in other tumor types.
Comment Here
Reference: TFE3 rearranged renal cell carcinoma
Comment Here
Reference: TFE3 rearranged renal cell carcinoma
Practice question #2
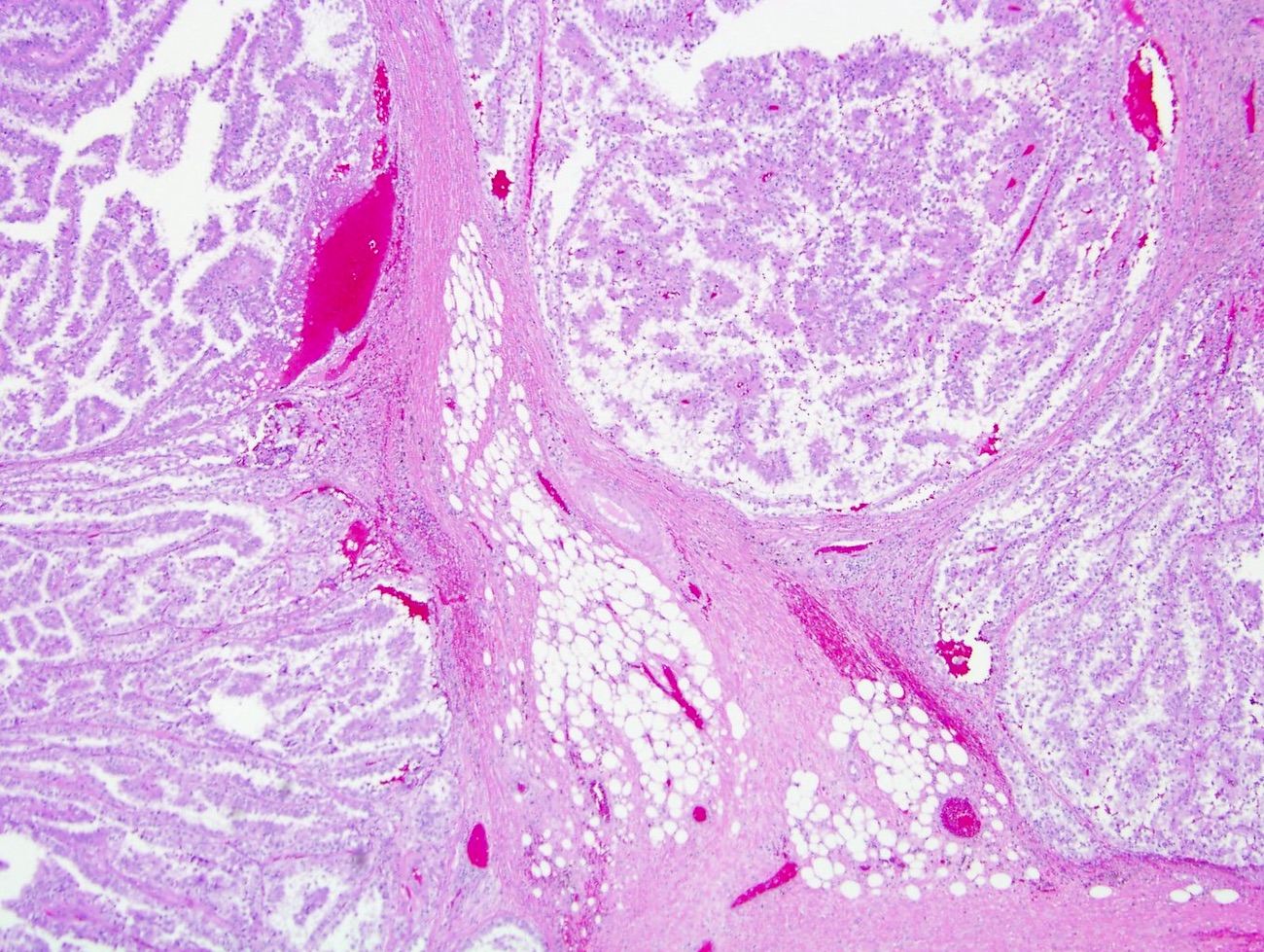
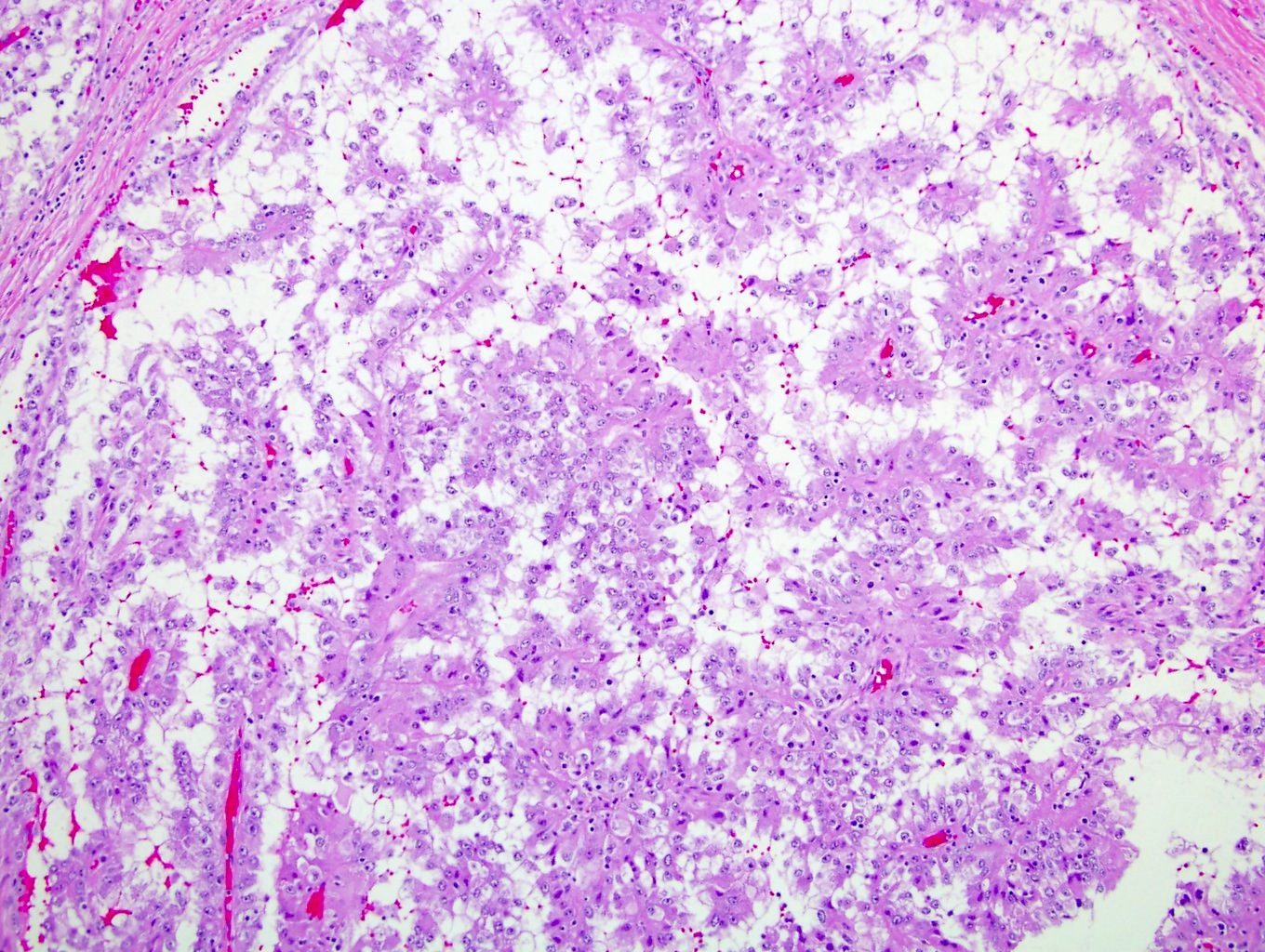
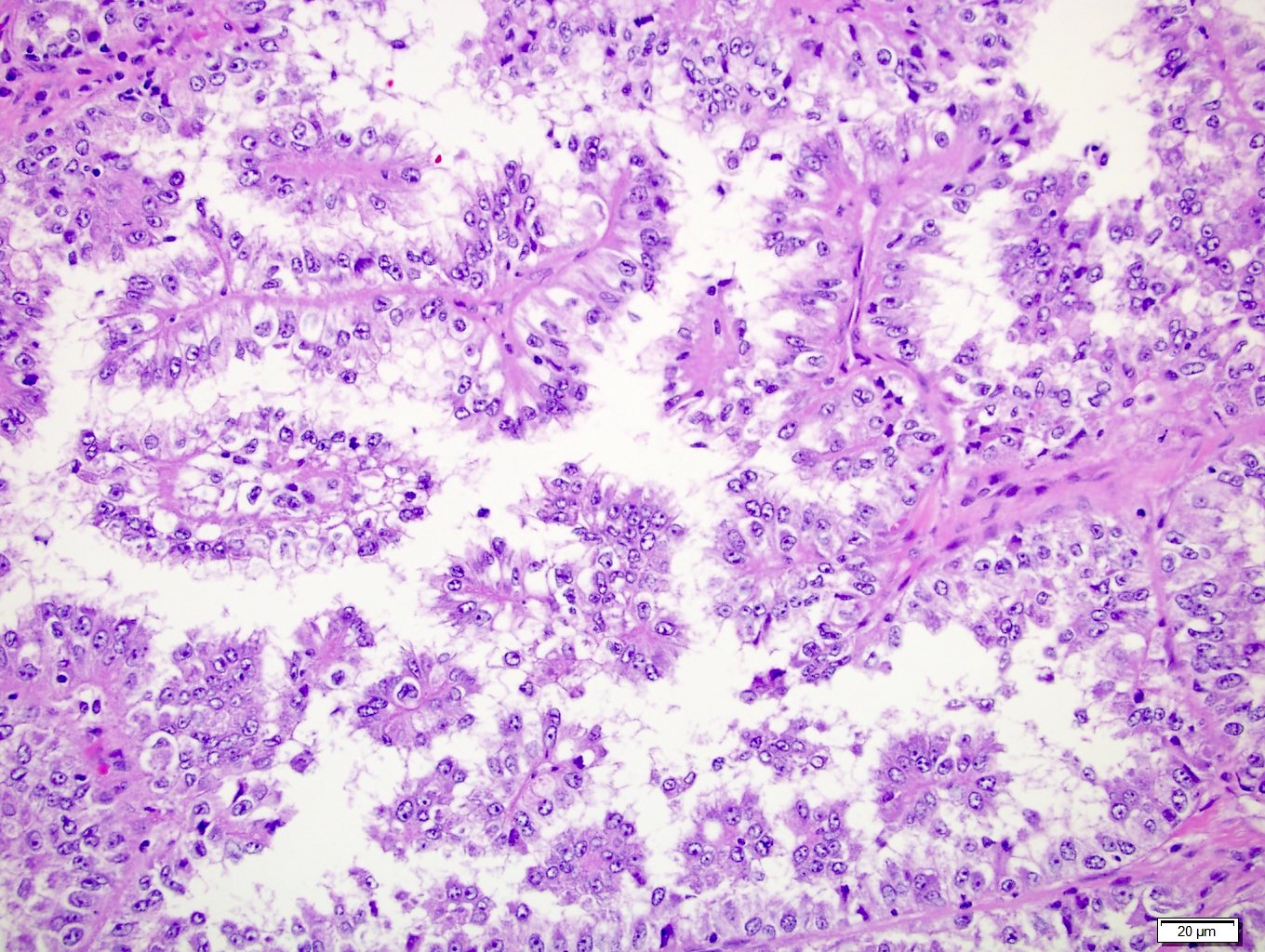
Based on the histologic features shown in the images above, what is the most likely diagnosis?
- Chromophobe renal cell carcinoma
- Clear cell papillary renal cell tumor
- Clear cell renal cell carcinoma
- Papillary renal cell carcinoma
- TFE3 rearranged renal cell carcinoma
Practice answer #2
E. TFE3 rearranged renal cell carcinoma. The images above illustrate key TFE3 rearranged renal cell carcinoma features, including papillary architecture, large cells with voluminous clear cytoplasm and prominent cell blistering. These cells are characteristically large, with well defined cell borders and discohesion, often resulting in free floating cell clusters.
Answer B is incorrect because this tumor typically shows a sawtooth or serrated architecture at low magnification and columnar cells that lack voluminous cytoplasm. Additionally, in a standard workup for clear cell renal neoplasm with this entity on the differential, CK and CAIX markers would be obtained. Clear cell papillary renal cell tumors would show characteristic cup-like staining with CAIX.
Answer C is incorrect because it is characterized by a chicken wire capillary pattern within the stroma between clusters of neoplastic cells, which is not observed in the images.
Answer D is incorrect because although the neoplasm exhibits a marked papillary architecture, the cells are too voluminous and there is characteristic blistering unique to TFE3 rearranged renal cell carcinoma, setting it apart.
Answer A is incorrect because this carcinoma is characterized by large voluminous cells with well defined borders, resulting in a plant-like morphology, which is not present in the images.
Comment Here
Reference: TFE3 rearranged renal cell carcinoma
Comment Here
Reference: TFE3 rearranged renal cell carcinoma
