Nasal cavity, paranasal sinuses, nasopharynx
Sinonasal carcinoma
High grade neuroendocrine carcinoma
Author: Bin Xu, M.D., Ph.D.
Editorial Board Member: Ruta Gupta, M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.

Last author update: 19 February 2024
Last staff update: 19 February 2024
Copyright: 2004-2025, PathologyOutlines.com, Inc.
PubMed Search: High grade neuroendocrine carcinoma
See Also: Laryngeal neuroendocrine neoplasm, Middle ear neuroendocrine tumor, Oropharnygeal neuroendocrine carcinoma, Salivary neuroendocrine carcinoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Xu B. High grade neuroendocrine carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/nasalsmallcell.html. Accessed September 18th, 2025.
Definition / general
- High grade / poorly differentiated neuroendocrine carcinoma, characterized by high mitotic count and (comedo type) tumor necrosis, morphologically similar to high grade neuroendocrine carcinoma occurring in other body sites
Essential features
- Diagnosis dependent on histologic and immunohistochemical evidence of neuroendocrine differentiation
- Can be further classified as small cell (neuroendocrine) carcinoma and large cell neuroendocrine carcinoma
- May be combined with another type of nonneuroendocrine carcinoma, most frequently squamous cell carcinoma, termed as combined carcinoma
Terminology
- Poorly differentiated neuroendocrine carcinoma
- Small cell carcinoma
- Small cell neuroendocrine carcinoma
- Large cell neuroendocrine carcinoma
- Neuroendocrine carcinoma, large cell type
ICD coding
Epidemiology
- Sinonasal small cell carcinoma accounts for ~35% of all head and neck small cell carcinomas (Laryngoscope 2017;127:1785)
- Mean age of presentation is in the 50s (Oral Oncol 2016;63:1, Int Forum Allergy Rhinol 2016;6:744, Laryngoscope 2017;127:1785)
Sites
- Nasal cavity, including nasal septum, is the most common site, being involved in 32 - 45% of cases (Int Forum Allergy Rhinol 2016;6:744, Laryngoscope 2017;127:1785)
- Other sites in descending order include maxillary sinus, ethmoid sinus, frontal sinus and sphenoid sinus
Etiology
- Subset is associated with high risk human papillomavirus (HPV) (Am J Surg Pathol 2013;37:185, Virchows Arch 2015;467:405)
Clinical features
- Nasal congestion and obstruction and epistaxis are the most common presenting symptoms, followed by facial pain, palpable facial mass and exophthalmos (Int Forum Allergy Rhinol 2016;6:744)
Diagnosis
- Diagnosis relies on demonstration of neuroendocrine differentiation, histologic features of small cell or large cell neuroendocrine carcinoma, high mitotic index (> 10 per 2 mm2) and tumor necrosis
Radiology description
- Destructive soft tissue mass of the sinonasal tract
Radiology images
Images hosted on other servers:

Mass of maxillary sinus
Prognostic factors
- Diagnosis designates a poor prognosis: 5 year disease specific survival of sinonasal small cell carcinoma is 46% (Oral Oncol 2016;63:1)
- Frequent local recurrence and distant metastasis despite multimodal therapy
- Stage does not appear to affect the prognosis (Oral Oncol 2016;63:1)
Case reports
- 22 year old woman with small cell carcinoma of the maxillary sinus (Natl J Maxillofac Surg 2013;4:111)
- 50 year old woman with HPV associated combined neuroendocrine carcinoma and squamous cell carcinoma in the nasal cavity (Head Neck Pathol 2022;16:1227)
- 56 year old woman with large cell neuroendocrine carcinoma of the nasal cavity (NMC Case Rep J 2021;8:485)
- 68 year old man with small cell carcinoma of the paranasal sinus with intraoral extension (J Oral Maxillofac Pathol 2017;21:286)
Treatment
- There are no specific management guidelines due to rarity of the tumor
- Multimodality treatment has been used with variable results
- Most common treatment modality is combined chemotherapy and radiation therapy (Int Forum Allergy Rhinol 2016;6:744)
Clinical images
Images hosted on other servers:

Expansile swelling of maxilla
Microscopic (histologic) description
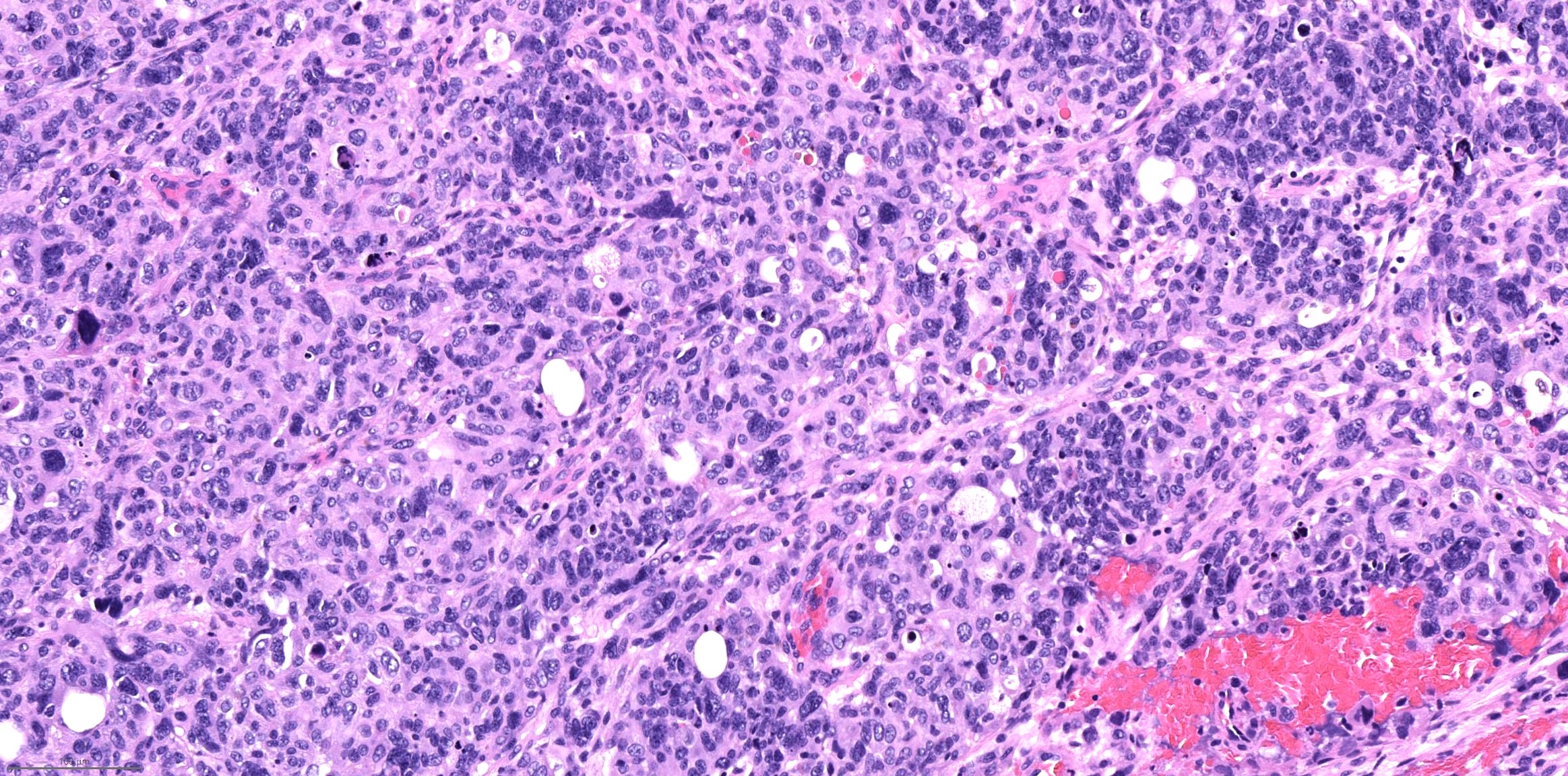
- High grade neuroendocrine carcinoma (general features)
- Mitotic index > 10 mitoses per 2 mm2, frequent apoptotic bodies and tumor necrosis
- Solid sheets or trabeculae of tumor cells, sometimes with peripheral palisading or rosette formation
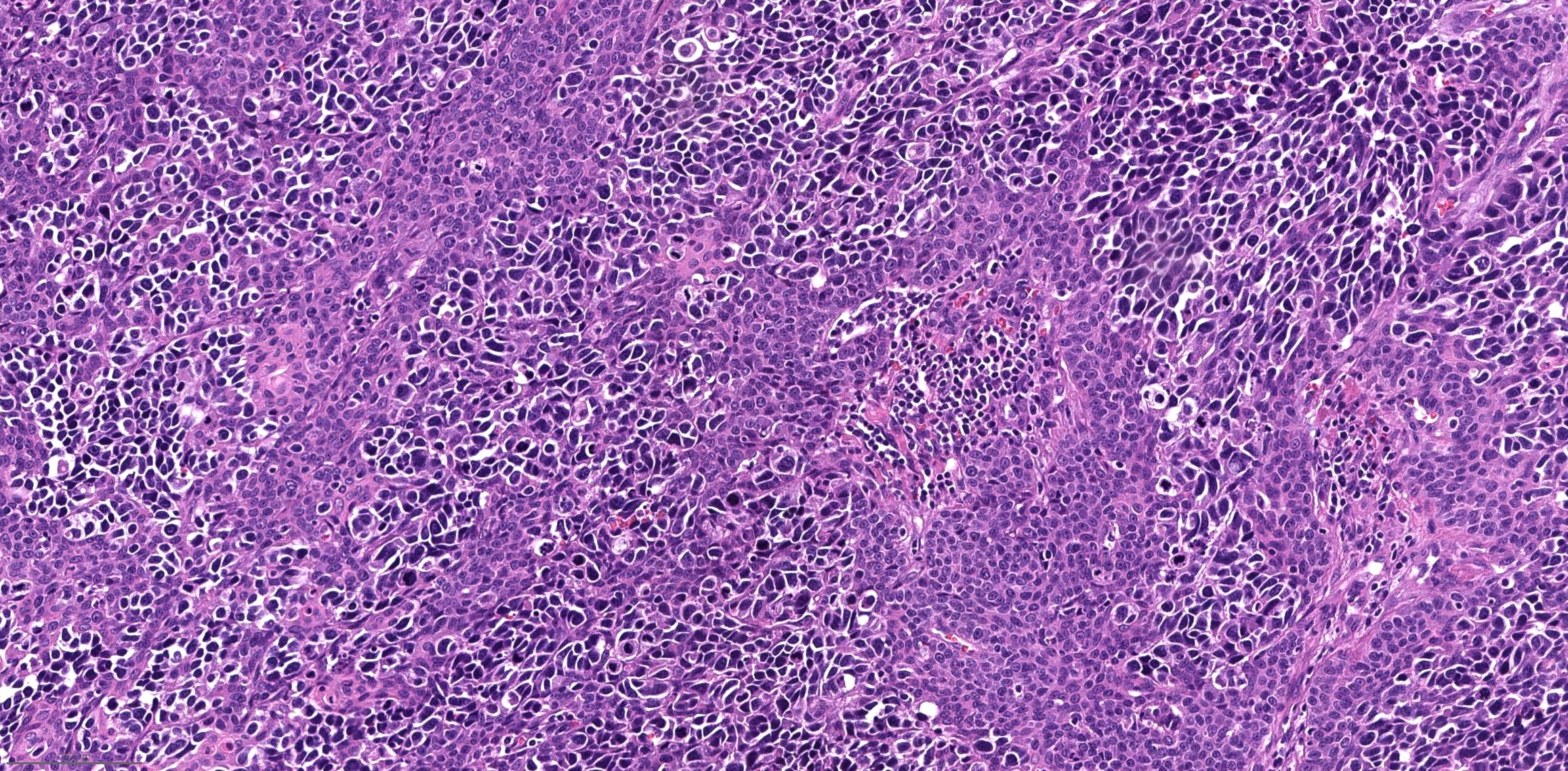
- Small cell carcinoma
- Small to medium sized cells: the diameter of tumor cells is < 3 times the diameter of a lymphocyte
- Scanty cytoplasm and indistinct cell boundary
- Finely granular salt and pepper chromatin
- No or inconspicuous nuclei
- Nuclear molding (conformity of adjacent nuclei to one another), nuclear spindling and crush artifacts of the nuclei may be seen
- Large cell neuroendocrine carcinoma
- Large sized cells: the diameter of tumor cells is > 3 times the diameter of a lymphocyte
- Abundant amphophilic to eosinophilic cytoplasm and distinct cell membrane
- Large nuclei with prominent nucleoli; chromatin pattern is variable, ranging from granular, vesicular, to coarse
- Combined neuroendocrine carcinoma
- Tumor that is composed of a high grade neuroendocrine carcinoma and a nonneuroendocrine carcinoma, commonly a squamous cell carcinoma
Microscopic (histologic) images
Contributed by Bin Xu, M.D., Ph.D.
Small cell carcinoma
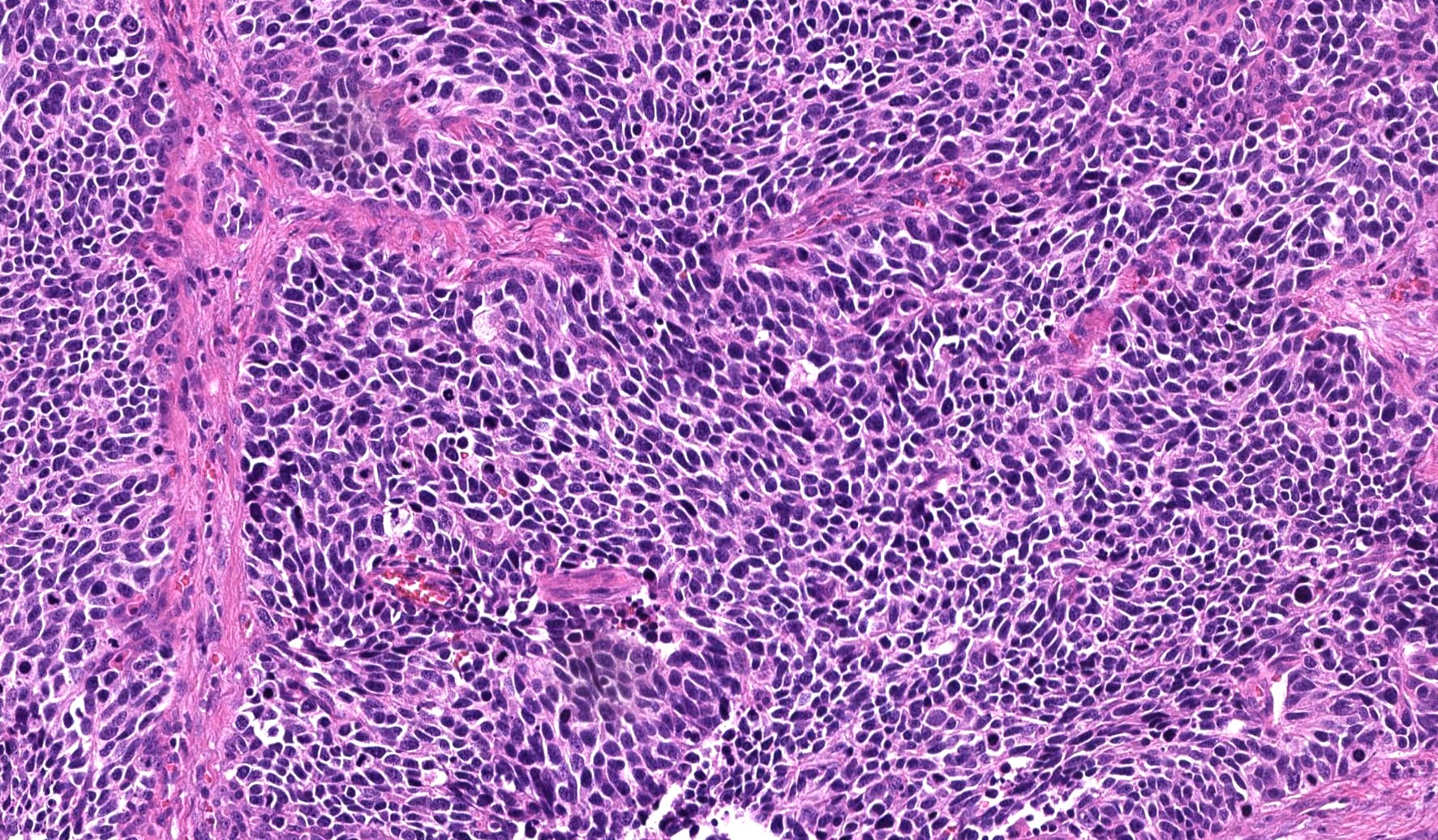
Finely granular chromatin
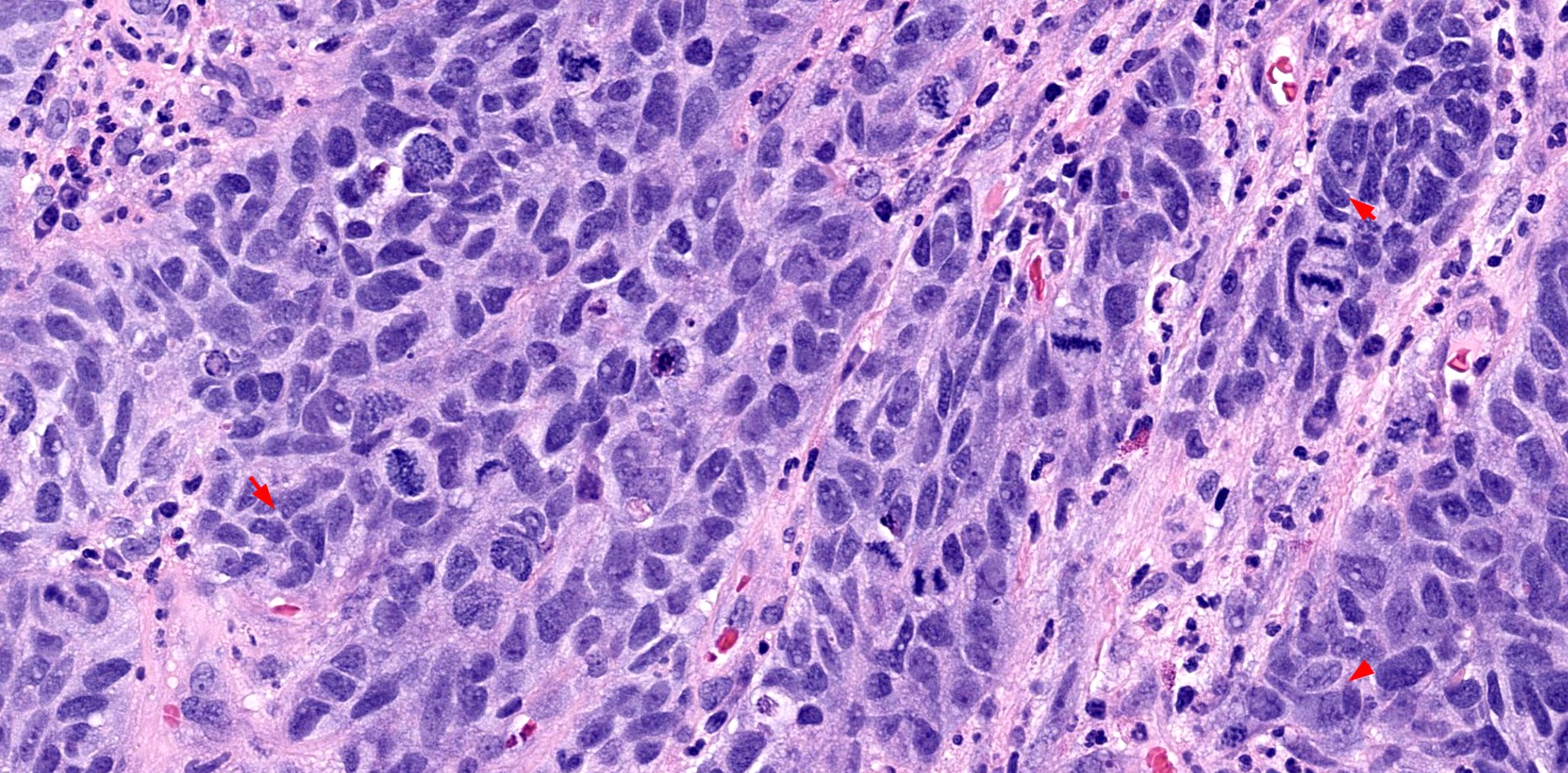
Frequent mitoses and nuclear molding
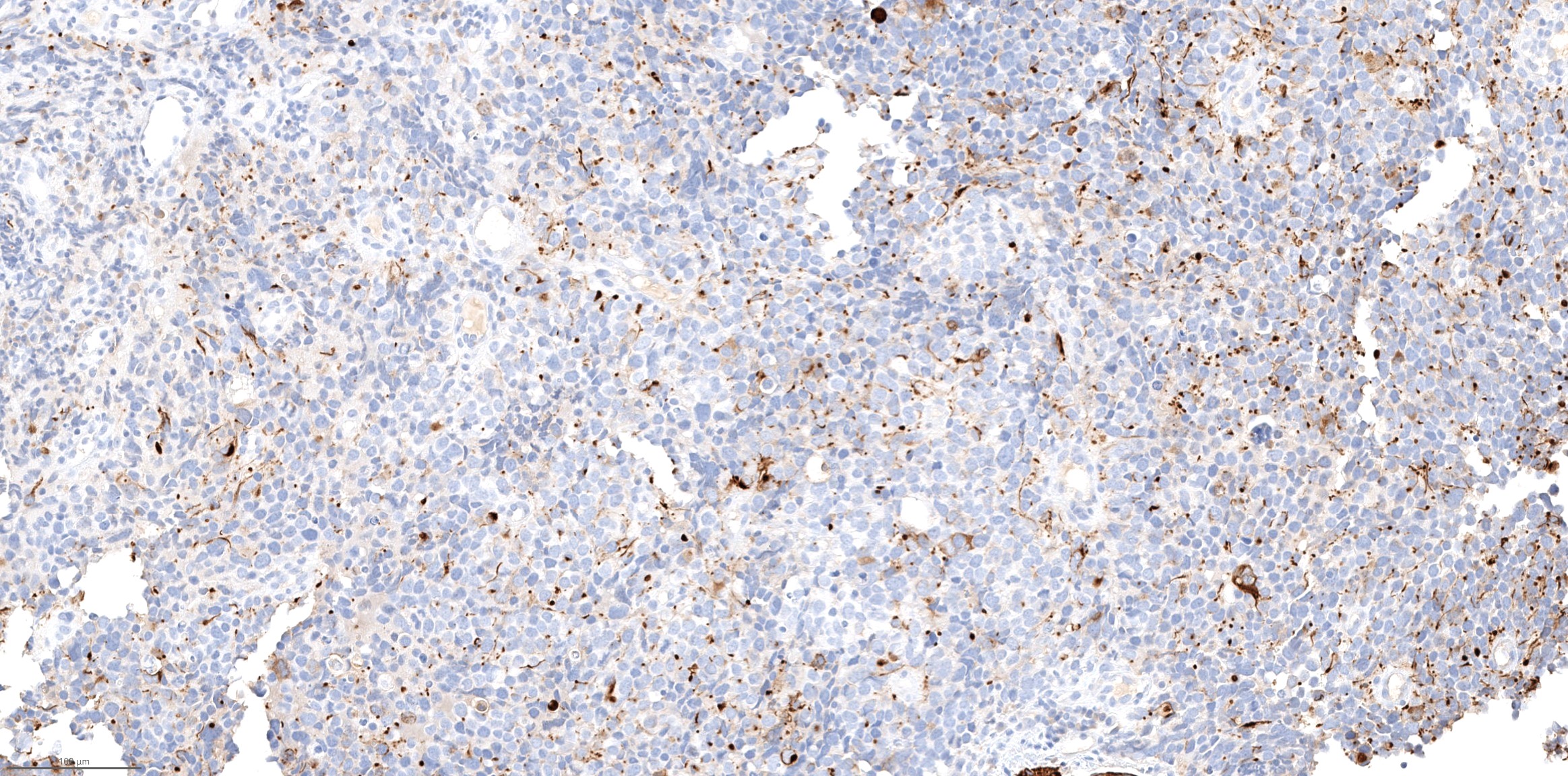
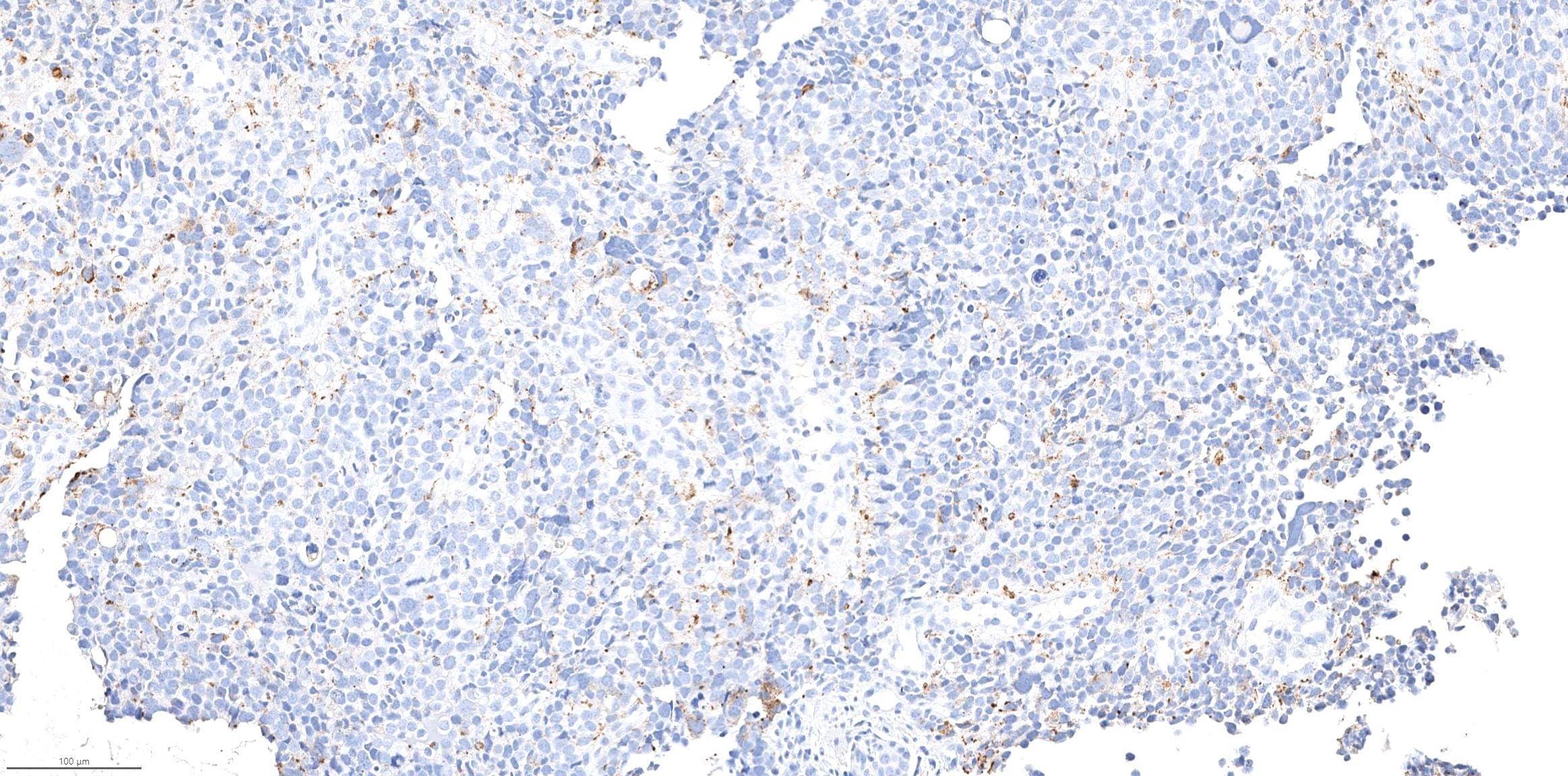
CAM5.2 (dot-like pattern)
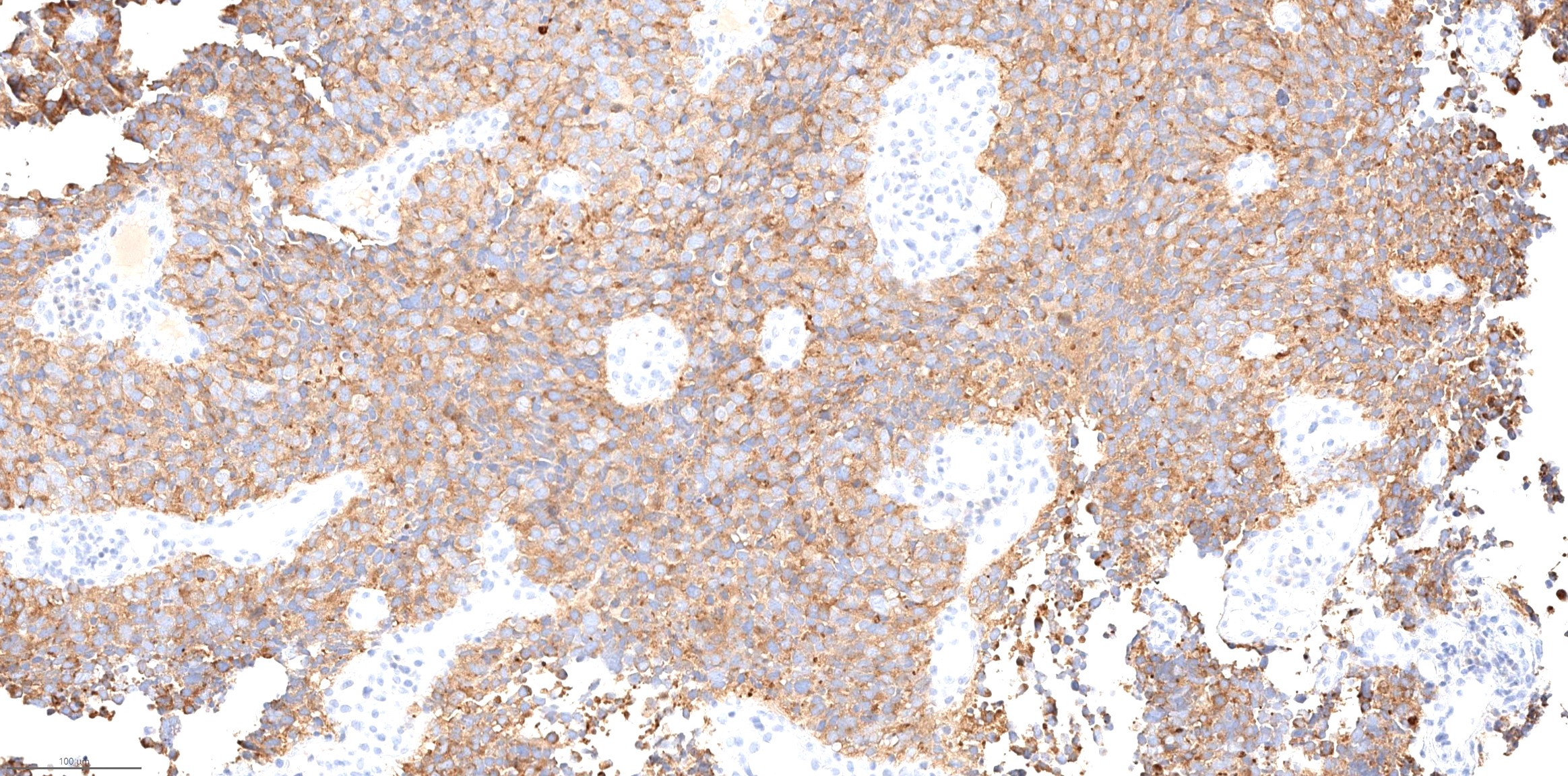
Synaptophysin
Chromogranin
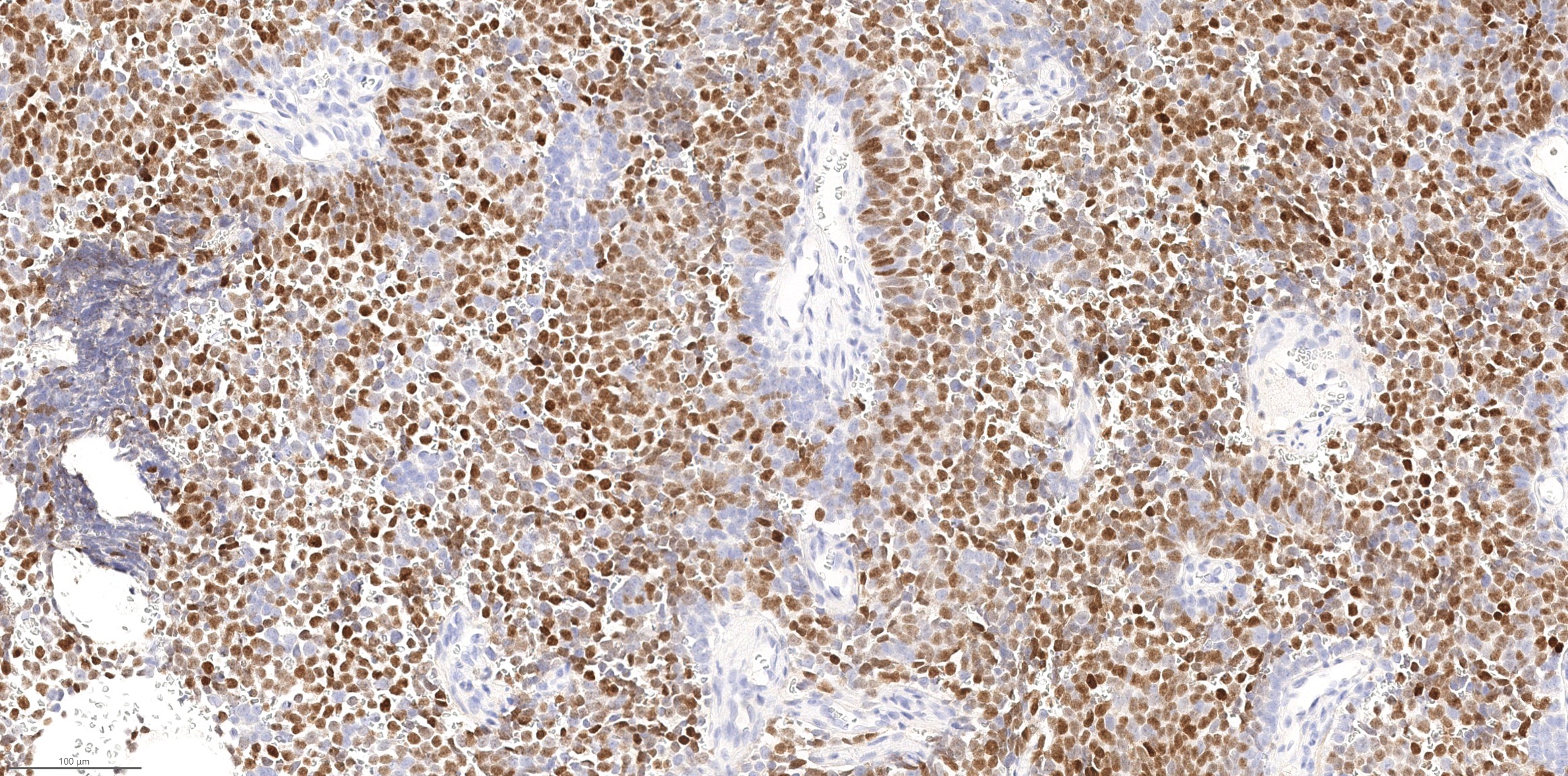
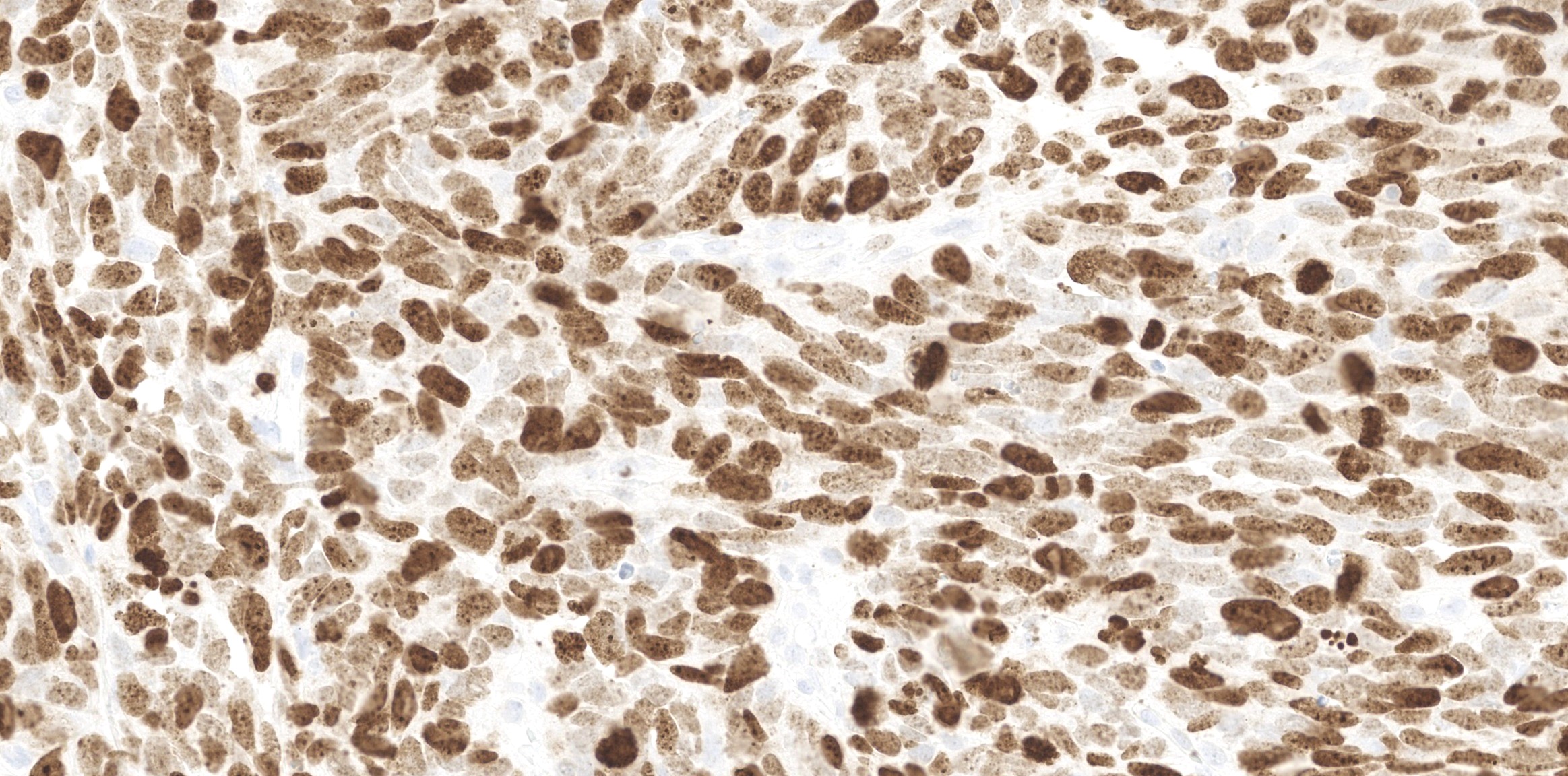
INSM1
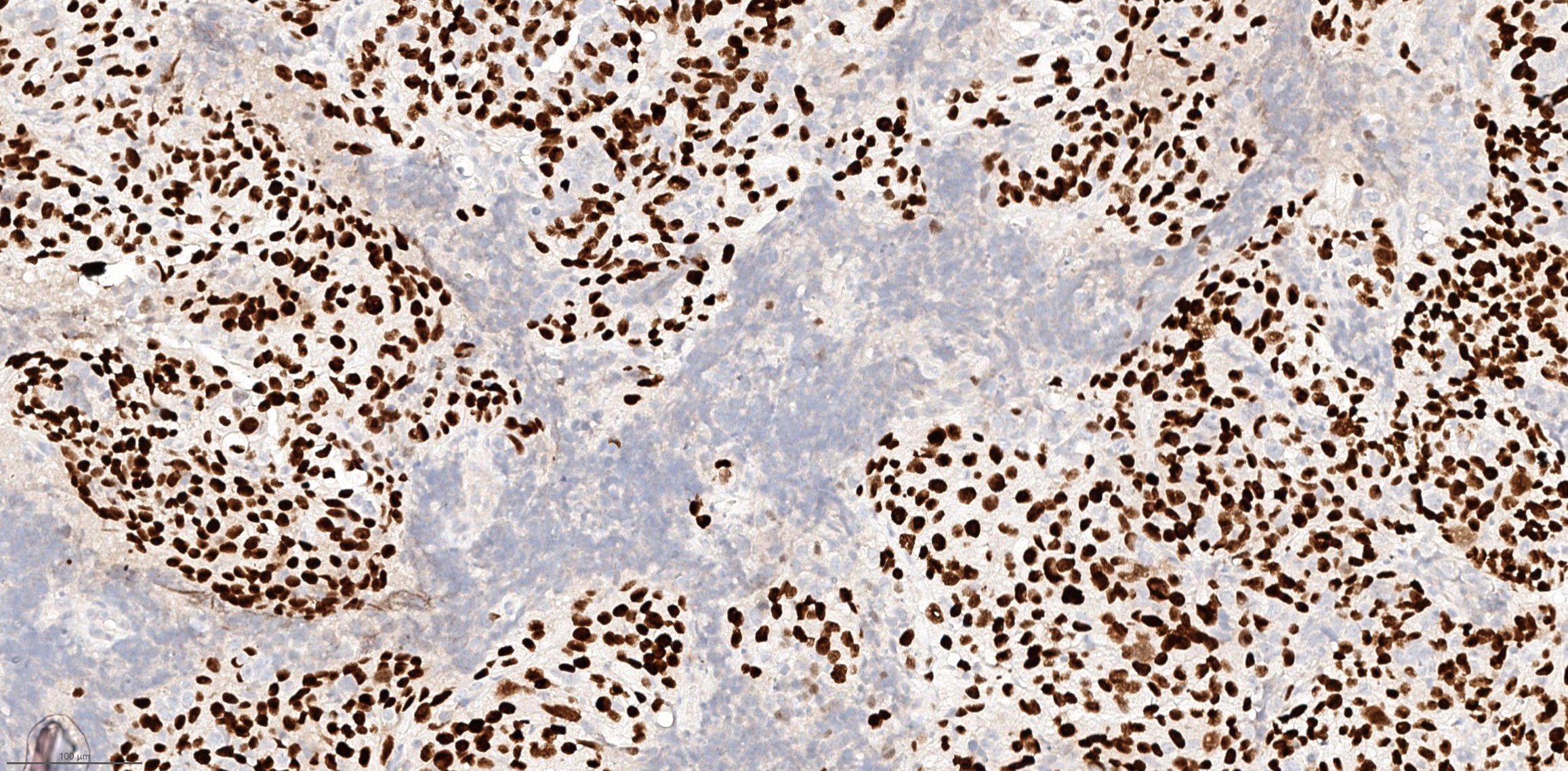
Elevated Ki67 proliferation index

TTF1
Large cell neuroendocrine carcinoma
Large tumor cells
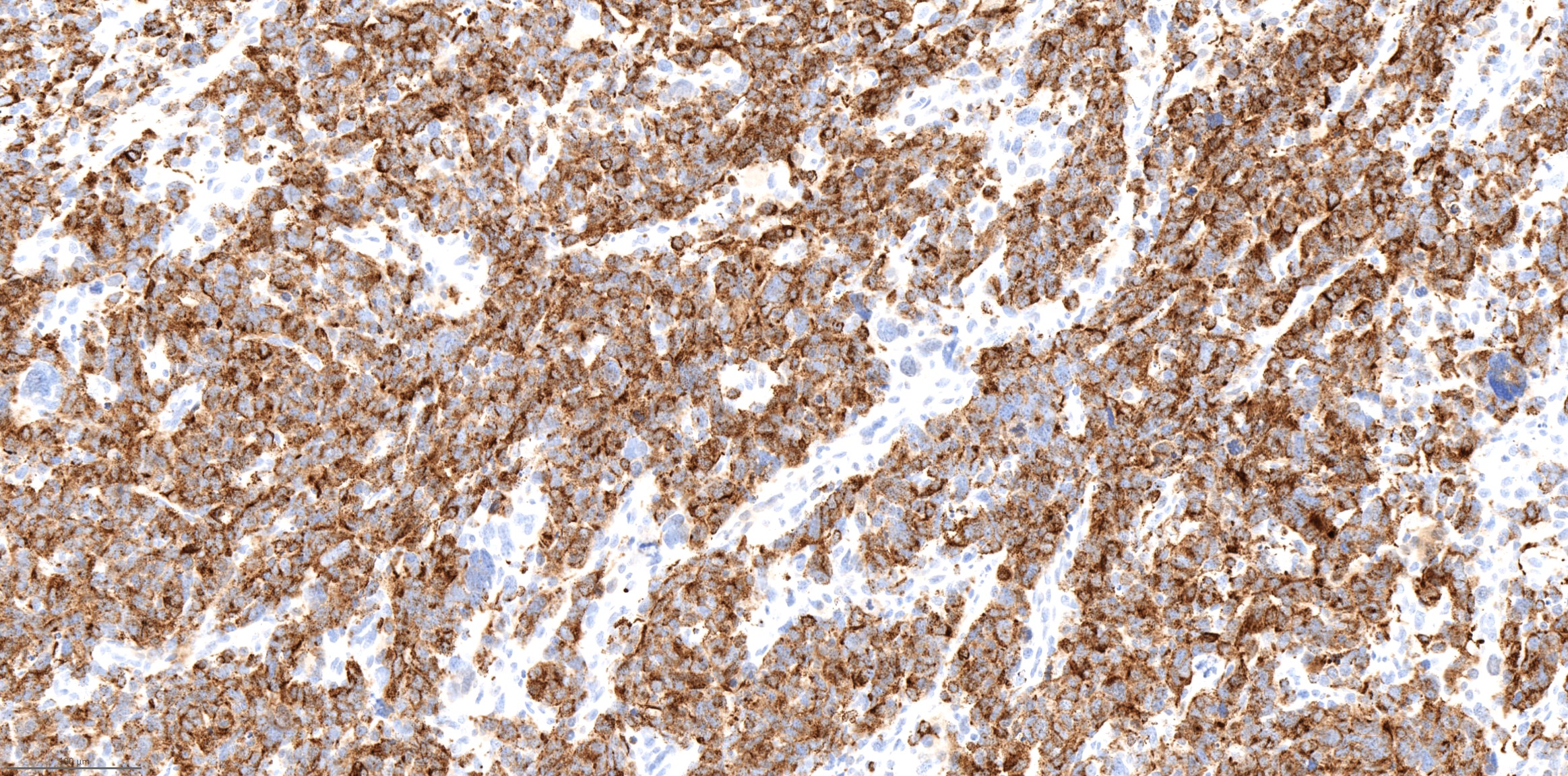
Synaptophysin
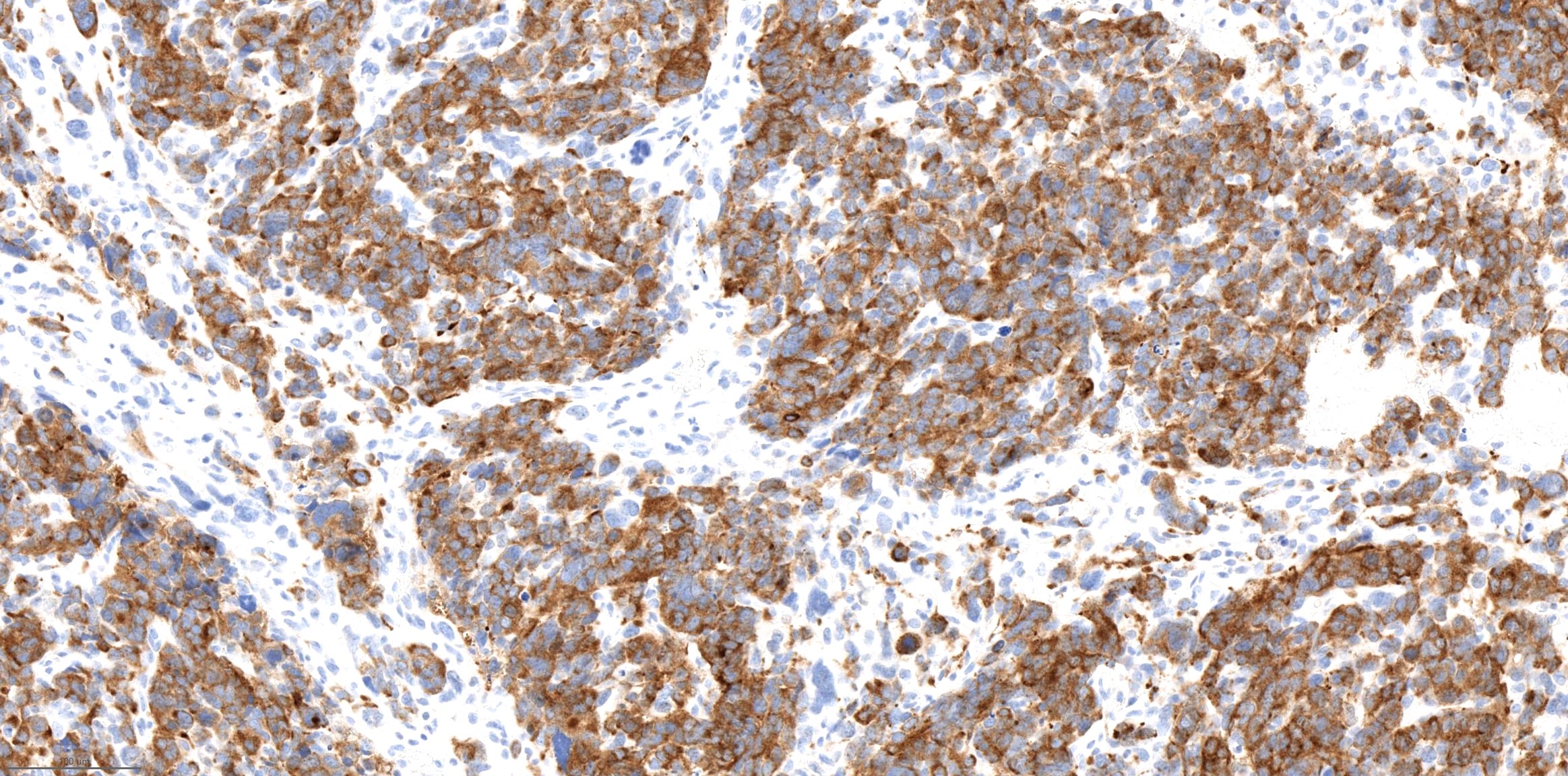
Chromogranin
Combined small cell carcinoma and squamous cell carcinoma
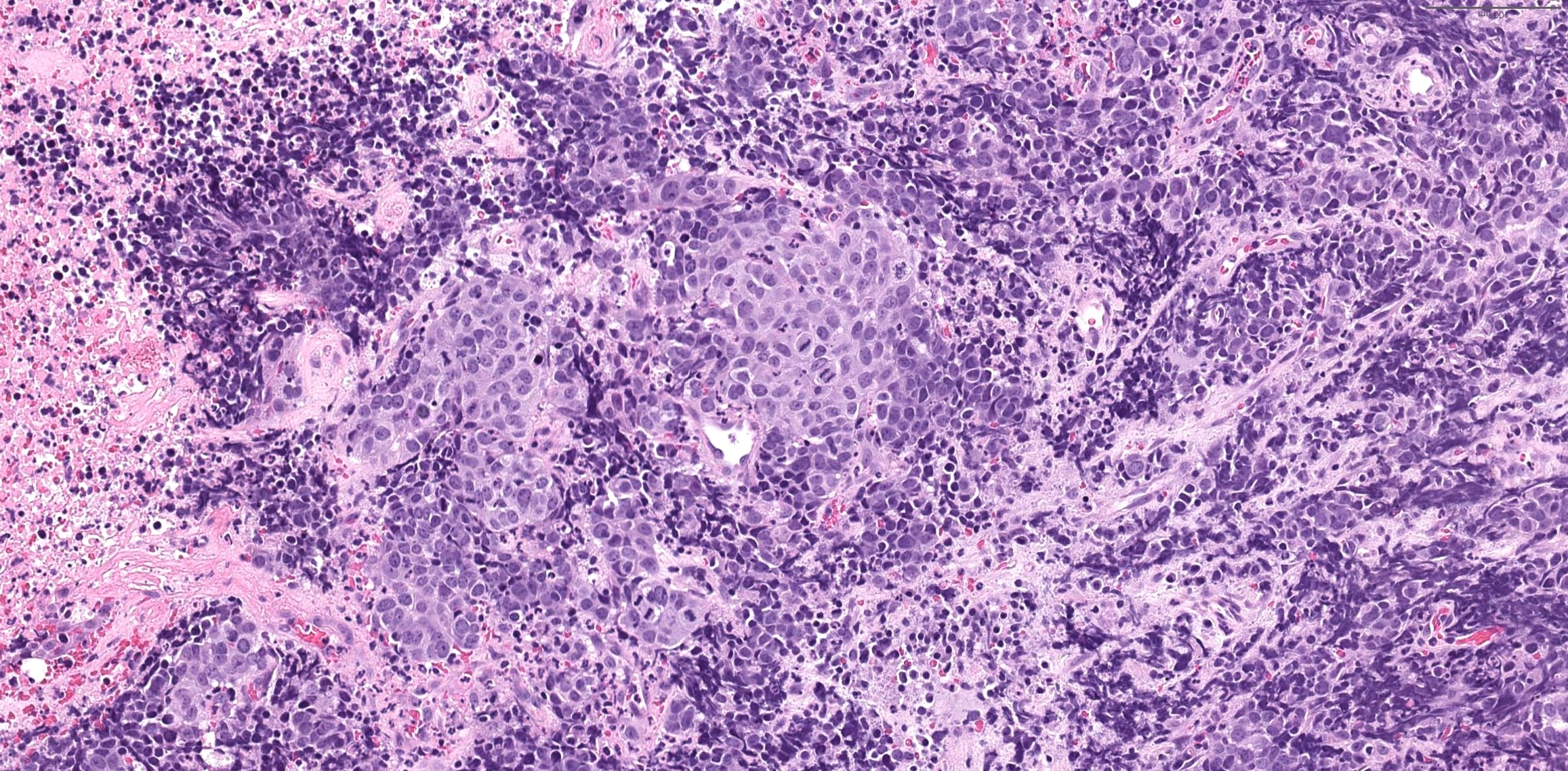
Squamous and neuroendocrine component
p40
Cytology description
- Small cell carcinoma: hypercellular sample, individual cells or small loose clusters, hyperchromatic nuclei, no nucleoli, nuclear molding, crush artifact and necrotic background
Cytology images
Contributed by Bin Xu, M.D., Ph.D.
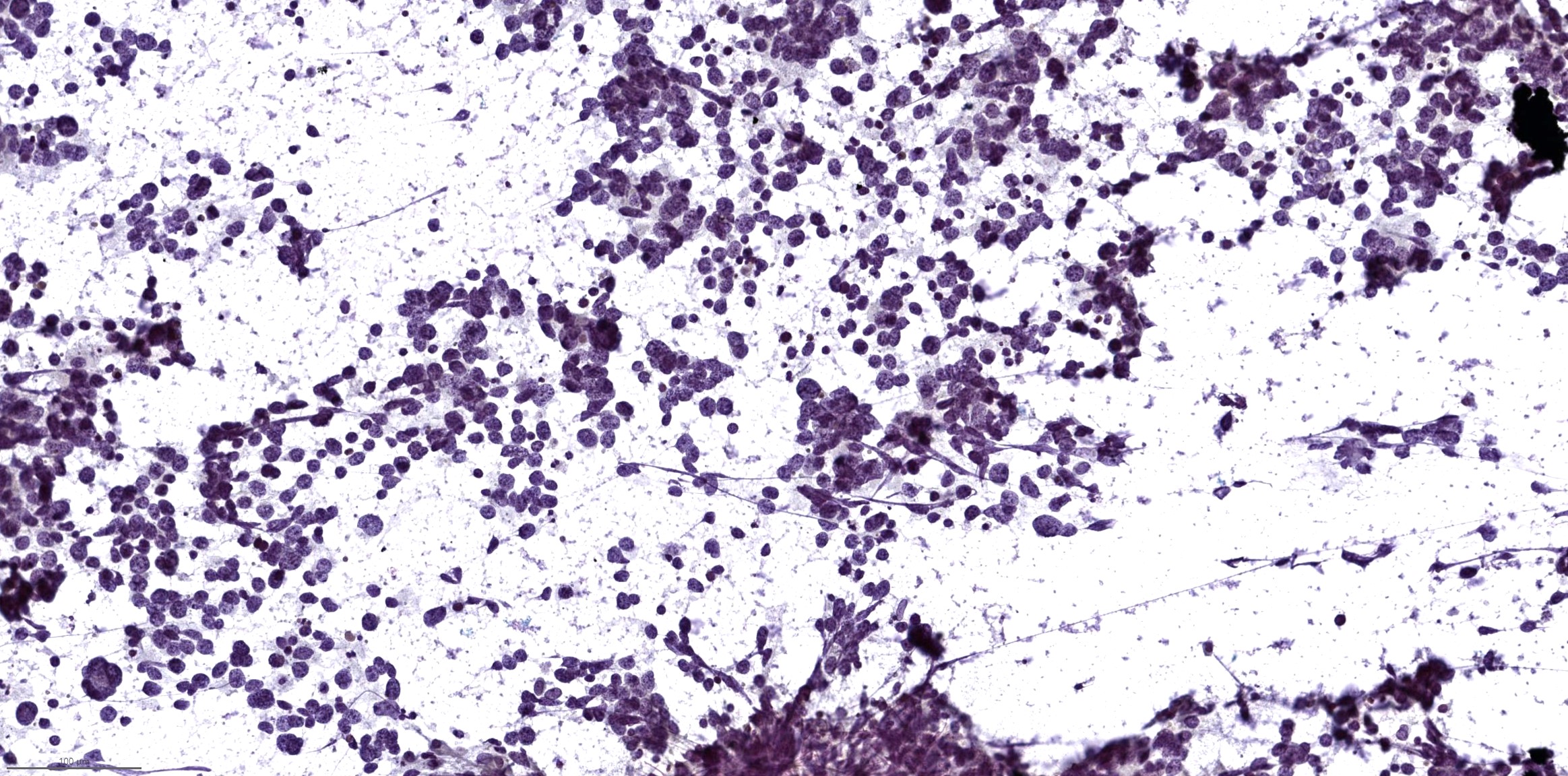
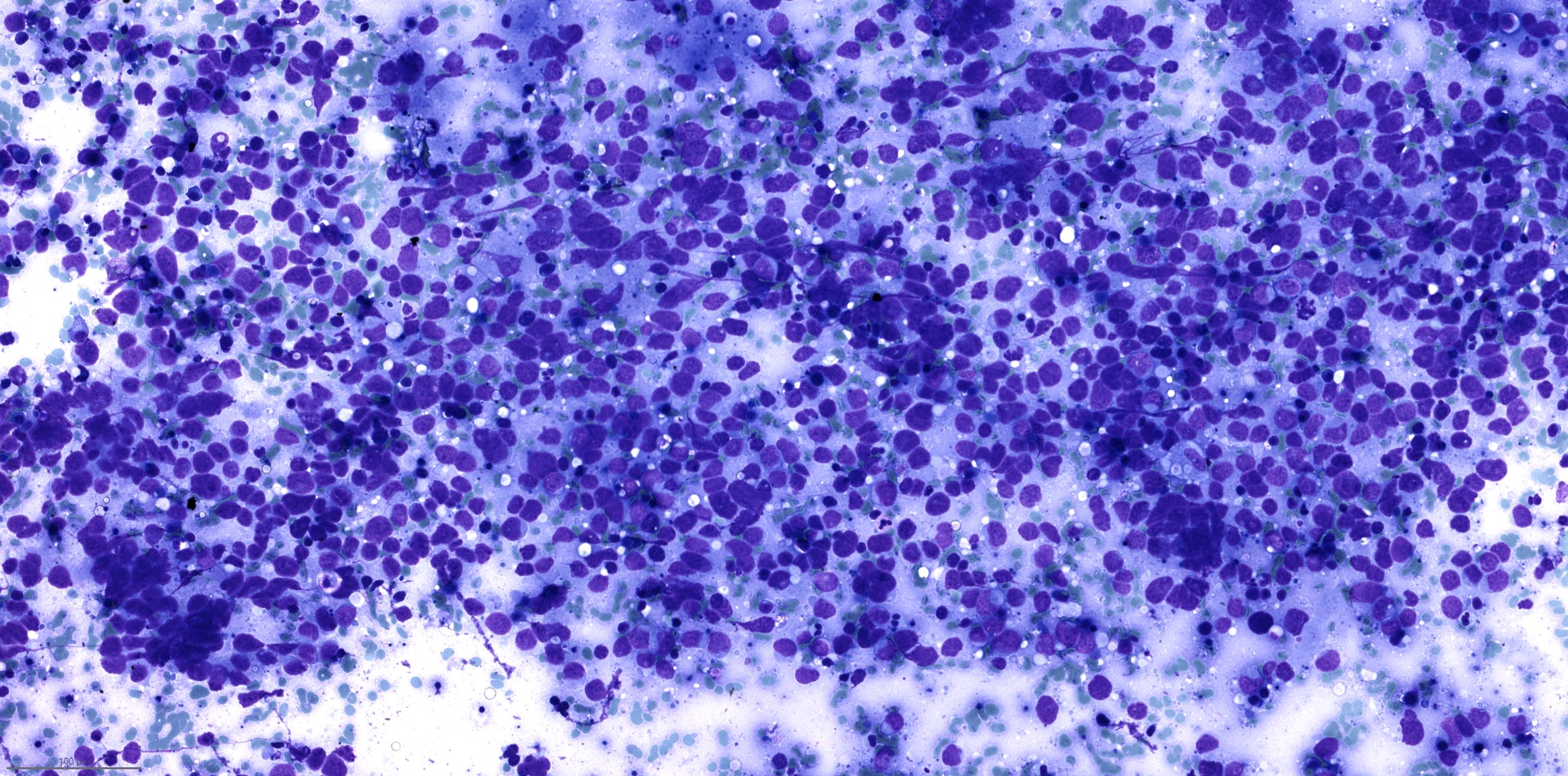
Small cell carcinoma
Positive stains
- Neuroendocrine markers such as chromogranin, synaptophysin and INSM1
- Cytokeratin AE1 / AE3 and CAM5.2: often show perinuclear dot-like staining pattern
- EMA
- TTF1 can be positive in high grade neuroendocrine carcinoma of sinonasal tract (Hum Pathol 2002;33:642)
- Ki67 proliferation index: by definition > 20% but is often much higher (> 50%)
Negative stains
- NUT
- No loss of SWF / SNF pathway proteins: immunoexpression of INI1 / SMARCB1 or SMARCA4 / BRG1 is retained
- S100
Molecular / cytogenetics description
- Subset of large cell neuroendocrine carcinoma has IDH2 R172 mutation (Mod Pathol 2019;32:1447)
- Small cell carcinoma does not have IDH2 mutation but may harbor ARID1A mutation (Mod Pathol 2019;32:1447)
Sample pathology report
- Nasal cavity, biopsy:
- Small cell carcinoma (high grade neuroendocrine carcinoma, small cell carcinoma type) (see comment)
- Comment: Immunohistochemistry studies show that the tumor is diffusely positive for synaptophysin, chromogranin, INSM1, cytokeratin AE1 / AE3 and CAM5.2, whereas it is negative for S100 and NUT. Immunoexpression of SMARCA2, SMARCA4 and SMARCB1 is retained in this tumor. Ki67 proliferation index is > 90%. The overall histologic features and immunoprofile support the diagnosis.
Differential diagnosis
- Olfactory neuroblastoma:
- Both entities are positive for synaptophysin and chromogranin
- Olfactory neuroblastoma usually has S100 positive sustentacular network and is negative for keratins (such as cytokeratin AE1 / AE3 and CAM5.2) and EMA
- Low grade olfactory neuroblastoma lacks necrosis and has a low mitotic index
- NUT carcinoma:
- Synaptophysin and chromogranin positivity can be seen in NUT carcinoma (Hum Pathol 2022;126:87)
- NUT immunopositivity or detection of NUTM1 translocation is essential for the diagnosis
- SWI / SNF complex deficient sinonasal carcinoma:
- 52% of SMARCB1 deficient sinonasal carcinomas express synaptophysin or chromogranin (Hum Pathol 2020;104:105)
- Loss of immunoexpression of SMARCB1, SMARCA2 or SMARCA4 is required for the diagnosis
- Sinonasal undifferentiated carcinoma (SNUC):
- SNUC can show very focal synaptophysin and chromogranin positivity (Am J Surg Pathol 2001;25:156)
- More than focal or diffuse synaptophysin and chromogranin immunopositivity excludes a diagnosis of SNUC
Additional references
Practice question #1
A biopsy was performed from a nasal cavity mass of a 60 year old man. The H&E, CAM5.2 and synaptophysin immunohistochemistry slides are shown above. What is the diagnosis?
- Large cell neuroendocrine carcinoma
- Olfactory neuroblastoma
- Sinonasal undifferentiated carcinoma
- Small cell carcinoma
Practice answer #1
D. Small cell carcinoma. The tumor shows diffuse synaptophysin expression and perinuclear dot-like expression of CAM5.2. The tumor cells have scanty cytoplasm, salt and pepper chromatin, inconspicuous nuclei, frequent mitoses and apoptotic bodies. Answer C is incorrect because diffuse synaptophysin expression excludes a diagnosis of sinonasal undifferentiated carcinoma. Answer B is incorrect because olfactory neuroblastoma is cytokeratin negative, while this tumor expresses CAM5.2. Answer A is incorrect because the tumor cells lack abundant cytoplasm and prominent nucleoli.
Comment Here
Reference: High grade neuroendocrine carcinoma
Comment Here
Reference: High grade neuroendocrine carcinoma
Practice question #2
Which of the following statements is true for high grade neuroendocrine carcinoma of the sinonasal tract?
- It is generally positive for INSM1 and S100
- It is universally negative for high risk human papillomavirus (HPV), distinguishing it from HPV related squamous cell carcinoma and HPV related multiphenotypic sinonasal carcinoma
- It may coexist with a squamous cell carcinoma
- Ki67 proliferation index is between 2% and 20%
Practice answer #2
C. It may coexist with a squamous cell carcinoma. High grade neuroendocrine carcinoma may coexist with a nonneuroendocrine carcinoma component (i.e., combined carcinoma). Answer B is incorrect because a subset can be positive for high risk human papillomavirus. Answer D is incorrect because Ki67 by definition should be > 20%. Answer A is incorrect because it is generally negative for S100.
Comment Here
Reference: High grade neuroendocrine carcinoma
Comment Here
Reference: High grade neuroendocrine carcinoma
