Thyroid & parathyroid
Other common thyroid carcinomas
Poorly differentiated thyroid carcinoma
Author: Shuanzeng (Sam) Wei, M.D., Ph.D.

Last author update: 1 November 2017
Last staff update: 6 September 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Poorly differentiated carcinoma [title] thyroid
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Etiology | Clinical features | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1Cite this page: Wei S. Poorly differentiated thyroid carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidinsular.html. Accessed September 29th, 2025.
Definition / general
- Malignant follicular cell neoplasm with limited evidence of follicular cell differentiation
- Intermediate clinical behavior between well differentiated (papillary and follicular carcinoma) and anaplastic carcinoma (Am J Surg Pathol 2007;31:1256, Surg Pathol Clin 2014;7:475, Lloyd: WHO Classification of Tumours of Endocrine Organs, 4th Edition, 2017)
Essential features
- Intermediate grade follicular cell carcinoma with limited evidence of follicular cell differentiation
Terminology
- Insular / trabecular carcinoma
- Primordial cell carcinoma
- Poorly differentiated follicular carcinoma
- Poorly differentiated papillary carcinoma
- Solid type follicular carcinoma
- High risk thyroid carcinoma of follicular cell origin
ICD coding
- ICD-10: C73 - malignant neoplasm of thyroid gland
Epidemiology
- Older patients, mean age 55 - 63 years
- 0.3 - 6.7% of thyroid carcinomas
- More common in Europe and South America than U.S. (Mod Pathol 2010;23:1269)
Etiology
- Iodine deficiency may be a risk factor; no association with radiation exposure (Clin Oncol (R Coll Radiol) 2011;23:261)
- Some tumors are de novo; some arise from dedifferentiation of follicular or papillary carcinoma
Clinical features
- Large solitary thyroid mass. Patient may have a history of recent growth in a longstanding uninodular or multinodular thyroid (Am J Surg Pathol 1984;8:655)
- Intermediate behavior between well differentiated and anaplastic carcinoma (World J Surg 2007;31:934)
- Has nodal and hematogenous metastases and 3 year survival of 38% (Langenbecks Arch Surg 2007;392:671)
- Extends to perithyroidal soft tissue in 60 - 70% cases
- Vascular invasion in 60 - 90% cases
- Regional lymph node metastasis in 15 - 65%
- Distant metastasis in 40 - 70%
Radiology description
- Ultrasound shows inhomogeneous hyoechoic mass (Cancer 2006;106:1286)
- Cold on scintigraphy and positive on FDG PET
Prognostic factors
- Tumors with overall 5 year survival rate: 60 - 70% (J Clin Endocrinol Metab 2014;99:1245)
- Poor prognosis associated with high stage and older age (> 45 years)
Case reports
- 4 year old girl with metastatic disease (Am J Otolaryngol 2009;30:61)
- 26 year old African American woman with benign biopsy but compressive symptoms (Case #435)
- 57 year old woman with unusual short term complete response to chemotherapy (J Clin Endocrinol Metab 2012;97:3046)
- 60 year old woman with metastatic poorly differentiated thyroid carcinoma within an intracranial meningioma (J Clin Endocrinol Metab 2014;99:3513)
- 64 year old woman with tumor arising from ectopic thyroid (Am J Clin Pathol 1995;104:408)
- 75 year old woman with superior vena cava metastasis (J Clin Oncol 2015;33:e119)
- 80 year old woman with neck mass (University of Pittsburgh: Case 24 - Neck Mass)
- 82 year old woman with extensive extracellular mucin in tumor (Hum Pathol 2005;36:698)
Treatment
- Total thyroidectomy, neck dissection, radioactive iodine and suppressive thyroxine
Gross description
- Large (median size: 5 cm), grayish white, some show soft pale areas of necrosis
- Pushing margins, may be partially encapsulated
- Can have satellite nodules (Am J Surg Pathol 1984;8:655)
Gross images
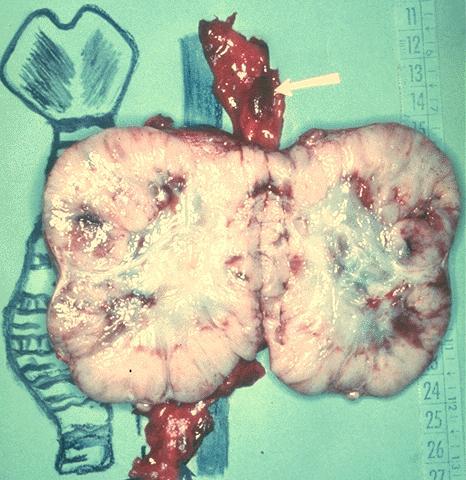
Contributed by Mark R. Wick, M.D. and AFIP images
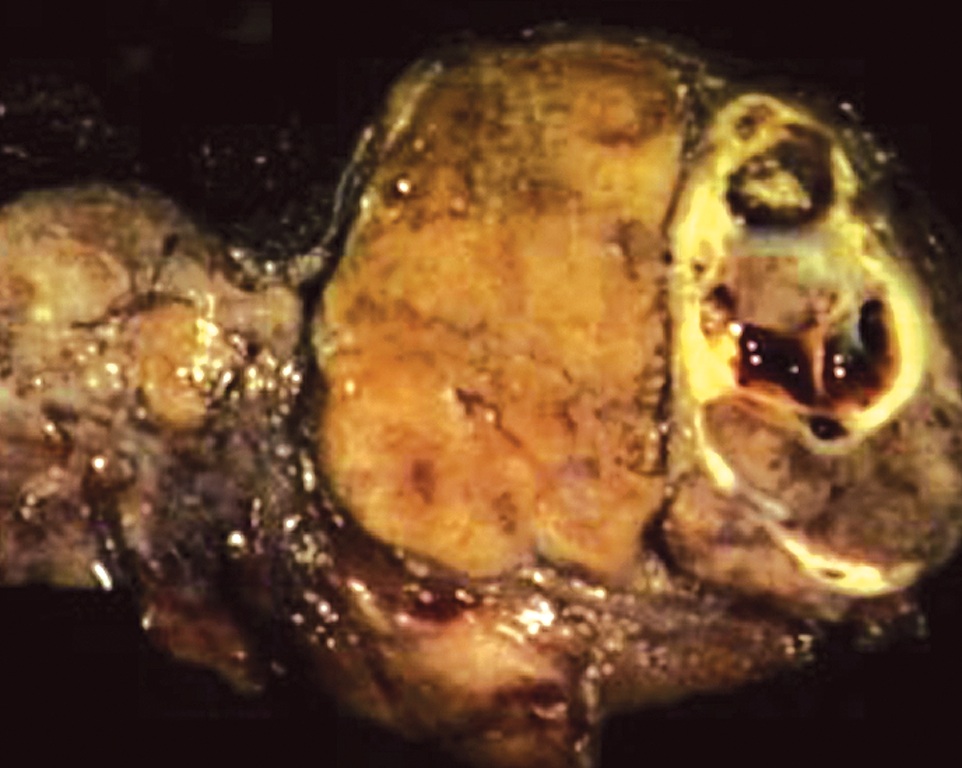
Various images
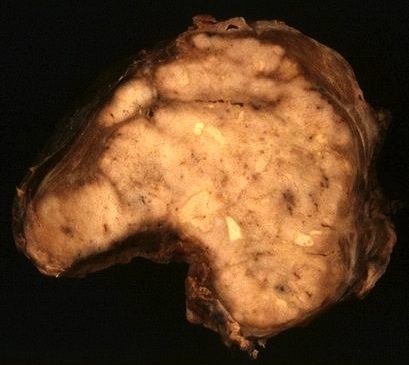
Poorly differentiated thyroid carcinoma
Massive cervical lymph node metastasis
Images hosted on other servers:

A well demarcated tumor

Tumor with invasive growth pattern
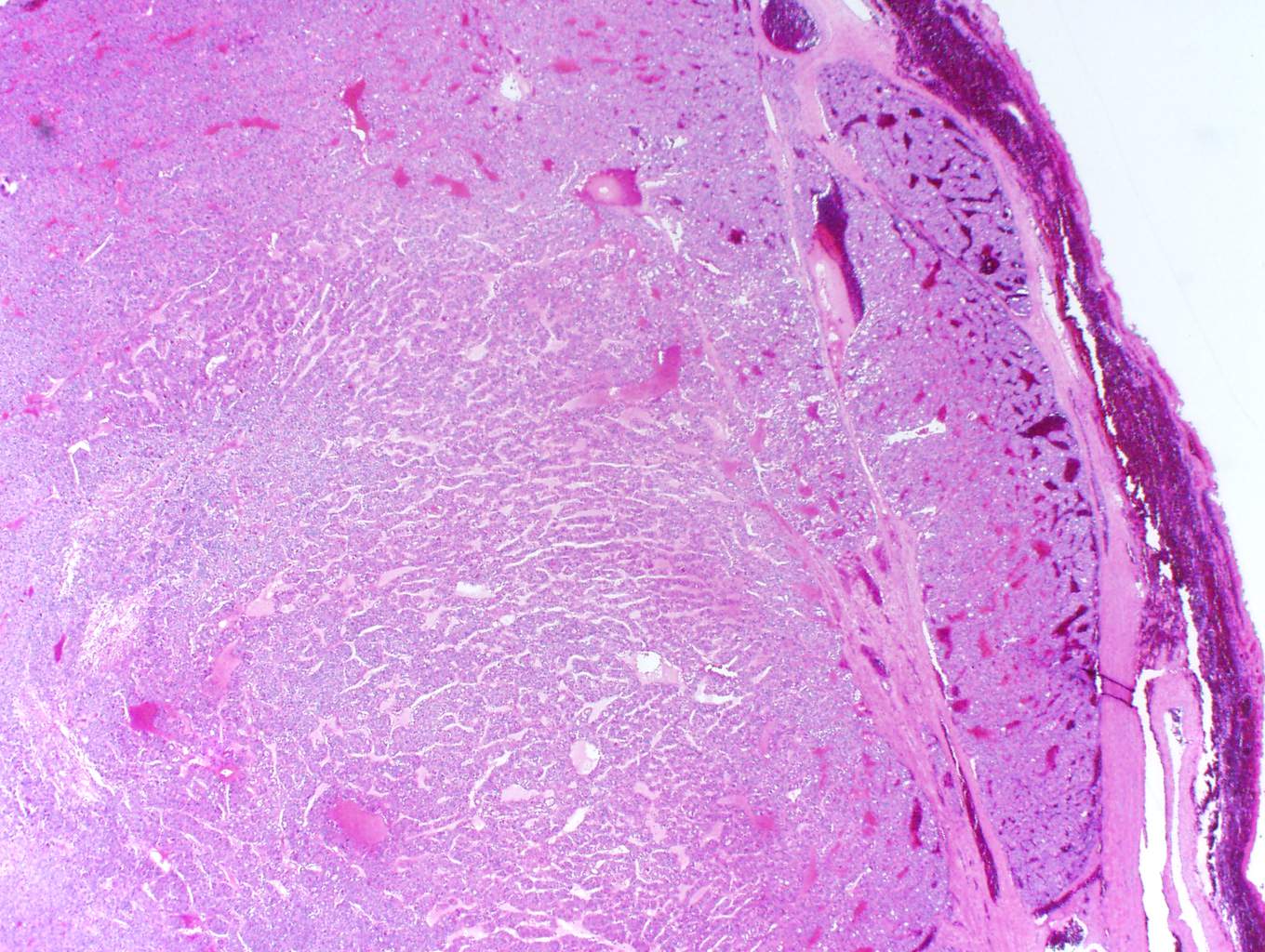
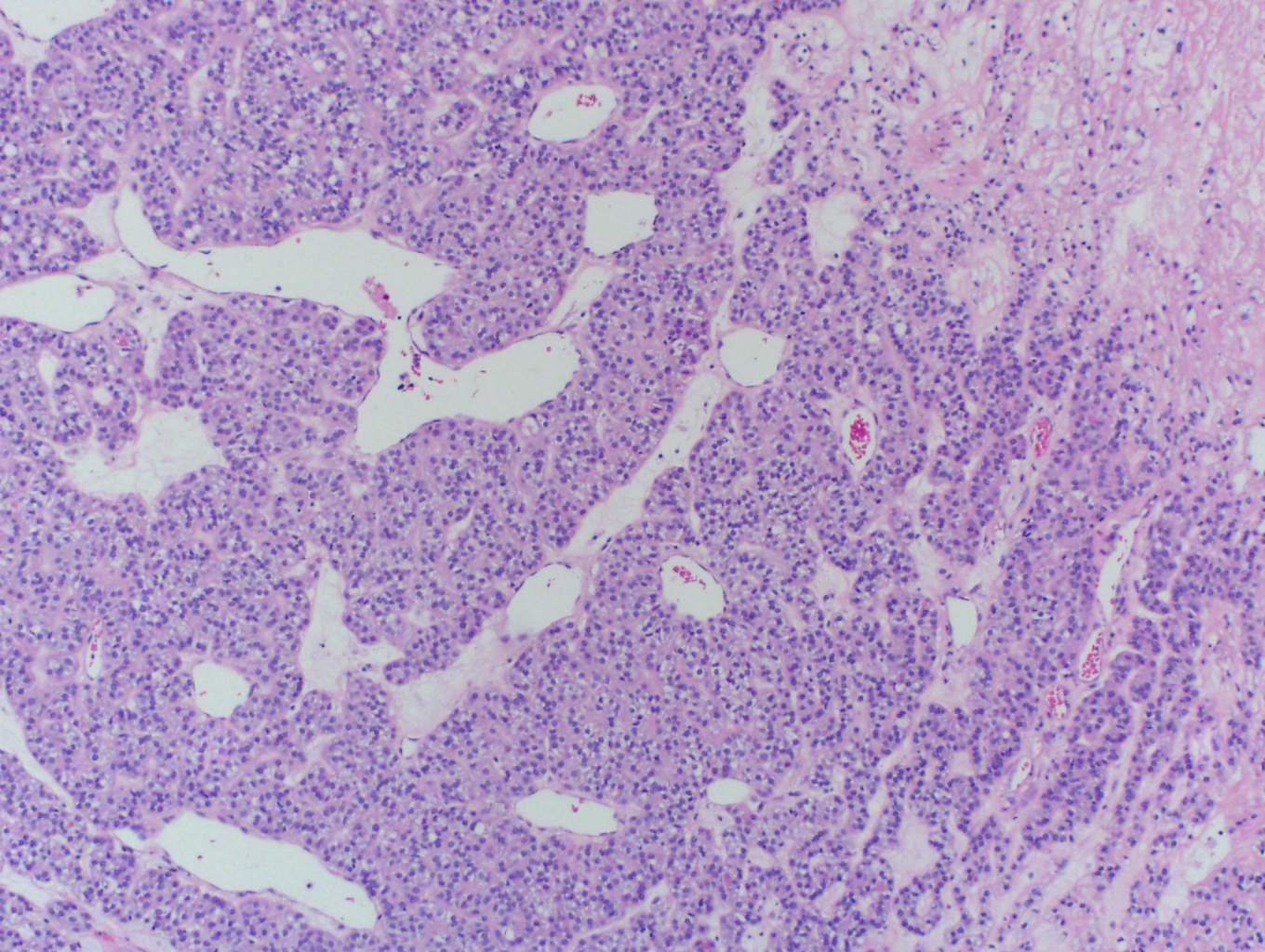
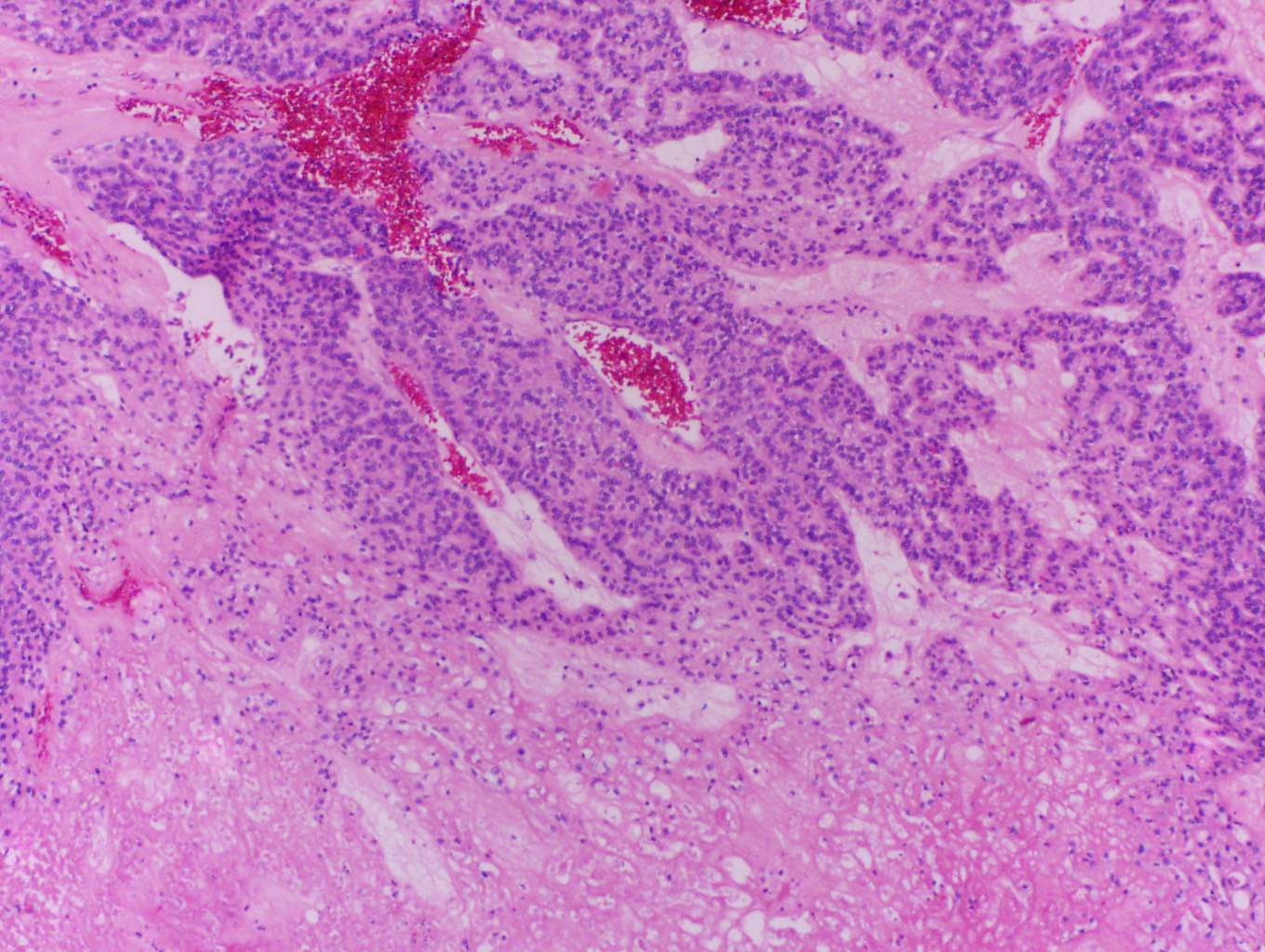
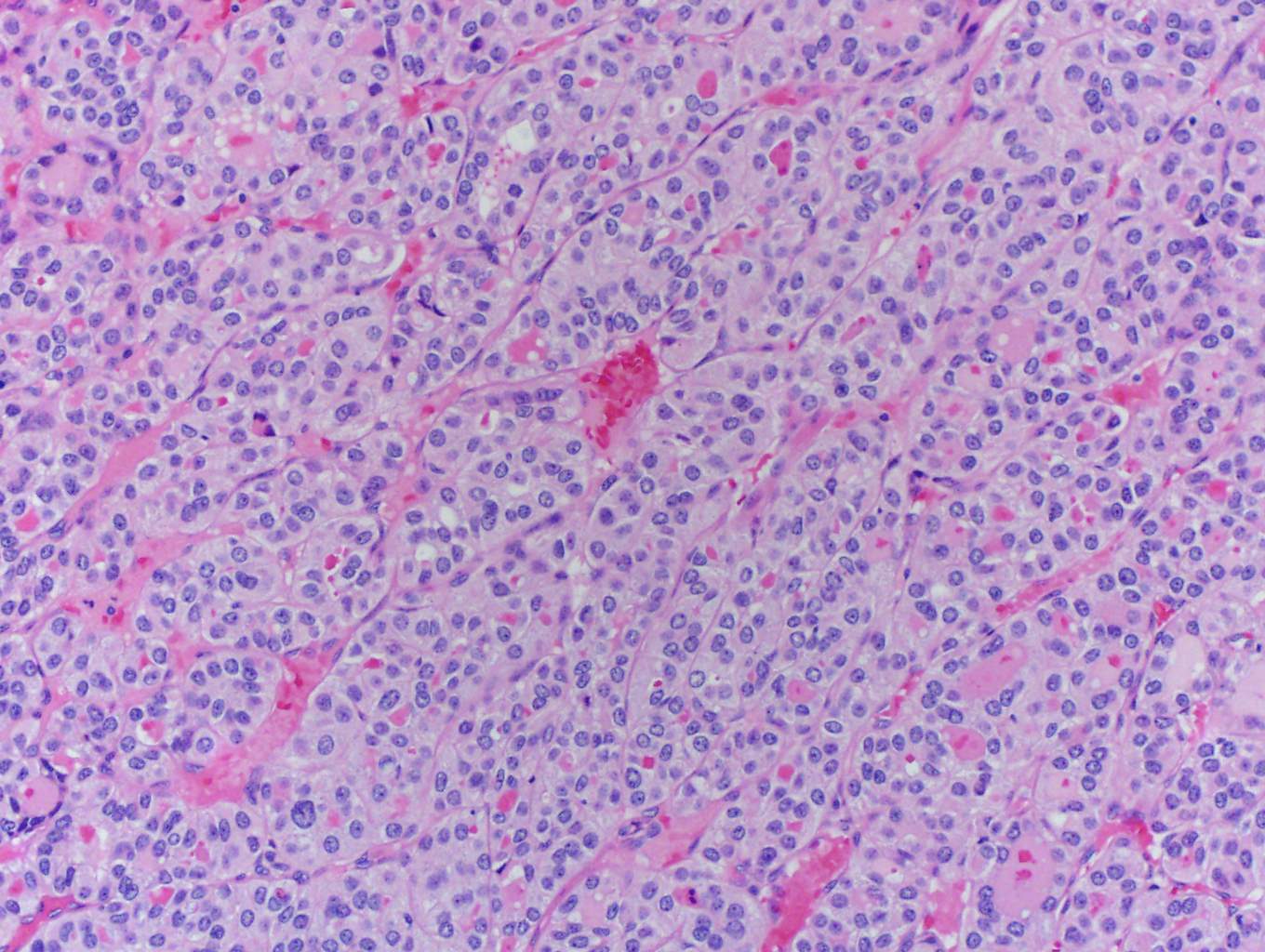
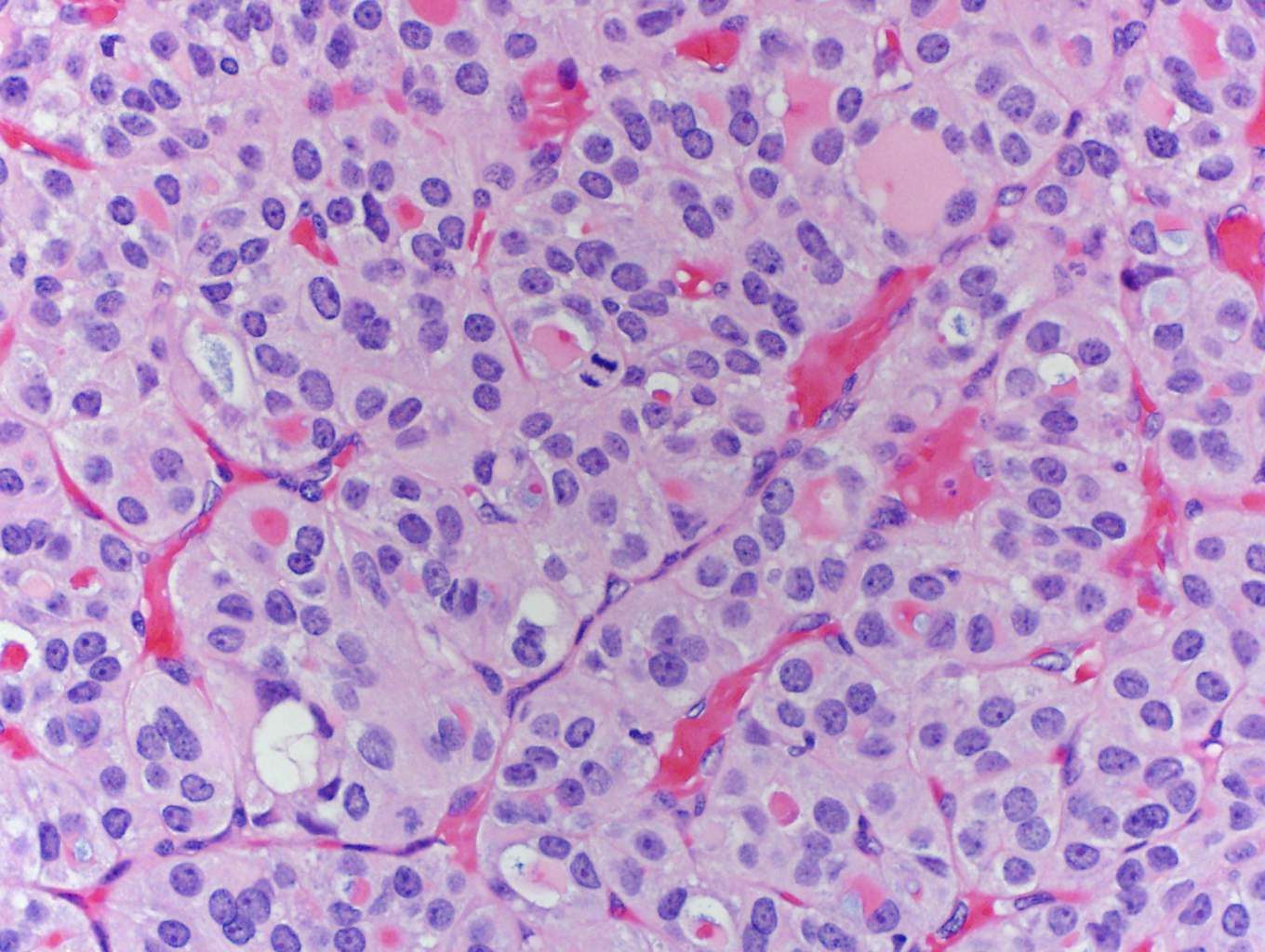
Microscopic (histologic) description
- Turin consensus diagnostic criteria:
- Solid / trabecular / insular growth pattern
- No nuclear features of papillary carcinoma
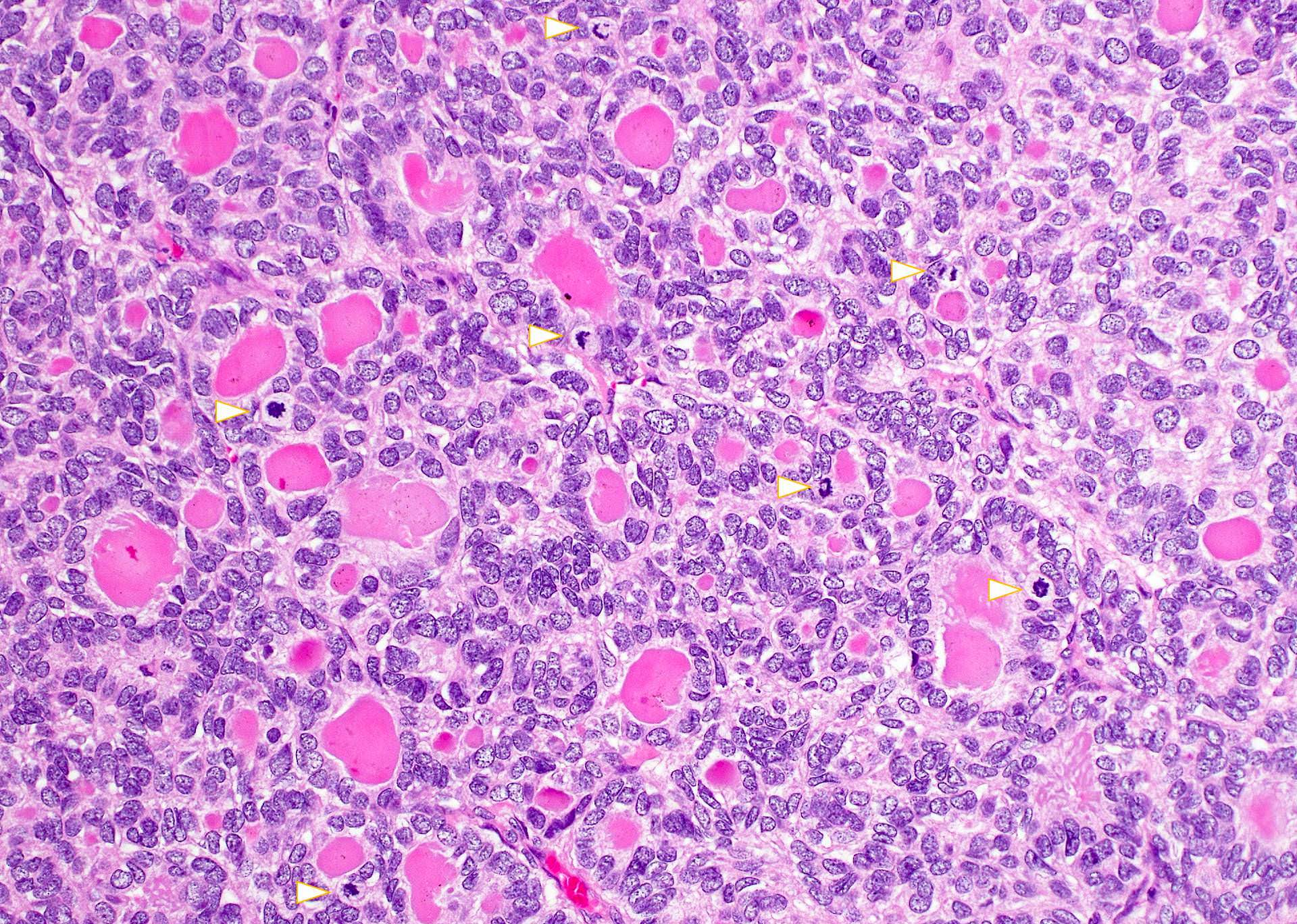
- Presence of at least one of following: convoluted nuclei, ≥ 3 mitotic figures/10 HPF, tumor necrosis (Am J Surg Pathol 2007;31:1256)
- Other:
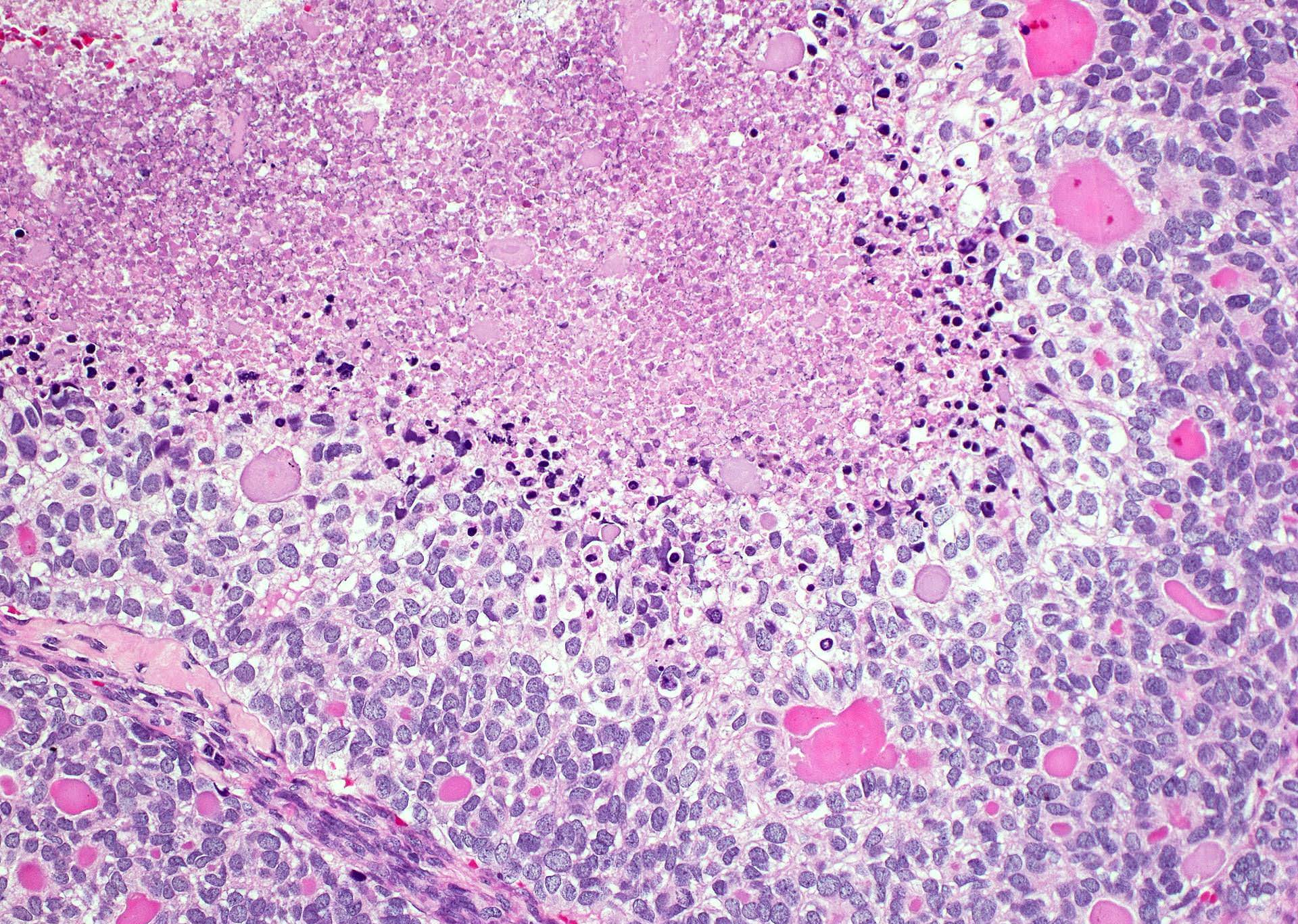
- Prototypical type insular carcinoma: solid nests (may contain microfollicules) composed of small uniform cell with round hyperchromatic nuclei or convoluted nuclei, increased mitotic figures, necrosis (Am J Surg Pathol 1984;8:655)
- Others tumors: solid nests composed of larger more pleomorphic tumor cells; may have oncocytic cells, clear cells, signet ring cells or rhabdoid cells
- Component of well differentiated tumor (papillary or follicular carcinoma) may also be present
- As few as 10% of poorly differentiated carcinomas (in otherwise well differentiated carcinomas) may be associated with unfavorable prognosis (Am J Surg Pathol 2011;35:1866)
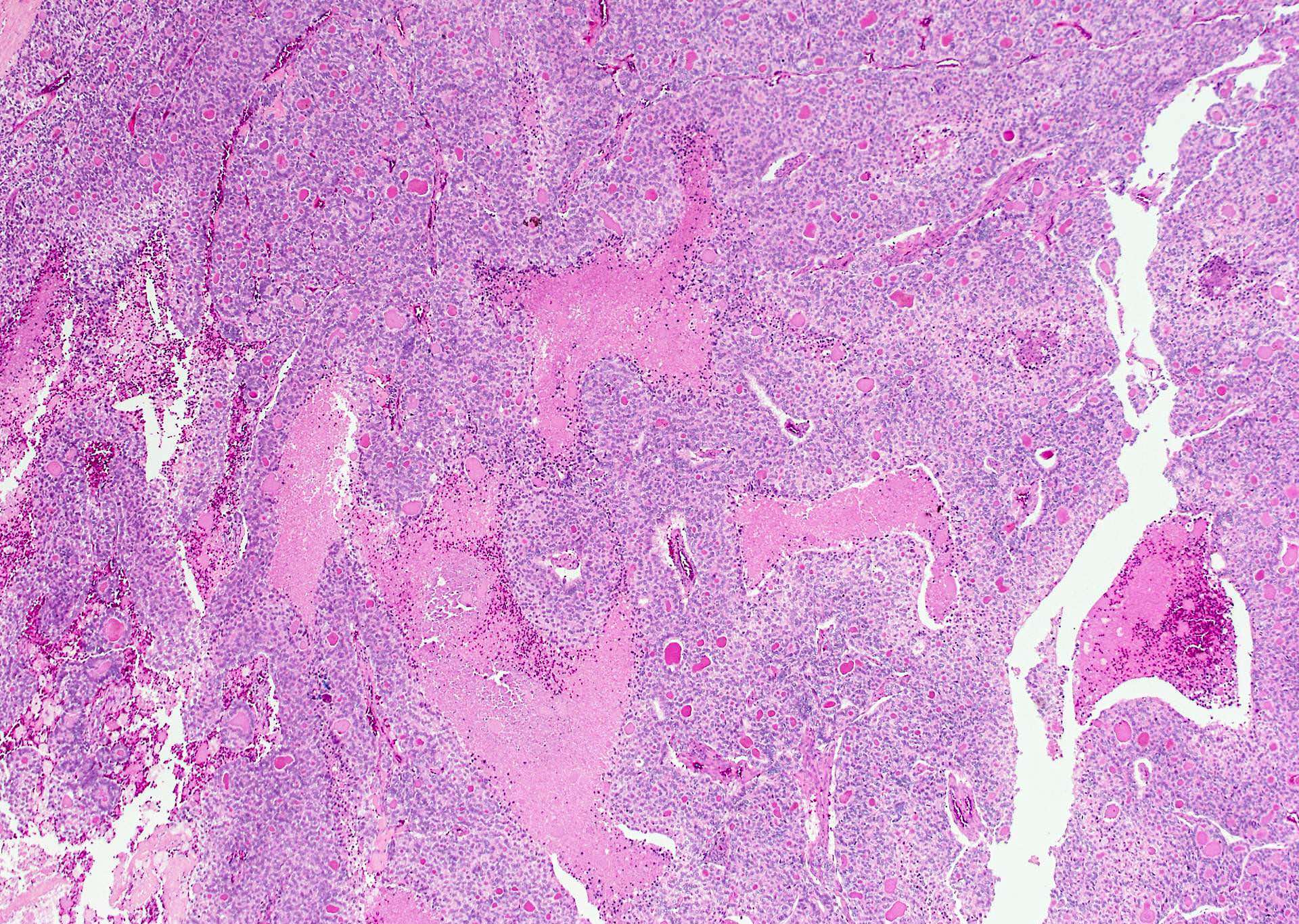
- May have peritheliomatous pattern (tumor cells around blood vessels with necrosis of tumor cells further away from vessels), vascular and capsular invasion (Lloyd: WHO Classification of Tumours of Endocrine Organs, 4th Edition, 2017)
Microscopic (histologic) images
Contributed by Shuanzeng Wei, M.D., Ph.D., Andrey Bychkov, M.D., Ph.D.
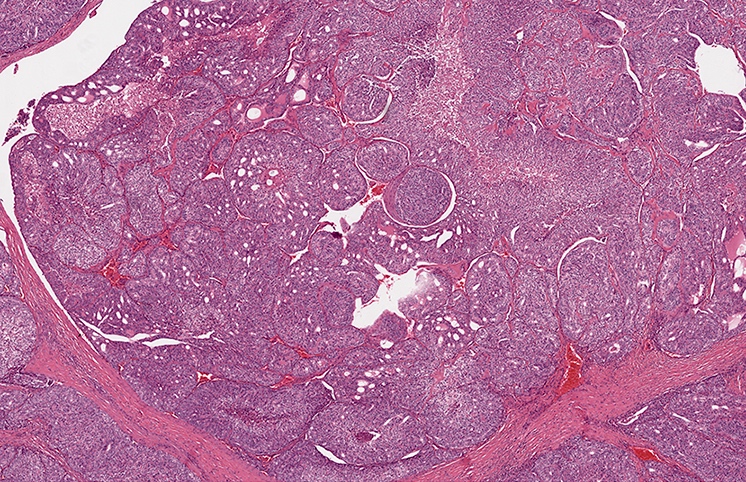
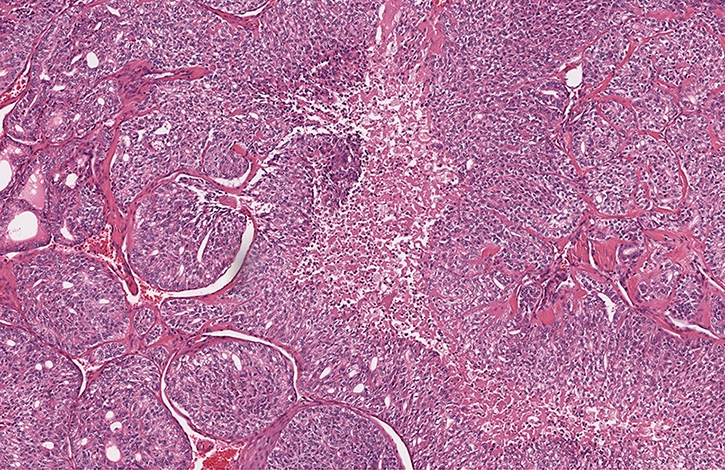
Nests of tumor with necrosis
Follicular carcinoma with high grade progression
Case #435
Various images
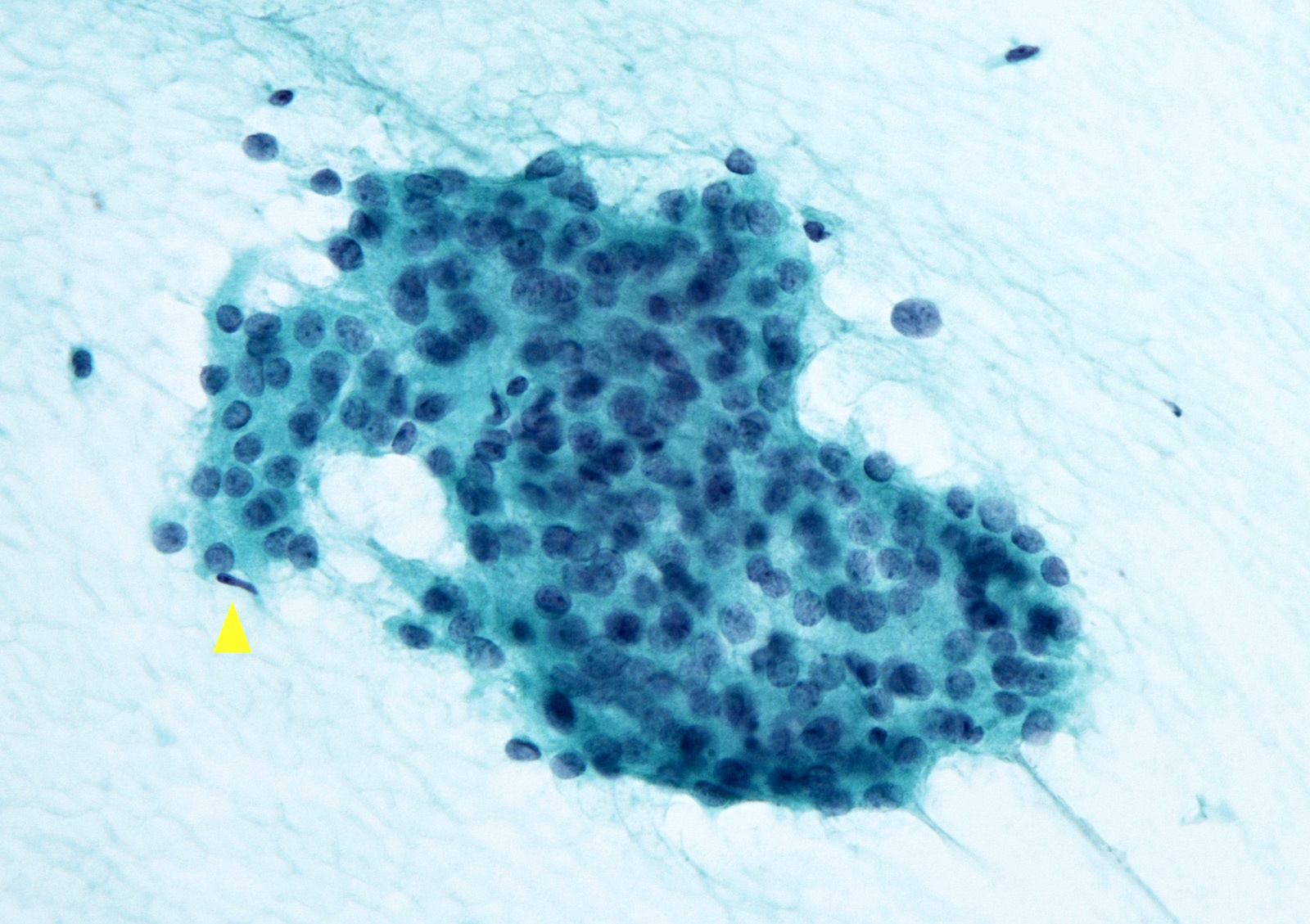
Cytology description
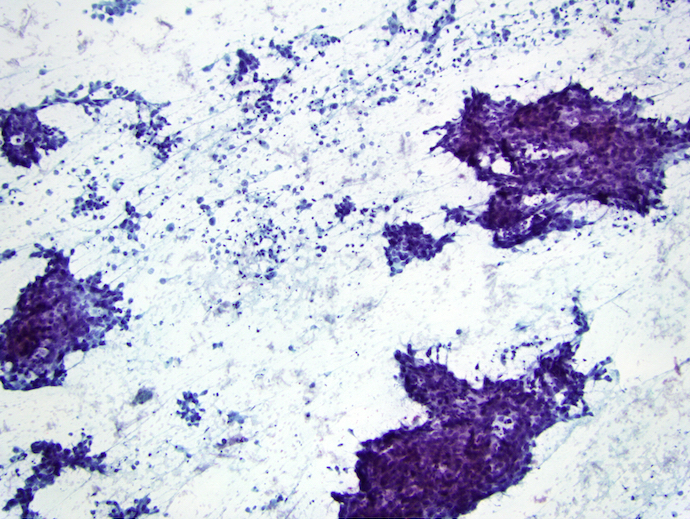
- Highly cellular, crowded cell clusters with solid, trabecular or insular morphology (Cancer 2009;117:185, Cytopathology 2016;27:176)
- Background of single cells with high N:C ratio
- May have necrotic background and increased mitotic figures
Cytology images
Contributed by Ayana Suzuki, C.T. and Shuanzeng Wei, M.D., Ph.D.
Insular pattern
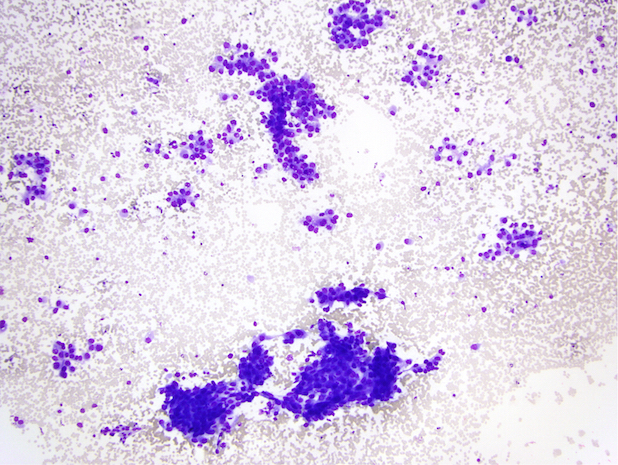
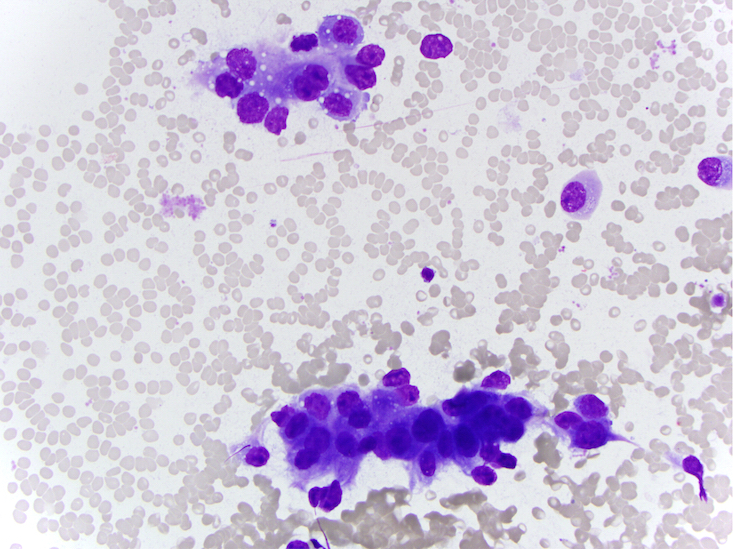
Diff-Quik stain
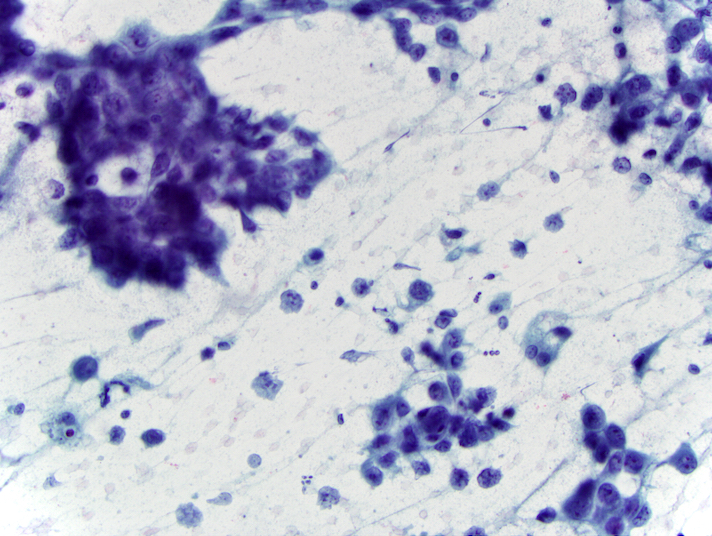
Pap stain
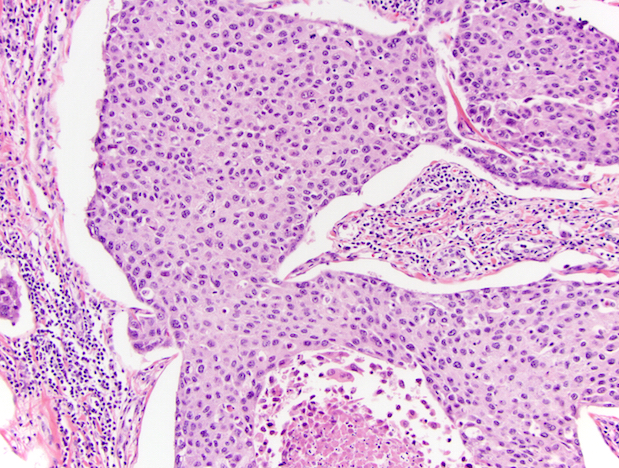
Corresponding histology shows mitosis and necrosis
Images hosted on other servers:

Nesting pattern of cells

Overlapping cells with round, regular nuclei

Large clusters and single cells

Cellular nests of loosely cohesive cells

Overlapping cells with mild atypia

Small microfollicle of tumor cells

Vacuolated cytoplasm with round nuclei
Positive stains
- Keratin, thyroglobulin (decreased expression), TTF1, Ki67: 10 - 30% (Lloyd: WHO Classification of Tumours of Endocrine Organs, 4th Edition, 2017)
Negative stains
Molecular / cytogenetics description
- Alteration of early event of thyroid carcinogenesis: RAS family and BRAF mutation (Surg Pathol Clin 2014;7:475)
- Alteration associated with dedifferentiation: mutation of p53, TERT, CTNNB1 and AKT1 (Lloyd: WHO Classification of Tumours of Endocrine Organs, 4th Edition, 2017)
Videos
Poorly differentiated thyroid carcinoma by M. Brandwein (2020)
Differential diagnosis
- Anaplastic thyroid carcinoma:
- Completely lacks follicular differentiation, prominent nuclear pleomorphism and necrosis
- Generally thyroglobulin- TTF1- (Surg Pathol Clin 2014;7:475)
- Hürthle cell tumors:
- Poorly differentiated thyroid carcinoma can be predominantly composed of oncocytic cells (often with a small cell component) but also has necrosis and ≥ 3 mitoses/10 HPF
- Metastatic carcinoma to thyroid:
- Pertinent tumor history
- Medullary thyroid carcinoma:
- Also has nesting pattern
- In addition, has prominent vasculature, granular cytoplasm and finely stippled chromatin, calcitonin+ thyroglobulin- with amyloid
- Parathyroid carcinoma:
- PTH+
- Solid variant papillary thyroid carcinoma:
- Typical papillary nuclear features throughout
Additional references
Practice question #1
Which of the following features are not required for the diagnosis of poorly differentiated thyroid carcinoma?
- Absence of conventional nuclear features of papillary thyroid carcinoma
- Necrosis / convoluted nuclei / increased mitotic activity
- Solid, trabecular or insular growth
- Vascular invasion
Practice answer #1
D. Vascular invasion. The Turin criteria specify solid / trabecular / insular growth, lack of conventional nuclear
features of papillary thyroid carcinoma and one of the following: necrosis, convoluted
nuclei or increased mitotic activity (3 or more mitoses/10 HPF). Vascular invasion
may be seen in a variety of thyroid carcinomas and is an adverse prognostic factor
regardless of histologic subtype or grade.
Comment Here
Reference: Poorly differentiated thyroid carcinoma
Comment Here
Reference: Poorly differentiated thyroid carcinoma
