Ovary
Tumor-like lesions
Corpus luteum cyst
Editorial Board Member: Gulisa Turashvili, M.D., Ph.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.


Last author update: 17 June 2021
Last staff update: 20 May 2025
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Corpus luteum cyst
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Busca A, Parra-Herran C. Corpus luteum cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/ovarynontumorcorpuslutcyst.html. Accessed September 24th, 2025.
Definition / general
- Ovarian cyst > 3 cm in diameter, lined by luteinized granulosa and theca cells
Essential features
- Cyst over 3 cm in size
- Cyst lining composed of inner layer of luteinized granulosa cells and outer layer of theca cells
ICD coding
- ICD-11: GA18.1 - corpus luteum cyst
Epidemiology
- Functional cysts in women of reproductive age, including pregnancy
- Rare in postmenopausal women
Sites
- Ovary
Pathophysiology
- Corpus luteum is a physiological postovulatory structure formed after the dominant follicle releases the ovum
- Its main purpose is to secrete estrogen and progesterone and it normally regresses at the end of the cycle
- Cystic dilation happens when corpus luteum fails to regress and becomes enlarged with fluid / blood
- Reference: StatPearls: Anatomy, Abdomen and Pelvis, Ovary Corpus Luteum [Accessed 20 May 2021]
Clinical features
- Patients can be asymptomatic or present with menstrual irregularities, amenorrhea, abdominal pain, palpable abdominal mass if large size
- If cyst ruptures, patient may present with acute abdomen and hemoperitoneum
- Reference: Turk J Obstet Gynecol 2020;17:300
Diagnosis
- On pelvic ultrasound, appears as simple ovarian cyst, often hemorrhagic; incidental finding or diagnosed during symptomatic workup
Laboratory
- No specific laboratory findings
Radiology description
- On ultrasound: unilocular cyst with prominent peripheral blood flow and thick crenulated vascular walls
- On CT: unilocular structure with crenulated walls and brisk enhancement (Abdom Radiol (NY) 2016;41:2270)
Radiology images
Images hosted on other servers:

CT: ruptured corpus luteum cyst and hemoperitoneum
Prognostic factors
- Most cysts resolve spontaneously
- Hemorrhagic cysts over 5 cm or simple cysts between 5 and 7 cm in women of reproductive age require follow up to ensure resolution (Ultrasound Q 2010;26:121)
- In postmenopausal women, consider surgical evaluation of hemorrhagic cysts, as the etiology is more likely neoplastic than functional (Radiology 2010;256:943)
- Vast majority of pregnancy associated simple cysts < 5 cm resolve by weeks 16 - 20 and require no intervention (Clin Obstet Gynecol 2006;49:492)
Case reports
- 15 year old girl with ruptured hemorrhagic corpus luteum cyst of undescended ovary, a rare cause of acute abdomen in an adolescent (J Pediatr Adolesc Gynecol 2016;29:e21)
- 15 year old girl with ruptured corpus luteum cyst of pregnancy with massive hemoperitoneum (J Pediatr Adolesc Gynecol 2007;20:97)
- 16 year old girl with hemoperitoneum from corpus luteum cyst rupture (Case Rep Emerg Med 2014;2014:252657)
- 18 year old woman with congenital hypofibrinogenemia with hemoperitoneum caused by ovulation (Obstet Gynecol Sci 2015;58:427)
Treatment
- Resection if symptomatic, rupture or suspicion for neoplastic process (Radiology 2010;256:943)
- For asymptomatic unilocular cysts with normal CA125, optimal management includes surveillance with ultrasound (Clin Obstet Gynecol 2006;49:506, Clin Exp Obstet Gynecol 2014;41:609)
Clinical images
Images hosted on other servers:

Intraoperative: hemorrhage of corpus luteum cyst
Gross description
- Single unilocular cyst with smooth surface
- Cyst wall and lining appears yellow and convoluted
- Serous or hemorrhagic contents
- Reference: Kurman: Blaustein's Pathology of the Female Genital Tract, 7th Edition, 2019
Gross images
Images hosted on other servers:

Corpus luteum cyst
Frozen section description
- Convoluted cyst wall lined by cells with abundant eosinophilic cytoplasm and bland nuclear features
- Cytoplasm may appear vacuolated on frozen tissue
Microscopic (histologic) description
- Cyst lining is convoluted, composed of an inner layer of luteinized granulosa cells and outer layer of theca cells
- Granulosa cells are polygonal in shape, with abundant eosinophilic cytoplasm and central round nuclei
- Mitotic figures may be seen in the granulosa cells
- Outer theca cells are smaller in size
- Prominent inner layer of fibrous tissue
- Reference: Kurman: Blaustein's Pathology of the Female Genital Tract, 7th Edition, 2019
Microscopic (histologic) images
Contributed by Aurelia Busca, M.D., Ph.D.
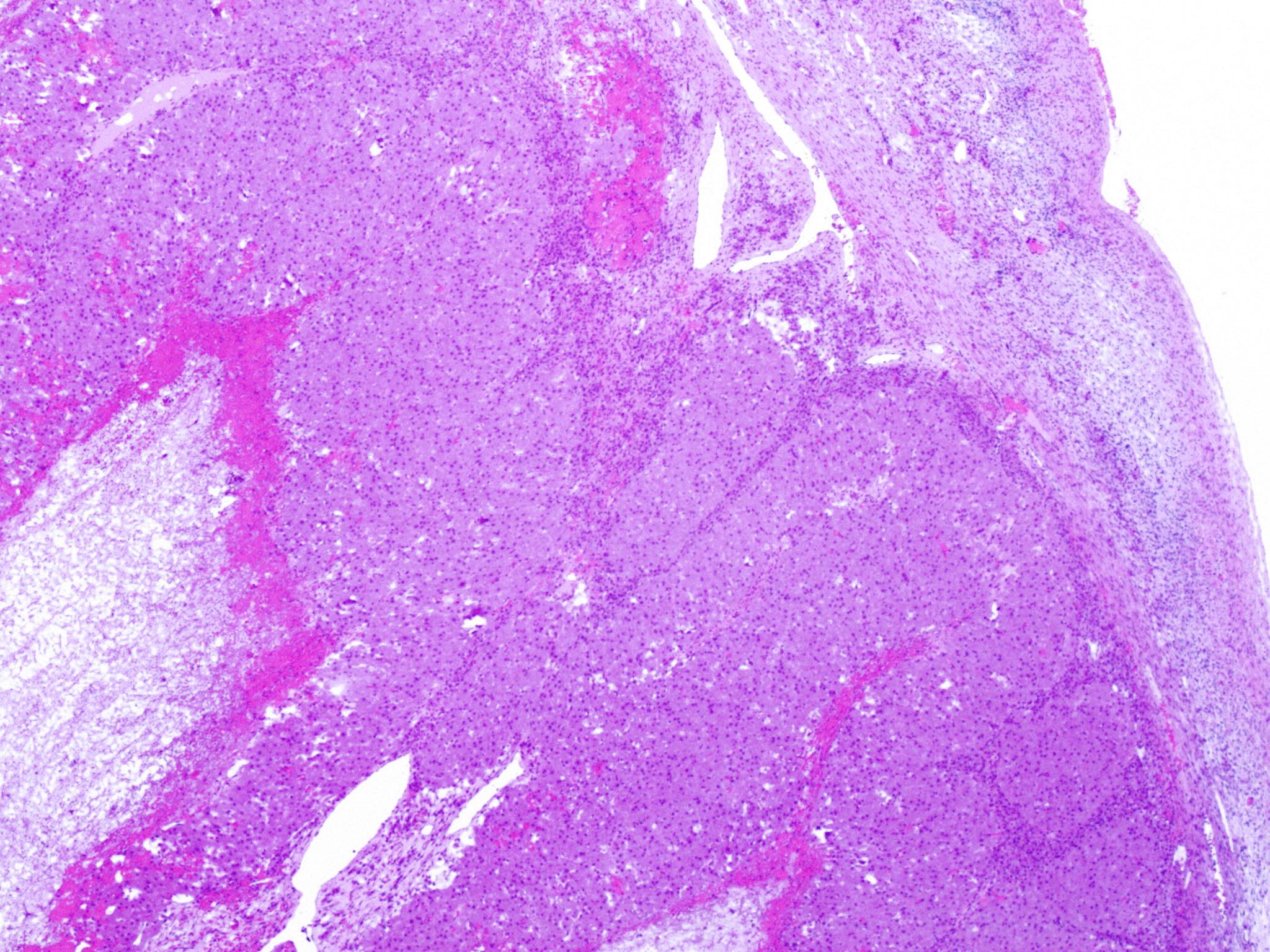
Convoluted cyst lining
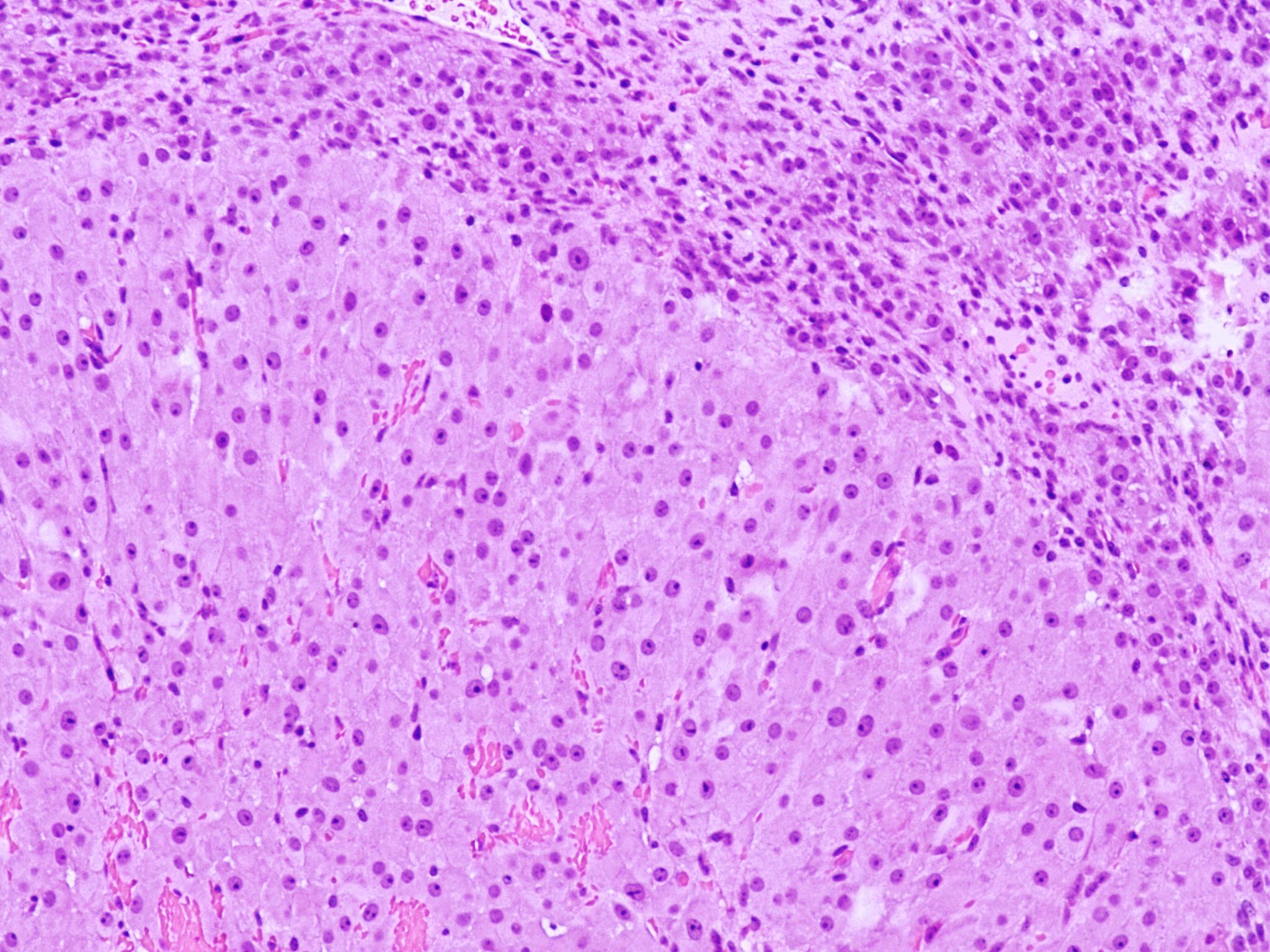
Bilayered cyst lining
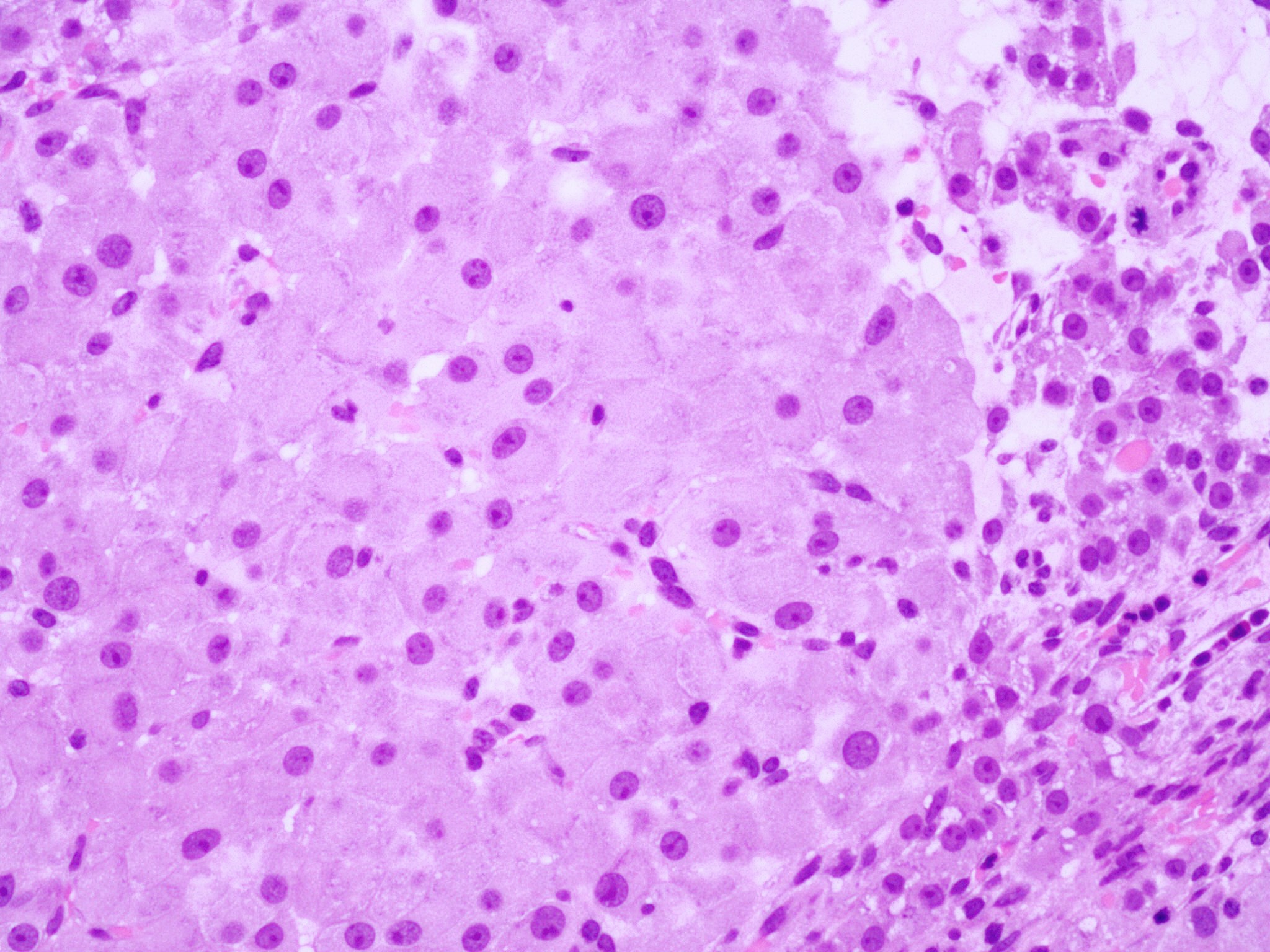
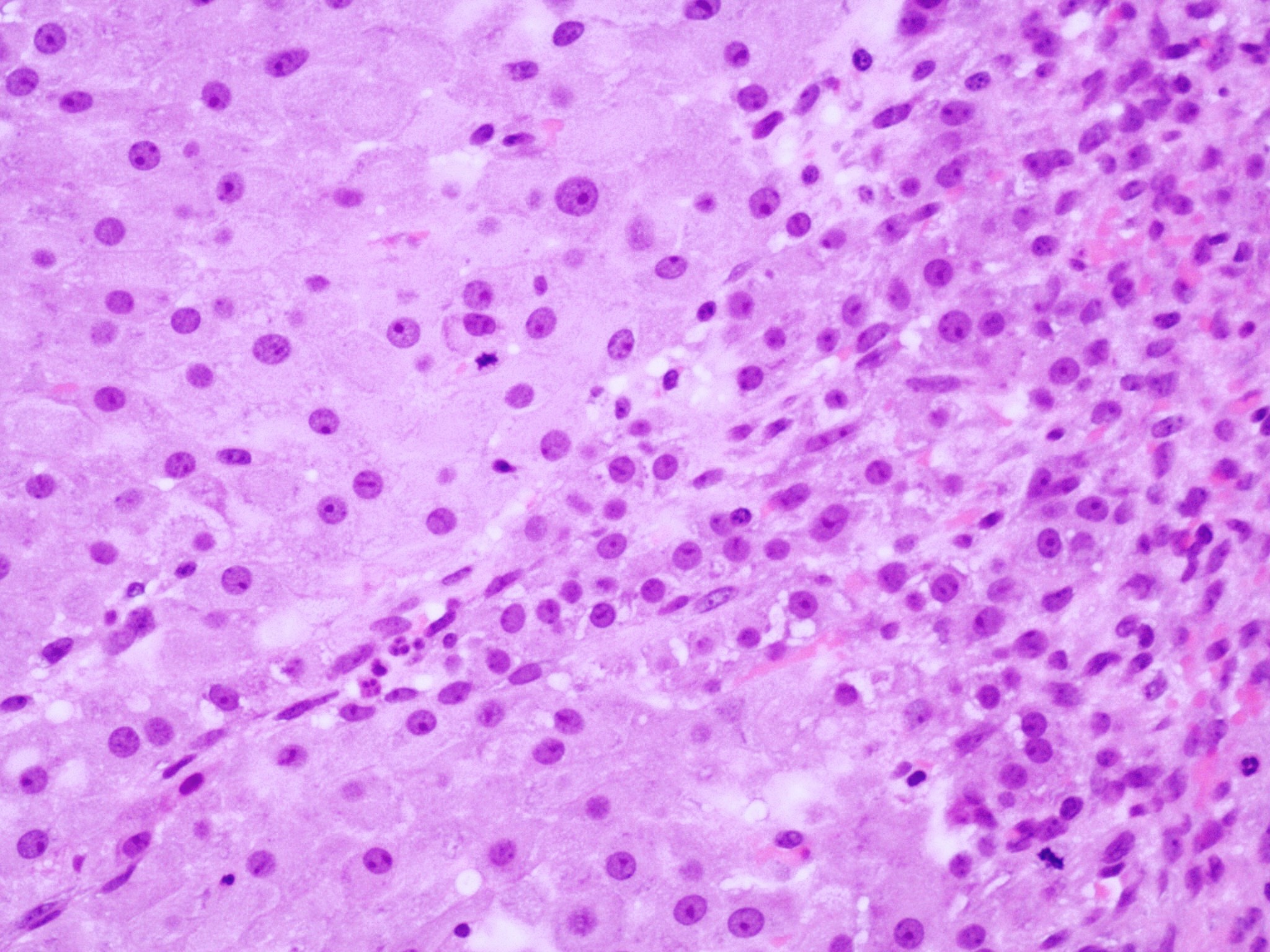
Granulosa and theca cells
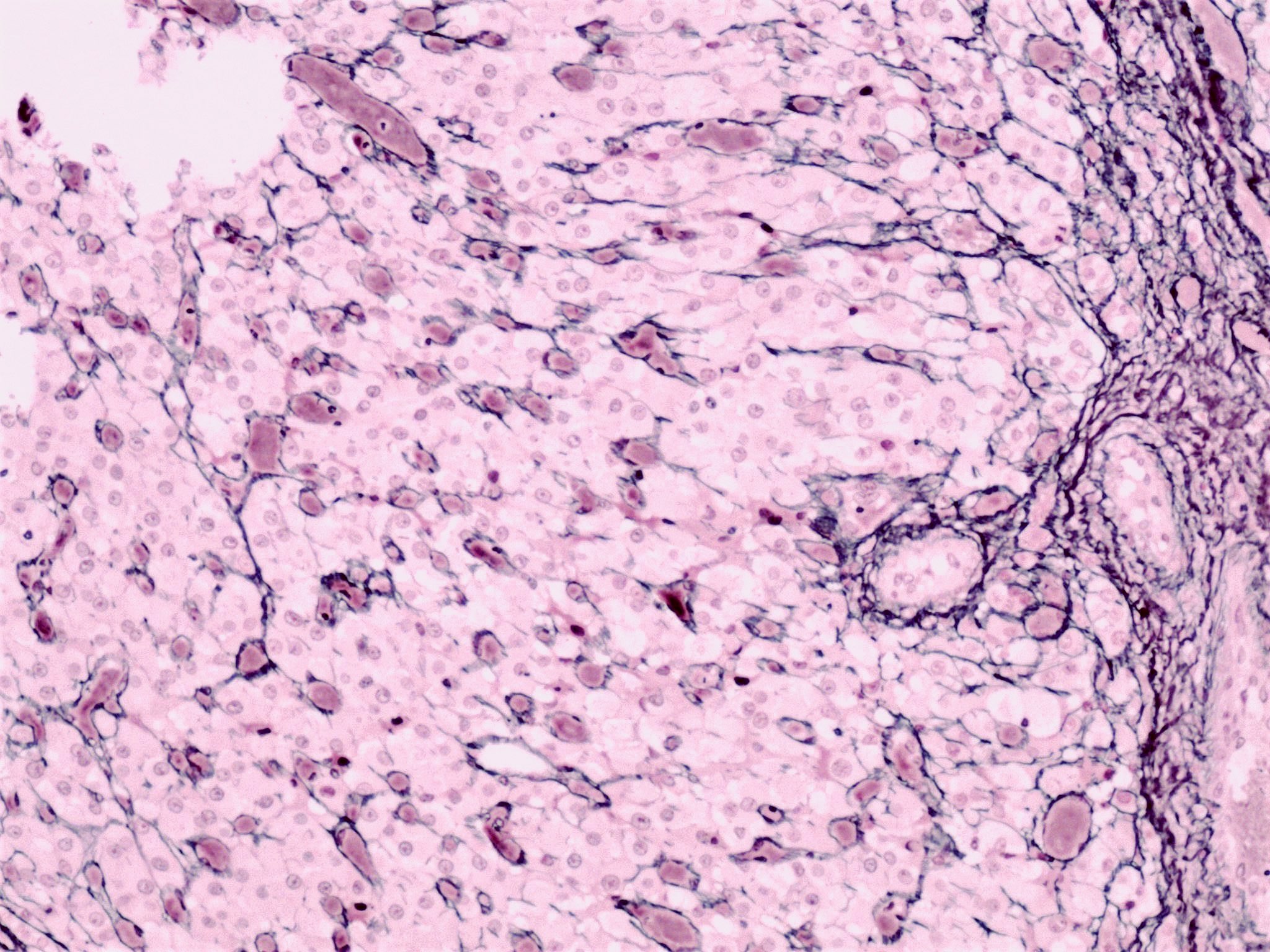
Reticulin stain
Cytology description
- Rarely performed
- Luteinized granulosa cells and hemosiderin laden macrophages in the background of blood and fibrin (Diagn Cytopathol 1990;6:77)
Positive stains
- Usually not necessary for diagnosis
- Calretinin (Histopathology 2001;38:403)
- Inhibin (J Clin Endocrinol Metab 1991;73:470)
- Progesterone receptor (Reproduction 2004;128:423)
- Reticulin preserved within the theca interna layer
Negative stains
- Cytokeratin
- Reticulin diminished / absent in the granulosa layer
Sample pathology report
- Ovary, right, cystectomy:
- Corpus luteum cyst
- Background ovary with cystic follicles and epithelial inclusion cysts
- Negative for malignancy
Differential diagnosis
- Cystic granulosa cell tumor:
- Usually larger
- The 2 cell types in the cyst wall have a more disorderly pattern
- Neoplastic cells can infiltrate the cyst wall
- With or without Call-Exner bodies
- Endometriotic cyst:
- Endometrial glands and stroma, hemosiderin laden macrophages
- Epithelial inclusion cyst:
- Lined by either ciliated (tubal type) or flat (ovarian surface / peritoneal type) epithelium
- Follicular cyst:
- > 3 cm: lined by an inner layer of granulosa cells and an outer layer of theca cells
- Luteinization is either absent or only focal
- Lacks the convoluted appearance on low power magnification
- Cystic corpus luteum:
- Size < 3 cm
Practice question #1
Which of the following is true about the 4 cm ovarian cyst shown in the image above?
- Affects predominantly postmenopausal women
- It is a benign finding, expected to undergo regression
- It is a precursor lesion for granulosa cell tumor
- It is lined by a single layer of granulosa cells
Practice answer #1
B. It is a benign finding, expected to undergo regression
Comment Here
Reference: Corpus luteum cyst
Comment Here
Reference: Corpus luteum cyst
Practice question #2
Which of the following is characteristic of a corpus luteum cyst of the ovary?
- Bilayered lining of granulosa and theca cells
- Presence of endometrial type stroma
- Single layer of ciliated cells with eosinophilic cytoplasm
- Single layer of granulosa cells
Practice answer #2
