Prostate gland & seminal vesicles
IHC overview
Deputy Editors-in-Chief: Bonnie Choy, M.D., Maria Tretiakova, M.D., Ph.D.

Last author update: 14 April 2025
Last staff update: 14 April 2025
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Prostate immunohistochemistry
Table of Contents
Definition / general | Essential features | Terminology | Pathophysiology | Uses by pathologists | Microscopic (histologic) description | Microscopic (histologic) images | Positive staining - normal | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2 | Practice question #3 | Practice answer #3 | Practice question #4 | Practice answer #4Cite this page: Ahmed S, Ma B, Xiao GQ. IHC overview. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/prostateihc.html. Accessed August 19th, 2025.
Definition / general
- Diagnostic biomarker study of prostate tissue is one of the most common applications of immunohistochemistry in surgical pathology, especially for prostate needle biopsies (Mod Pathol 2018;31:S12)
- In an appropriate histomorphologic setting, immunohistochemistry is very helpful in distinguishing between prostatic adenocarcinoma and its benign mimickers (Adv Anat Pathol 2018;25:387)
Essential features
- Most used immunohistochemical stains include basal cell markers and prostate specific markers (Mod Pathol 2018;31:S12)
- Hallmark of prostatic adenocarcinoma is the loss of basal cells; however, not all prostate glands without basal cells are carcinoma (Mod Pathol 2018;31:S12)
- Very rarely, prostatic adenocarcinoma is positive for basal cell marker (p63 or 34 beta E12) (Prostate 2023;83:462, Am J Surg Pathol 2008;32:461)
- During embryonic development, the prostate originates from the urogenital sinus (negative for PAX8) and seminal vesicles originate from the Wolffian / mesonephric duct (positive for PAX8)
Terminology
- Triple antibody cocktail (also called PIN4 or PIN cocktail): mixture of p63, 34 beta E12 and AMACR / P504S
Pathophysiology
- Survival and growth of normal and prostate cancer cells rely on the constitutive expression of androgen receptor (AR) and its signaling (Front Oncol 2019;9:858)
- Prostate cancer is often associated with increased fatty acid metabolites due to overexpression of AMACR (J Cancer Res Ther 2017;13:21)
- Overexpression of ERG from TMPRSS2::ERG gene rearrangement plays an important role in the initiation of almost half of prostate cancers (Oncogene 2016;35:403)
Uses by pathologists
- Diagnosis of primary invasive prostatic adenocarcinoma, mainly in the following settings
- Small focus of atypical glands / atypical small acinar proliferation (ASAP)
- Atypical hyperplastic appearing glands
- Postradiation prostatic adenocarcinoma with treatment effect
- Differentiation of invasive cribriform carcinoma from intraductal carcinoma / atypical intraductal proliferation / atypical cribriform lesion
- Confirming prostatic origin of disseminated / metastatic carcinoma (Arch Pathol Lab Med 2020;144:290, Mod Pathol 2018;31:S12)
- Markers for primary prostatic neoplasia (Arch Pathol Lab Med 2020;144:290, Mod Pathol 2018;31:S12, Adv Anat Pathol 2018;25:387, Am J Clin Pathol 2020;153:407)
- Triple antibody cocktail (PIN cocktail): most widely used
- ERG: highly specific (in the setting of absent basal cells) but not sensitive for prostatic adenocarcinoma
- Acinar prostatic adenocarcinoma
- Positive staining
- AMACR / P504S (often, ~80%)
- Negative staining
- p63, 34 beta E12 (no basal cells)
- Rare prostatic adenocarcinoma expressing p63 (usually low grade group) or 34 beta E12 (usually high grade group)
- p63, 34 beta E12 (no basal cells)
- Positive staining
- Ductal adenocarcinoma
- Positive staining
- AMACR / P504S (often, ~80%)
- Negative staining
- p63, 34 beta E12 (no basal cells)
- Can occasionally be p63 and 34 beta E12 positive (focal / sparse basal cells, likely represent residual benign ductal epithelium)
- Positive staining
- Intraductal carcinoma / atypical intraductal proliferation / atypical cribriform lesion / carcinoma in situ
- Positive staining
- AMACR / P504S (often, ~80%)
- p63, 34 beta E12 (continuous or discontinuous layer of basal cells)
- Positive staining
- Markers for prostatic origin of disseminated / metastatic carcinoma
- Positive staining
- NKX3.1: highly sensitive and specific
- AR: highly sensitive but much less specific than NKX3.1
- ERG, PSA: highly specific, moderately sensitive
- PSMA, prostein: moderately specific and sensitive
- Others
- CK7, CK20
- Negative in low grade prostatic carcinoma
- Negative or focally positive in high grade prostatic carcinoma
- CDX2 can be positive
- CK7, CK20
- Negative staining
- PAX8, PAX2, TTF1, GATA3, 34 beta E12, p63 and p40 (with rare exceptions)
- Positive staining
Microscopic (histologic) description
- Nuclear markers: AR (androgen receptor), NKX3.1, p63, ERG
- Cytoplasmic markers: AMACR / P504S (alpha methylacyl CoA racemase), PSA, prostein / P501S
- Cytoplasmic and membrane markers: 34 beta E12 (also called cytokeratin 903), PSMA (prostate specific membrane antigen)
- References: Am J Surg Pathol 2007;31:889, Prostate 2023;83:462, Am J Surg Pathol 2008;32:461
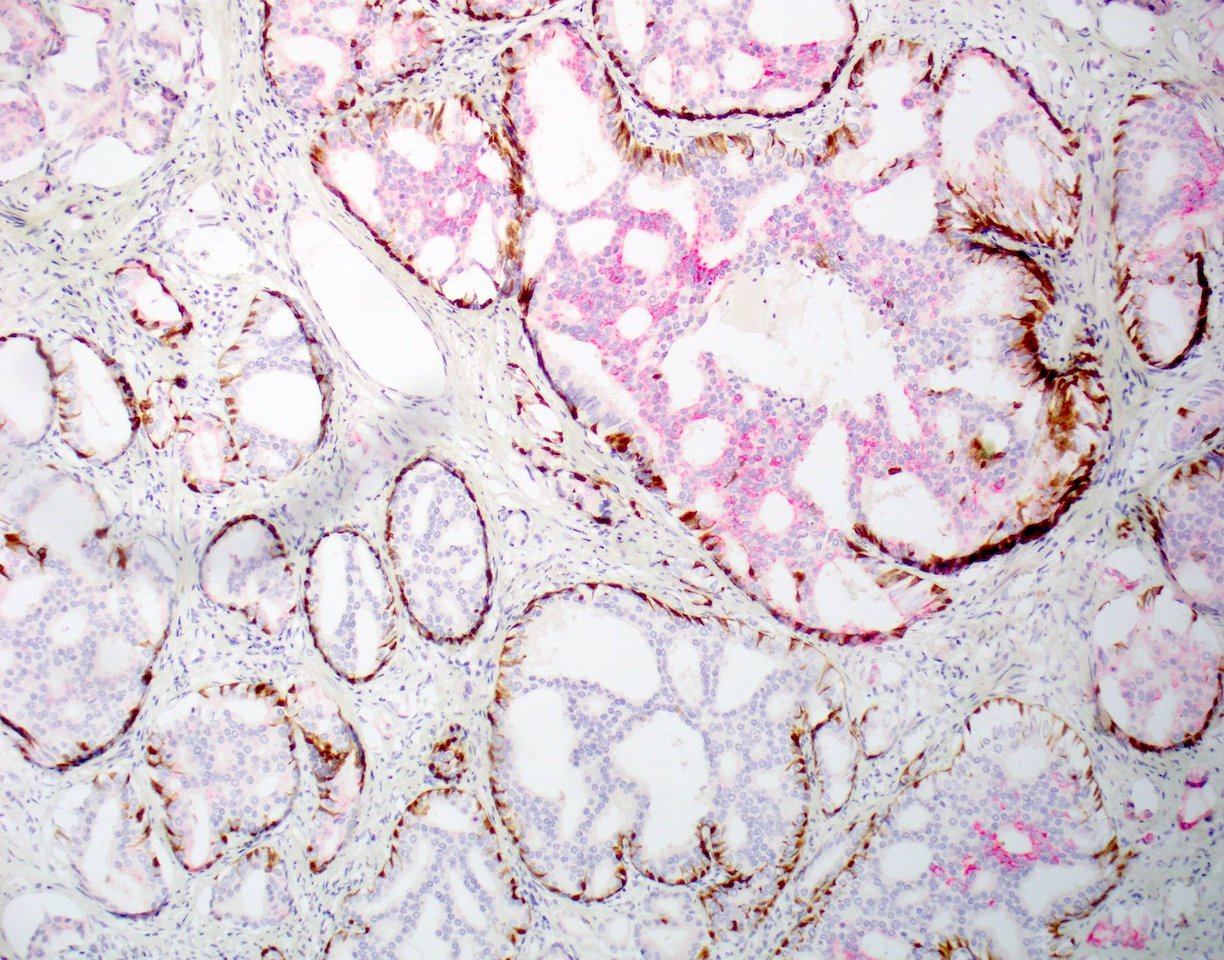
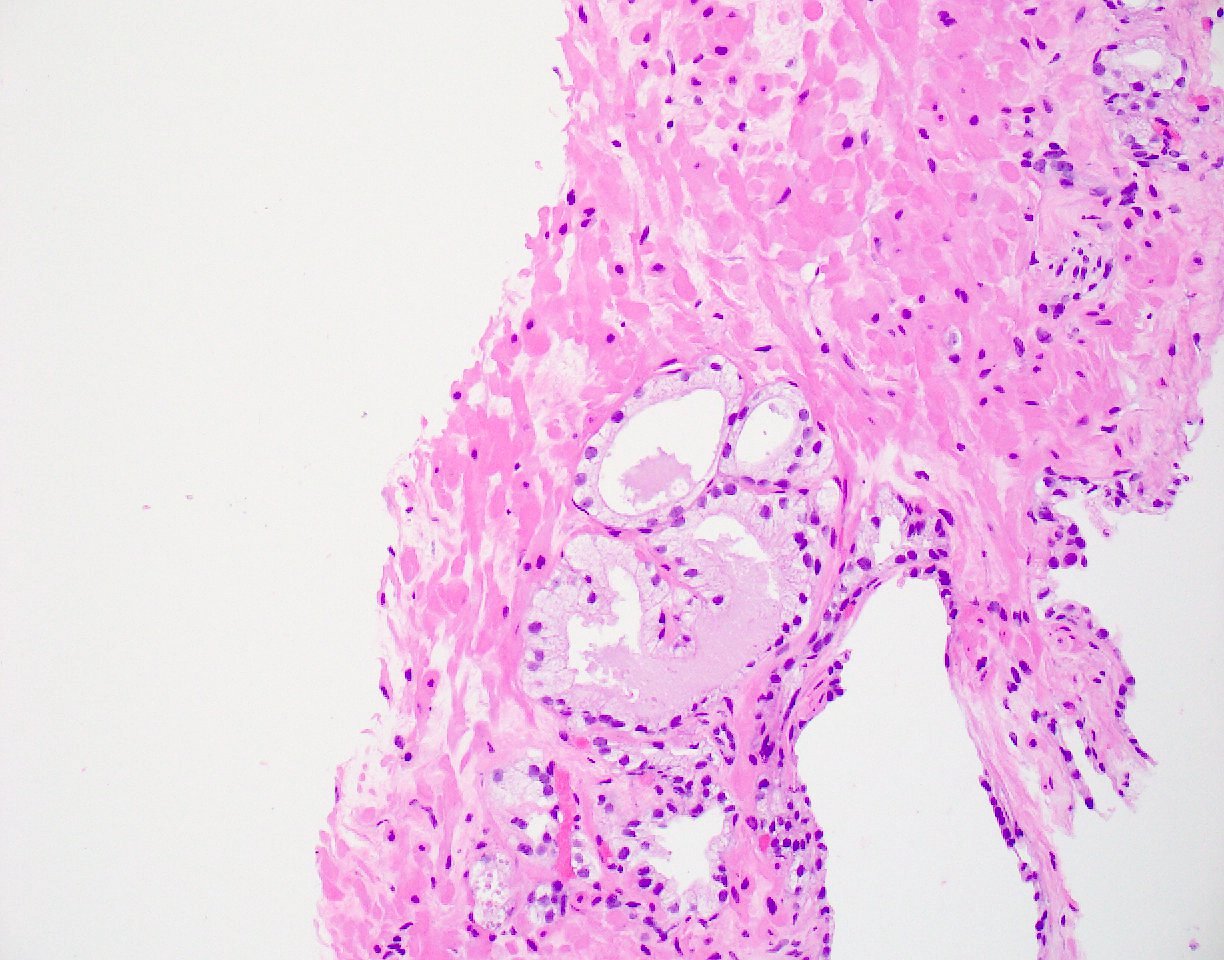
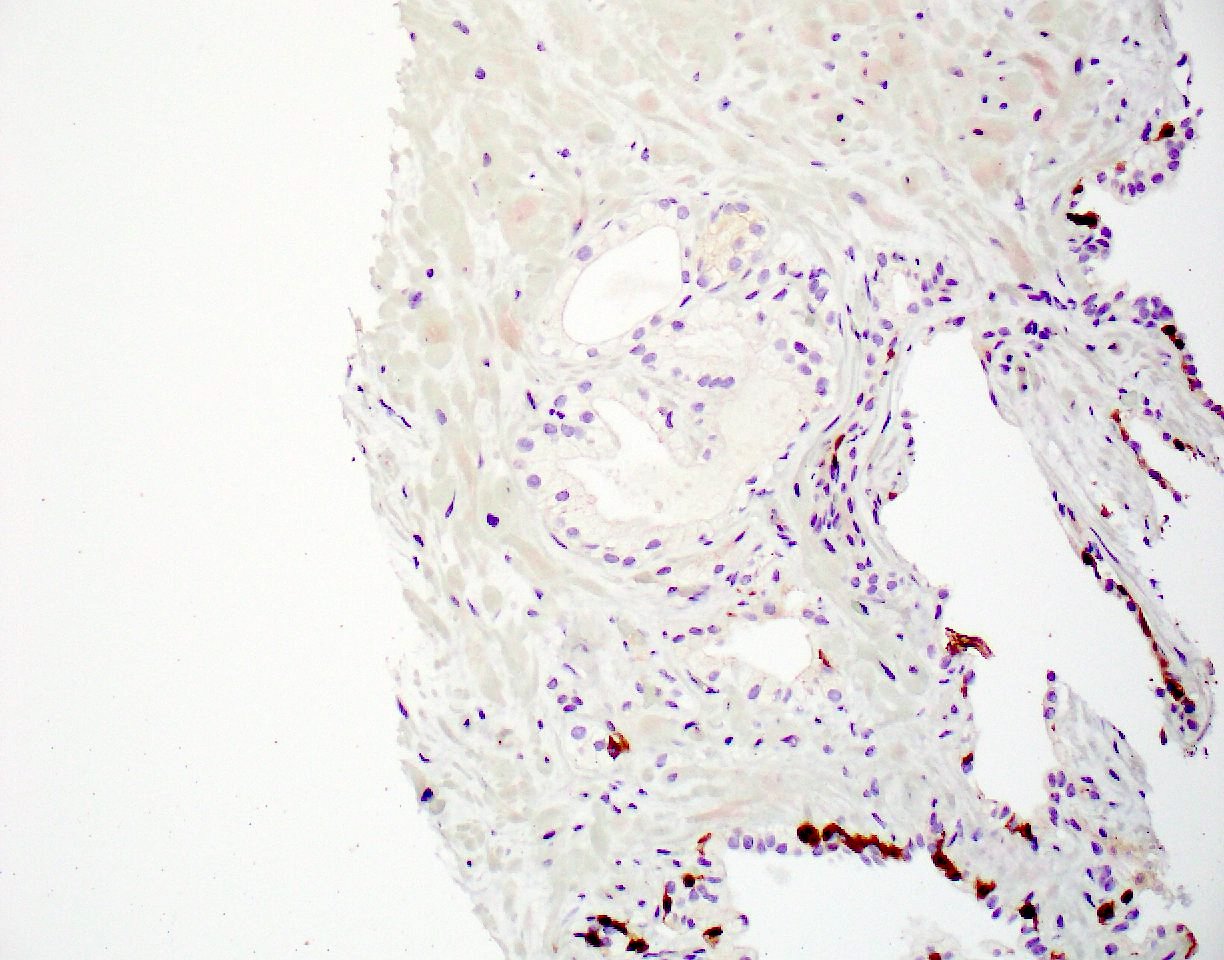
Microscopic (histologic) images
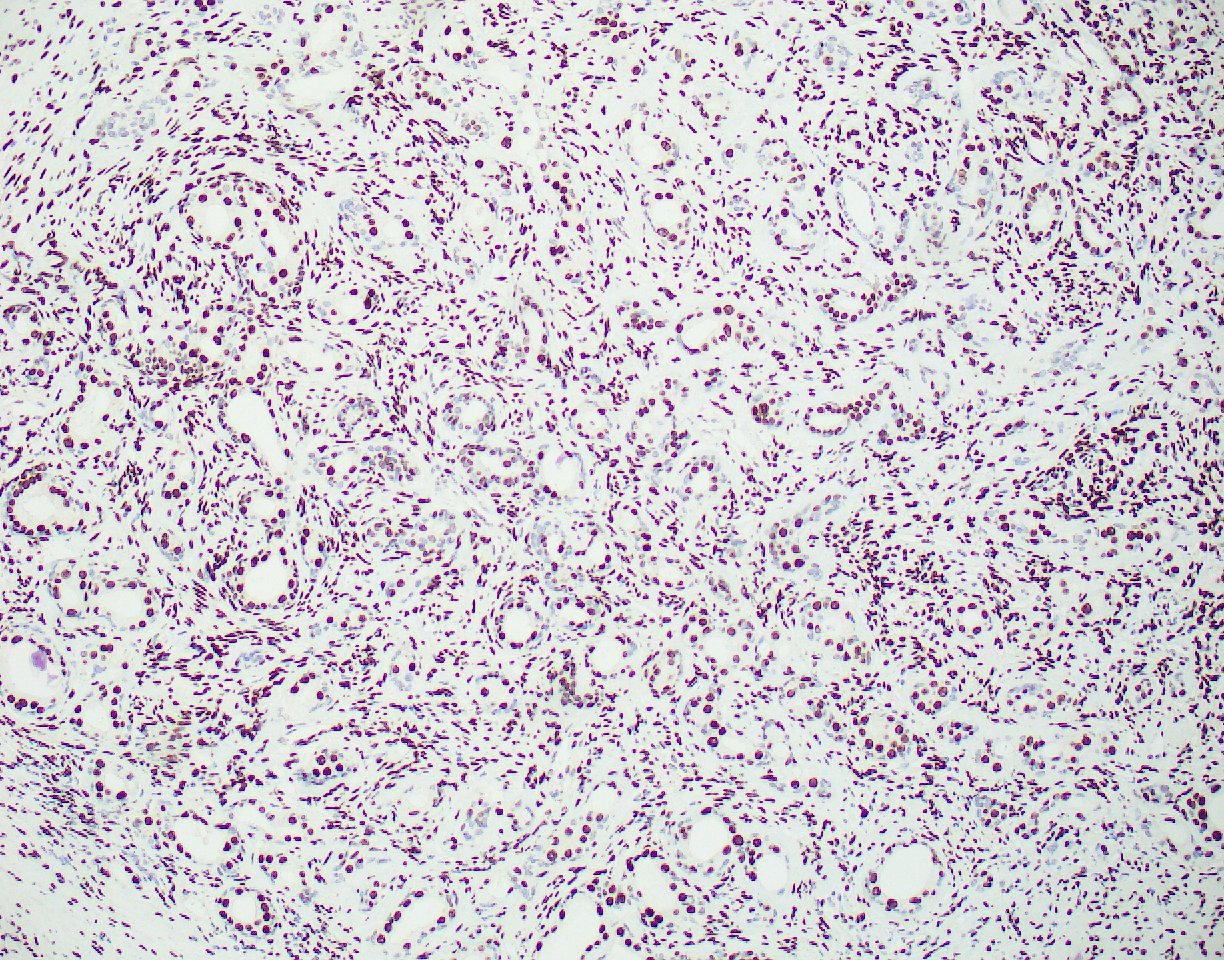
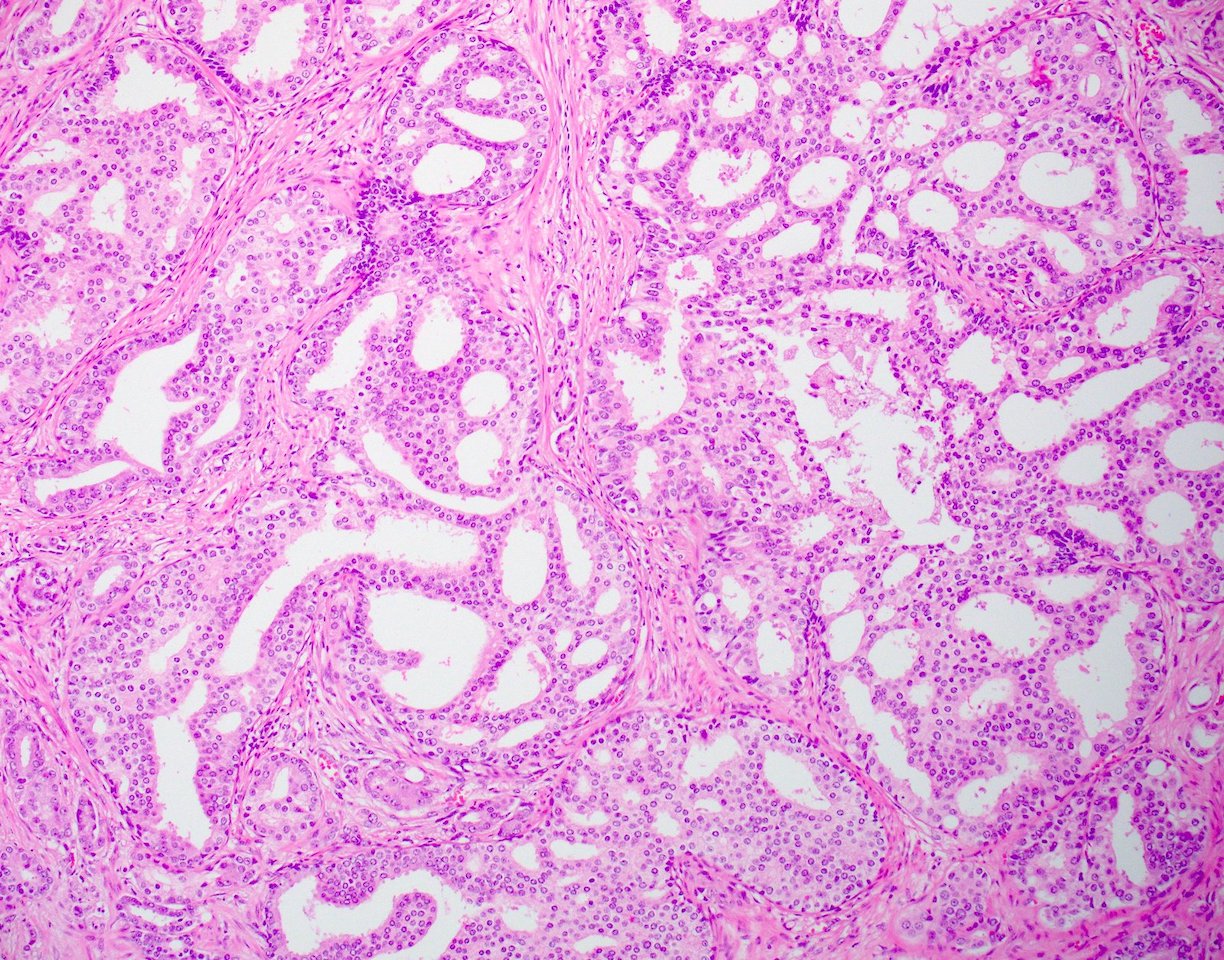
Contributed by Guang-Qian Xiao, M.D., Ph.D.
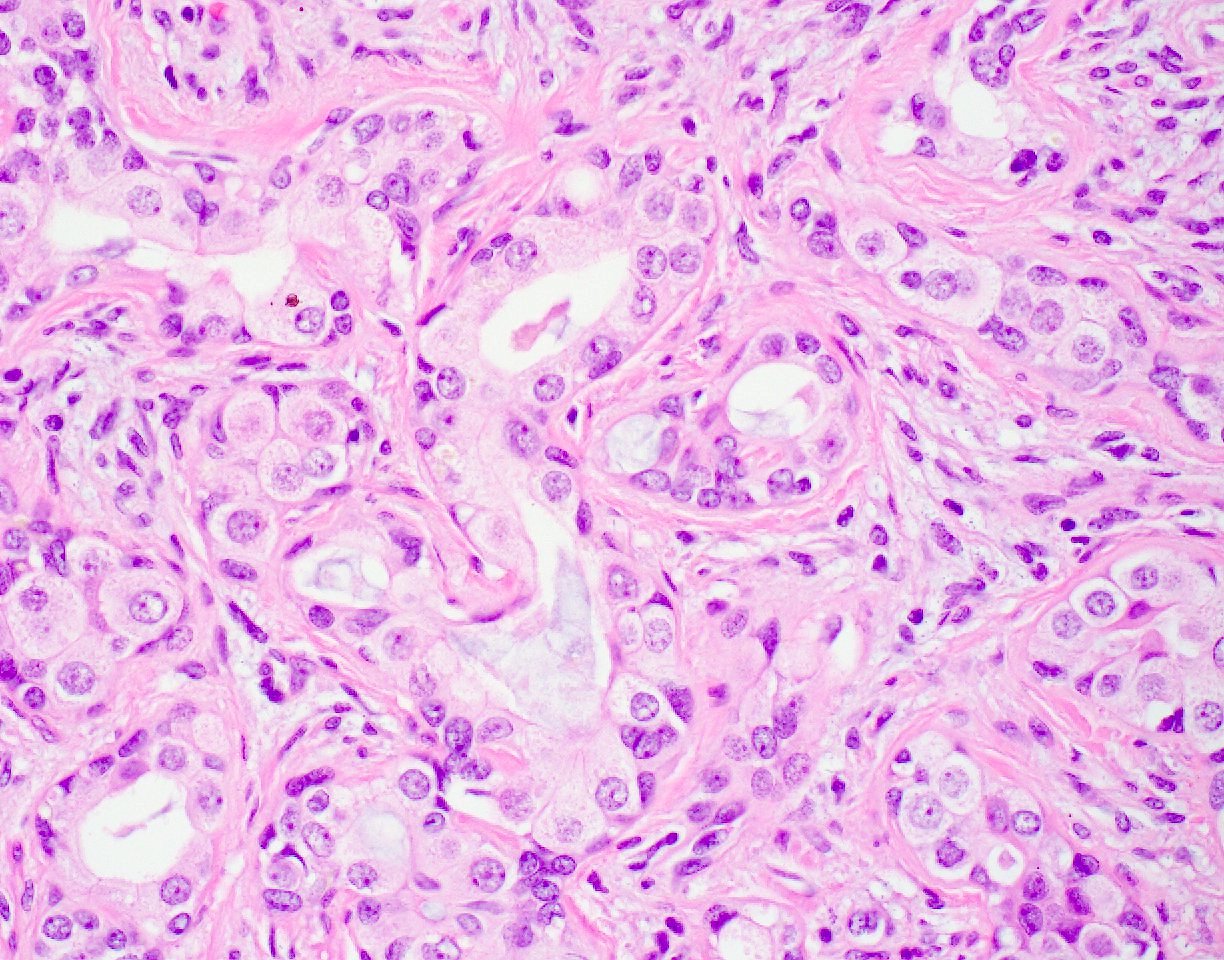
Adenosis


Prostatic adenocarcinoma
Atypical cribriform lesion


Prostatic adenocarcinoma
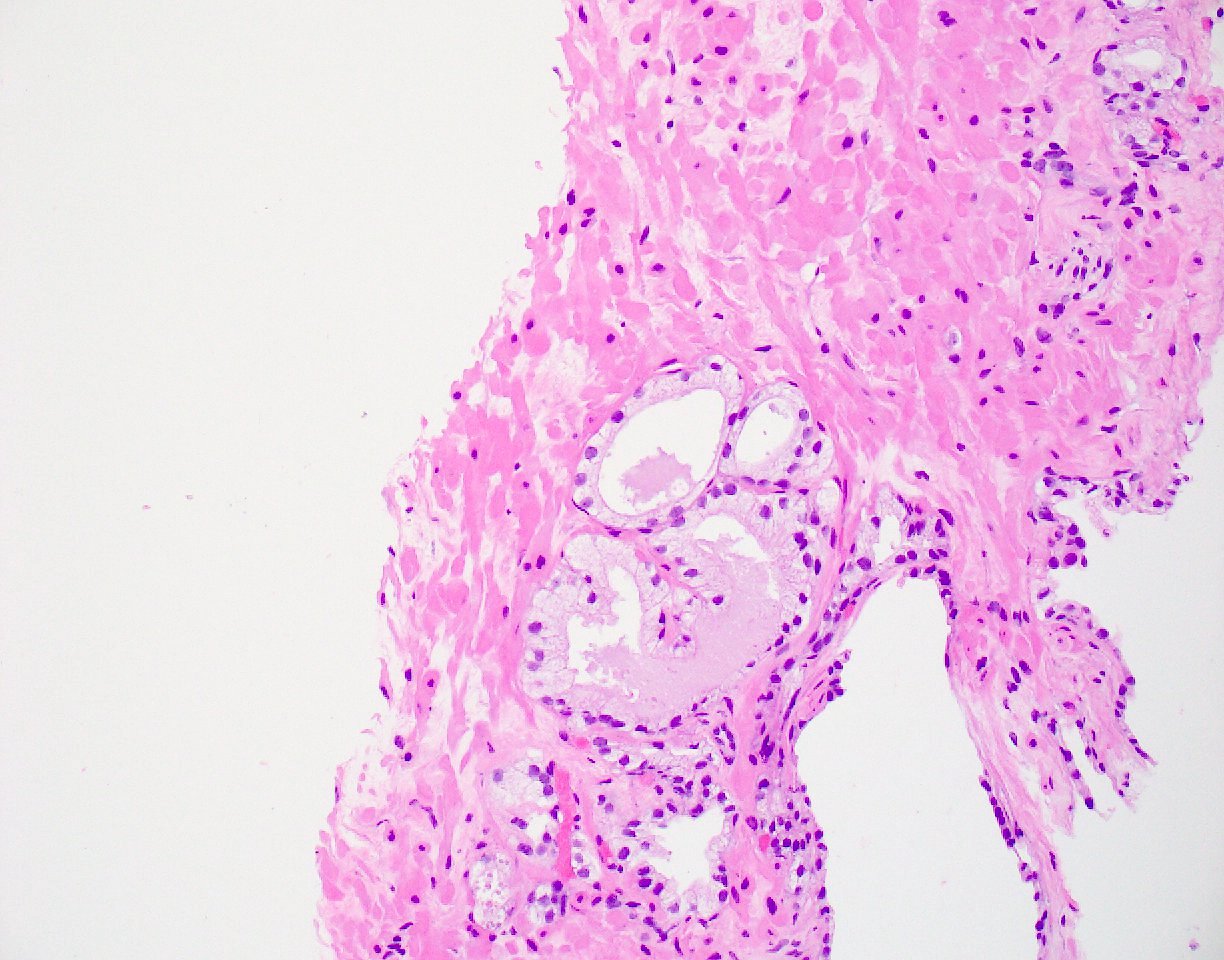
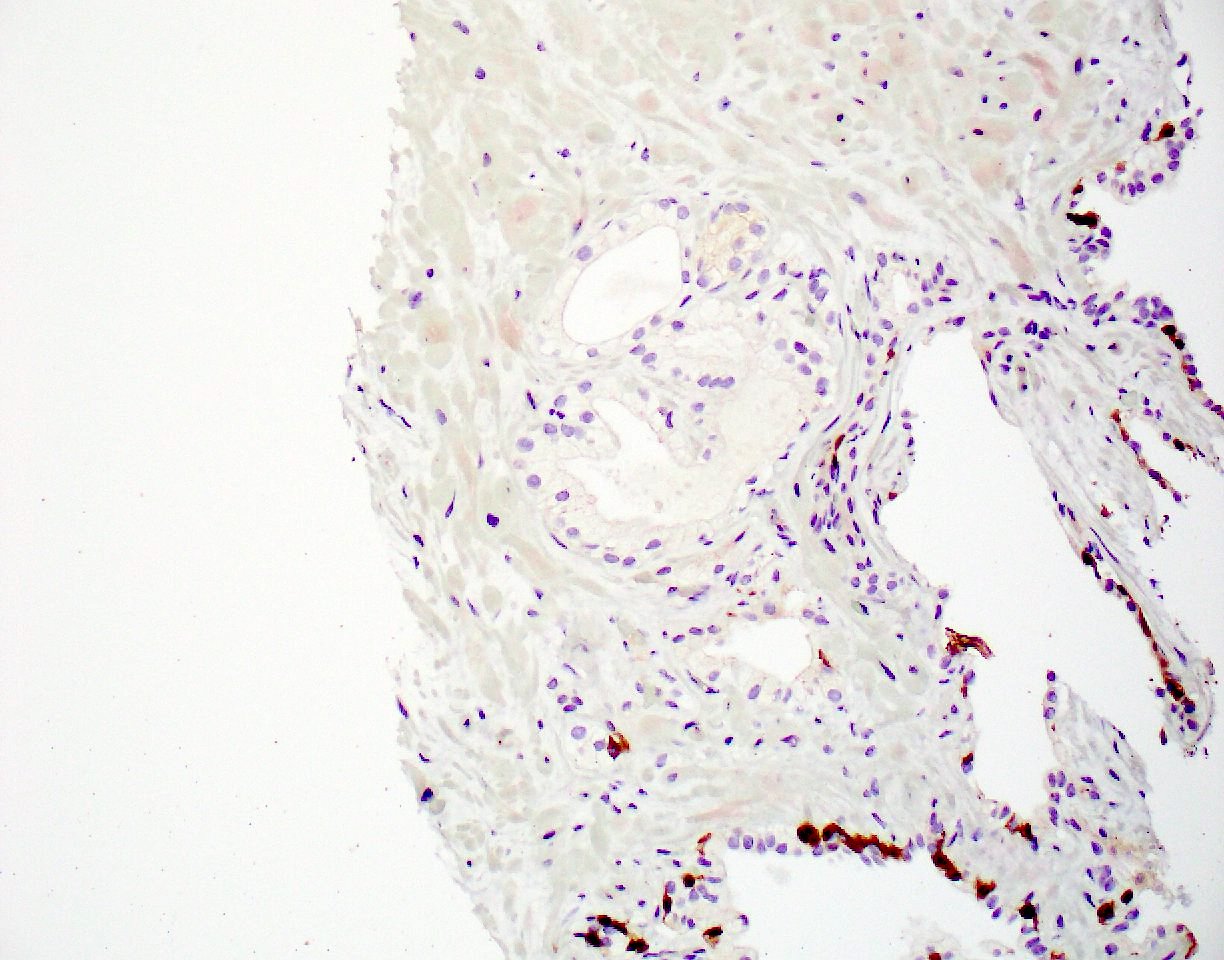
Partial atrophy


Partial atrophy


Carcinoma with radiation effect


Partial atrophy / neoacini


Prostatic ductal adenocarcinoma


p63 expressing prostatic adenocarcinoma


High molecular weight cytokeratin expressing prostatic adenocarcinoma
Positive staining - normal
- Prostate
- Basal cells: p63, 34 beta E12
- Luminal cells: PSA, prostein, PSAP / PAP, PSMA, NKX3.1, AR, CAM5.2 (J Pathol Transl Med 2016;50:345)
- Neuroendocrine cells: chromogranin, synaptophysin, CD56 and INSM1 (less specific)
- Seminal vesicles
- Positive for AR, PAX8, p63 and 34 beta E12
- References: Mod Pathol 2018;31:S12, Adv Anat Pathol 2018;25:387
Sample pathology report
- Prostate, needle biopsy:
- Prostatic adenocarcinoma, acinar type (see comment)
- Gleason score 3 + 4 (10%) = 7, grade group 2
- Cribriform Gleason pattern 4: focally present
- Number of involved cores: 1 of 1 core
- Tumor length: 2 mm
- Percentage involvement: 15% of the tissue
- Perineural invasion: not identified
- Intraductal carcinoma: not present
- Comment: PIN cocktail IHCs reveal atypical prostatic glands to be negative for p63 and 34 beta E12 (absence of basal cells) and positive for AMACR / P504S, supporting the diagnosis.
Differential diagnosis
- Benign mimickers of prostatic carcinoma can include adenosis and partial atrophy or prostatic neoacini (Arch Pathol Lab Med 2020;144:290, Mod Pathol 2018;31:S12, Adv Anat Pathol 2018;25:387):
- AMACR can be positive in both adenosis and partial atrophy
- ERG positivity (in the absence of basal cells) supports prostatic adenocarcinoma
- Prostate cancer, when involving the bladder, can be misdiagnosed as urothelial carcinoma if immunohistochemistry not performed (Arch Pathol Lab Med 2020;144:290, Adv Anat Pathol 2018;25:387):
- Useful IHC markers
- Positive for prostatic carcinoma: NKX3.1, ERG, PSA, PSMA, prostein, AR (small percentage of urothelial carcinoma can be AR positive)
- Positive for urothelial carcinoma: GATA3, p63, CK5/6, 34 beta E12 (very rarely, these markers can be positive in prostatic carcinoma)
- Useful IHC markers
Practice question #1
Which is the most sensitive marker for prostate origin?
- ERG
- NKX3.1
- P504S / AMACR
- PSA
Practice answer #1
B. NKX3.1. Both NKX3.1 and AR are very sensitive for prostatic secretory epithelium and are seen in almost 100% of naive / untreated prostatic adenocarcinoma (PAC). Even hormonal treated PACs are still 90% positive for NXK3.1 in various degrees. NKX3.1 is also much more specific than AR. Answer A is incorrect because ERG is only seen in up to 50% of PAC. Answer C is incorrect because P504S / AMACR is seen in about 80% of PAC. It can also be seen in benign glands and high grade prostatic intraepithelial neoplasia. Answer D is incorrect because PSA is not sensitive for poorly differentiated PAC.
Comment Here
Reference: Prostate gland & seminal vesicles - IHC overview
Comment Here
Reference: Prostate gland & seminal vesicles - IHC overview
Practice question #2
Which of the following lesions in the prostate can present with no basal cell layer?
- Atypical cribriform lesion
- High grade prostatic intraepithelial neoplasia
- Intraductal carcinoma
- Partial atrophy
Practice answer #2
D. Partial atrophy. Partially atrophic glands or neoacini can have sparse or no basal cells, especially in small, focal areas. Answers A, B and C are incorrect because by definition, high grade prostatic intraepithelial neoplasia, intraductal carcinoma and atypical cribriform lesions all retain a layer of basal cells (either continuous or discontinuous).
Comment Here
Reference: Prostate gland & seminal vesicles - IHC overview
Comment Here
Reference: Prostate gland & seminal vesicles - IHC overview
Practice question #3
A 72 year old man with a history of prostate cancer treated with radiation therapy undergoes a biopsy due to a rising PSA level. Histologic examination reveals atypical glands with cytologic atypia and fibrosis in the surrounding stroma, raising concern for posttreatment prostatic adenocarcinoma. Which of the following immunohistochemical profiles would be most useful in distinguishing postradiation recurrent prostatic adenocarcinoma from radiation associated benign glandular atypia?
- AMACR+, p63+, 34 beta E12+
- ERG-, p63+, AMACR+
- NKX3.1-, p40+, GATA3+
- NKX3.1+, p63-, 34 beta E12-
Practice answer #3
D. NKX3.1+, p63-, 34 beta E12-. Recurrent adenocarcinoma loses basal cell markers (p63, 34 beta E12) but retains NKX3.1, unlike benign irradiated glands, which keep a basal layer. Answer B is incorrect because p63 positivity indicates the presence of basal cells, which are retained in benign irradiated glands but lost in recurrent prostatic adenocarcinoma. Answer A is incorrect because the presence of basal cells excludes prostatic adenocarcinoma. Answer C is incorrect because p40 and GATA3 positivity suggest the presence of intact basal cells, which is characteristic of benign glands rather than recurrent prostatic adenocarcinoma.
Comment Here
Reference: Prostate gland & seminal vesicles - IHC overview
Comment Here
Reference: Prostate gland & seminal vesicles - IHC overview
Practice question #4
A 68 year old man presents with multiple bone metastases. A biopsy from a lytic lesion reveals poorly differentiated carcinoma with solid growth. The clinician suspects metastatic prostate cancer but wants to rule out other possible primaries. Which of the following IHC profiles provides the strongest evidence that this is a metastatic prostatic carcinoma rather than a malignancy of nonprostatic origin?
- NKX3.1+, PSA+, ERG+, p63-, CDX2+
- PAX8+, PSA-, AMACR+, 34 beta E12-, CK7+
- PSA-, AMACR+, NKX3.1-, CK7-, p63-
- PSA-, GATA3+, CK20-, CDX2+
Practice answer #4
A. NKX3.1+, PSA+, ERG+, p63-, CDX2+. PSA, NKX3.1, PSA and ERG are highly specific for prostate cancer. Additionally, the absence of p63 expression further supports prostate adenocarcinoma, which often loses basal cells. Answer C is incorrect because NXK3.1 negativity strongly argues against a malignancy of prostatic origin as it is rarely absent in prostate cancer. Answer B is incorrect because PAX8 expression suggests a Müllerian / renal origin, making prostate cancer unlikely. Answer D is incorrect because GATA3 positivity is characteristic of urothelial or breast carcinoma rather than prostate cancer.
Comment Here
Reference: Prostate gland & seminal vesicles - IHC overview
Comment Here
Reference: Prostate gland & seminal vesicles - IHC overview
