Bone & joints
Chondrosarcoma
Mesenchymal chondrosarcoma
Editorial Board Members: Jose G. Mantilla, M.D., Borislav A. Alexiev, M.D.


Last author update: 14 July 2021
Last staff update: 2 June 2025
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Mesenchymal chondrosarcoma
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Brčić I, Liegl-Atzwanger B. Mesenchymal chondrosarcoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissueeskchondrosarcomamesenchymal.html. Accessed September 18th, 2025.
Definition / general
- Malignant biphasic mesenchymal neoplasm with a well differentiated hyaline cartilage component
- Most cases have HEY-NCOA2 fusions; however IRF2BP2-CDX1 fusion has also been described (PLoS One 2012;7:e49705)
Essential features
- Malignant biphasic neoplasm that most commonly involves soft tissue, bone and intracranial sites, with tendency for late local recurrences and distant metastases
ICD coding
- ICD-O: 9240/3 - mesenchymal chondrosarcoma
- ICD-10
- ICD-11: 2B50.Z & XH8X47 - chondrosarcoma of bone and articular cartilage of unspecified sites & mesenchymal chondrosarcoma
Epidemiology
- Usually adolescents and young adults
- Slight female predominance
Sites
- Most commonly bone, soft tissue (head and neck, thigh), intracranial sites (meninges) and visceral organs
- Bone lesion: up to 50% in jaw (Arch Pathol Lab Med 2012;136:61)
Pathophysiology
- Gene fusion driven
Etiology
- HEY1-NCOA2 fusion evokes many different mechanisms, including direct DNA binding, protein - protein interaction and epigenetic modification
- Combination of these pathway dysregulations (including Notch signaling pathway, chromatin remodeling, apoptosis and transforming growth factor beta [TGFβ] signaling) results in a chimeric fusion protein that drives the biology of mesenchymal chondrosarcoma (Curr Oncol Rep 2018;20:37)
Clinical features
- Clinical symptoms depend on the tumor location and can last for years prior to diagnosis
- Enlarging, usually painful mass
- Neurologic symptoms If arising in spine / cranium (Arch Pathol Lab Med 2012;136:61)
Diagnosis
- Diagnostic diagram includes radiology, histology (biopsy, resection specimen) with immunohistochemistry and molecular analysis
Radiology description
- CT scan:
- Lobulated, destructive lytic lesion with granular, ring and arc or irregularly shaped calcifications (Radiology 1993;186:819, Skeletal Radiol 2005;34:785)
- Bone lesion: usually erodes / destroys the cortex and involves the surrounding soft tissue
- MRI:
- Lobulated, heterogeneous lesion with low signal intensity on T1 weighted images and high signal intensity on T2 (Skeletal Radiol 2005;34:785)
Radiology images
Contributed by Borislav A. Alexiev, M.D.

Anterior mediastinal mass
Prognostic factors
- In one study, 5, 10 and 20 year overall survival was 55.0%, 43.5% and 15.7%, respectively (PLoS One 2015;10:e0122216)
- With chemotherapy: 5 year and 10 year overall survival is 84% and 80%, respectively
- Without chemotherapy, under surveillance: 5 year and 10 year overall survival is 73% and 46%, respectively (Eur J Cancer 2015;51:374)
Case reports
- 30 year old man with dizziness, headache and imbalance (Neurol India 2012;60:121)
- 31 year old man with vascular lesion near knee (Case #335)
- 34 year old man with expansile, erosive tumor of mandible (J Cancer Res Ther 2011;7:192)
- 52 year old man with progressive proptosis of eye (Case Rep Med 2012;2012:292147)
- 64 year old man with renal mass (Diagn Pathol 2012;7:125)
- 64 year old woman with renal mass (Oncol Lett 2020;19:885)
Treatment
- Wide local excision with negative margins
- If tumor is not resected in toto, chemotherapy can be used (however, better survival is published in only one study) (Cancer 2008;112:2424, PLoS One 2015;10:e0122216)
- Radiotherapy
Gross description
- Lobulated, solid, firm, gray-tan, fleshy mass with scattered gritty white calcifications
- Bone lesions arise in the medullary cavity or on the bone surface, causing cortical destruction and extension into the soft tissue (Arch Pathol Lab Med 2012;136:61)
Gross images
Contributed by Iva Brčić, M.D., Ph.D. and Bernadette Liegl-Atzwanger, M.D.
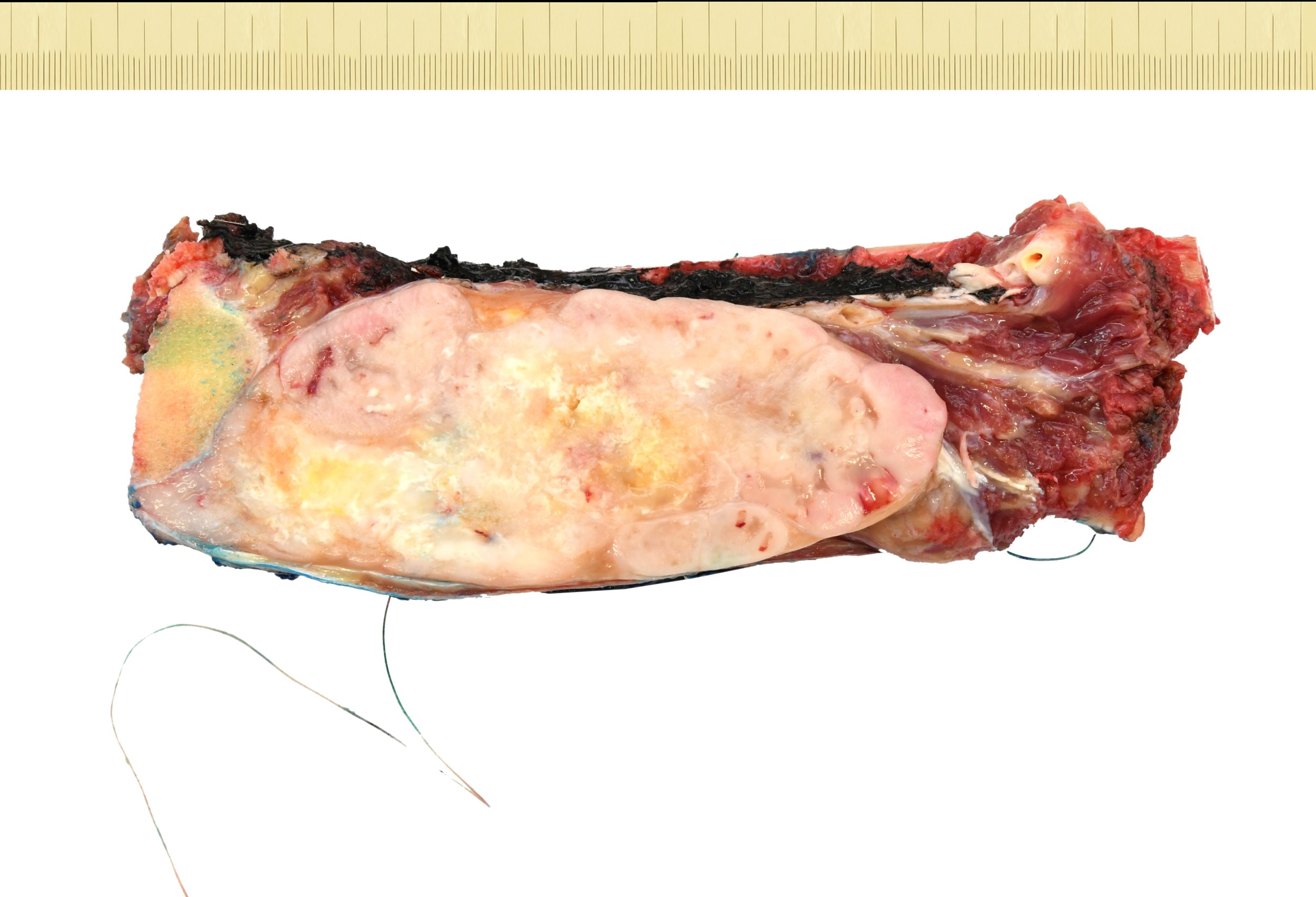
Lobulated mass
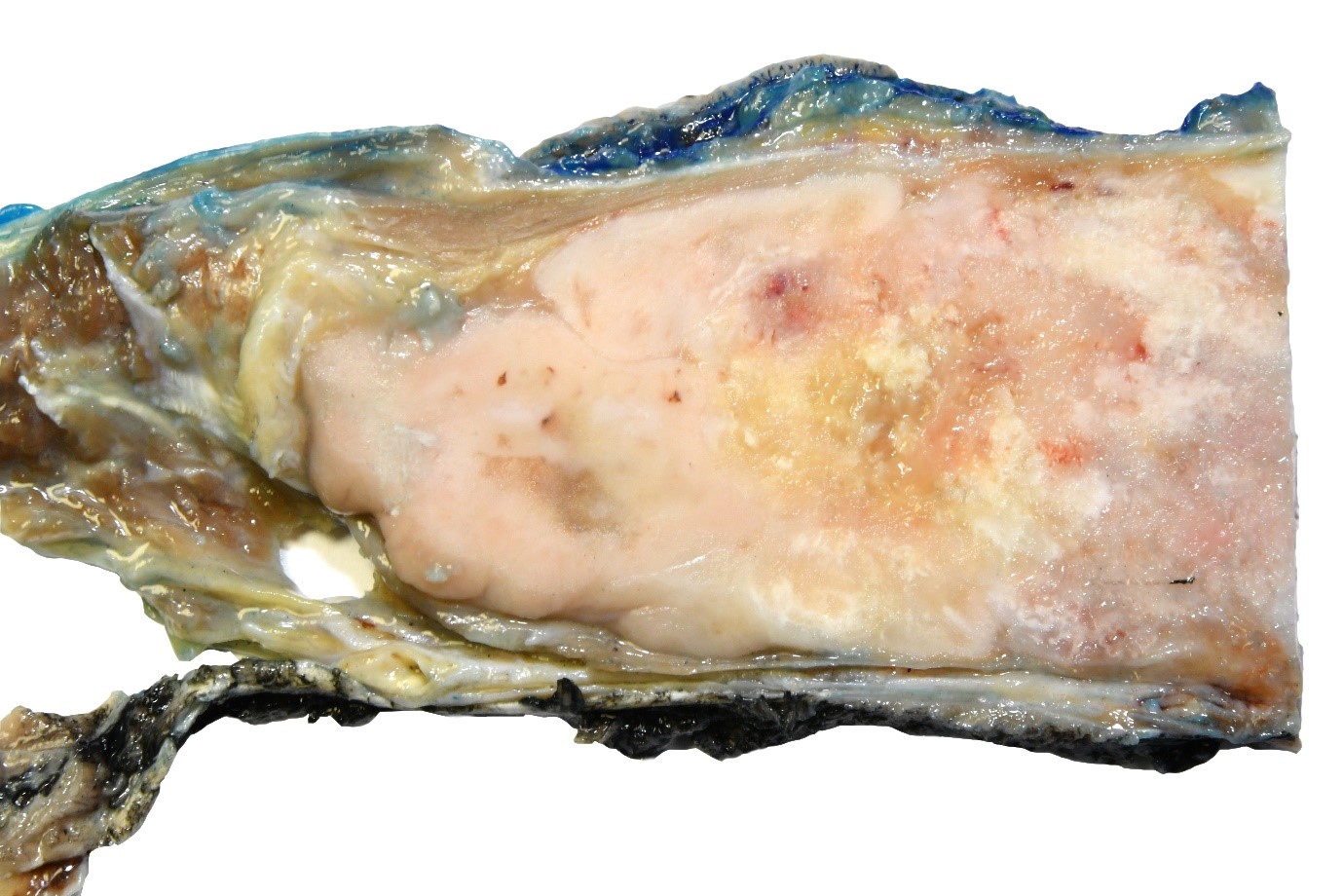
Calcifications
Frozen section description
- Tumor composed of islands of well differentiated hyaline cartilage and primitive mesenchymal cells / undifferentiated small blue cells
Microscopic (histologic) description
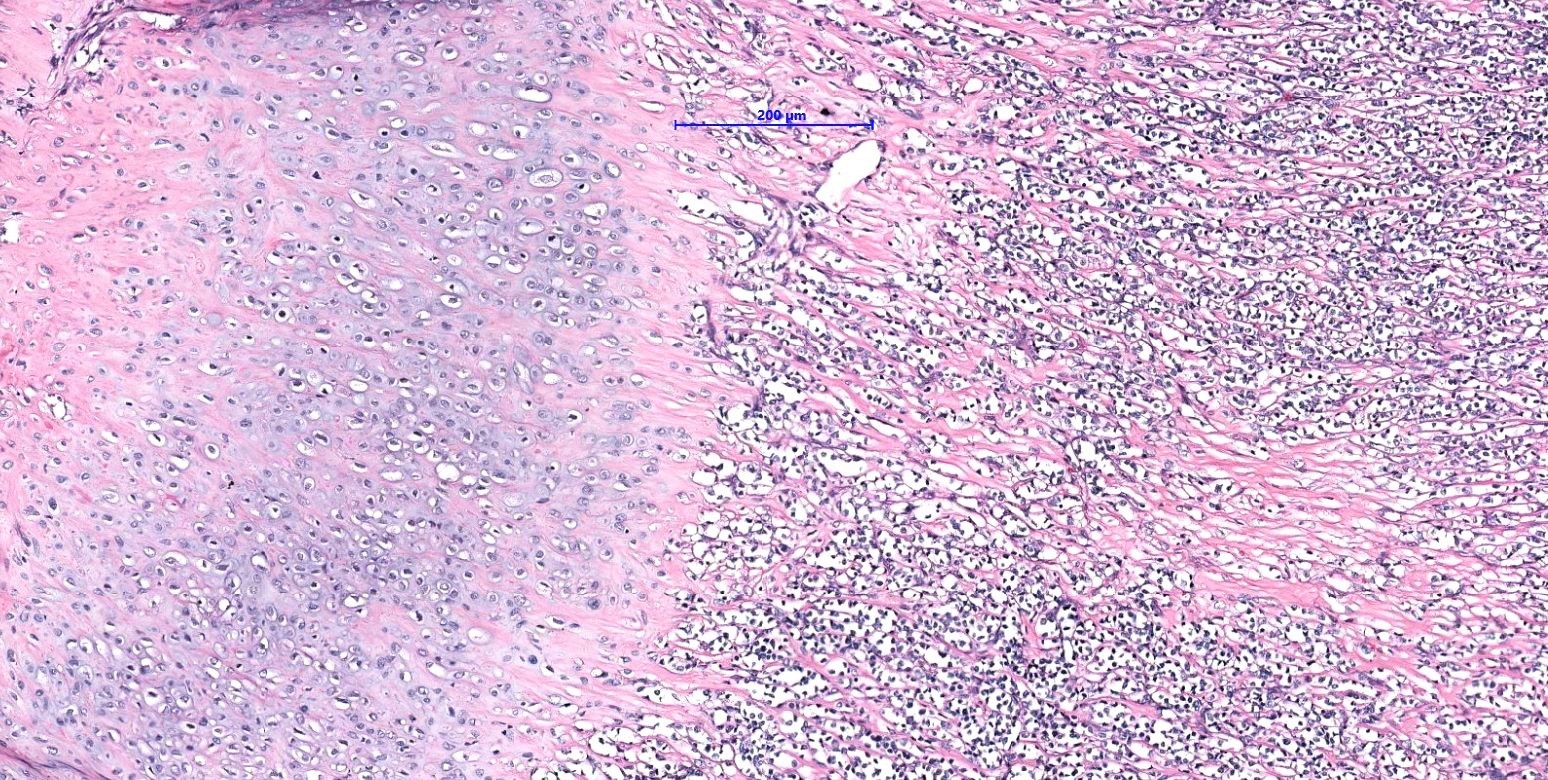
- Solid sheets of undifferentiated small blue cells with a hemangiopericytoma-like vascular pattern mixed with islands of mature appearing, well differentiated hyaline cartilage
- Usually mitotic activity or necrosis present (Arch Pathol Lab Med 2018;142:1421, Arch Pathol Lab Med 2012;136:61)
Microscopic (histologic) images
Contributed by Iva Brčić, M.D., Ph.D. and Bernadette Liegl-Atzwanger, M.D.
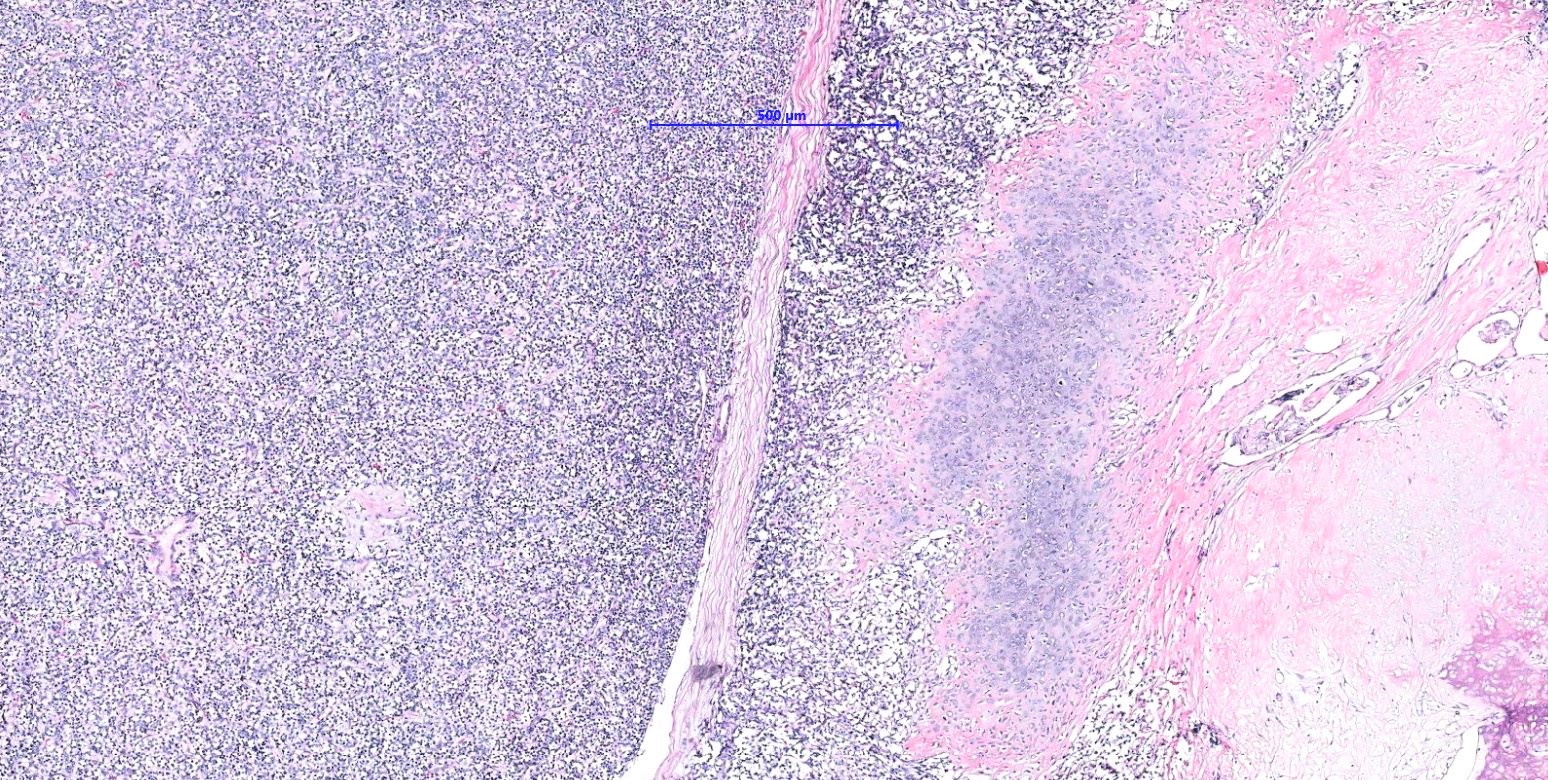
Biphasic tumor
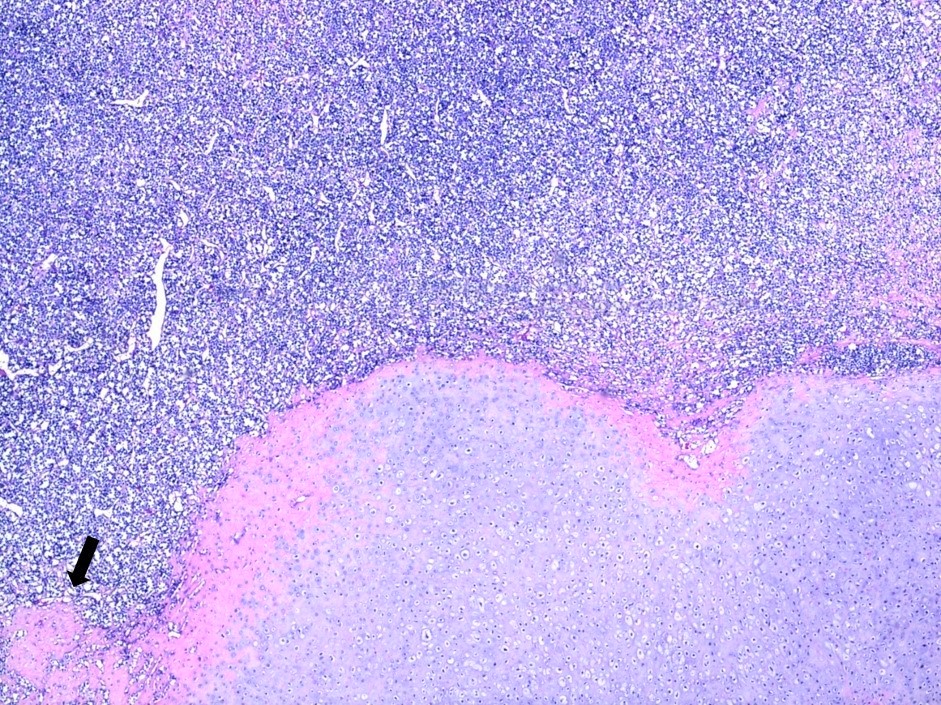
Abrupt transition
2 components
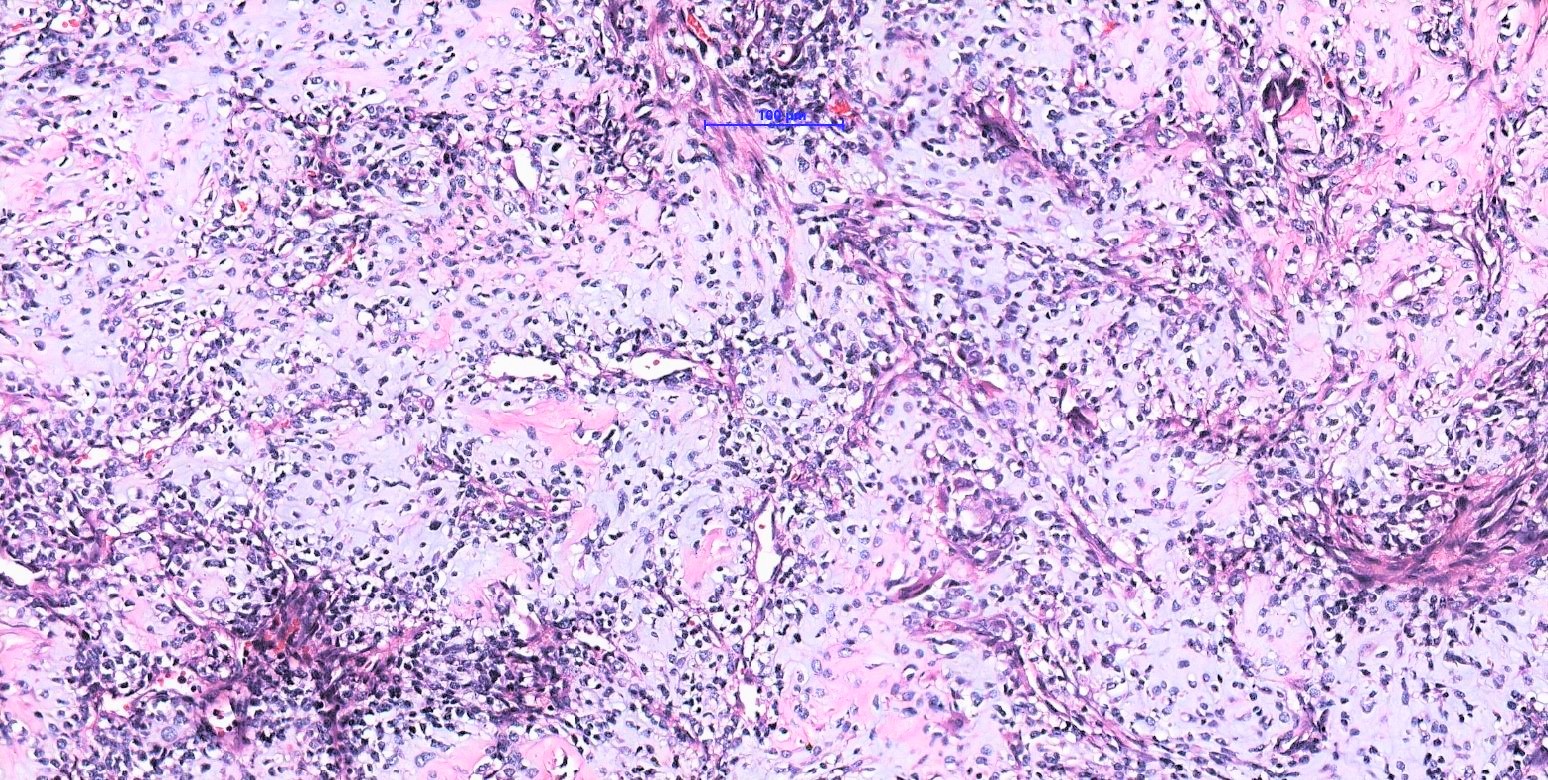
Spindle cell morphology
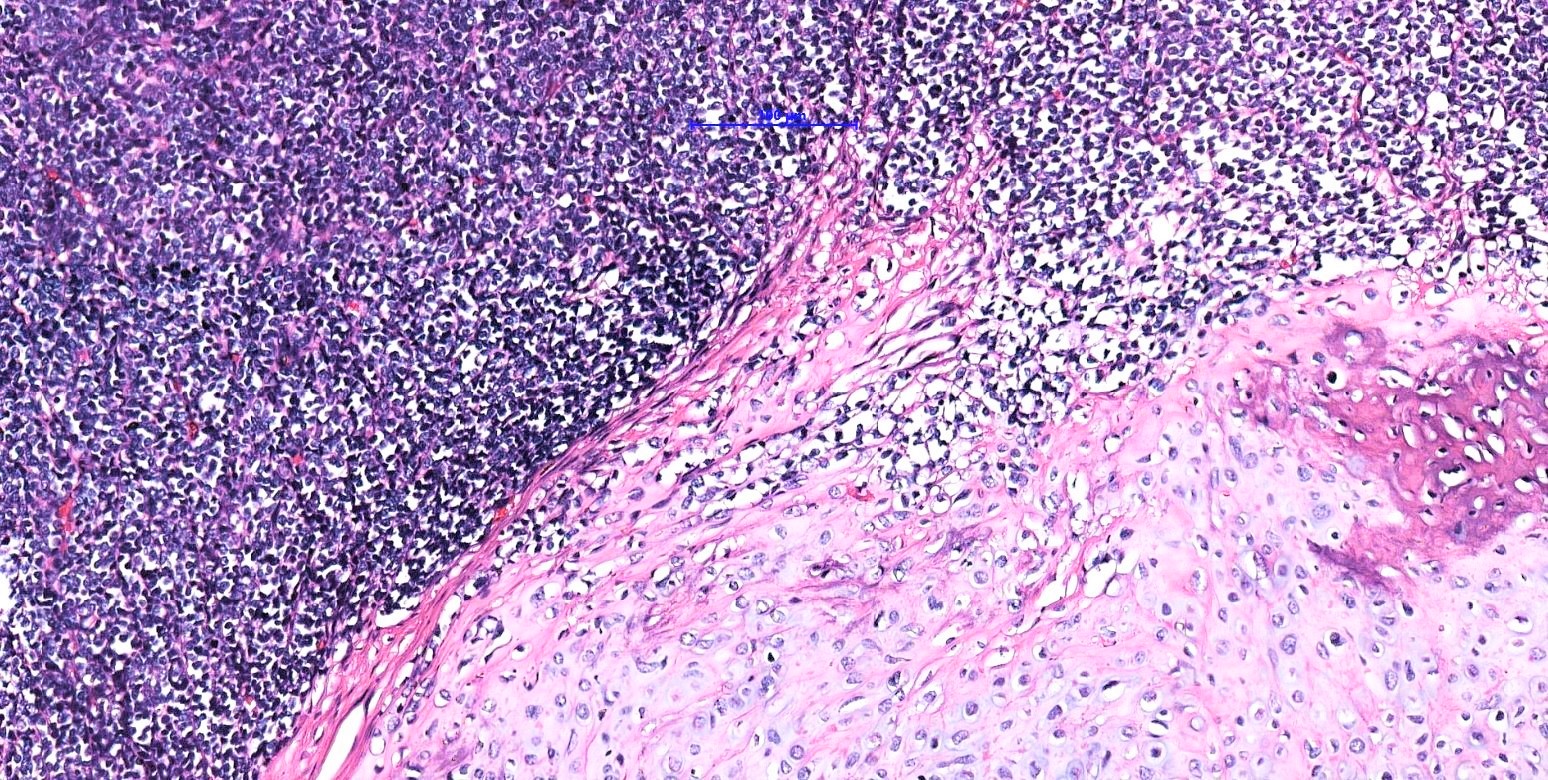
Transition higher power
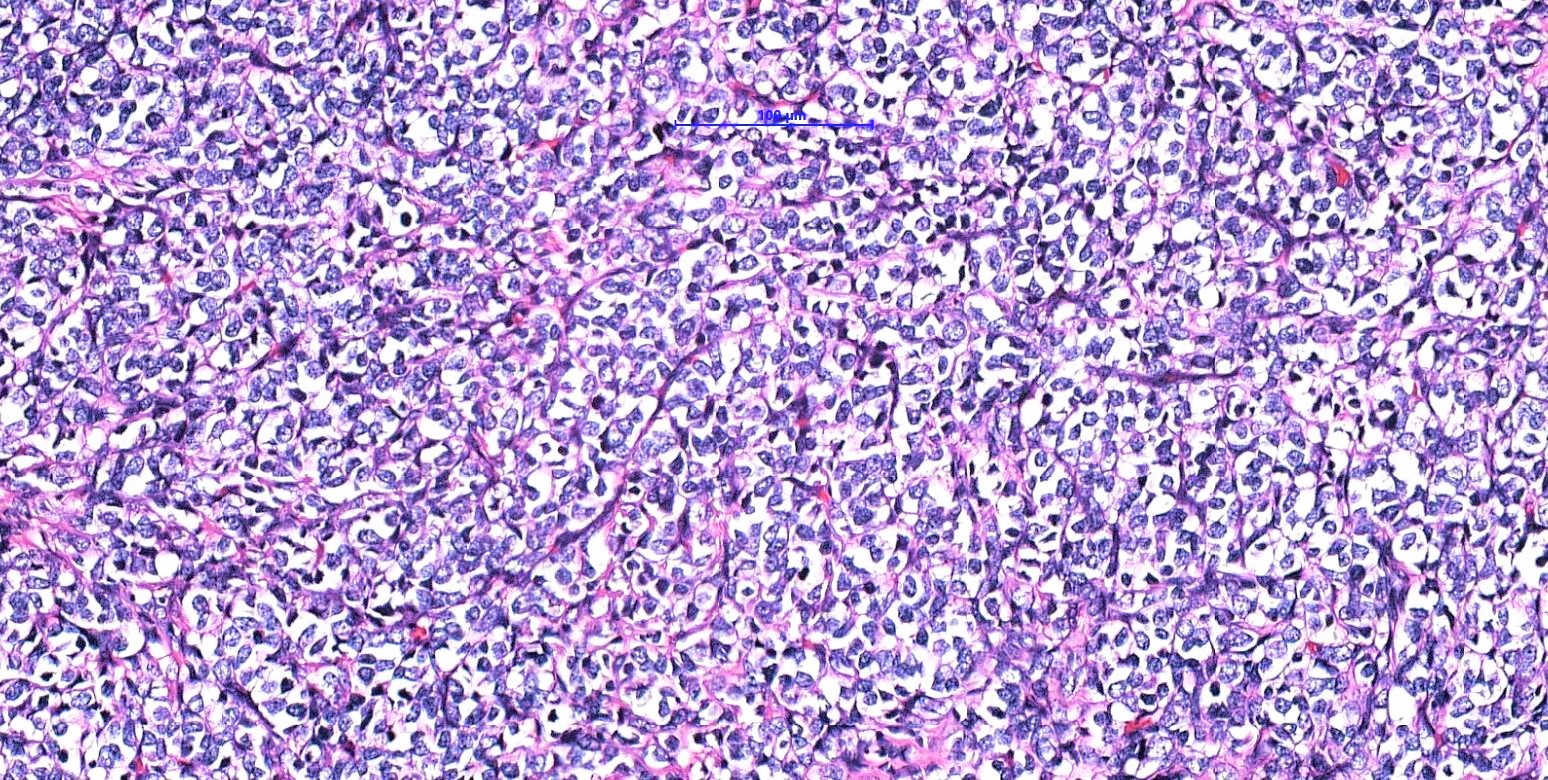
Cellular atypia
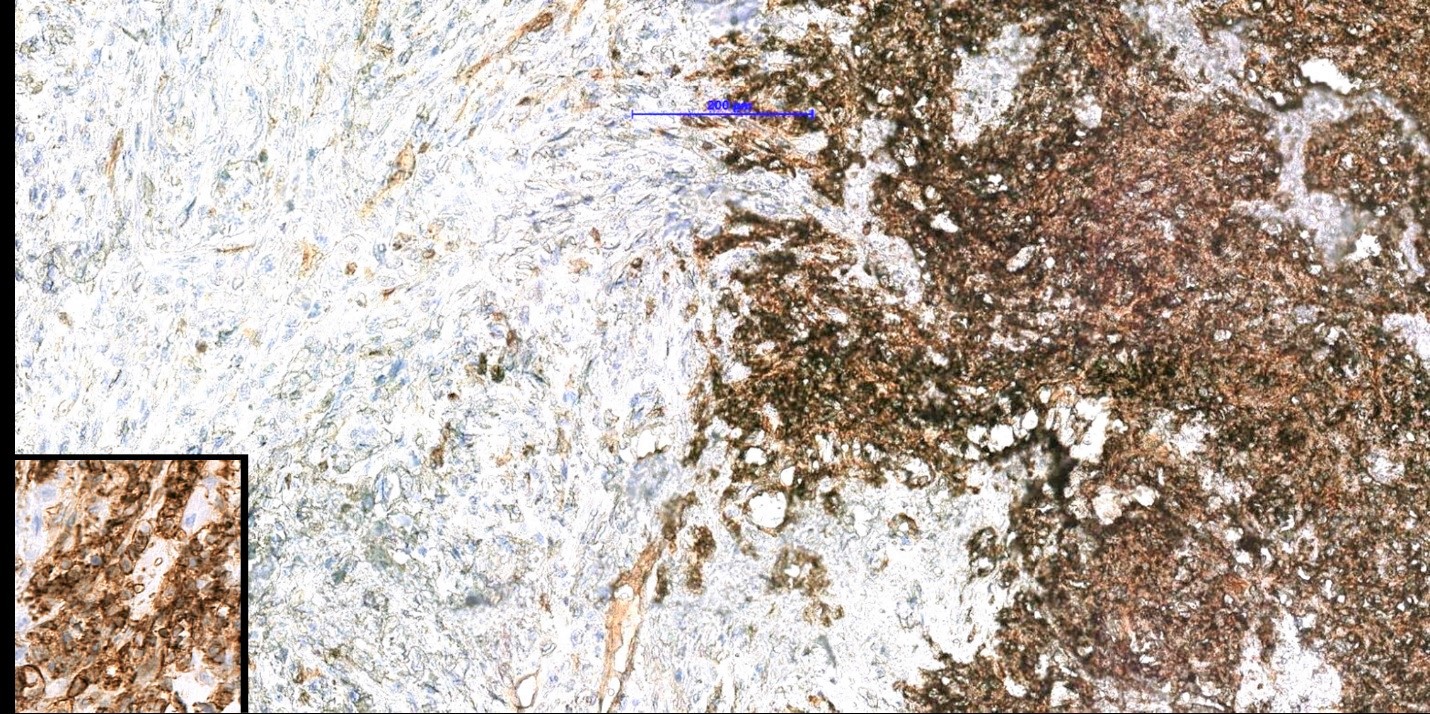
CD99 staining
Cytology description
- Highly cellular smears composed of small round blue cells with high nuclear to cytoplasmic ratio infiltrating the fibrillary matrix (Arch Pathol Lab Med 2018;142:1421)
Positive stains
- Cartilaginous nodules: S100
- Small round cell component:
- CD99 (usually membranous), NKX2.2 (in up to 75%, Mod Pathol 2016;29:370)
- NKX3.1 (Am J Surg Pathol 2020;44:719) although in one study, negative in all cases (Histopathology 2021;78:334)
- SOX9 (both components) (Arch Pathol Lab Med 2018;142:1421)
- Occasionally myogenic markers, such as desmin
Molecular / cytogenetics description
- In most cases, recurrent HEY1-NCOA2 gene fusion (Genes Chromosomes Cancer 2012;51:127)
- In one case, IRF2BP2-CDX1 fusion described (PLoS One 2012;7:e49705)
Sample pathology report
- Right thigh, excision:
- Extraskeletal mesenchymal chondrosarcoma (see comment)
- Comment: Tumor is composed of islands of well differentiated hyaline cartilage and primitive mesenchymal cells. Immunohistochemically, the tumor cells are positive for S100, focally positive for CD99 and SOX9 and are negative for CD20 and keratin. The morphology and immunoprofile strongly support the diagnosis of mesenchymal chondrosarcoma.
Differential diagnosis
- Other small round cell neoplasms:
- Rule out metastatic small cell carcinoma and melanoma, especially when only the undifferentiated component is present in the biopsy
- Ewing sarcoma:
- Lymphoma:
- Lack of cartilaginous component; lymphoid antibodies positive
- Rhabdomyosarcoma:
- Synovial sarcoma:
- Malignant solitary fibrous tumor:
Practice question #1
Which of the following is true about mesenchymal chondrosarcoma?
- Cut surface is white with myxoid areas
- Cytology smears are paucicellular
- On imaging, calcifications are rare
- Tumor cells are typically negative for S100
- Tumor is composed of undifferentiated small blue cells mixed with islands of mature appearing, well differentiated hyaline cartilage
Practice answer #1
E. Tumor is composed of undifferentiated small blue cells mixed with islands of mature appearing, well differentiated hyaline cartilage
Comment Here
Reference: Mesenchymal chondrosarcoma
Comment Here
Reference: Mesenchymal chondrosarcoma
Practice question #2
A 24 year old man presented with an intracranial mass arising from the meninges. Histologically, tumor is composed of areas with small blue cells and islands of well differentiated hyaline cartilage. Which of the following is most likely the correct diagnosis?
- B cell lymphoma
- Ewing sarcoma
- Mesenchymal chondrosarcoma
- Rhabdomyosarcoma
- Synovial sarcoma
Practice answer #2
