

Lung
General
Biopsies
Author: Phillip McMullen, M.D., Ph.D.
Editorial Board Member: Jefree J. Schulte, M.D.

Last author update: 25 November 2022
Last staff update: 20 January 2023
Copyright: 2019-2024, PathologyOutlines.com, Inc.
PubMed Search: Lung biopsy
See Also: Adenocarcinoma, Squamous cell carcinoma

Table of Contents
Definition / general | Essential features | Epidemiology | Sites | Diagrams / tables | Diagnosis | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Molecular / cytogenetics description | Sample pathology report | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: McMullen P. Biopsies. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumorbiopsies.html. Accessed May 12th, 2024.
Definition / general
- Precise histologic classification of lung cancer is essential due to advances in tailored therapies for specific subtypes
- Biopsy is the initial step for the classification of advanced or metastatic disease and for obtaining tissue for molecular / biomarker testing
- Obtaining multiple biopsy specimens to allow for both IHC and molecular / biomarker testing is optimal
Essential features
- Diagnosis in small biopsies utilizes morphologic features and judicial immunohistochemical / special stain evaluation in cases with ambiguous morphologies
- Biopsy materials should be preserved as much as possible for molecular / biomarker testing
- Diagnostic terminology can differ between small biopsies and resection specimens
Epidemiology
- Up to 90% of lung cancers are directly attributable to smoking (Transl Lung Cancer Res 2018;7:220)
- 10 - 15% of lung cancers occur in never smokers (Transl Lung Cancer Res 2018;7:220)
- These are often associated with driver mutations (such as EGFR mutations and ALK fusions)
- Majority of cases present with advanced stage where diagnosis is often limited to small biopsies (CA Cancer J Clin 2018;68:7)
Sites
- Biopsies may be obtained from either primary or metastatic sites
Diagrams / tables



Diagnosis
Terminology in small biopsy and cytology versus resection specimens for adenocarcinoma and squamous cell carcinoma (adapted from Table 3, J Thorac Oncol 2022;17:362)
Terminology for small biopsies and cytology versus resection specimens for small cell carcinoma, large cell neuroendocrine carcinoma, adenosquamous carcinoma and pleomorphic carcinoma (adapted from Table 4, J Thorac Oncol 2022;17:362)
Guidelines for good practice of small biopsies and cytologic preparations (adapted / reprinted from J Thorac Oncol 2022;17:362):
(Abbreviations: ADC, adenocarcinoma; AIS, adenocarcinoma in situ; NOS, not otherwise specified; NSCC, non-small cell carcinoma; SQCC, squamous cell carcinoma)
| Morphology / stains | Terminology for small biopsies and cytology specimens | Terminology for resection specimens |
| Morphologic squamous cell patterns clearly present | Squamous cell carcinoma | Squamous cell carcinoma |
| Morphologic adenocarcinoma patterns clearly present | Adenocarcinoma (list patterns in the diagnosis) | Adenocarcinoma predominant patterns: Lepidic Acinar Papillary Solid Micropapillary |
| Adenocarcinoma with lepidic pattern (if pure, list the differential diagnosis on the right and add a comment that an invasive component cannot be excluded) | Minimally invasive adenocarcinoma, adenocarcinoma in situ or an invasive adenocarcinoma with a lepidic component | |
| Invasive mucinous adenocarcinoma (list the patterns; use the term mucinous adenocarcinoma with lepidic pattern if pure lepidic pattern and mention the differential diagnosis listed on the right) | Invasive mucinous adenocarcinoma, minimally invasive adenocarcinoma or adenocarcinoma in situ, mucinous type | |
| Adenocarcinoma with colloid features | Colloid adenocarcinoma | |
| Adenocarcinoma with fetal features | Fetal adenocarcinoma | |
| Adenocarcinoma with enteric features a | Enteric adenocarcinoma | |
| Morphologic squamous cell patterns not present but supported by stains (i.e., p40+) | Non-small cell carcinoma, favor squamous cell carcinoma b | Squamous cell carcinoma (nonkeratinizing pattern may be a component of the tumor) |
| Morphologic adenocarcinoma patterns not present but supported by special stains (i.e., TTF1+) | Non-small cell carcinoma, favor adenocarcinoma b | Adenocarcinoma (solid pattern may just be one component of the tumor) |
| No clear adenocarcinoma, squamous or neuroendocrine morphology or staining pattern | Non-small cell carcinoma, NOS c | Large cell carcinoma |
- Metastatic carcinomas should be carefully excluded with clinical and appropriate but judicious immunohistochemical examination
- Categories do not always correspond to solid predominant adenocarcinoma or nonkeratinizing squamous cell carcinoma, respectively; poorly differentiated components in adenocarcinoma or squamous cell carcinoma may be sampled
- Non-small cell carcinoma, NOS pattern can be seen not only in large cell carcinomas but also when the solid, poorly differentiated component of adenocarcinomas or squamous cell carcinomas is sampled but does not express immunohistochemical markers or mucin
Terminology for small biopsies and cytology versus resection specimens for small cell carcinoma, large cell neuroendocrine carcinoma, adenosquamous carcinoma and pleomorphic carcinoma (adapted from Table 4, J Thorac Oncol 2022;17:362)
| Terminology for small biopsies and cytology specimens | Terminology for resection specimens |
| Small cell carcinoma | Small cell carcinoma |
| Non-small cell carcinoma with neuroendocrine morphology and positive neuroendocrine markers, possible large cell neuroendocrine carcinoma | Large cell neuroendocrine carcinoma |
| Morphologic squamous cell and adenocarcinoma patterns both present: non-small cell carcinoma, NOS
(Comment that adenocarcinoma and squamous components are present and that this could represent adenosquamous carcinoma) | Adenosquamous carcinoma (if both components ≥ 10%) |
| Morphologic squamous cell or adenocarcinoma patterns not present but immunohistochemical stains favor separate squamous and adenocarcinoma components: non-small cell carcinoma, NOS
(Specify the results of the immunohistochemical stains and the interpretation and comment that this could represent adenosquamous carcinoma but that diagnosis requires a resection specimen) | Adenocarcinoma, squamous cell carcinoma, adenosquamous carcinoma or large cell carcinoma with unclear immunohistochemical features |
| Non-small cell carcinoma with spindle cell or giant cell carcinoma (Mention if adenocarcinoma or squamous carcinoma is present and comment that this could represent a pleomorphic carcinoma; however, that diagnosis requires a resection specimen) | Pleomorphic, spindle cell or giant cell carcinoma |
Guidelines for good practice of small biopsies and cytologic preparations (adapted / reprinted from J Thorac Oncol 2022;17:362):
- For small biopsies and cytology, NSCC should be further classified into a more specific type, such as ADC or SQCC
- The term non-small cell lung carcinoma, NOS (NSCLC, NOS) should be used as little as possible
- When a diagnosis is made in a small biopsy or cytology specimen in conjunction with special studies, it should be clarified whether the diagnosis was established on the basis of light microscopy alone or if special stains were required
- The term nonsquamous cell carcinoma (non-SQCC) should not be used by pathologists
- Terminology in above tables should be used in routine diagnosis, future research and clinical trials, in order to ensure a uniform classification of disease cohorts in relation to tumor subtypes
- When paired cytology and biopsy specimens exist, they should be reviewed together to achieve the most specific and concordant diagnosis
- The terms AIS and minimally invasive ADC should not be used for diagnosis of small biopsies or cytology specimens (a noninvasive pattern is present in a small biopsy should be referred to as a lepidic growth pattern)
- The term large cell carcinoma should not be used for diagnosis in small biopsy or cytology specimens and should be restricted to resection specimens where the tumor is thoroughly sampled to exclude a differentiated component
- Tumors exhibiting sarcomatoid features (marked nuclear pleomorphism, malignant giant cells or spindle cell morphology) should be classified as specifically as possible (i.e., ADC; NSCC, favor ADC; SQCC; or NSCC favor SQCC) with an additional statement that giant or spindle cell features are present (note: if diagnosis specific features are not present, the term NSCC, NOS should be used, again with comment on the sarcomatoid features)
- Neuroendocrine immunohistochemical markers should be performed only in cases where there is suspected neuroendocrine morphology
(Abbreviations: ADC, adenocarcinoma; AIS, adenocarcinoma in situ; NOS, not otherwise specified; NSCC, non-small cell carcinoma; SQCC, squamous cell carcinoma)
Treatment
- Identification of targetable mutations has led to overall decrease in NSCLC mortality disproportionate to the decrease in incidence (N Engl J Med 2020;383:640)
- PDL1 evaluation recommended for all nonneuroendocrine carcinomas (J Thorac Oncol 2022;17:362)
Microscopic (histologic) description
- Adenocarcinoma: gland formation, mucin production and variety of architectural patterns
- Squamous cell carcinoma: intracellular bridges, keratinization
- Adenosquamous carcinoma: mixed adenocarcinomatous and squamous differentiation or solid proliferation without obvious differentiation but with immunophenotypic evidence of both squamous and glandular differentiation; can only be diagnosed on resection specimens
- Non-small cell carcinoma: carcinoma without obvious glandular or squamous differentiation further characterized by immunostaining
- Neuroendocrine tumors: salt and pepper chromatin, organoid / trabecular / nested growth
- Small cell carcinoma: fine chromatin, nuclear molding, marked mitotic activity, necrosis
Microscopic (histologic) images
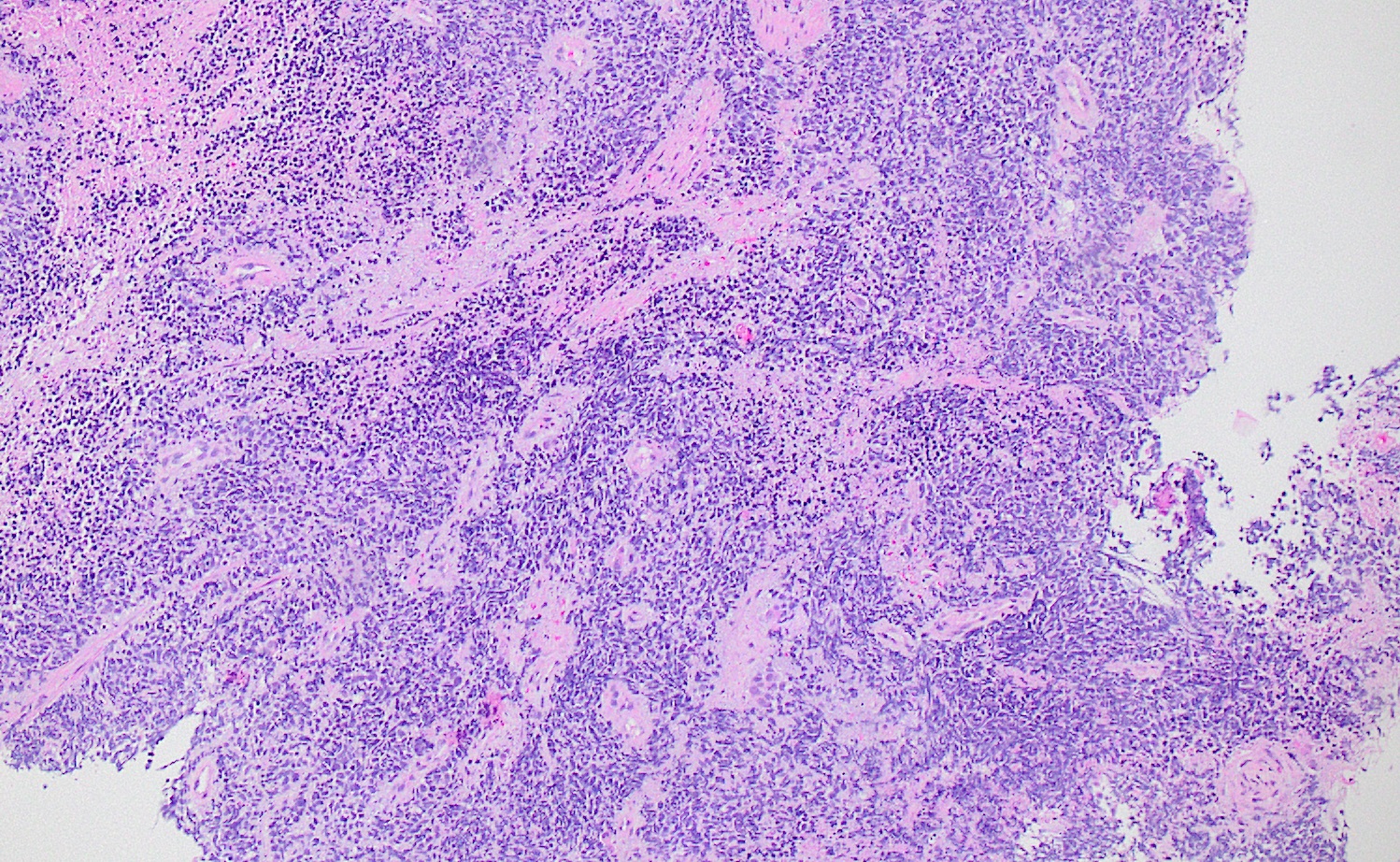
Contributed by Phillip McMullen, M.D., Ph.D.
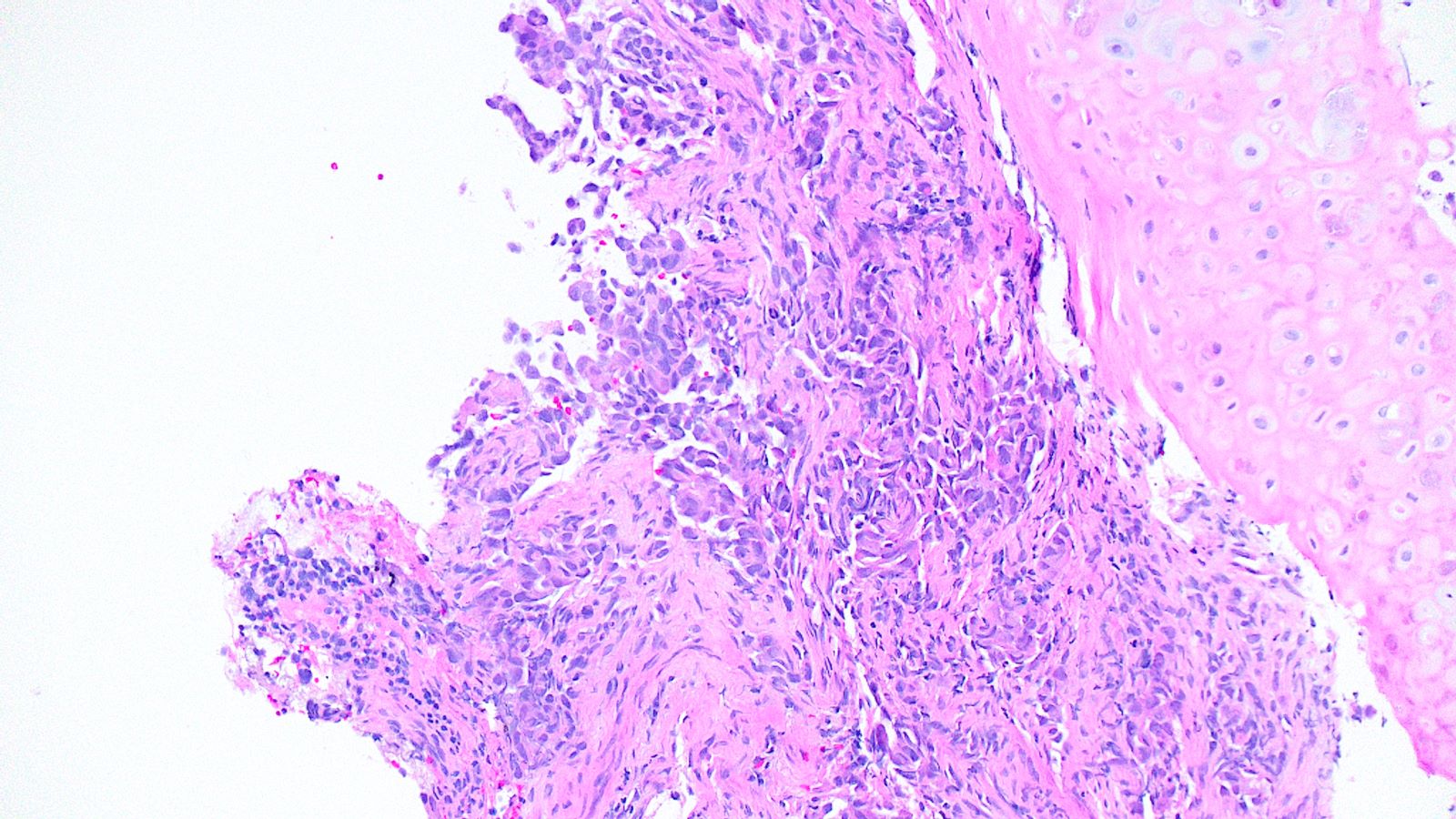
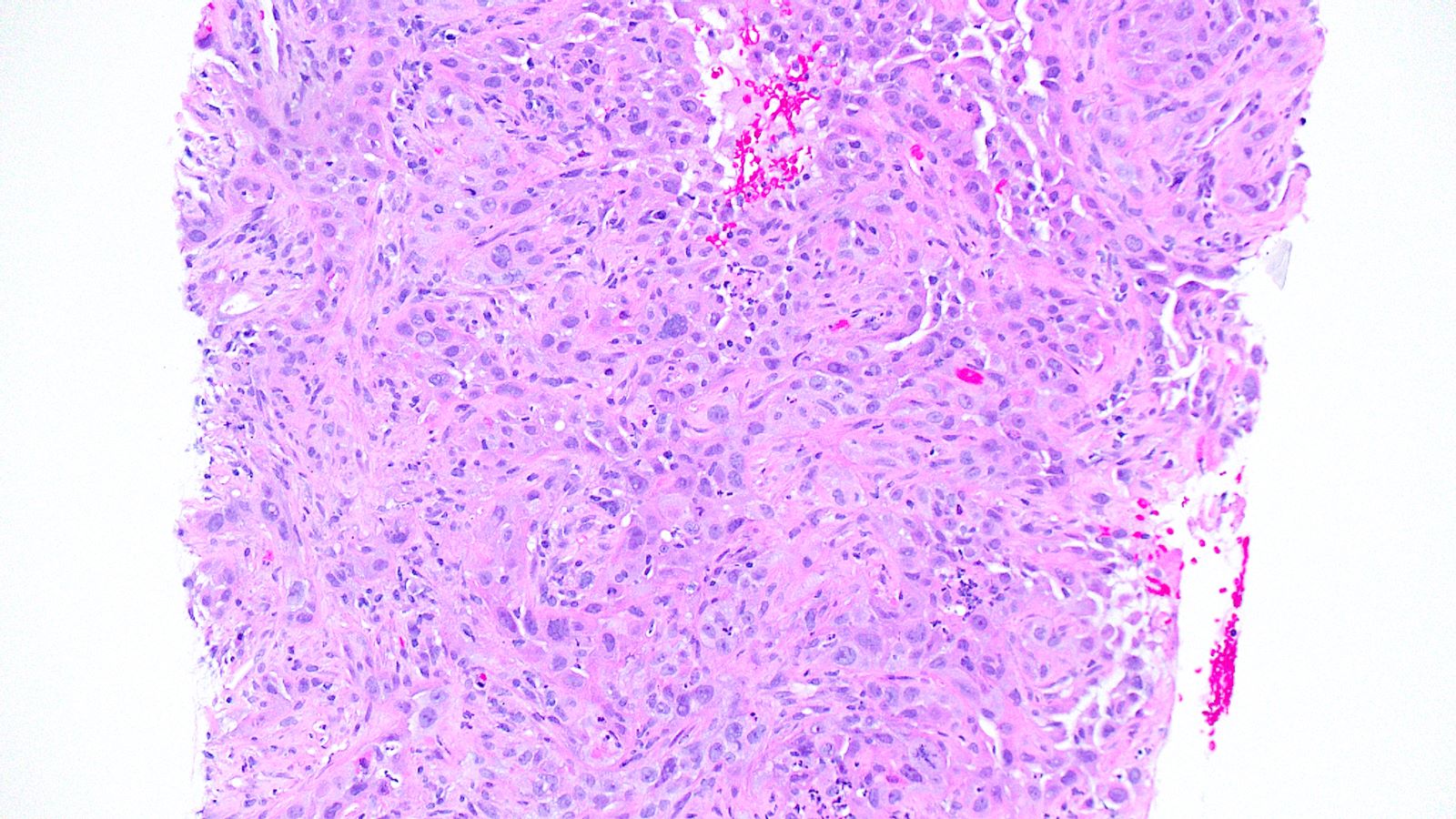
Lung mass
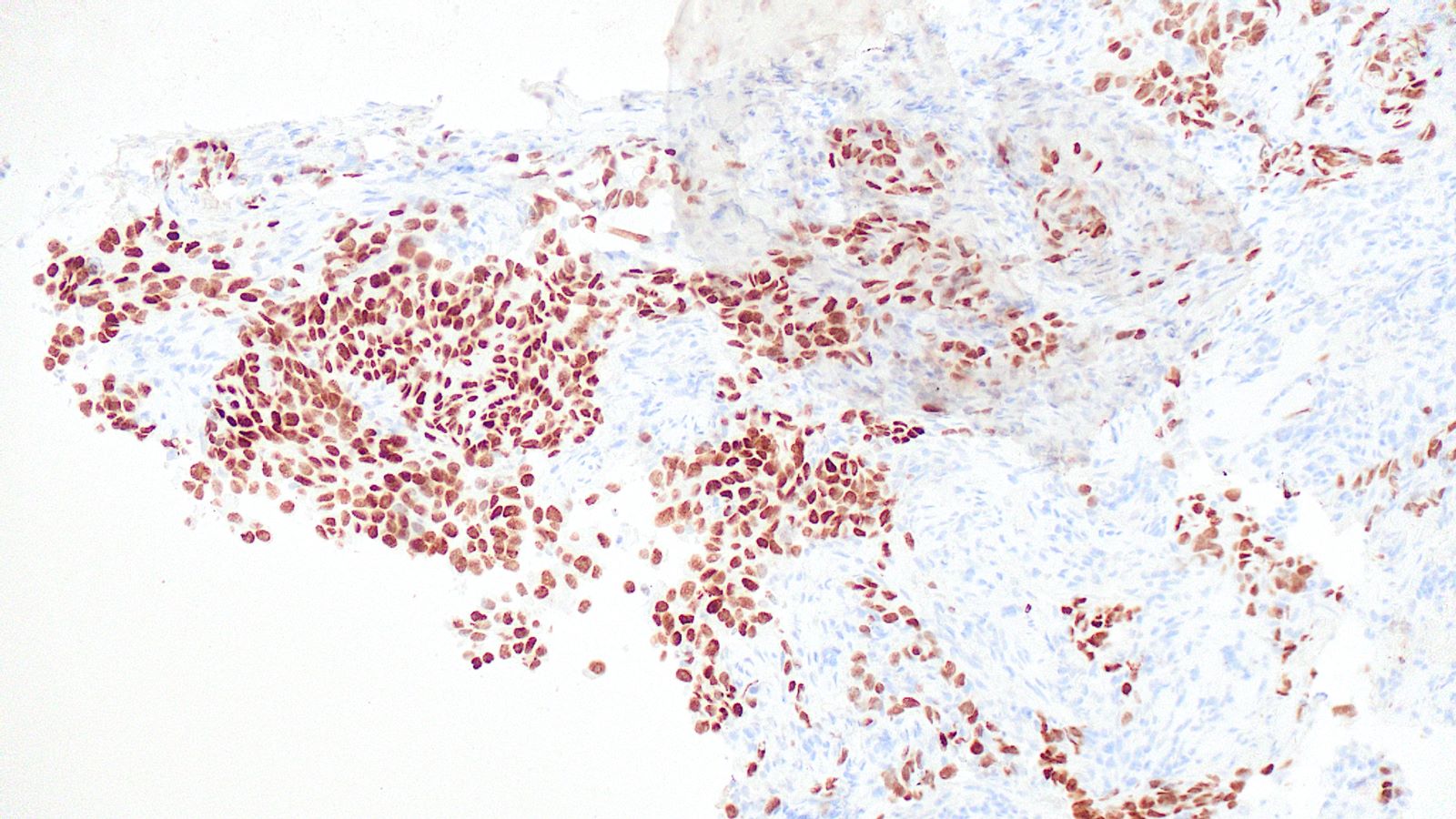
TTF1
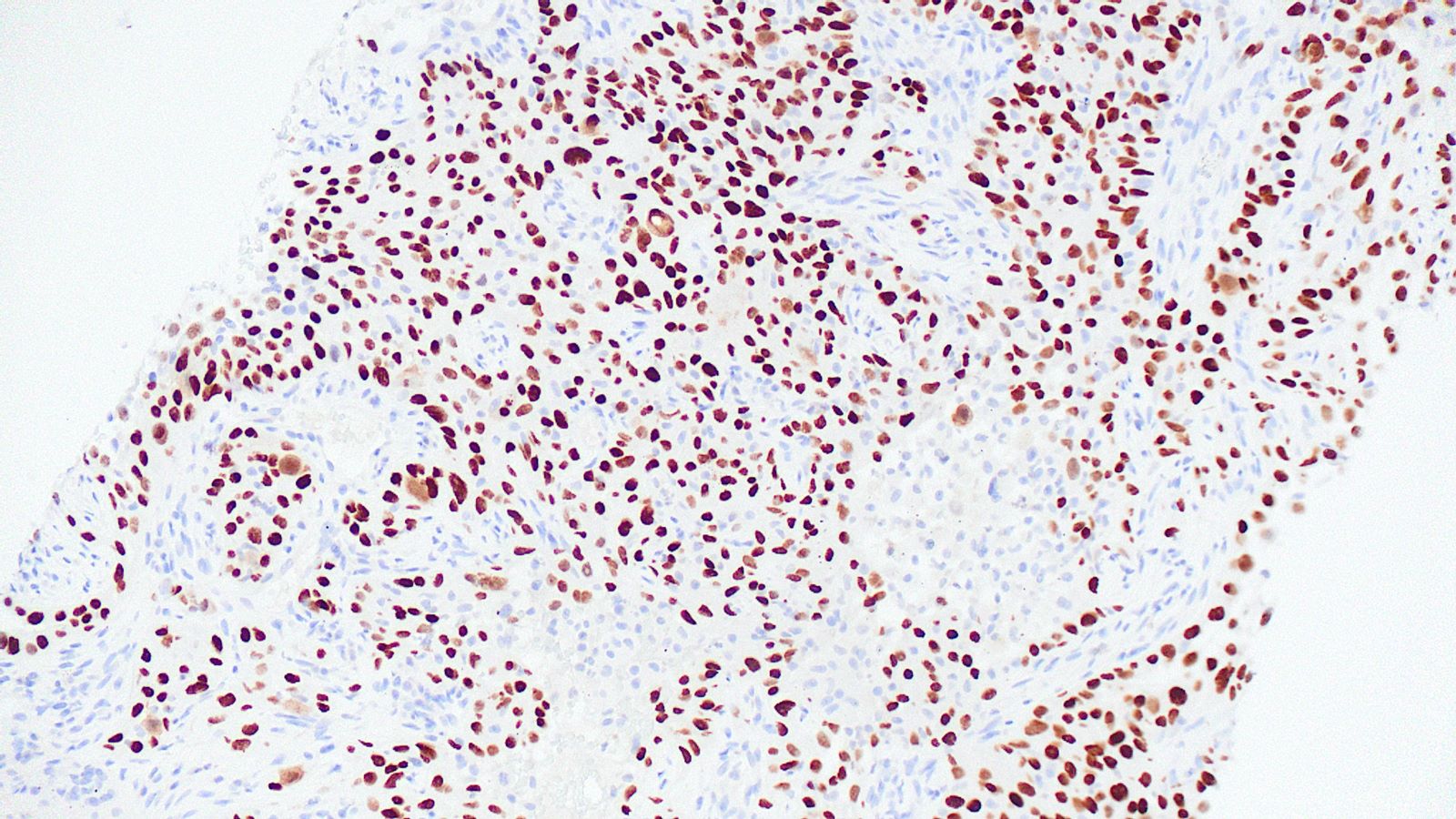
p40
Positive stains
- Adenocarcinoma: TTF1, napsin A, mucicarmine
- Squamous cell carcinoma: p40, CK5/6, p63 (less specific)
- Neuroendocrine tumors: keratins, TTF1 (~50% depending on location), synaptophysin, chromogranin, CD56
- Small cell carcinoma: pancytokeratin, TTF1 (~80%), neuroendocrine markers may be absent, Ki67 useful in crushed / distorted biopsies
Molecular / cytogenetics description
- CAP / IASLC / AMP guidelines for molecular testing of lung cancer (Arch Pathol Lab Med 2018;142:321):
- EGFR, ALK and ROS1 are “must test†genes
- BRAF, MET, ERBB2 (HER2) and RET are recommended for patients suitable for clinical trials
- KRAS sequencing may be helpful to exclude KRAS mutant patients from extended panel testing
- While these recommendations are primarily regarding pulmonary adenocarcinoma, physicians may utilize molecular testing in nonadenocarcinomatous tumors when there are clinical features that may indicate the presence of an oncogenic driver
Sample pathology report
- Right lung, upper lobe, transbronchial biopsies:
- Non-small cell carcinoma, favor adenocarcinoma (see comment)
- Comment: The tumor cells lack morphologic evidence of squamous or glandular differentiation. Immunohistochemical studies performed with appropriate controls reveal the tumor cells are positive for TTF1 and negative for p40. The results support the rendered diagnosis and favor adenocarcinoma of lung origin.
Additional references
Board review style question #1
Transbronchial biopsy of a PET avid lung mass reveals a solid proliferation of malignant epithelial cells lacking obvious keratinization and glandular morphology. The tumor cells show variable p40 reactivity and are negative for both TTF1 and mucicarmine. What is the best designation for this tumor?
- Non-small cell carcinoma, favor adenocarcinoma
- Non-small cell carcinoma, favor squamous cell carcinoma
- Non-small cell carcinoma, not otherwise specified
- Squamous cell carcinoma
- Squamous cell carcinoma, nonkeratinizing
Board review style answer #1
B. Non-small cell carcinoma, favor squamous cell carcinoma. A poorly differentiated malignancy without morphologic evidence of keratinization / squamous differentiation or glandular / adenocarcinomatous differentiation requires judicious use of immunostains for further classification. A basic panel of TTF1 and p40 is sufficient to classify most lung tumors. Addition of mucicarmine is useful in occasional cases of TTF1 negative adenocarcinomas. Such undifferentiated tumors, in small biopsies, are primarily classified as non-small cell carcinoma with further classifications being favored based on the results of ancillary studies. Given the variable positivity for p40 and negative TTF1 and mucicarmine results, the best classification would be non-small cell carcinoma, favor squamous cell carcinoma.
Comment Here
Reference: Lung - Biopsies
Comment Here
Reference: Lung - Biopsies
Board review style question #2
Transbronchial biopsy of a PET avid lung mass reveals a solid proliferation of malignant epithelioid cells lacking obvious keratinization and glandular morphology. The tumor cells show no reactivity with TTF1, p40 or mucicarmine. The clinical radiologic features support a primary lung malignancy. What is the best designation for this tumor?
- Adenocarcinoma, solid pattern
- Non-small cell carcinoma, favor adenocarcinoma
- Non-small cell carcinoma, favor large cell carcinoma
- Non-small cell carcinoma, not otherwise specified
- Squamous cell carcinoma, nonkeratinizing
Board review style answer #2
D. Non-small cell carcinoma, not otherwise specified. A poorly differentiated malignancy without morphologic evidence of keratinization / squamous differentiation or glandular / adenocarcinomatous differentiation requires judicious use of immunostains for further classification. A basic panel of TTF1 and p40 is sufficient to classify most lung tumors. Addition of mucicarmine may be useful for occasional cases of TTF1 negative adenocarcinomas. Such undifferentiated tumors, in small biopsies, are primarily classified as non-small cell carcinoma with further classifications being favored based on the results of ancillary studies. In this case, there is no reactivity with ancillary studies to allow further designation. The absence of reactivity with ancillary studies could reflect a diagnosis of large cell carcinoma but could also represent sampling of an undifferentiated portion of an otherwise poorly differentiated squamous cell carcinoma or adenocarcinoma. The diagnosis of large cell carcinoma requires a resection specimen and thorough sampling to ensure that a differentiated component is not missed.
Comment Here
Reference: Lung - Biopsies
Comment Here
Reference: Lung - Biopsies
Board review style question #3

A 75 year old man with a 100 pack year smoking history presents with hemoptysis and is found to have a hilar mass and lymphadenopathy. Biopsy of one of the lymph nodes reveals the proliferation seen in the above images. Mitotic activity is approximately 35 mitoses per 2 mm2 and necrosis is present. Immunophenotyping is attempted; however, the block was inadvertently exhausted and stains are not available. What is the best diagnosis that can be rendered?
- Atypical carcinoid tumor
- Carcinoid tumor, not otherwise specified
- Epithelial neoplasm, not further classifiable
- No diagnosis can be rendered, rebiopsy is needed
- Small cell carcinoma
Board review style answer #3
E. Small cell carcinoma. Small cell carcinoma remains a morphologic diagnosis and does not require immunophenotyping for confirmation. The clinical history and description of the malignant cells are consistent with a diagnosis of small cell carcinoma. Immunophenotyping, including the use of Ki67, is most useful in cases with more ambiguous morphologic features or in crushed biopsies where morphologic features are obscured.
Comment Here
Reference: Lung - Biopsies
Comment Here
Reference: Lung - Biopsies
