Lung
Squamous cell carcinoma
Squamous cell carcinoma
Authors: Alex McGeough, M.D., Divya Sharma, M.D.
Editorial Board Member: Matthew J. Cecchini, M.D., Ph.D.


Last author update: 8 August 2023
Last staff update: 20 September 2024
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Squamous cell carcinoma lung
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2 | Practice question #3 | Practice answer #3Cite this page: McGeough A, Sharma D. Squamous cell carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumorscc.html. Accessed September 15th, 2025.
Definition / general
- Malignant tumor arising from epithelial cells with squamous differentiation demonstrated either immunohistochemically or morphologically, with the presence of keratinization or intercellular bridges
- Can be keratinizing or nonkeratinizing and subtypes include solid, cystic, papillary, pseudoglandular, alveolar filling and sarcomatoid / spindle cell change
Essential features
- Morphologically identified with keratinization, keratin pearls and intercellular bridges
- Poorly differentiated lesions may lose morphologic features of squamous differentiation and require IHC to separate from other non-small lesions, p40 positivity will help
- Primary and metastatic tumors have an overlapping morphology and immunohistochemical profiles; in most cases it is not possible to determine the primary site of squamous cell carcinoma
Terminology
- Epidermoid carcinoma: historical and no longer recommended
ICD coding
Epidemiology
- Strong association with history of tobacco smoking (80% of men and 90% of women) (Thorax 1973;28:354)
- Primarily in patients over 50 years of age
- 85% of primary lung cancers are non-small cell carcinomas and squamous cell makes up 30% of these cases (Clin Cancer Res 2012;18:2443)
Sites
- Can present in any site of the lungs or bronchus but is more commonly central
- Metastasis is frequently observed (Ann Oncol 2018;29:iv192)
- Mediastinal lymph nodes are the primary site
- Hematogenous spread to distant organs
- Bone is the most common
- Liver is the second most common
Pathophysiology
- Squamous cells lining the respiratory tract transformed from carcinogen exposure, most frequently smoking
- Occupational heavy metal exposure has also been reported (Int Arch Occup Environ Health 2009;82:867)
- Extrapulmonary squamous cell carcinoma is also possible
Etiology
- See Pathophysiology
Clinical features
- Wide range of nonspecific pulmonary symptoms reported including cough, chest pain, shortness of breath, hemoptysis, wheezing, weight loss, recurrent infections, loss of appetite and fatigue (StatPearls: Squamous Cell Lung Cancer [Accessed 31 May 2023])
- If the mass compresses the recurrent laryngeal nerve it may also present with hoarseness
Diagnosis
- Can be made on biopsy or cytology specimen, though a lack of keratinization or in poorly differentiated cases immunohistochemical testing may be required (Thorax 2016;71:177)
Laboratory
- Humoral hypercalcemia of malignancy secondary to paraneoplastic syndrome is seen in up to 10% of cases and is associated with a poor prognosis (World J Clin Oncol 2014;5:197)
Radiology description
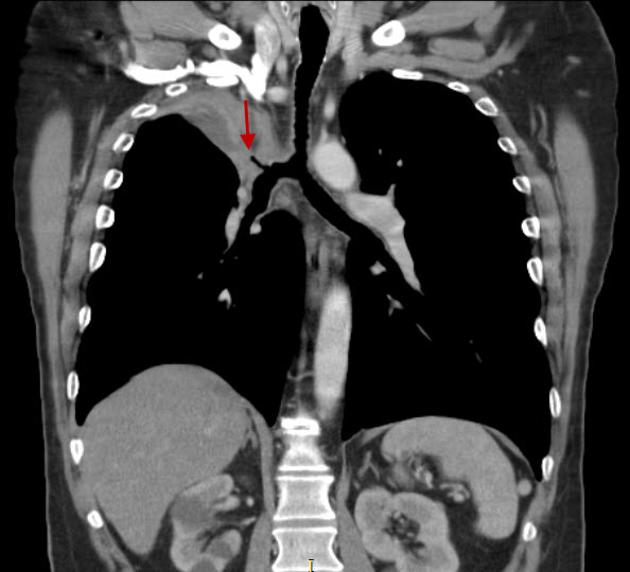
- CT is the imaging of choice for lung cancer evaluation and demonstrates a nonspecific mass with irregular borders, often with central cavitation
- Centrally located tumors are more common and often cause obstruction with associated pneumonitis or lung collapse
- Squamous cell carcinoma cannot be distinguished definitively from radiological findings as other lesions may have the same radiologic appearance
- Reference: Radiopaedia: Squamous Cell Carcinoma of the Lung [Accessed 31 May 2023]
Radiology images
Images hosted on other servers:

Central mass with cavitation
Peripheral mass with collapse
Prognostic factors
- Stage at time of diagnosis is the best predictor of prognosis
Case reports
- 52 year old woman with lung cancer responding to alectinib (BMC Cancer 2017;17:471)
- 56 year old man with primary lung cancer and metastasis to tongue (Medicine (Baltimore) 2017;96:e8208)
- 60 year nonsmoking woman with lung cancer treated with osimertinib (Intern Med 2021;60:1067)
Treatment
- Primary treatment is surgical excision through wedge resection, lobectomy or pneumonectomy (J Natl Compr Canc Netw 2022;20:497)
- Systemic chemotherapy including PDL1 immunotherapy (if applicable) and radiation therapy (Transl Lung Cancer Res 2018;7:S198)
Gross description
- Often cavitary mass with white, smooth cut surfaces that frequently contain hemorrhage and necrosis
- Mass is more often central than peripheral and may be within the bronchus
Gross images
Contributed by @yro854 and @Andrew_Fltv on Twitter
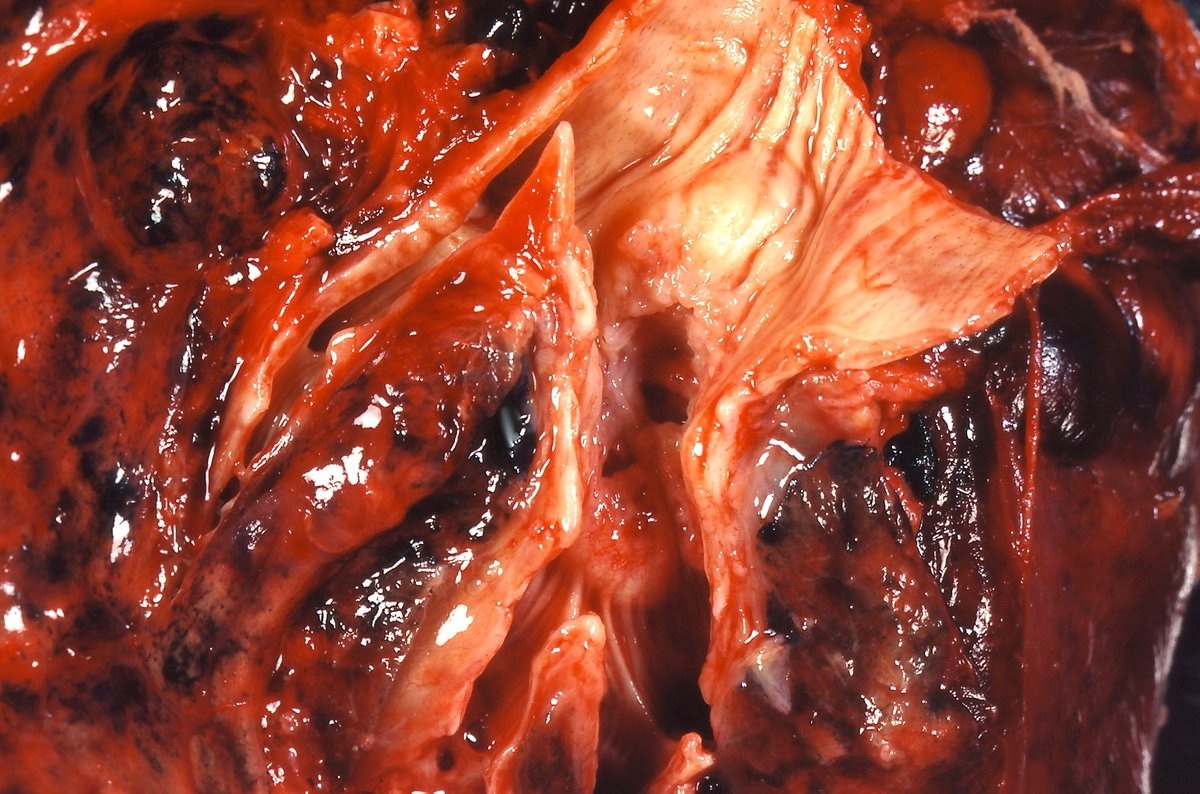
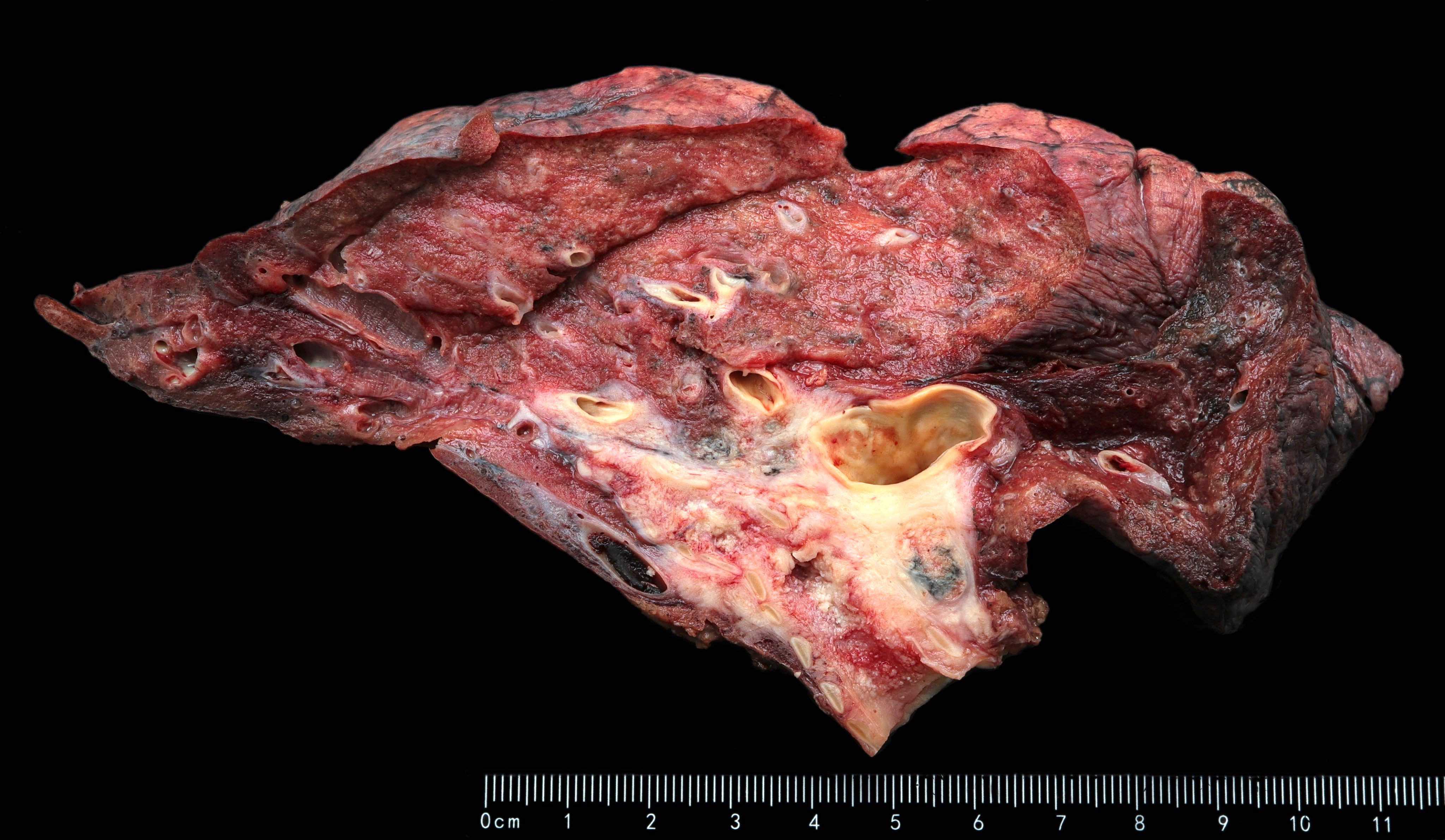
Squamous cell carcinoma
Images hosted on other servers:

Central cavitation

Tumor obstructing bronchus

Tumor extending to pleura
Microscopic (histologic) description
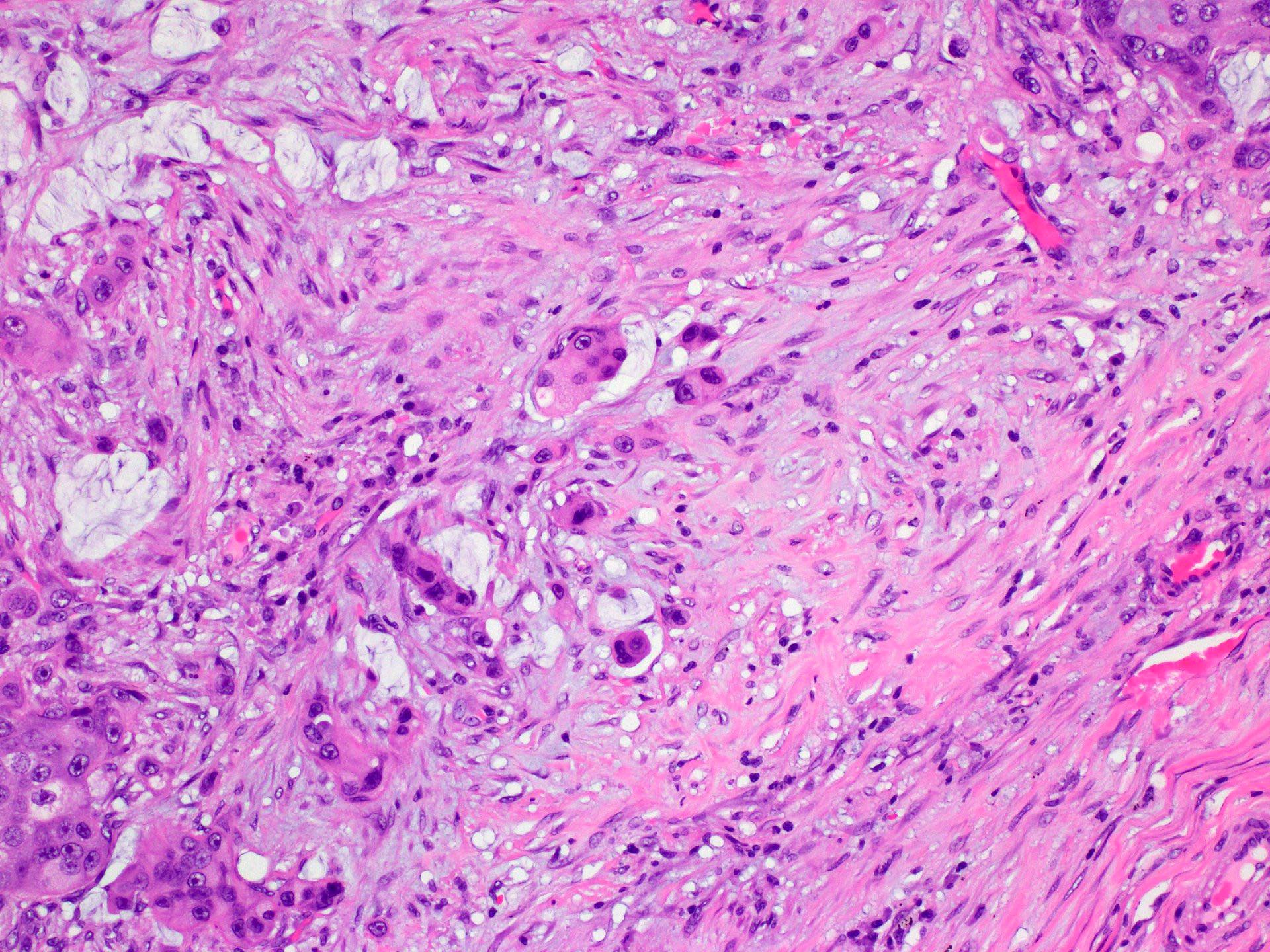
- Presence of keratinization including keratin pearls, intercellular bridging, abundant inflammation and necrosis are all frequent but not required for diagnosis
- There is currently no established grading system for squamous cell carcinoma of the lung and cases and intuitively graded based on the degree of perceived differentiation
- Poorly differentiated squamous cell carcinoma exhibits severe cellular and nuclear atypia, abundant mitosis and often requires IHC studies to differentiate from other poorly differentiated lesions
- Reference: Acad Pathol 2017;4:2374289517705950
Microscopic (histologic) images
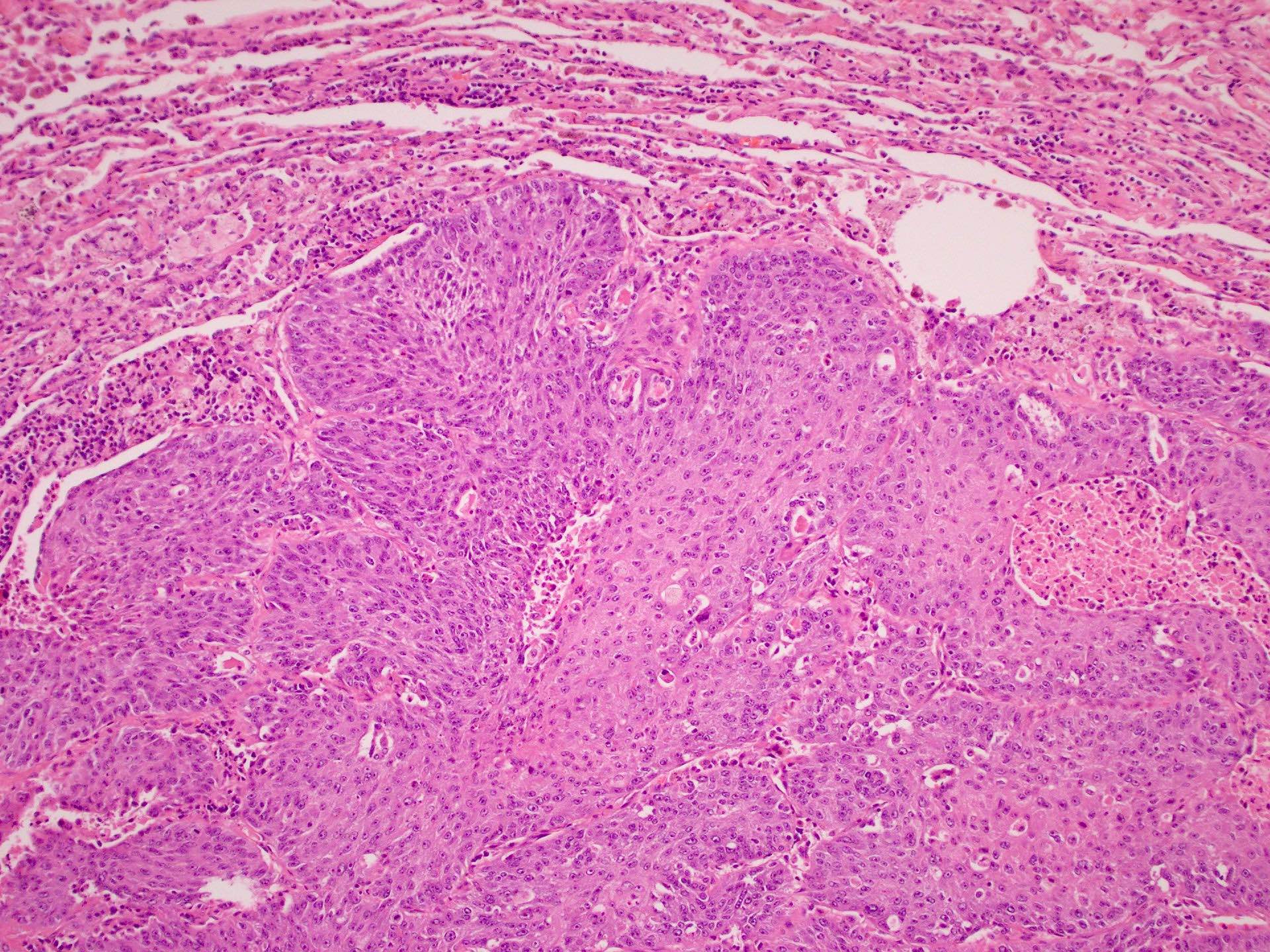
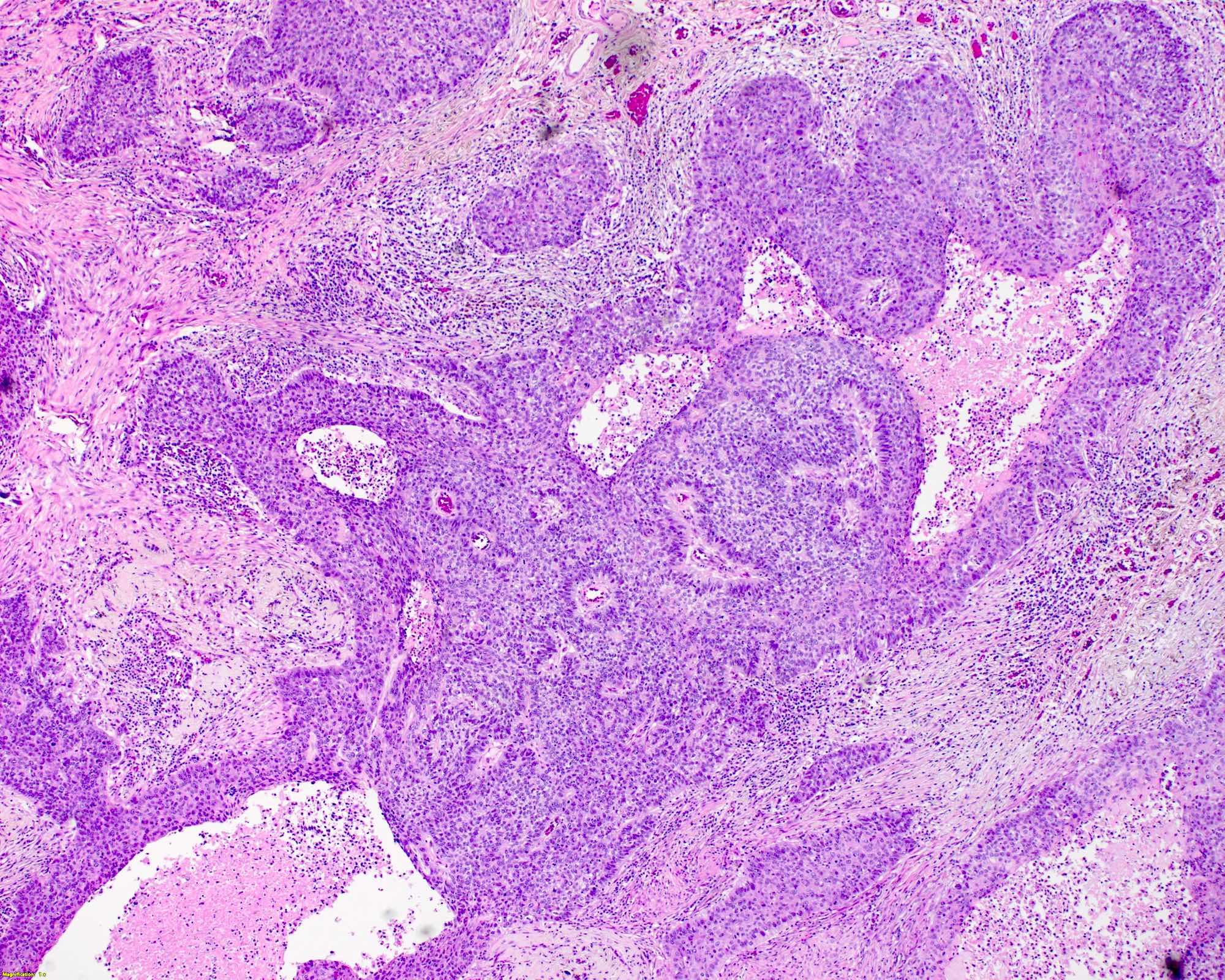
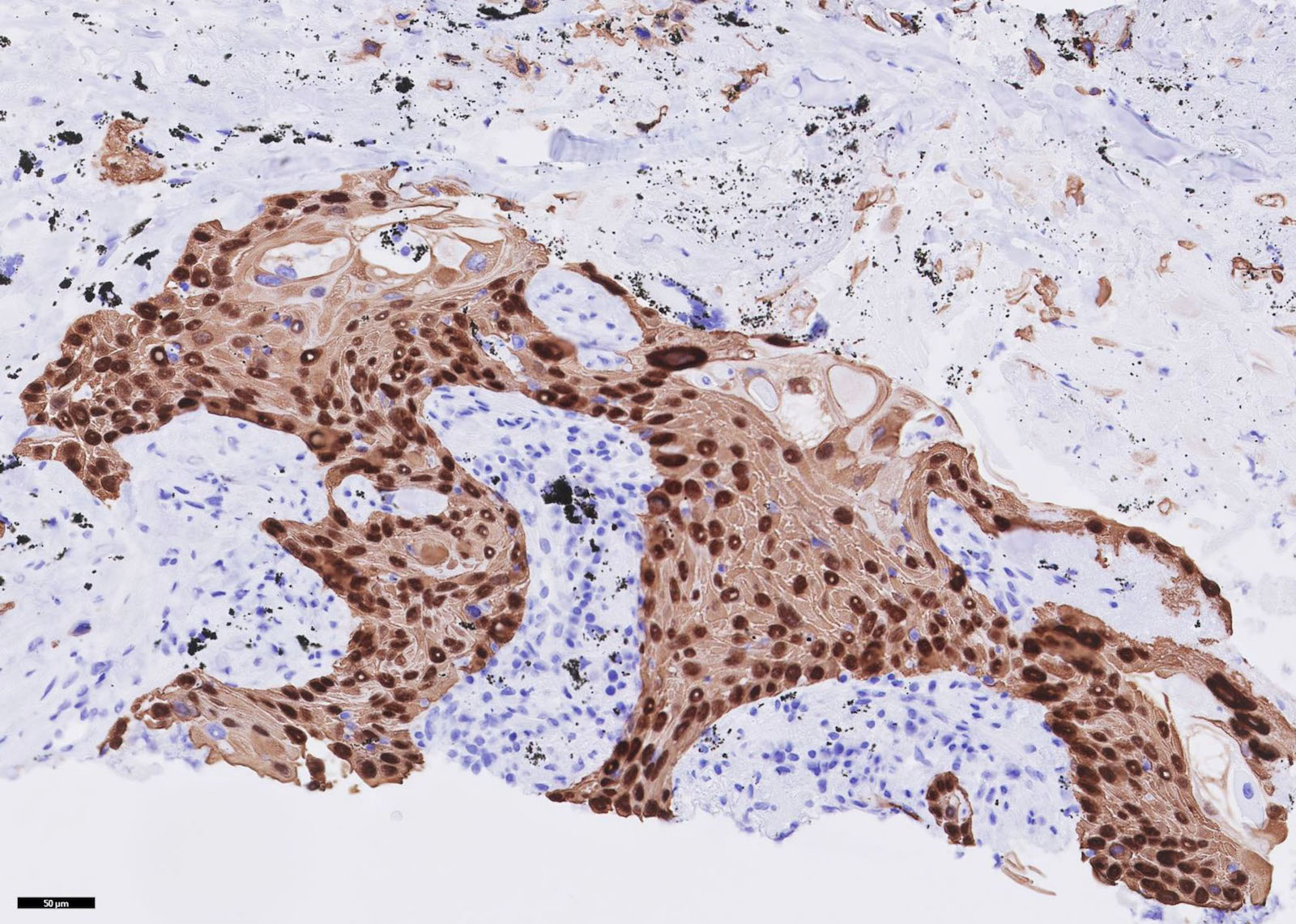
Contributed by Alex McGeough, M.D. and Andrey Bychkov, M.D., Ph.D.
Tumor budding
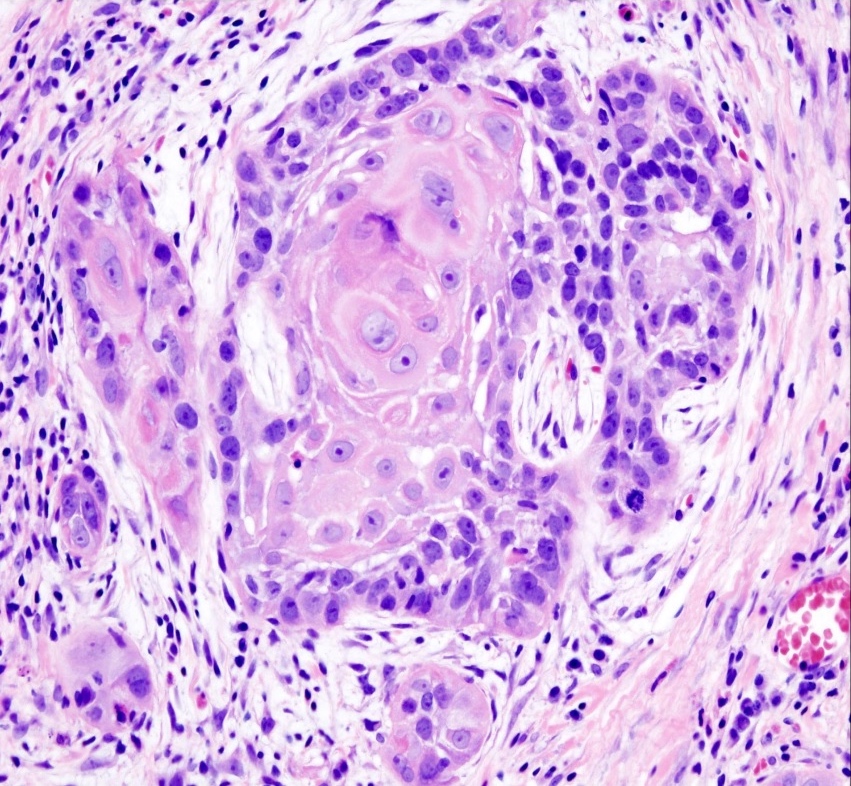
Well differentiated
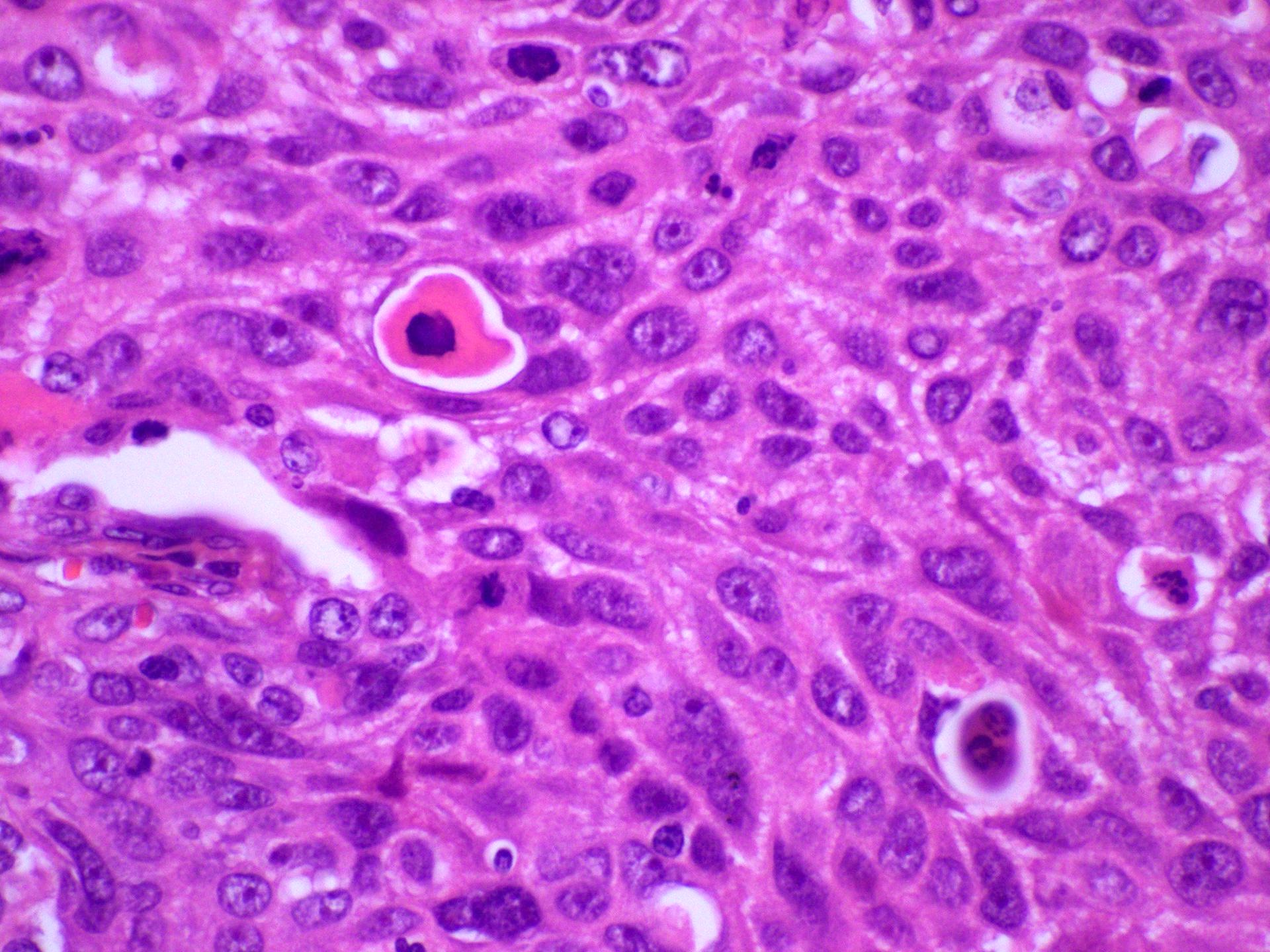
Intercellular bridging
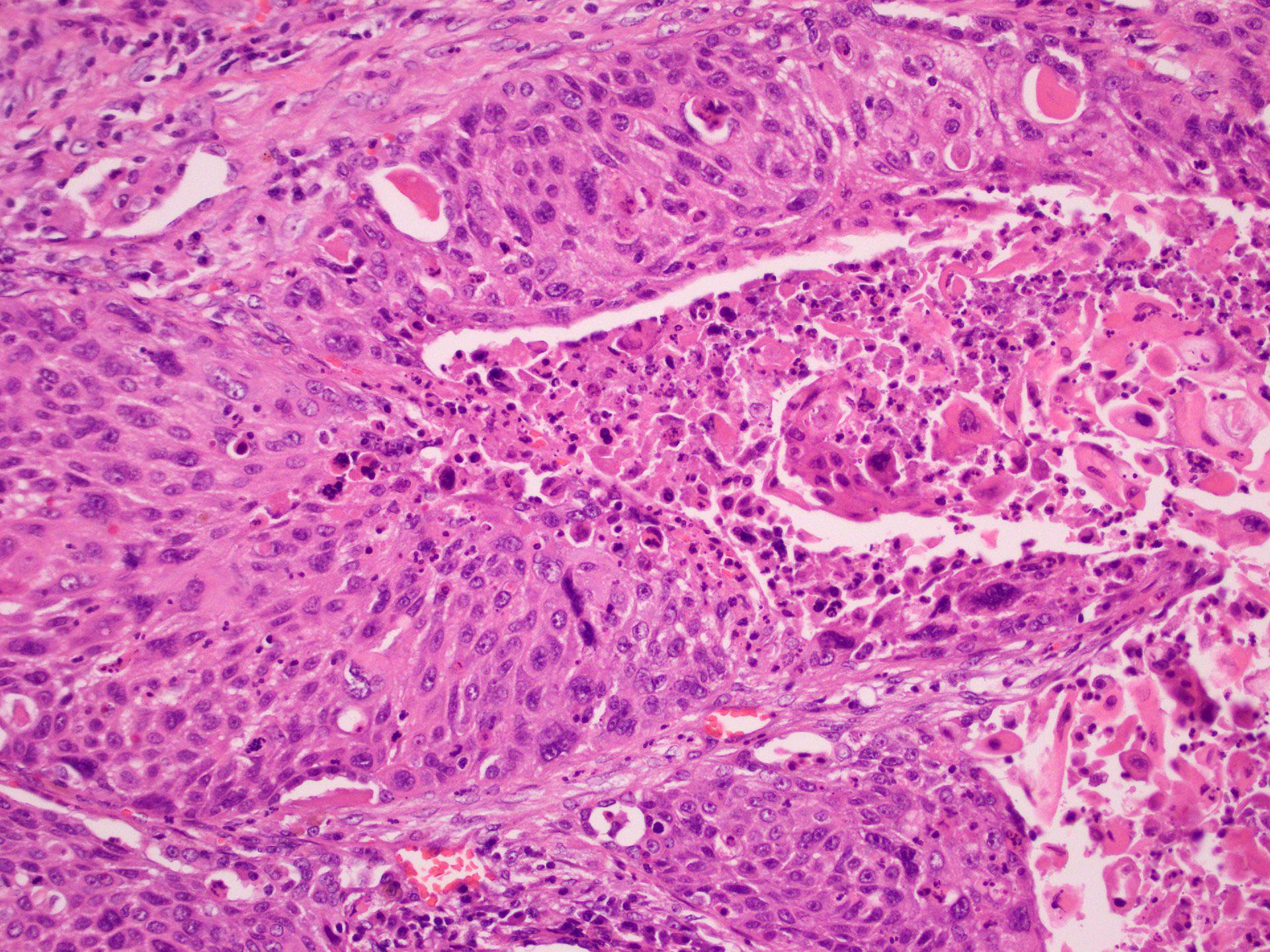
Intratumoral necrosis
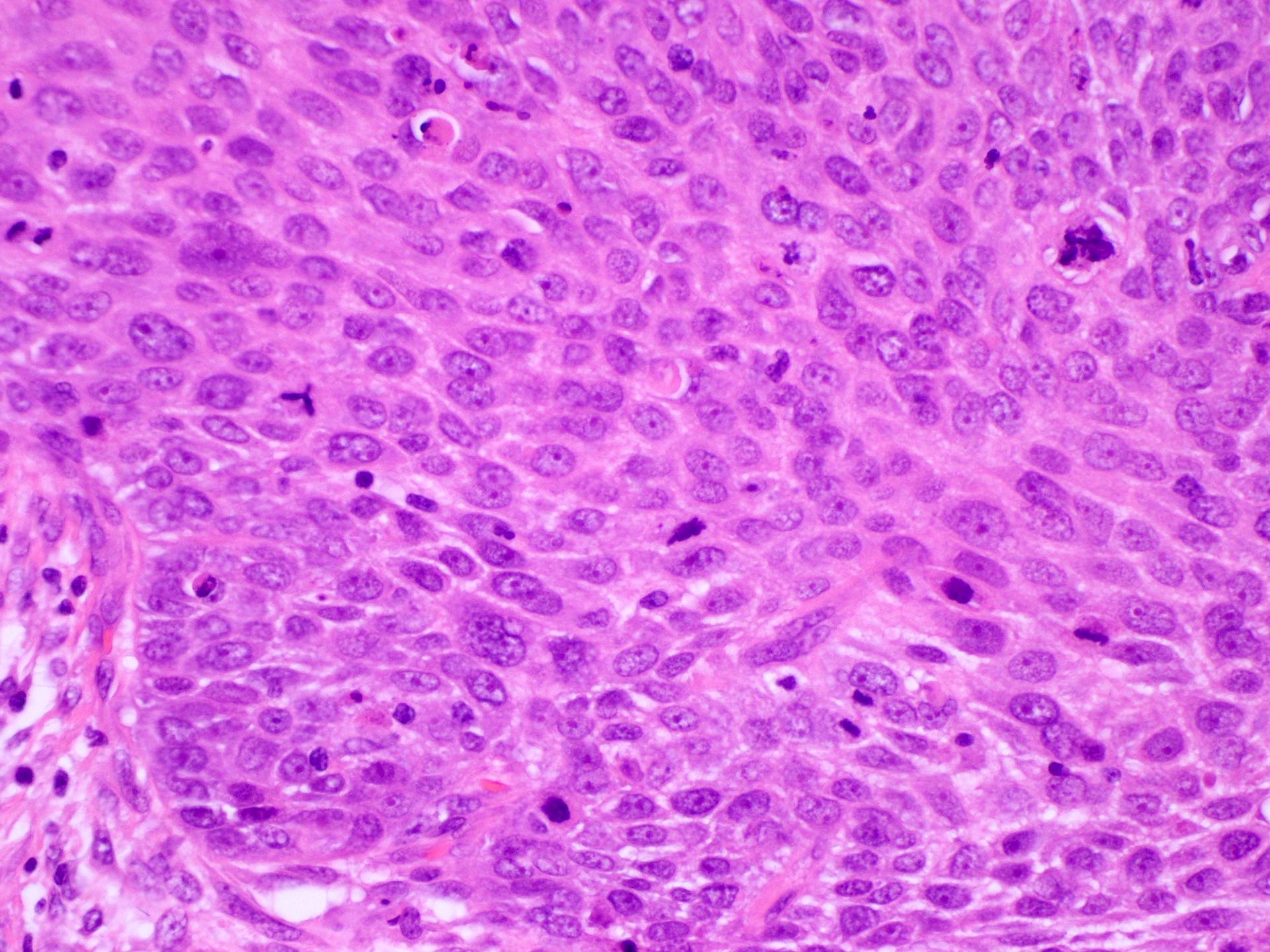
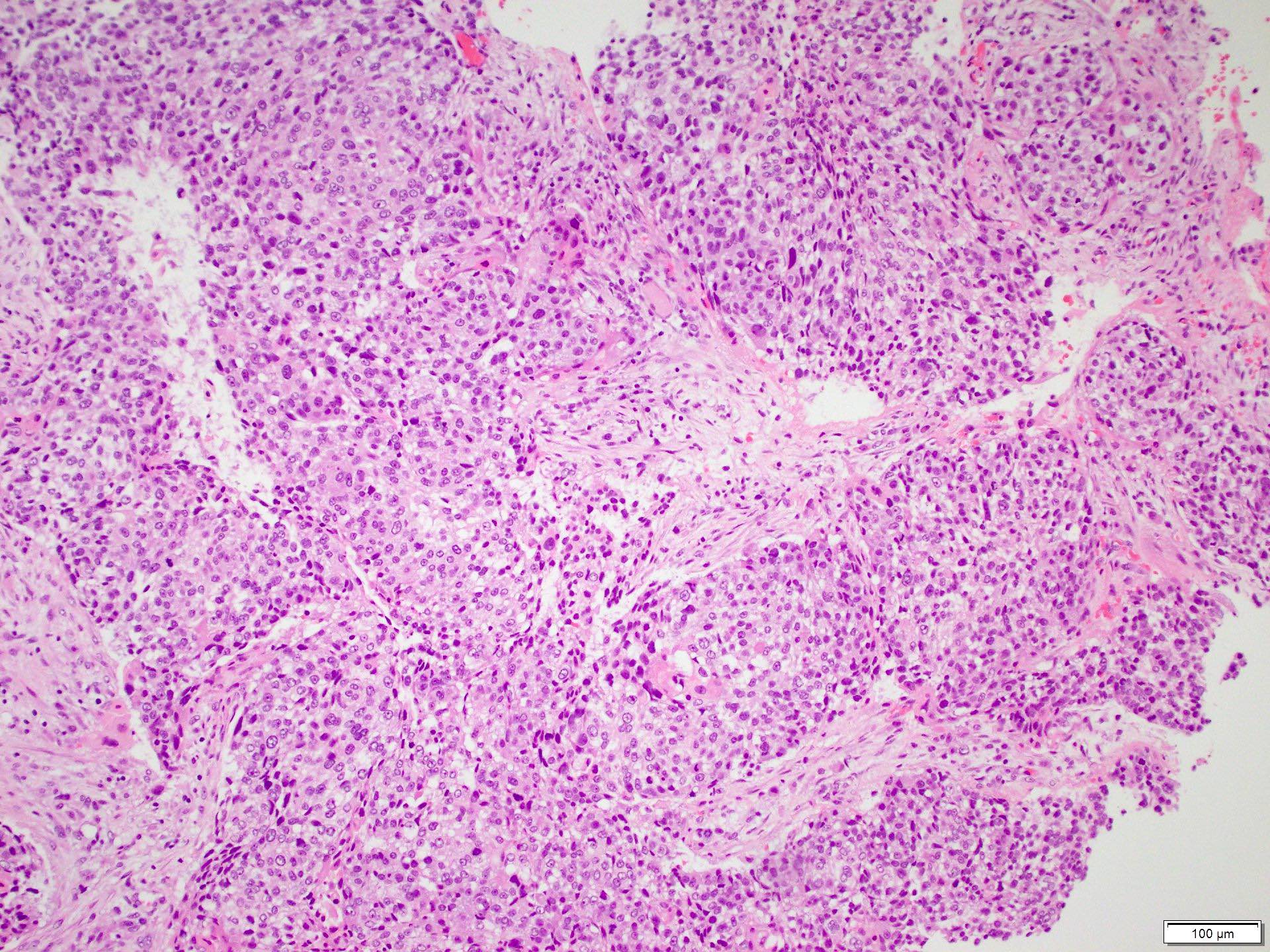
Poorly differentiated
Moderately differentiated
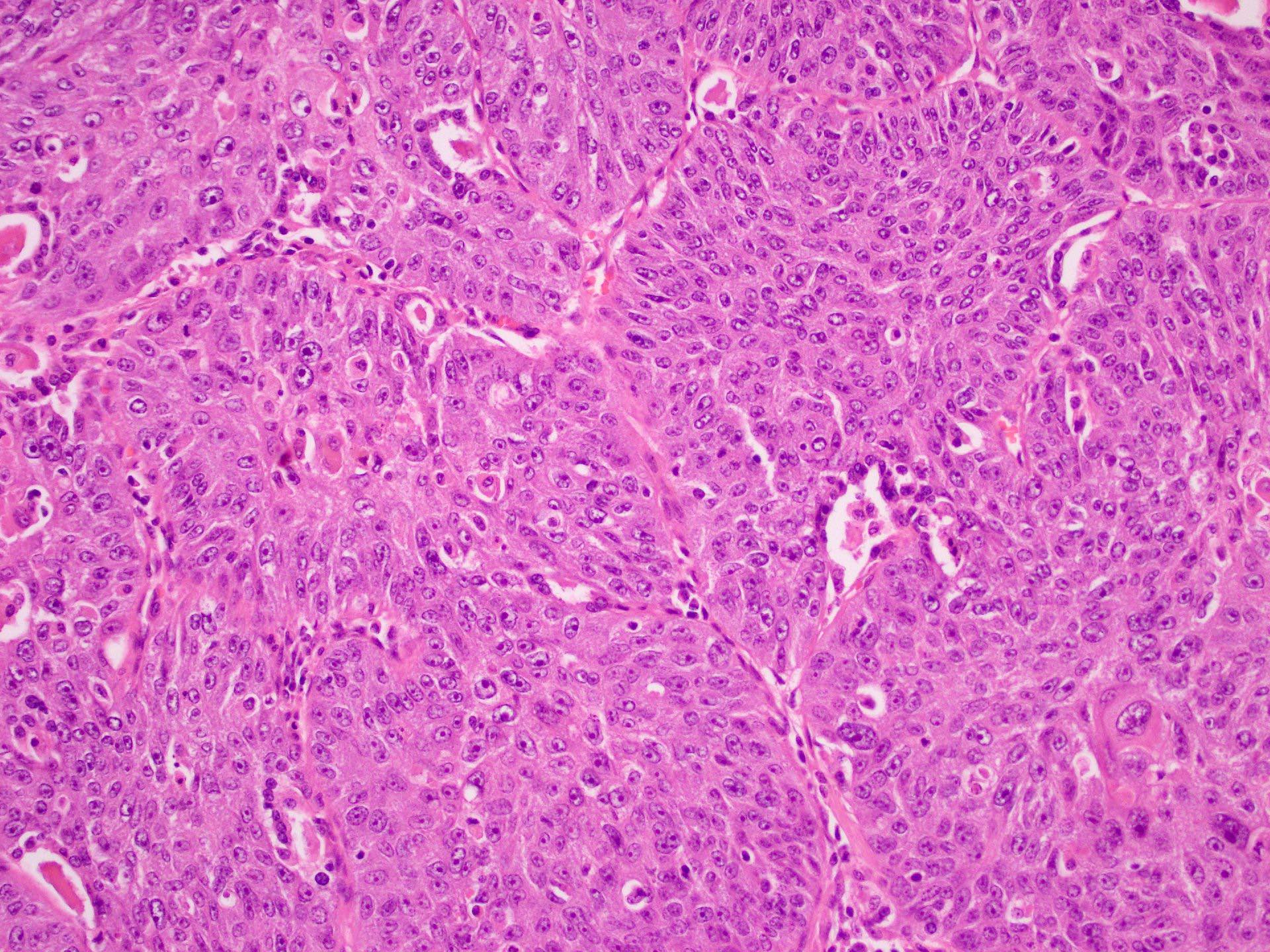
Prominent cytologic atypia
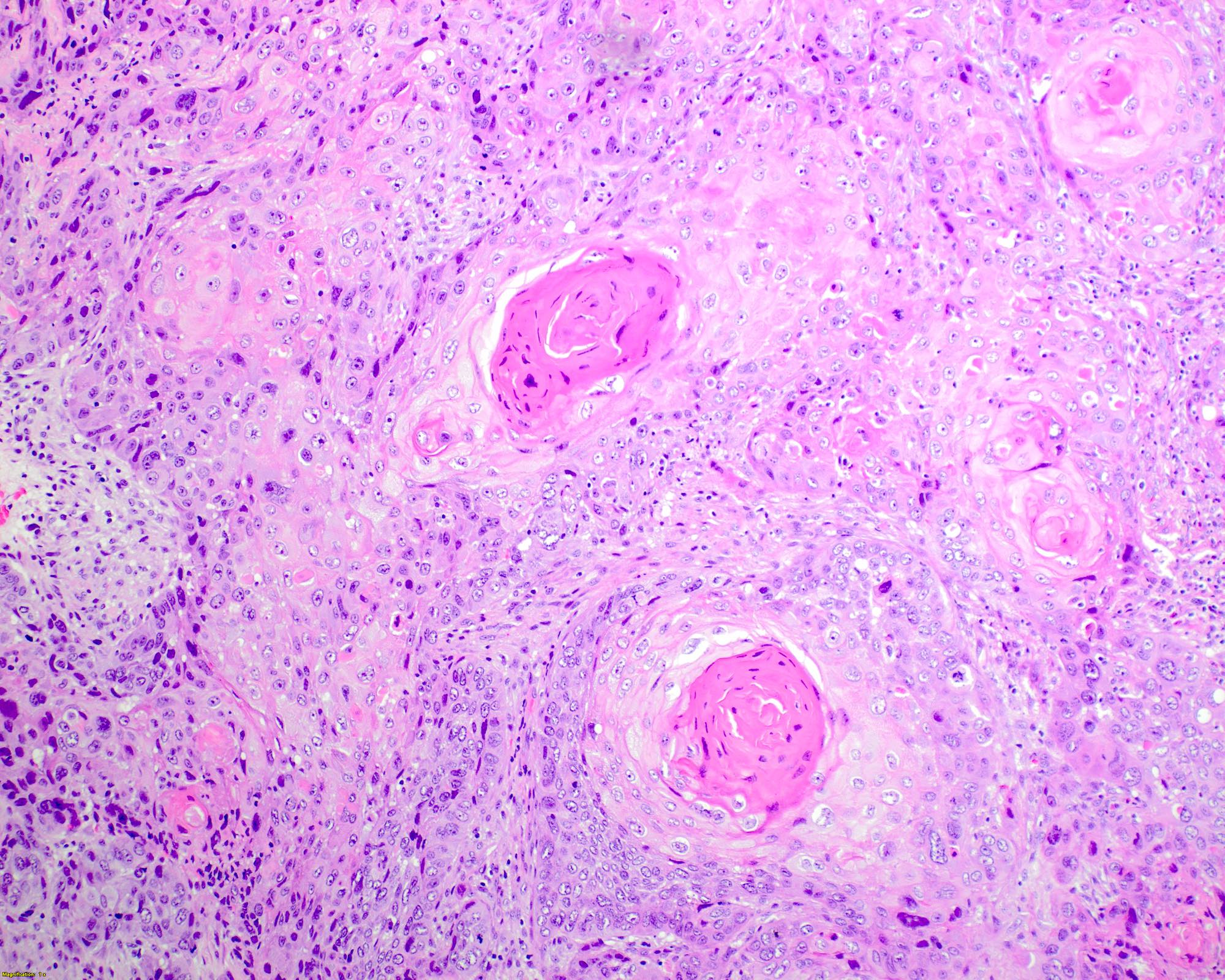
Keratin pearls
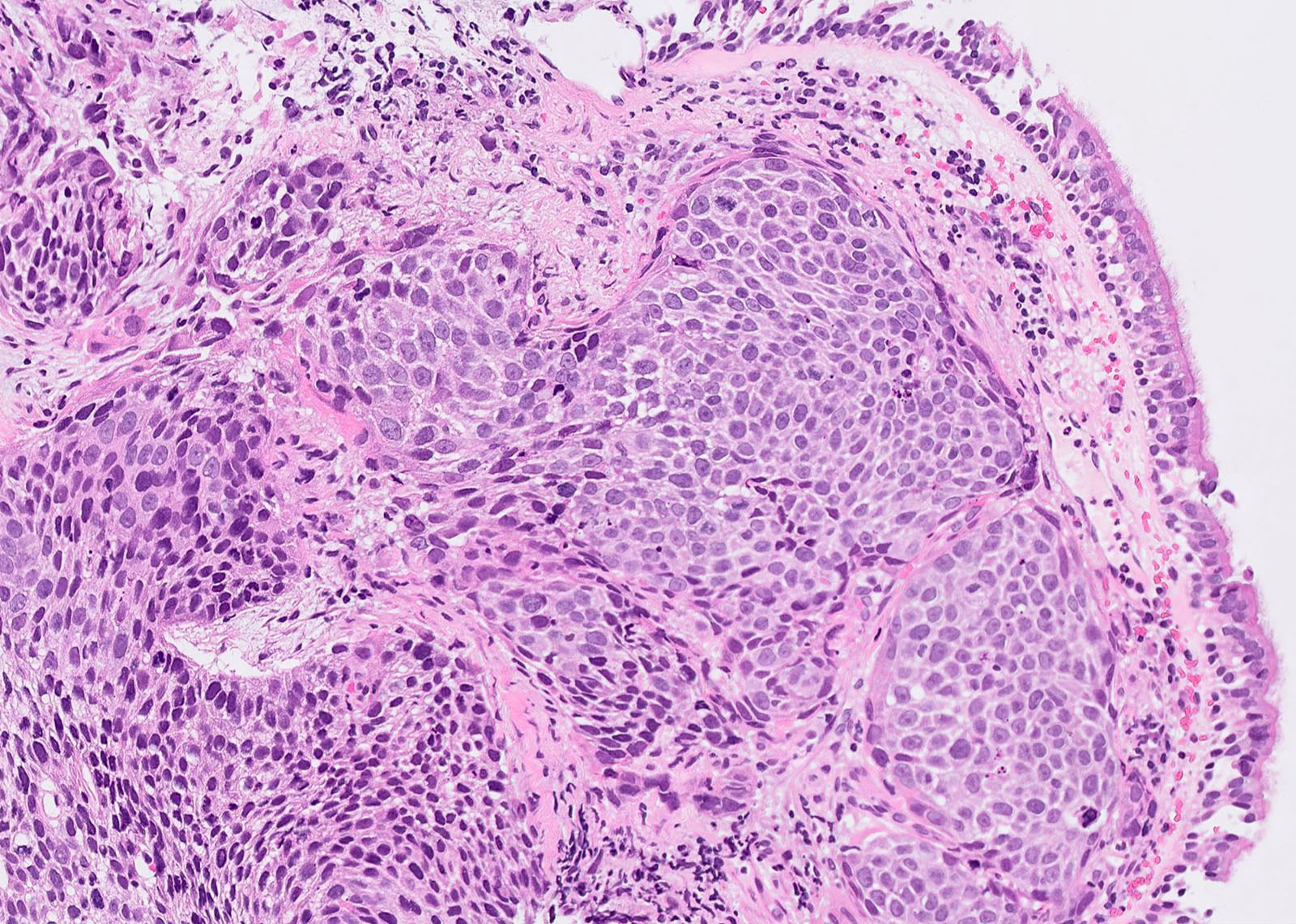
Basaloid type
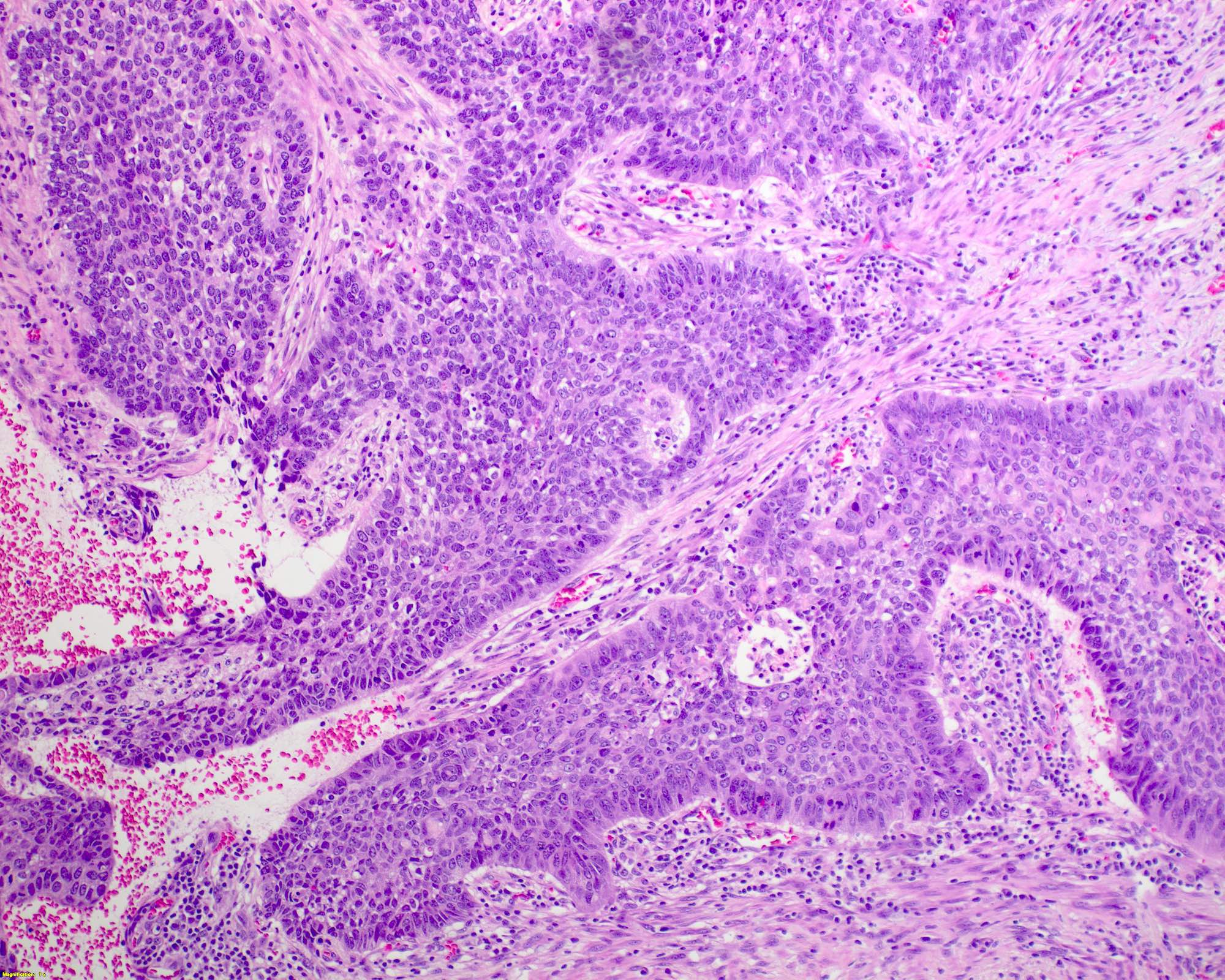
Palisading nuclei in basaloid type
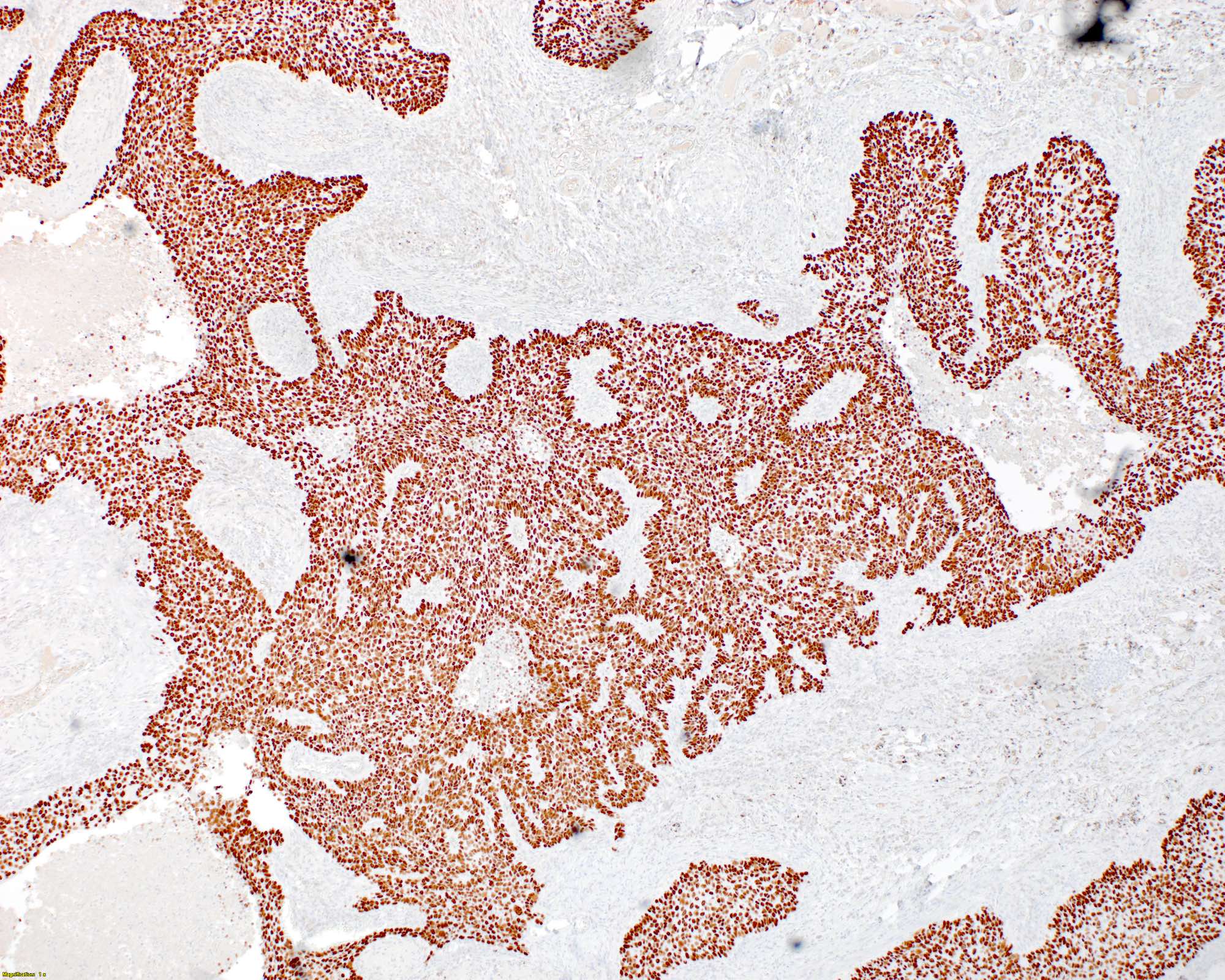
p40 positive in basaloid type
Bronchial biopsy
Nonkeratinizing
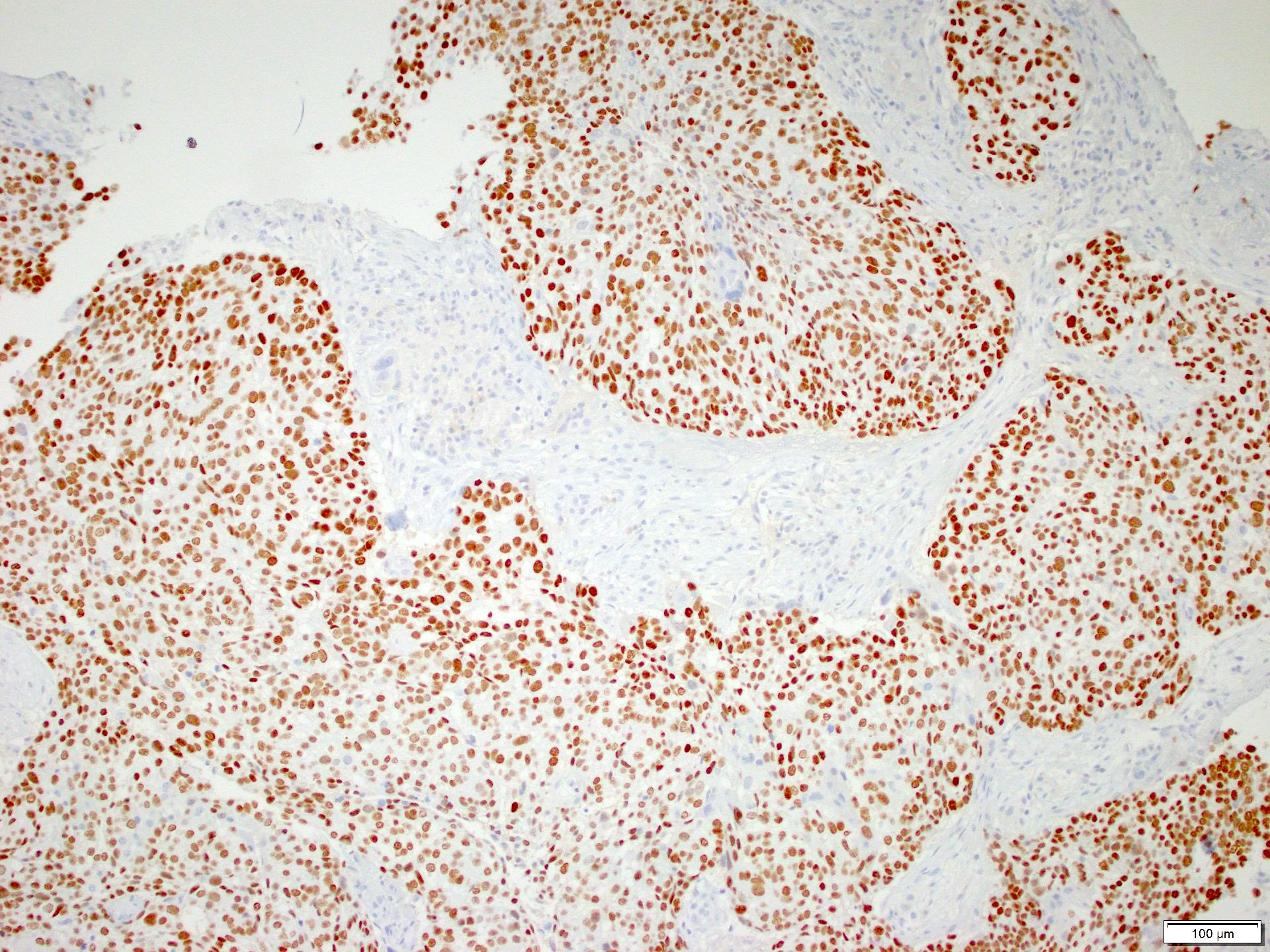
p40 staining
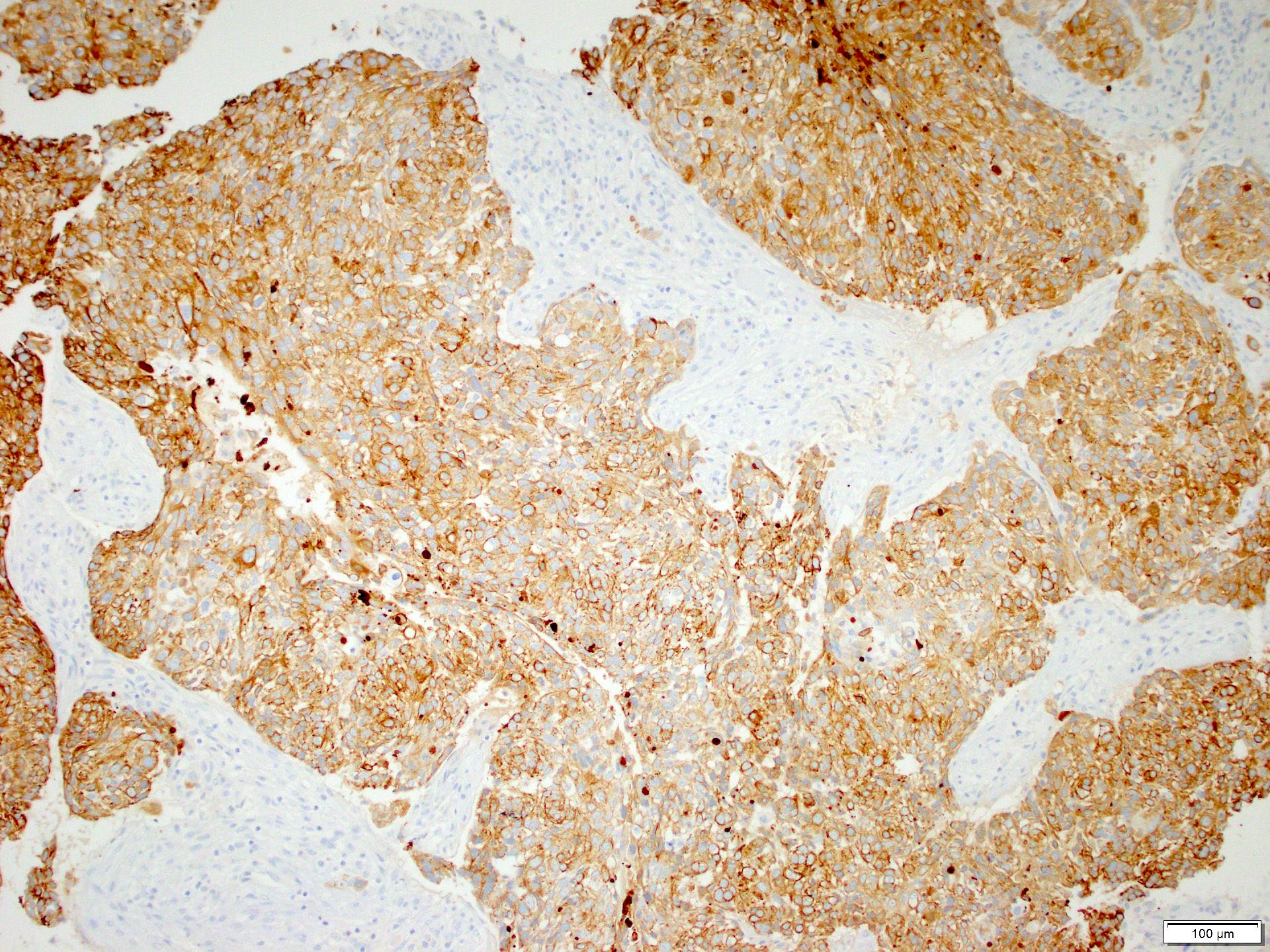
CK 5/6
SCC cocktail
Cytology description
- Atypical cells with keratinization are seen in well differentiated cases
- Higher grade lesions may have similar cytologic appearance to adenocarcinoma and IHC studies can be performed on the cell block to differentiate
- Often demonstrates stretching of the cytoplasm referred to as tadpole cells
- Reference: Int J Clin Exp Pathol 2010;3:367
Cytology images
Images hosted on other servers:

Keratinization and tadpole cell
Positive stains
- p40, p63 are strongly and diffusely positive and are more specific for squamous differentiation; however, p63 is less specific so p40 is preferred
- CK7, high molecular weight keratins, pankeratins and CK5/6 are positive in the majority of cases but will also stain adenocarcinoma (J Pathol 2002;198:100)
- PDL1 expression is variable and is scored using tumor proportion score (Lung Cancer 2017;104:7)
Electron microscopy description
- Abundant tonofilaments, complex desmosomes, basal lamina
Molecular / cytogenetics description
- Abundant molecular alterations are present and testing does not have the prognostic value seen in adenocarcinoma
- Molecular testing for targetable driver mutations is recommended in cases of adenosquamous carcinoma
- EGFR and ALK targetable variants can occur in squamous cell carcinoma; as such, molecular testing may be considered in young or nonsmoking patients
Sample pathology report
- Lung, right upper lobe, wedge resection:
- Invasive, moderately differentiated, keratinizing squamous cell carcinoma (1 cm greatest dimension) (see synoptic report)
- Pathologic tumor stage: pT1a, pN0, pMX
- Margins of resection are free of tumor (4 cm bronchial margin of resection)
Differential diagnosis
- Solid pattern adenocarcinoma:
- High grade small cell carcinoma:
- Usually strongly positive for neuroendocrine markers and may express TTF1
- Also look for precursor lesion
- Melanoma:
- Adenosquamous carcinoma:
- Will have > 10% adenocarcinoma component
- Important to identify as it allows for molecular testing, which may impact prognosis
- NUT carcinoma:
- Positive for NUT IHC or have rearrangements detected by FISH or NGS testing
- Squamous cell metaplasia:
- Arises secondary to lung damage and will not have an associated mass on imaging
- Large cell neuroendocrine carcinoma:
- Mucoepidermoid carcinoma:
- Most often has mucocytes present and lacks keratinization and squamous cell carcinoma in situ
- Lymphoepithelial carcinoma:
- Dense lymphocyte predominant inflammation present
- Not strongly associated with smoking history
- May have positive EBV ISH
- Large cell carcinoma:
- Pleomorphic carcinoma:
- Squamous cell carcinoma elements can be seen admixed with cases of pleomorphic (sarcomatoid carcinoma)
- If there is > 10% spindle or giant cells admixed with squamous cell carcinoma, the WHO recommends classification as a pleomorphic (sarcomatoid) carcinoma
- SMARCA4 deficient undifferentiated tumor
Practice question #1
Practice answer #1
B. Intercellular bridges. Intercellular bridging can be easily appreciated between adjacent tumor cells, which is a defining histologic feature of squamous cell carcinoma. Answers A, C and D are incorrect because these are nonspecific findings and can be seen in other lung lesions.
Comment Here
Reference: Lung - Squamous cell carcinoma
Comment Here
Reference: Lung - Squamous cell carcinoma
Practice question #2
What molecular testing is routinely recommended in squamous cell carcinoma of the lung?
- EGFR
- KRAS
- PDL1
- PTEN
Practice answer #2
C. PDL1. PDL1 is the correct answer as PDL1 expression assessed by the tumor proportion score (TPS) may predict response to immunotherapy. Answers A and B are incorrect because EGFR and KRAS are only routinely recommended in lung adenocarcinoma. Answer D is incorrect because PTEN is associated with colorectal cancer and thyroid cancer.
Comment Here
Reference: Lung - Squamous cell carcinoma
Comment Here
Reference: Lung - Squamous cell carcinoma
Practice question #3
The above tumor is found in the lung. Which stain will allow differentiation between basaloid squamous cell carcinoma and other basaloid neoplasms?
- CK5/6
- CK7
- p40
- TTF1
Practice answer #3
C. p40 is the stain of choice for the identification of squamous cell carcinoma and will help demonstrate squamous differentiation. Answers A and B are incorrect because while CK7 and CK5/6 would also both be positive in this lesion, they would not prove squamous differentiation, as they are positive in the majority of lung carcinomas. Answer D is incorrect because TTF1 would support neuroendocrine or adenocarcinoma differentiation instead of squamous.
Comment Here
Reference: Lung - Squamous cell carcinoma
Comment Here
Reference: Lung - Squamous cell carcinoma
