Salivary glands
Primary salivary gland neoplasms
Benign
Oncocytoma
Authors: Jenny Tung Hiong Lee, M.D., Ruta Gupta, M.D.
Editorial Board Member: Marc Pusztaszeri, M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.


Last author update: 21 May 2025
Last staff update: 21 May 2025
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Oncocytoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Lee JTH, Gupta R. Oncocytoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/salivaryglandsoncocytoma.html. Accessed September 17th, 2025.
Definition / general
- Benign tumor of salivary gland origin
- Exclusively or predominantly composed of oncocytes
- Accounts for 1 - 2% of salivary gland neoplasms
Essential features
- Rare, benign salivary gland neoplasm
- Usually unilateral and mostly occurs in parotid
- Tumor is composed exclusively or predominantly of oncocytes
- Cytoplasm is eosinophilic and granular due to the presence of abundant mitochondria within the cytoplasm
- Can be positron emission tomography (PET) avid
- Treated with local excision
Terminology
- Oncocytic adenoma, oxyphilic adenoma
ICD coding
Epidemiology
- Rare; constitutes < 2% of all salivary gland neoplasms (Head Neck Pathol 2024;18:126)
- Age group: 60 - 80 years old
- No sex predilection
Sites
- Most (> 80%) occur in the parotid; ~10% occur in the submandibular gland
- The rest occur in the sublingual gland, minor salivary glands and respiratory tract
Pathophysiology
- Pathogenesis remains unclear; could be neoplastic / hyperplastic or metaplastic growth
- Oncocytoma may arise in the background of multinodular oncocytic hyperplasia
- Eosinophilic granular cytoplasm of oncocytes is due to the presence of increased intracytoplasmic mitochondrial content
- Reference: Ann Maxillofac Surg 2018;8:330
Etiology
- Associated with radiation exposure or radiotherapy
- Smoking
- Older age
- Reference: Head Neck Pathol 2024;18:126
Clinical features
- Usually presents as a unilateral, slow growing, painless and solitary mass
- Rarely bilateral (Cancer Diagn Progn 2024;4:814)
- Rarely presents with obstructive symptoms if occurring in the nasal or respiratory tract
- Rarely occurs in Birt-Hogg-Dubé syndrome (BHD) (Case Rep Radiol 2018;2018:6265175, Head Neck Pathol 2024;18:52)
Diagnosis
- Typically requires histopathologic examination for definitive diagnosis
- Fine needle aspiration cytology along with clinical and radiologic correlation can often suggest the diagnosis
Radiology description
- Ultrasound: sonographic features are nonspecific and include (J Ultrasound 2021;24:241)
- Ovoid mass, usually homogeneously hypoechoic but can be heterogeneous
- Typically well defined, occasionally lobulated
- Vascular
- Computed tomography (CT): often seen as a well defined mass showing homogeneous enhancement (AJNR Am J Neuroradiol 2010;31:1413)
- Magnetic resonance imaging (MRI): appearance can be variable (J Ultrasound 2021;24:241)
- T1: hypointense
- T2: isointense to hypointense
- T1C+: isointense
- PET FDG: high fluorodeoxyglucose (FDG) uptake (due to mitochondrial accumulation) (J Ultrasound 2021;24:241)
Radiology images
Images hosted on other servers:

Ultrasound

CT

MRI

Increased FDG uptake
Prognostic factors
- Favorable prognosis of a benign tumor following removal
- Low risk for local recurrence
- Malignant transformation is extremely rare
- Reference: Head Neck Pathol 2024;18:126
Case reports
- 73 year old man with right parotid swelling for 35 years (J Oral Maxillofac Pathol 2023;27:S41)
- Case series of submandibular gland swelling (J Maxillofac Oral Surg 2023;22:127)
Treatment
- Complete surgical removal is the treatment of choice (Head Neck Pathol 2024;18:126)
Clinical images
Images hosted on other servers:

Extraoral facial asymmetry
Gross description
- Usually tumor presents as well circumscribed, lobulated, reddish brown nodules
- Mean tumor size is 19.8 mm (AJNR Am J Neuroradiol 2010;31:1413)
- Major salivary glands: tumor is usually encapsulated and solid
- Minor salivary glands: tumor is unencapsulated and less well delineated; cystic change may be present
Gross images
Contributed by Jenny Tung Hiong Lee, M.D. and Ruta Gupta, M.D.

Multiple nodules

Well circumscribed nodule
Microscopic (histologic) description
- Generally a well circumscribed nodule; may lack circumscription in the minor salivary glands
- Solid sheets, nested, trabecular or ductular architecture; microcysts and macrocysts are rare
- Exclusively or predominantly composed of oncocytes and separated by thin fibrovascular septae
- Oncocytes are large, polyhedral shaped with distinct cell membranes and abundant granular eosinophilic cytoplasm (Head Neck Pathol 2024;18:126)
- Nuclei are centrally located, round, vesicular with prominent nucleoli
- Absence of significant nuclear pleomorphism, increased mitoses and necrosis
- Absence of infiltrative growth
- Psammoma bodies and tyrosine-like crystals may be present
- Other cell types that may present in limited quantity within the tumor, especially following a fine needle aspiration: mucous cells, squamous cells or sebaceous cells
- Basal cells can be seen at the periphery of the tumor
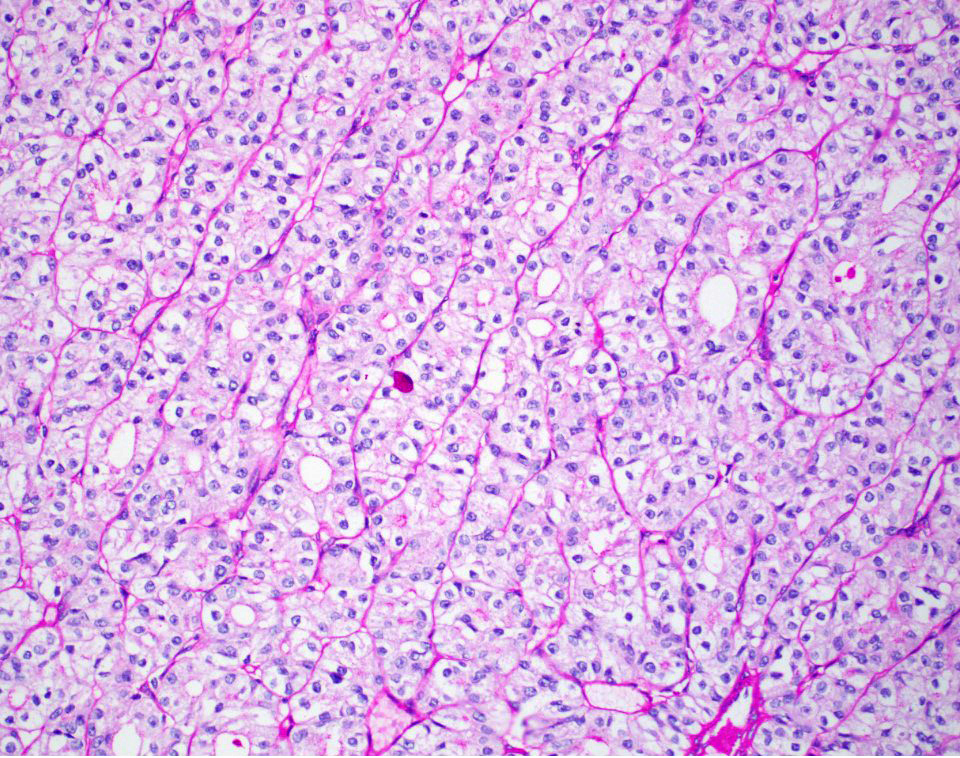
- Clear cell oncocytoma is a histologic variant that consists entirely or predominantly of clear cells
- Reasons for clear cytoplasm
- Fixation and tissue processing artifact
- Accumulated glycogen content that displaces the mitochondria to the periphery of cells
Microscopic (histologic) images
Contributed by Jenny Tung Hiong Lee, M.D. and Ruta Gupta, M.D.
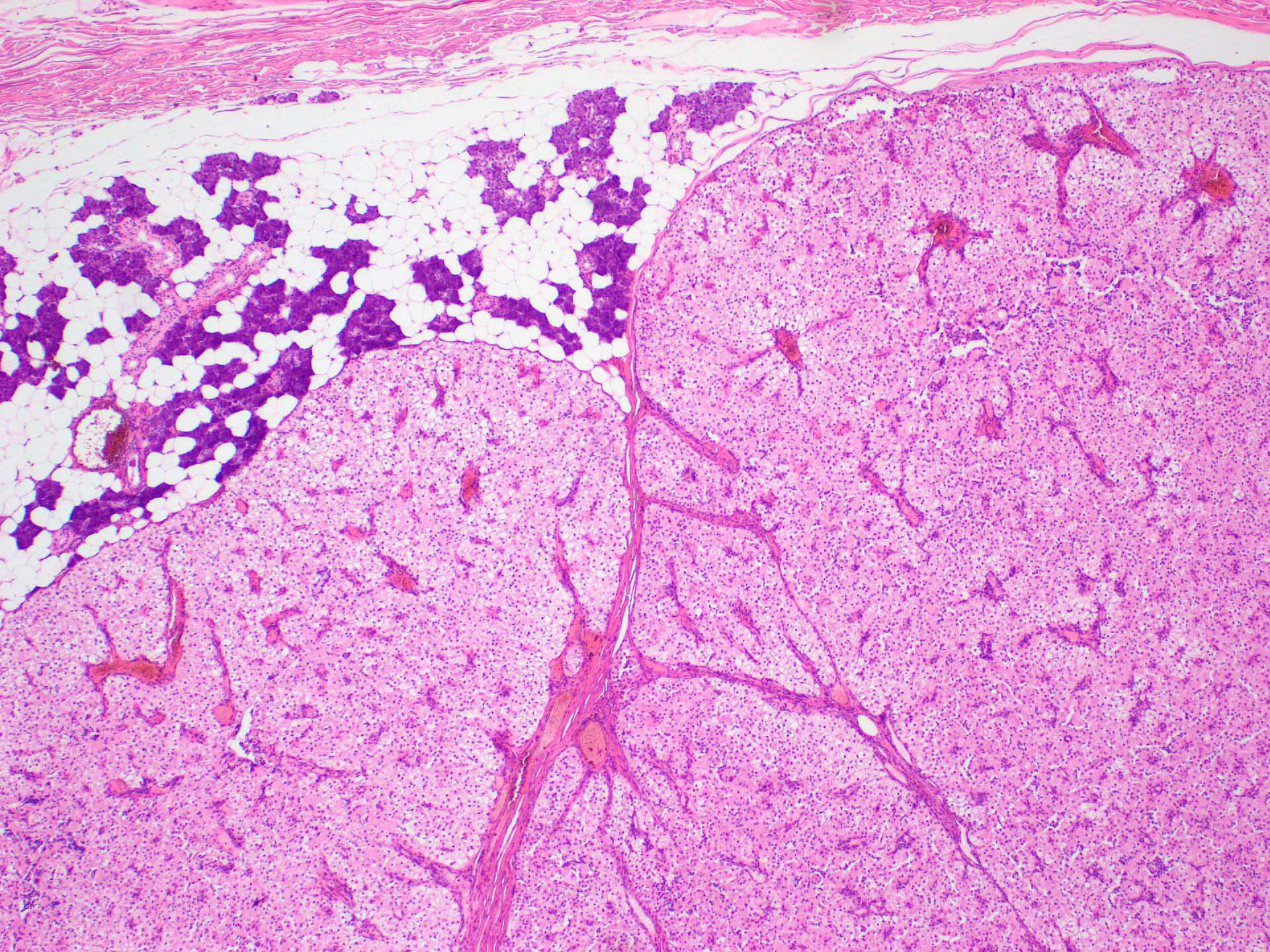
Well circumscribed oncocytic tumor
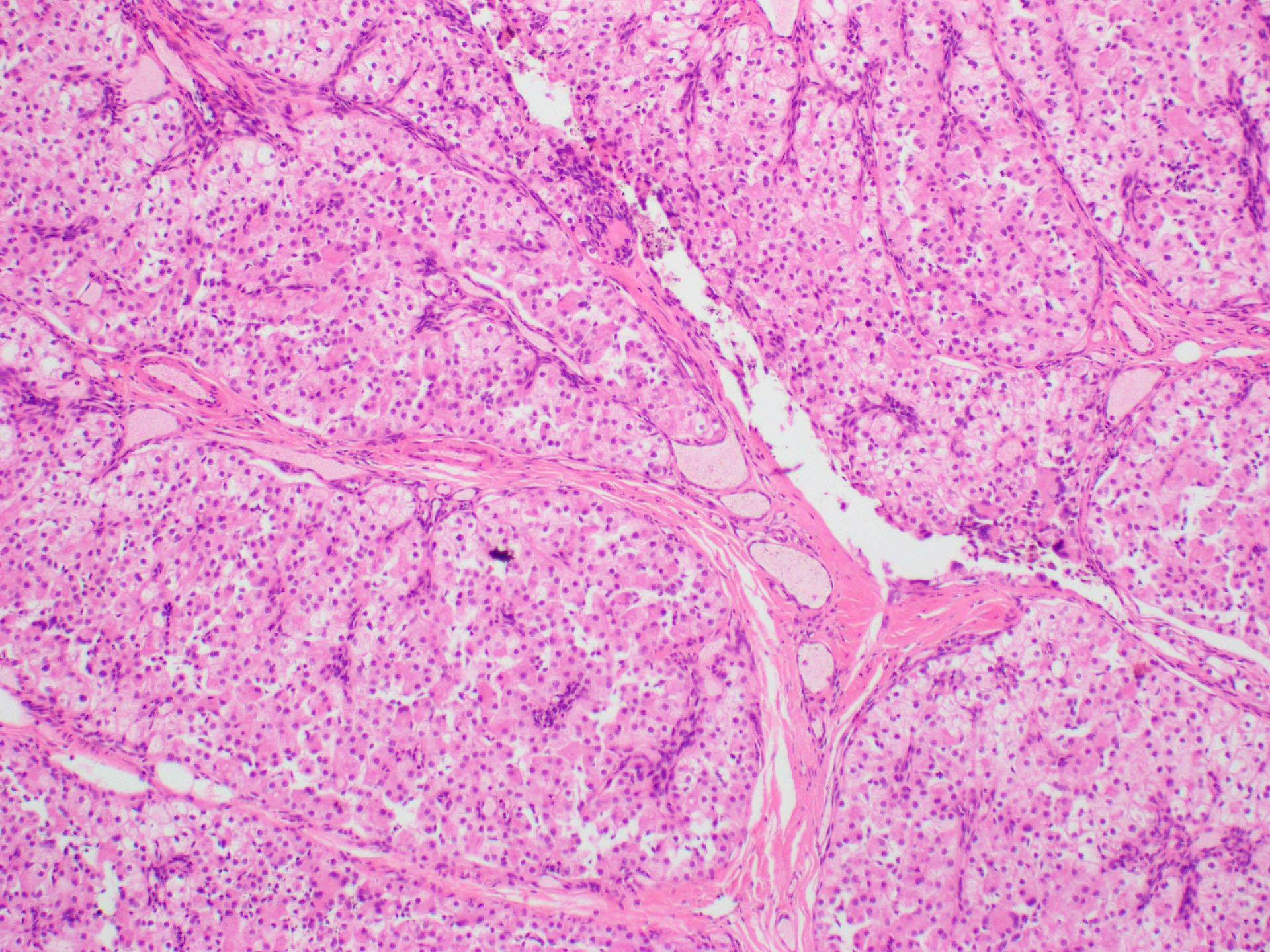
Tumor cells arranged in nests
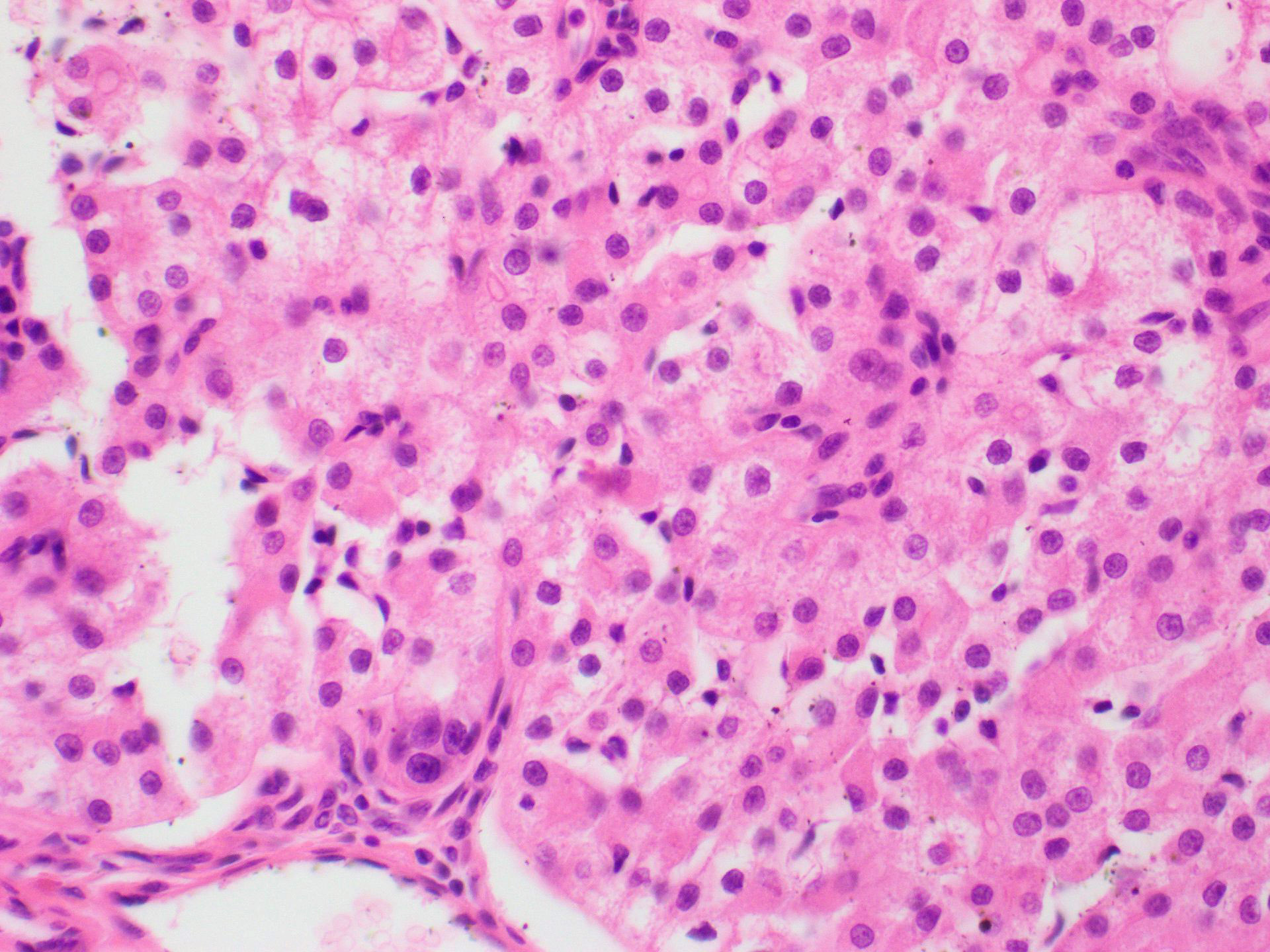
Oncocytes
PASD resistant mucous cells
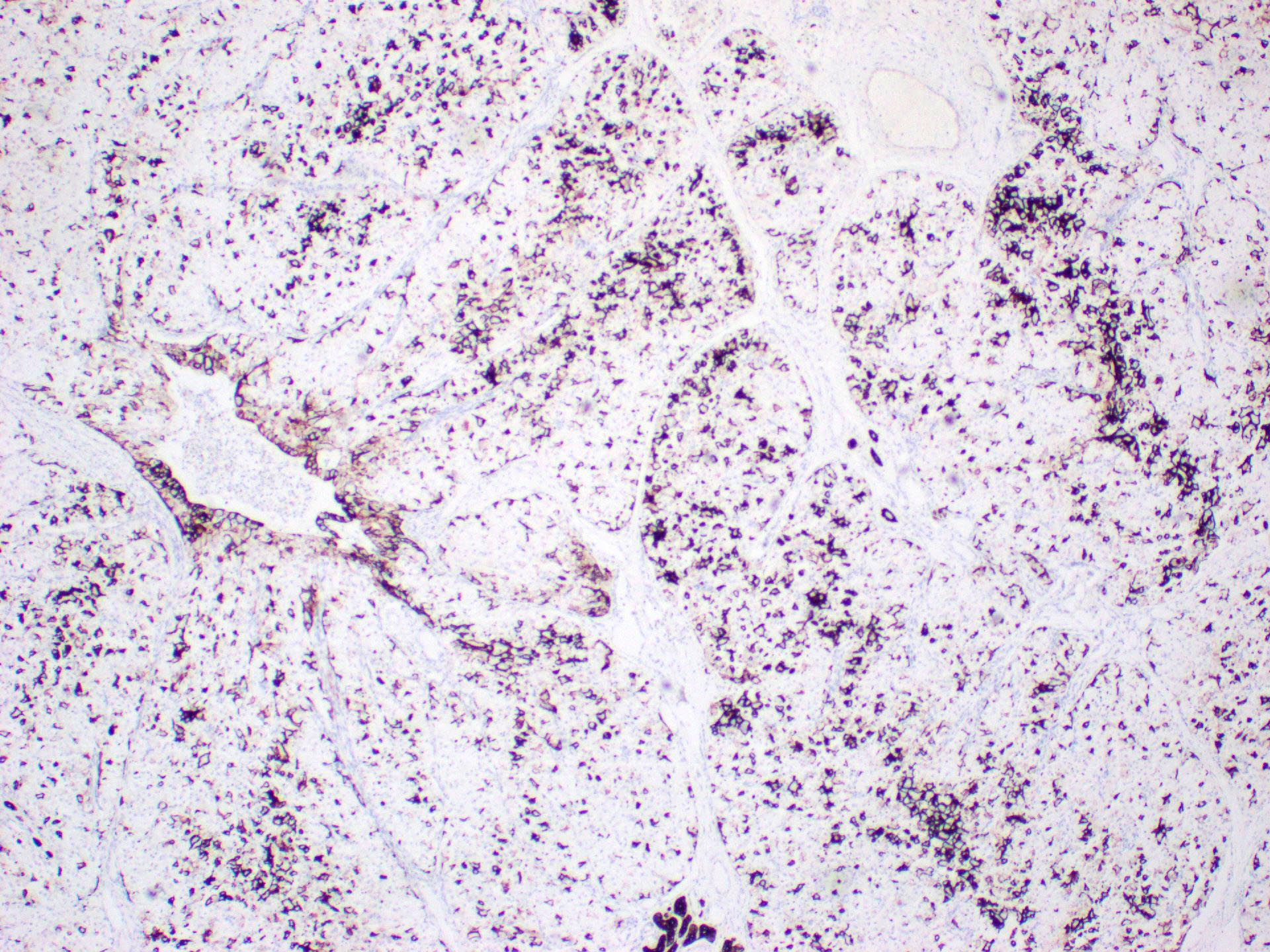
CK7
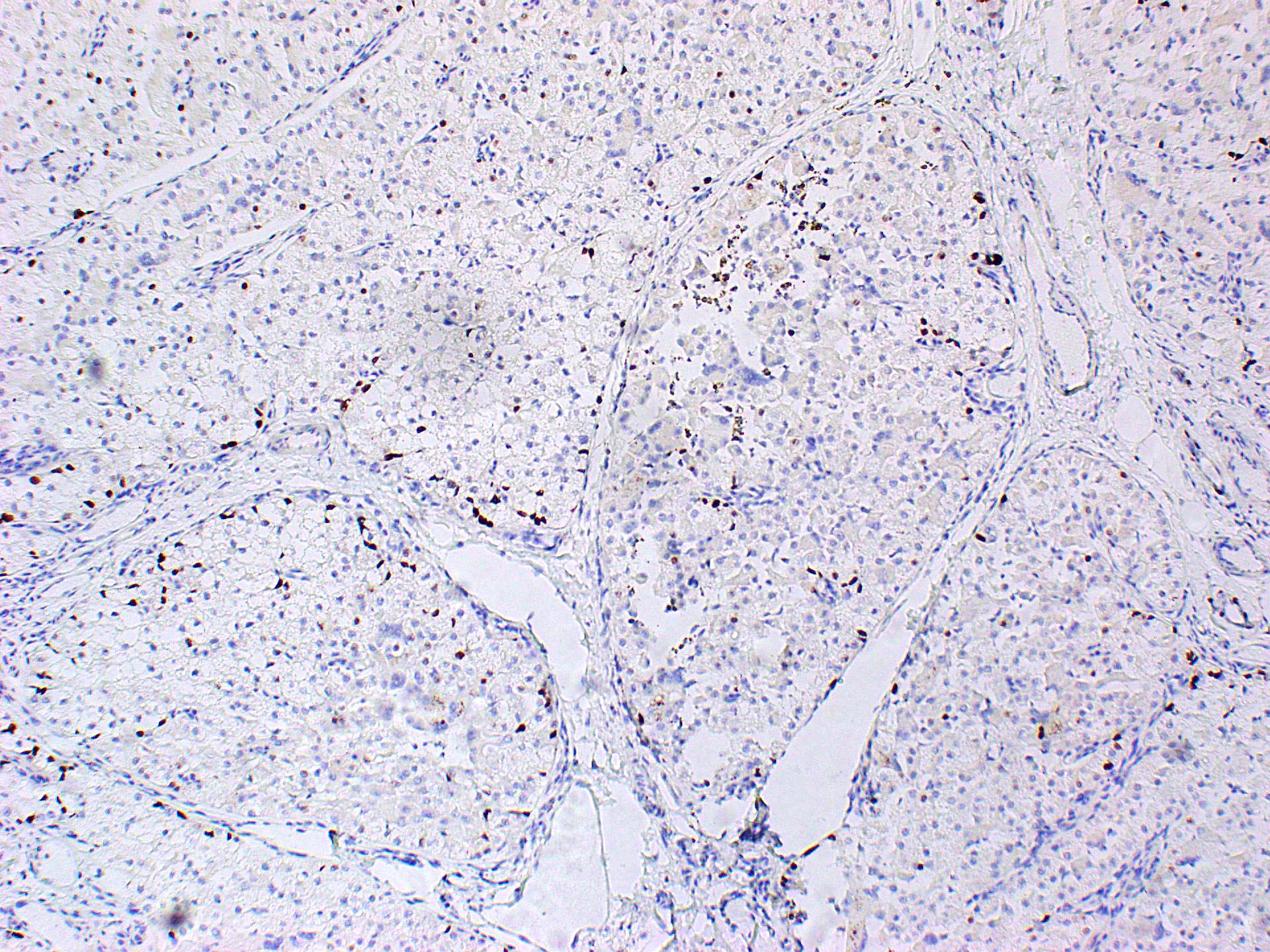
p63
Cytology description
- Smears are usually cellular
- Oncocytes (cells with granular eosinophilic cytoplasm) are arranged in sheets, papillary fragments and individual cells
- Cytologic atypia is absent to minimal
- Absence or very sparse lymphoid component
- Distinction of oncocytoma from oncocytosis or another salivary gland lesion with prominent oncocytic metaplasia may not be possible on cytology alone
- Reference: Head Neck Pathol 2024;18:126
Cytology images
Contributed by Jenny Tung Hiong Lee, M.D. and Ruta Gupta, M.D.
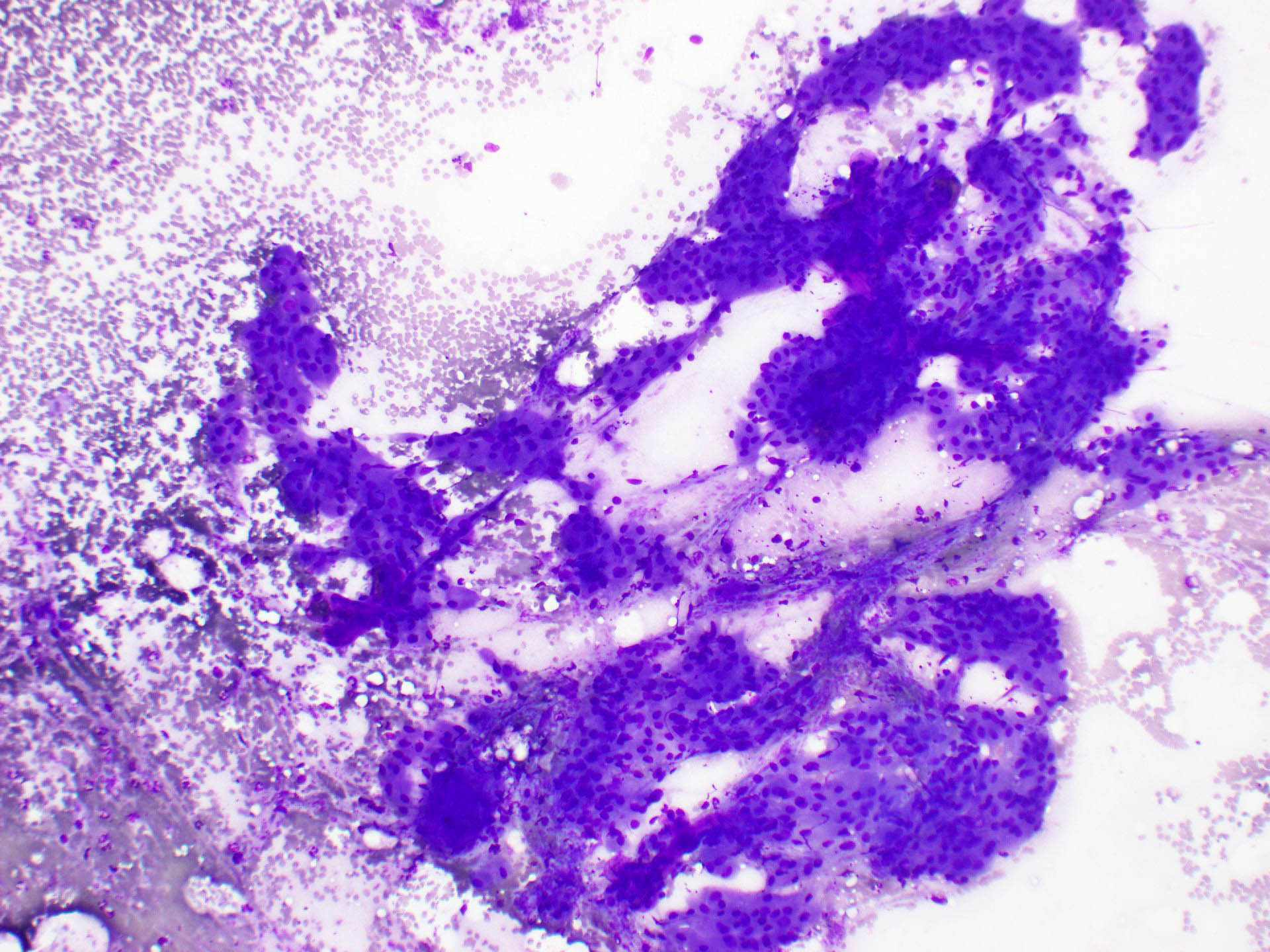
Loosely cohesive tumor cells
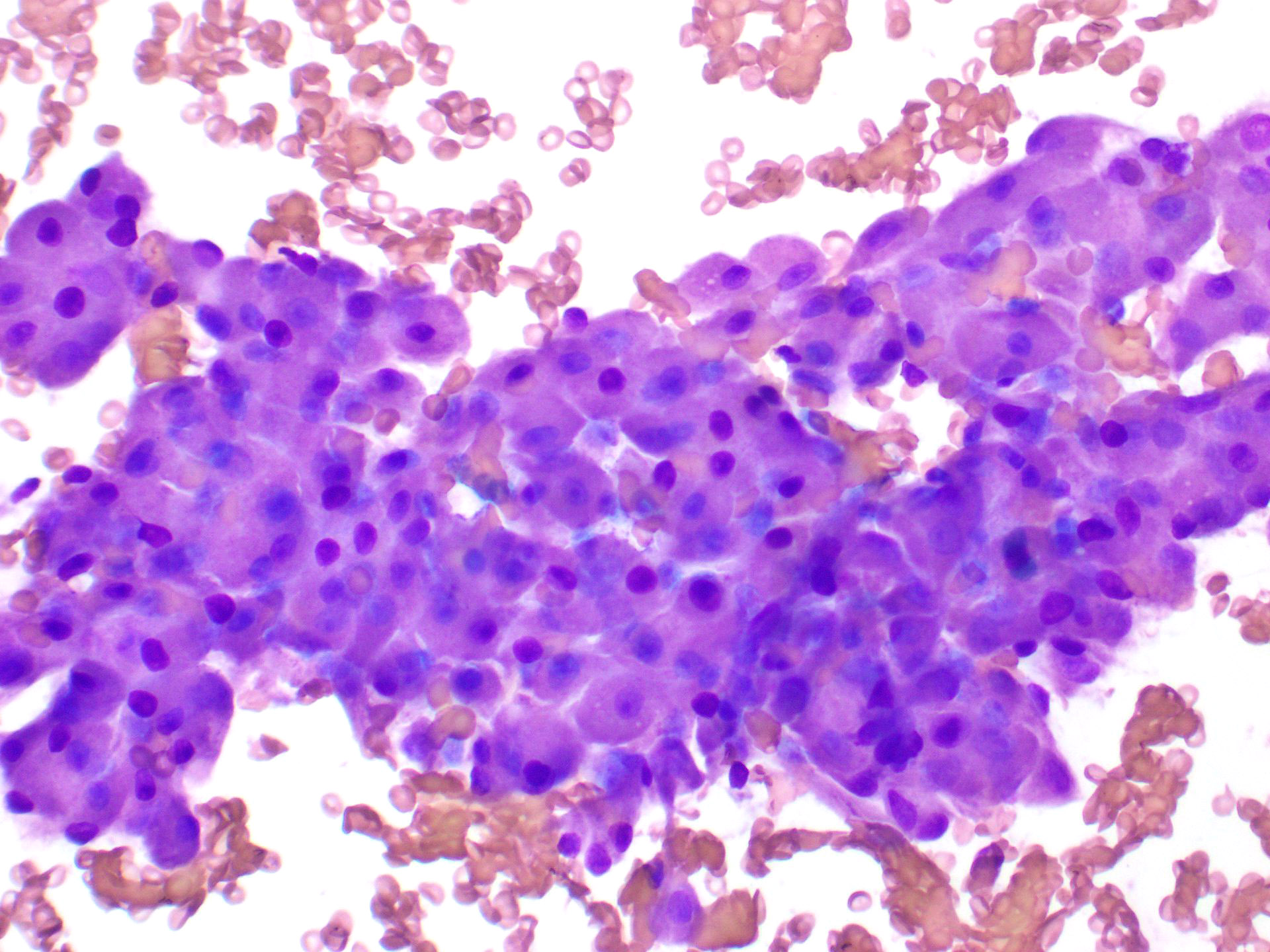
Low N:C ratio
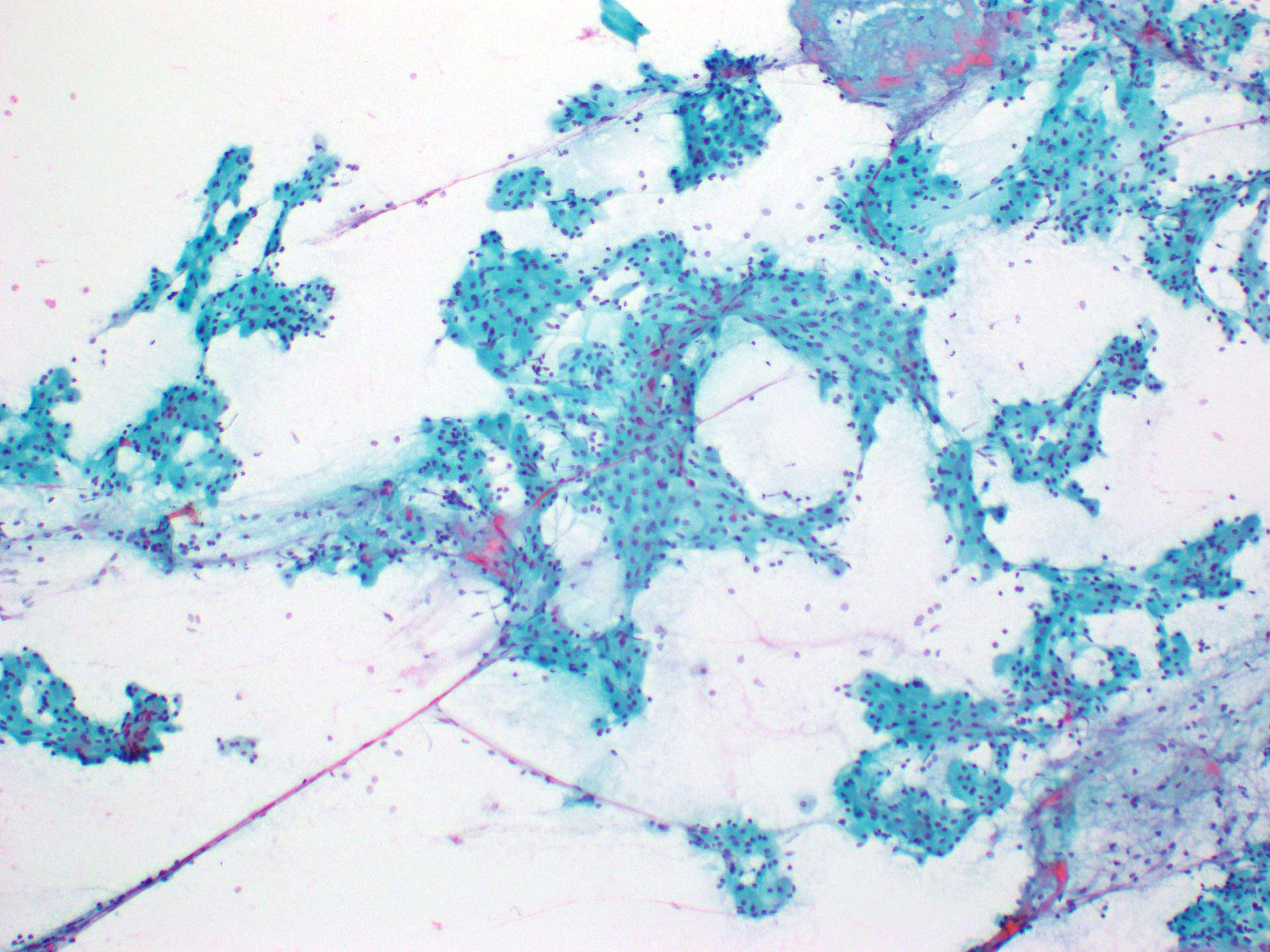
Papillary architecture
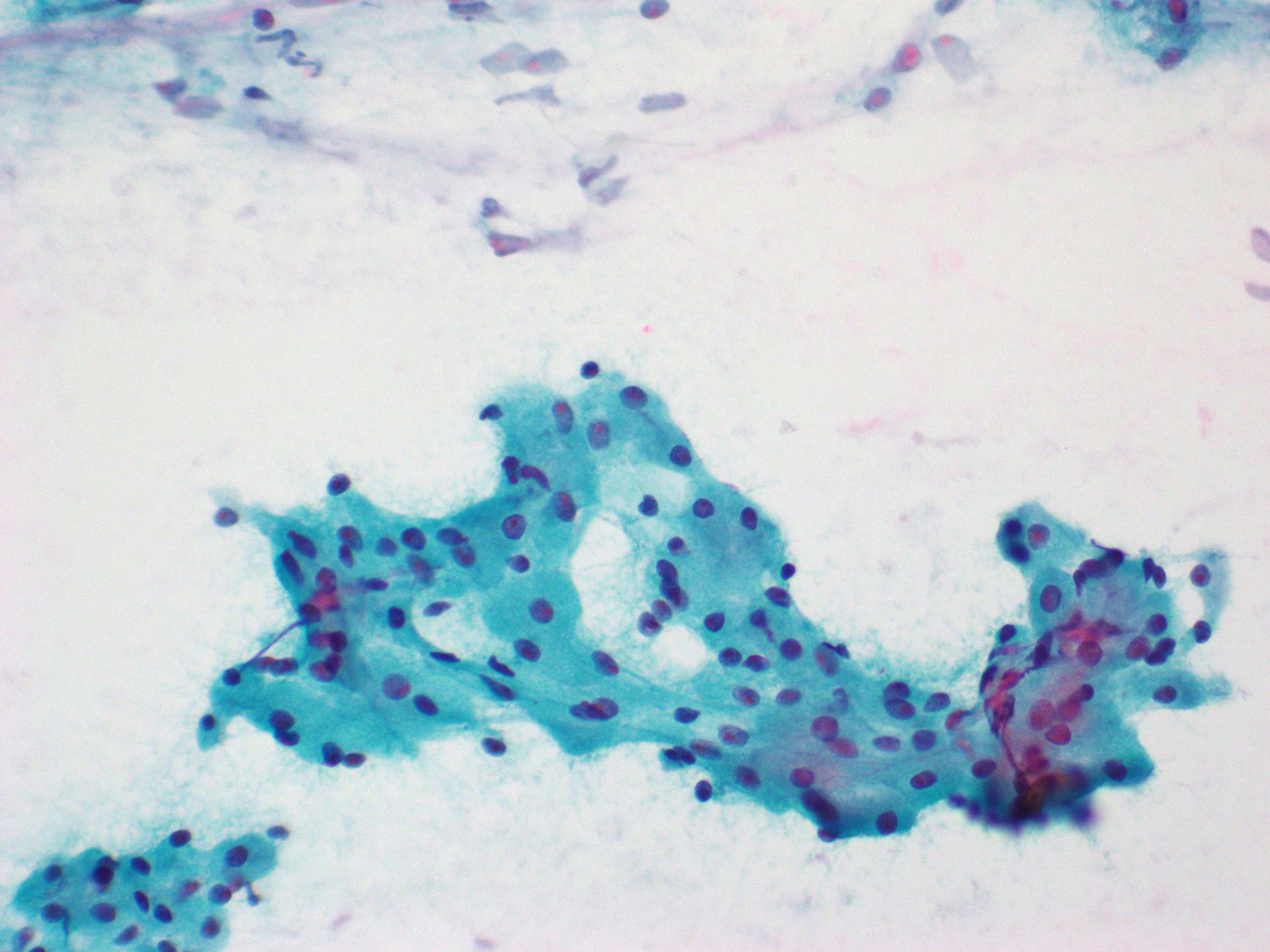
Dense, finely granular cytoplasm
Positive stains
Negative stains
Electron microscopy description
- Cytoplasm of the oncocytes is packed with abundant mitochondria, which are oval or elongated in shape with stacked cristae
- Other organelles, such as endoplasmic reticulum and Golgi complex, are sparse
- Continuous basement membrane around cell clusters
- Reference: Cancer 1976;37:1606
Electron microscopy images
Images hosted on other servers:

Cytoplasm packed
with mitochondria
with stacked cristae
Sample pathology report
- Left parotidectomy:
- Oncocytoma with background multinodular oncocytic hyperplasia (see comment)
- Comment: There is a dominant encapsulated oncocytic nodule. The salivary gland parenchyma shows occasional scattered microscopic oncocytic nodules. There is no evidence of malignancy.
Differential diagnosis
- Oncocytic metaplasia:
- Metaplastic change
- No mass forming lesion
- Ductal and acinar epithelium transformed into oncocytes due to metaplastic process in aging
- Oncocytosis:
- Proliferation of oncocytic cells within the salivary glands
- Often presents as multiple microscopic oncocytic nodules (nodular oncocytic hyperplasia)
- Difficulty in differentiating oncocytoma from diffuse oncocytosis with detectable mass
- Nonencapsulation, multiple nodules and presence of entrapped normal salivary gland parenchyma assist in distinction from oncocytoma
- Pleomorphic adenoma with extensive oncocytic cells:
- Primary salivary gland carcinomas predominantly composed of oncocytic cells:
- Oncocytic mucoepidermoid carcinoma:
- Acinic cell carcinoma (zymogen poor variant):
- Tumor cells are PAS positive, PASD resistant
- They are also positive for DOG1, SOX10 and NOR1 / NR4A3
- Salivary duct carcinoma (oncocytic variant):
- Aggressive and infiltrative tumor frequently involving adjacent structures
- Tumor cells have apocrine phenotype: cytoplasm is granular and eosinophilic and nuclei are large, pleomorphic with prominent nucleoli
- Perineural and lymphovascular invasion is present
- Tumor cells are positive for AR; HER2 is positive in about 30% of cases
- Clear cell carcinoma:
- Usually occurs in minor salivary glands, such as soft palate, buccal and floor of mouth
- Tumor is infiltrative, usually composed of tumor cells with clear cytoplasm within densely hyalinized stroma; perineural invasion may be present
- Diffuse staining for p63, p40 and CK5/6
- Positive for EWSR1 gene rearrangement
- Metastatic renal cell carcinoma:
- Thyroid oncocytic carcinoma:
- Positive for thyroglobulin and TTF1
Additional references
Practice question #1
Which of the following statements regarding oncocytoma of the salivary gland is true?
- The tumor is common in young patients
- The tumor is malignant
- The tumor is positive for PAX8
- The tumor is rare and occurs mostly in the parotid gland
Practice answer #1
D. The tumor is rare and occurs mostly in the parotid gland. Oncocytoma constitutes about 1 - 2% of salivary gland neoplasms and mostly occurs in the parotid gland, followed by the submandibular gland and minor salivary gland. Answer A is incorrect because this tumor occurs mostly in middle aged to older people. Answer B is incorrect because oncocytoma is benign. Answer C is incorrect because oncocytoma is PAX8 negative, which is useful in differentiating this tumor from metastatic renal cell carcinoma.
Comment Here
Reference: Oncocytoma
Comment Here
Reference: Oncocytoma
Practice question #2
Which of the following statements about oncocytic cells in oncocytoma of the salivary gland is true?
- Cytology can differentiate oncocytosis from oncocytoma
- FISH analysis is positive for MAML2 rearrangement
- Oncocytic cells are diffusely positive for p63, p40 and CK5/6
- The main organelle in the cytoplasm of oncocytic cells is the mitochondria
Practice answer #2
D. The main organelle in the cytoplasm of oncocytic cells is the mitochondria. The presence of increased intracytoplasmic mitochondrial content contributes to the eosinophilic granular cytoplasm of oncocytes. Answer C is incorrect because oncocytic cells are predominantly positive for cytokeratins such as CK7 and EMA but very focally positive for p63, p40 and CK5/6, which is useful in differentiating this tumor from mucoepidermoid carcinoma. Answer A is incorrect because cytology cannot differentiate oncocytosis from oncocytoma. Answer B is incorrect because MAML2 rearrangement is seen in mucoepidermoid carcinoma.
Comment Here
Reference: Oncocytoma
Comment Here
Reference: Oncocytoma
