Salivary glands
Primary salivary gland neoplasms
Malignant
Mucoepidermoid carcinoma
Authors: Saeed Asiry, M.D., Rema A. Rao, M.D.
Editorial Board Member: Lisa Rooper, M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.


Last author update: 15 October 2021
Last staff update: 1 April 2024
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Mucoepidermoid carcinoma salivary gland
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2 | Practice question #3 | Practice answer #3Cite this page: Asiry S, Rao RA. Mucoepidermoid carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/salivaryglandsmec.html. Accessed October 5th, 2025.
Definition / general
- Malignant glandular epithelial neoplasm characterized by mucous, intermediate and epidermoid cells, with columnar, clear cell or oncocytoid features
Essential features
- Malignant epithelial neoplasm
- Characterized by mucous, intermediate and epidermoid cells, with columnar, clear cell or oncocytoid features
- Most common malignant salivary gland neoplasm in both adults and children
- Prognosis influenced by tumor stage, tumor site, surgical margins (WHO 2017)
- Associated with a specific translocation t(11;19)(q14-21;p12-13) with CRTC1(MECT1)-MAML2 fusion
Terminology
- Mucoepidermoid carcinoma (MEC)
- Not recommended: mucoepidermoid tumor
ICD coding
Epidemiology
- Most common malignant salivary gland tumor (adults and children) (Br J Oral Maxillofac Surg 2013;51:399)
- Represents 10 - 15% of all salivary gland tumors (Br J Oral Maxillofac Surg 2013;51:399)
- Adults: wide age range (15 - 86 years, median 49 years) (Am J Surg Pathol 2001;25:835)
- Children: 11 - 15 years (median 13 years) (Int J Pediatr Otorhinolaryngol 2019;120:93)
- F > M (slight predominance) (Br J Oral Maxillofac Surg 2013;51:399)
Sites
- Occurs in major and minor salivary glands (predominance of major > minor) (Eur J Surg Oncol 2021;47:1376)
- Major: parotid > submandibular > sublingual (Eur J Surg Oncol 2021;47:1376)
- Minor: palate, buccal mucosa, retromolar region (Indian J Pathol Microbiol 2018;61:397)
- Rarely occurs in sinonasal tract, nasopharynx, lungs and intraosseous mandible (Int Forum Allergy Rhinol 2019;9:1046, Expert Rev Respir Med 2018;12:249, Case Rep Dent 2018;2018:9348540)
Etiology
- Possible association with ionizing radiation (Indian J Pathol Microbiol 2018;61:397)
Clinical features
- In one study, 33% of patients are asymptomatic; however, varies with tumor site and size (J Stomatol Oral Maxillofac Surg 2020;121:713)
- Most common presentation is painless swelling with pressure and discomfort
- Can be variably fixed, rubbery or soft mass (J Stomatol Oral Maxillofac Surg 2020;121:713)
Diagnosis
- Preoperative assessment (radiology) may consist of:
- Ultrasonography (USG) for small tumors in major salivary glands
- Larger recurrent tumors: CT imaging for bone involvement, MRI for soft tissue delineation (Semin Radiat Oncol 2012;22:245)
- Evidence of (18)-fluorodeoxyglucose positron emission tomography CT in locoregionally advanced tumors (Nucl Med Commun 2013;34:211)
- Preoperative assessment (fine needle aspiration)
Radiology description
- Influenced by tumor size, location and possibly tumor grade
- Ultrasonography:
- Typically a well circumscribed hypoechoic lesion, with a partial or completely cystic appearance against a relatively hyperechoic normal parotid gland
- CT:
- Lower grade tumors are well circumscribed with cystic component (see Radiology images)
- Enhancing solid component and calcifications occasionally seen
- Higher grade tumors are solid and show poorly defined, infiltrative margins
- MRI:
- Low grade tumors are similar in appearance to a pleomorphic adenoma
- Higher grade tumors are solid, with a lower signal on T2 and poorly defined margins
- Reference: Radiopaedia: Mucoepidermoid Carcinoma of Salivary Glands [Accessed 8 January 2021]

Prognostic factors
- Adults:
- Excellent prognosis, with approximately 98.8% 5 year survival rate in low grade and 97.4% in intermediate grade tumors
- About 67% 5 year survival rate for high grade tumors
- Children:
- 5 year survival of 98%, as they predominantly present with low to intermediate grade tumors
- Negative prognostic variables
- Tumor arising in the submandibular gland: lymph node metastases common
- Positive surgical margins
- Extraparenchymal extension
- Nodal / distant metastases
- Increased expression of MUC1
- References: J Stomatol Oral Maxillofac Surg 2020;121:713, Wenig: Atlas of Head and Neck Pathology, 3rd Edition, 2016
Case reports
- 16 year old boy with a mandibular radiolucent lesion (Case Rep Dent 2018;2018:9348540)
- 36 year old man with a left parotid gland mass (Anticancer Res 2019;39:3213)
- 69 year old woman with a right submental mass (Eur Ann Otorhinolaryngol Head Neck Dis 2017;134:355)
Treatment
- Complete surgical resection
- Conservative approach for stage I and stage II tumors
- Wide excision with wide margin for high grade tumors or tumors with positive margins
- Neck lymph node dissection (depends on nodal status and histologic grade)
- Adjuvant radiotherapy and chemotherapy might be considered for higher grade tumors
- Reference: J Stomatol Oral Maxillofac Surg 2020;121:713
Gross description
- Incompletely encapsulated or unencapsulated
- Well circumscribed
- Low grade: often cystic
- High grade: often solid, necrotic, tan-pink
- References: J Stomatol Oral Maxillofac Surg 2020;121:713, Wenig: Atlas of Head and Neck Pathology, 3rd Edition, 2016
Gross images
Contributed by Kelly Magliocca D.D.S., M.P.H.
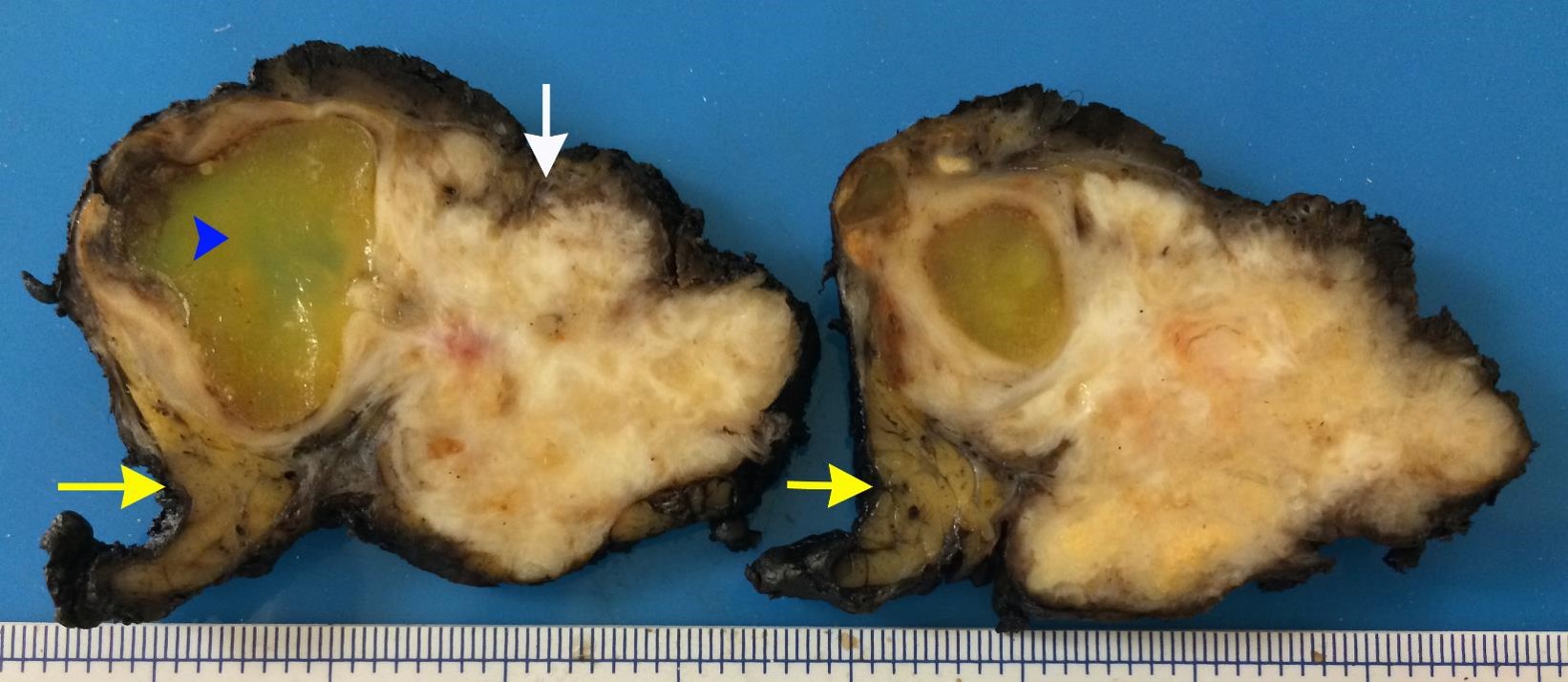
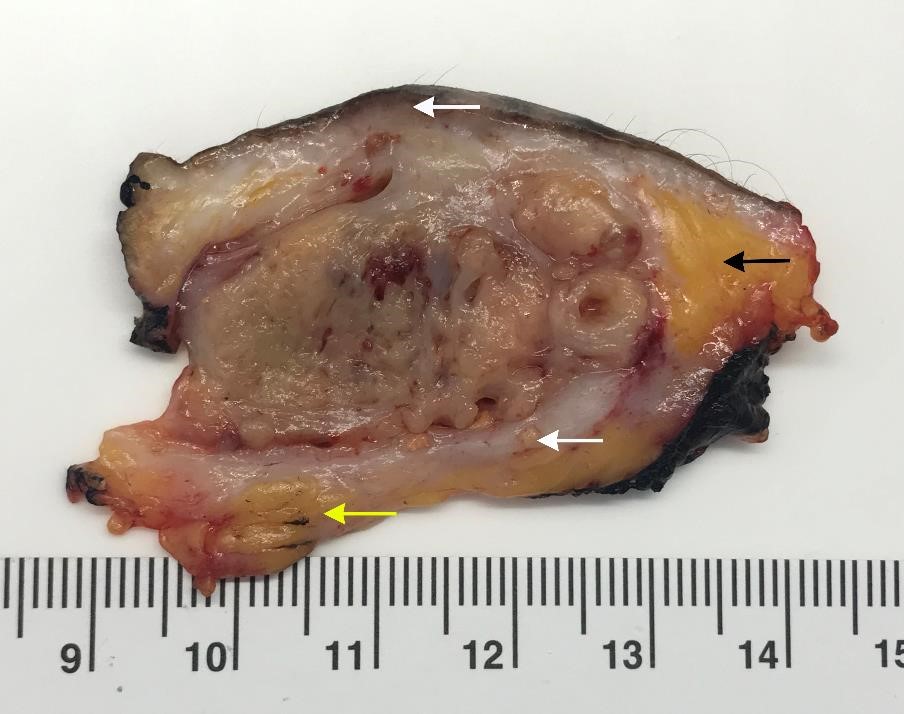
Cut surface, high grade
Frozen section description
- Higher grade tumors can be mistaken for squamous cell carcinoma, a pitfall (Cancer 2004;100:1876)
Frozen section images
Contributed by Rema A. Rao, M.D. and Saeed Asiry, M.D.

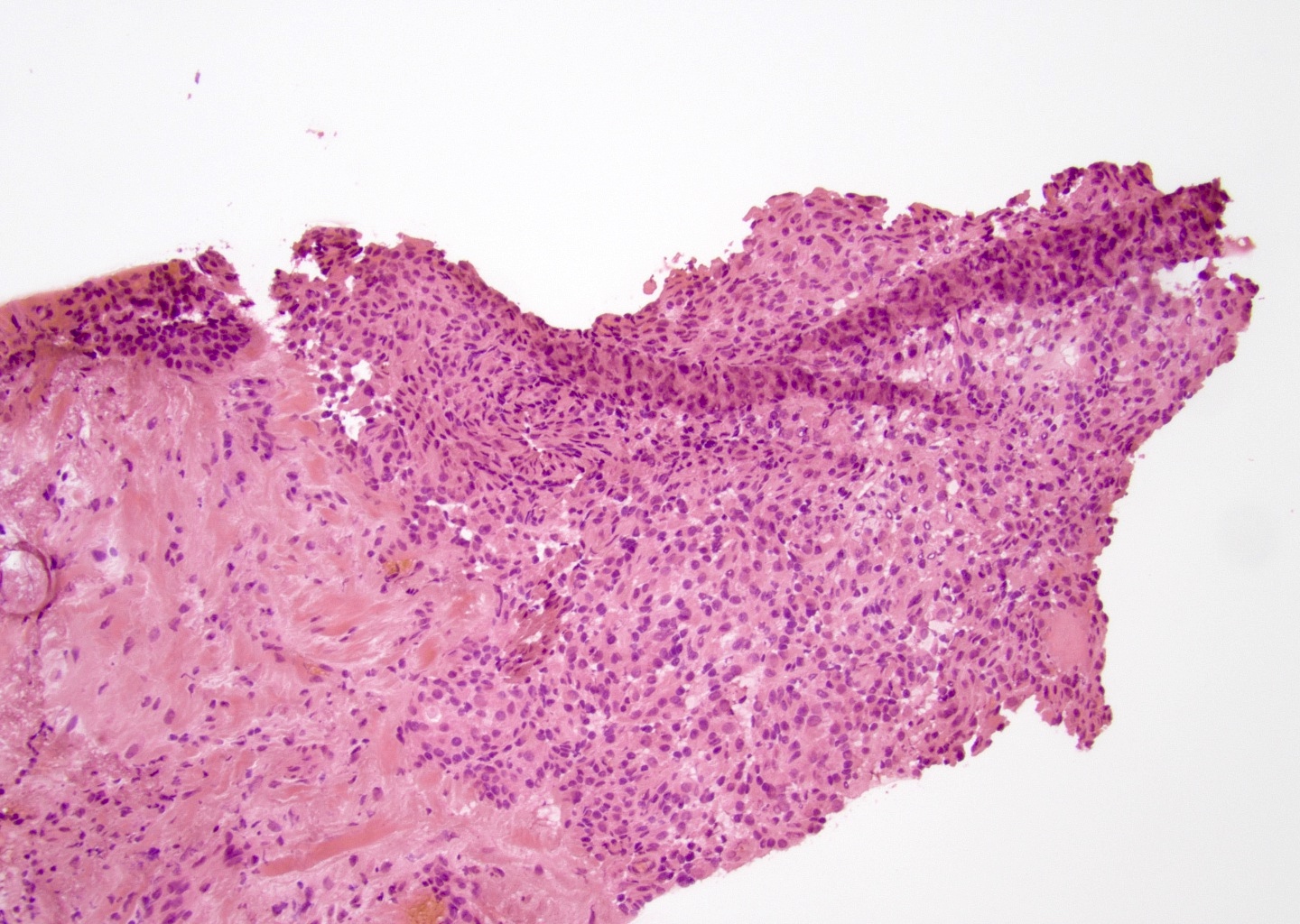
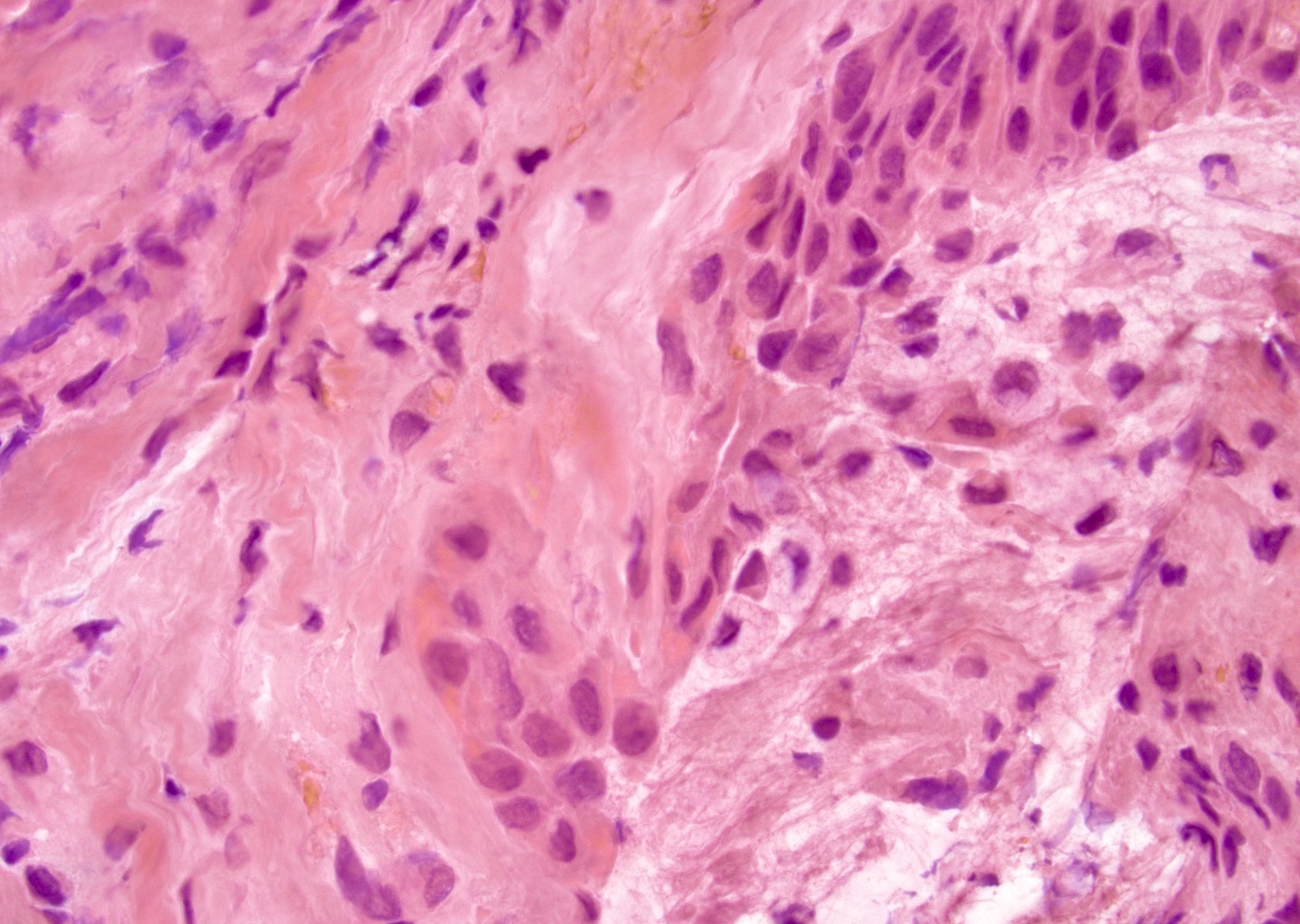
Positive margin for tumor
Microscopic (histologic) description
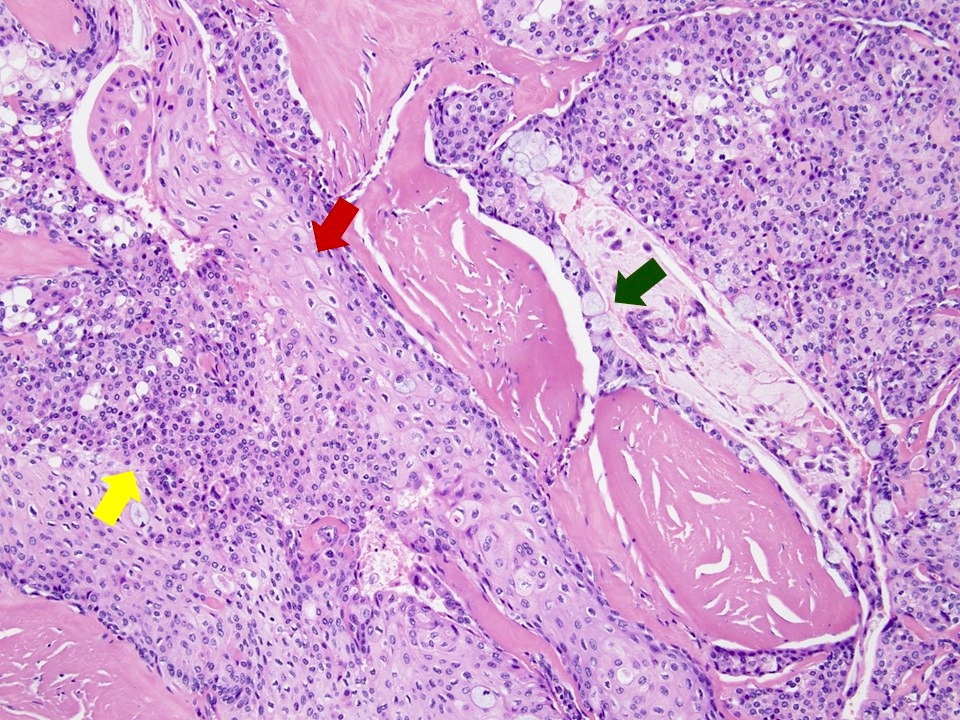
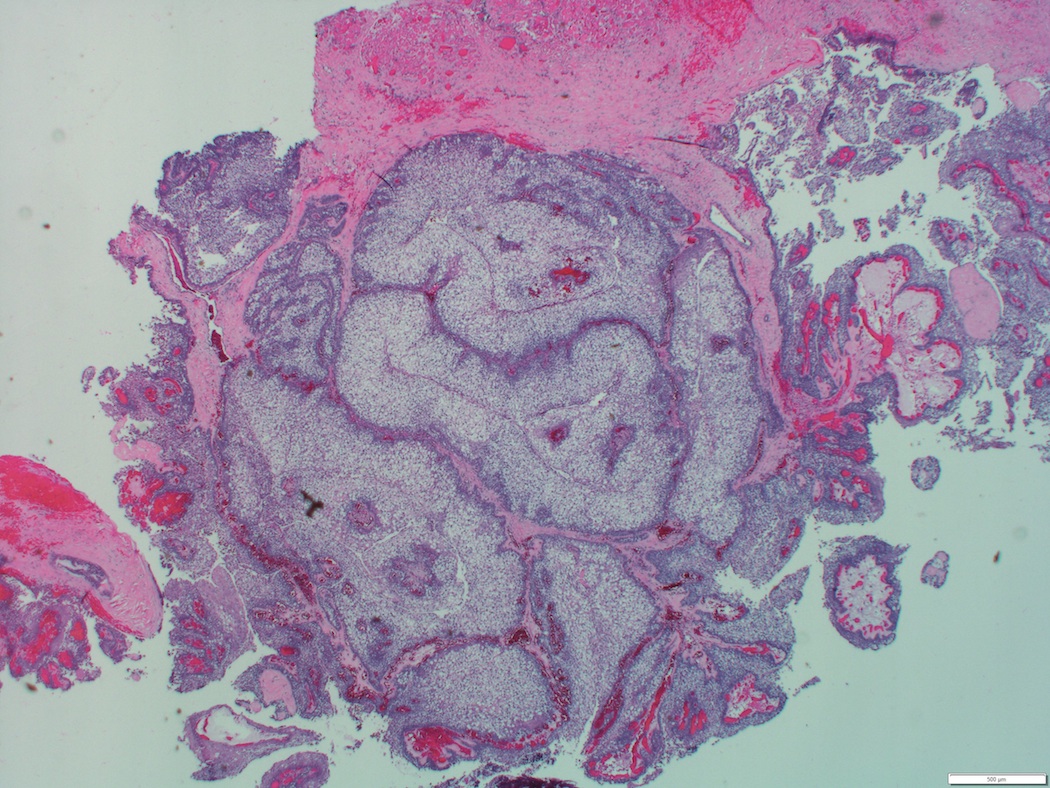
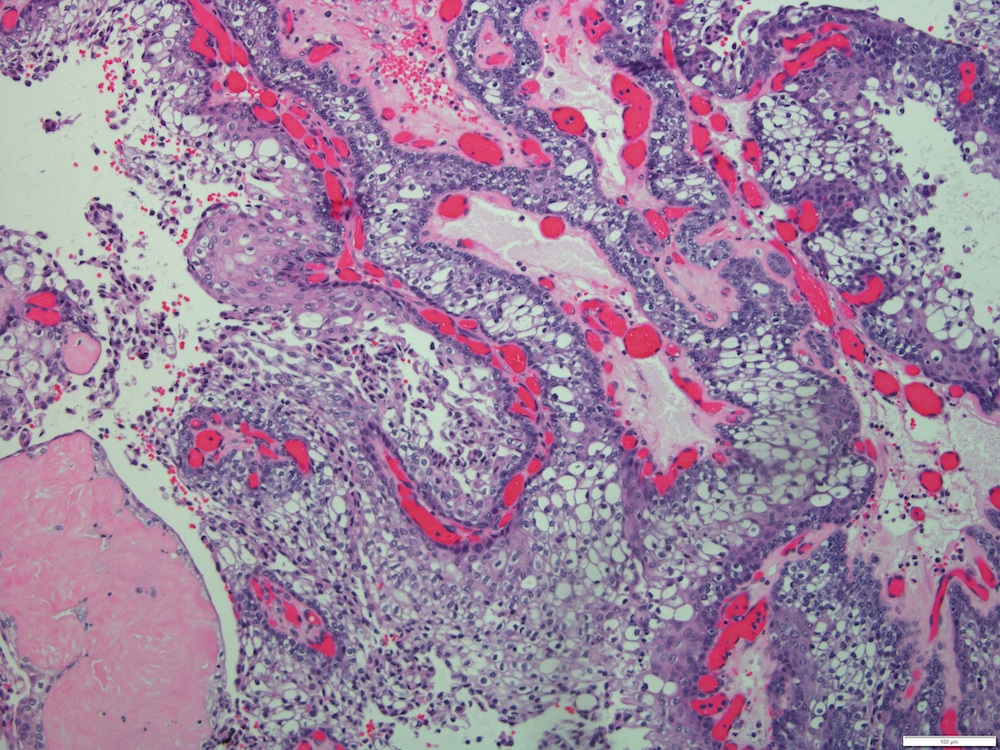
- Solid, cystic or mixed growth patterns
- Can show papillary or glandular growth pattern
- Areas suggesting a capsule can be seen in low grade mucoepidermoid carcinoma
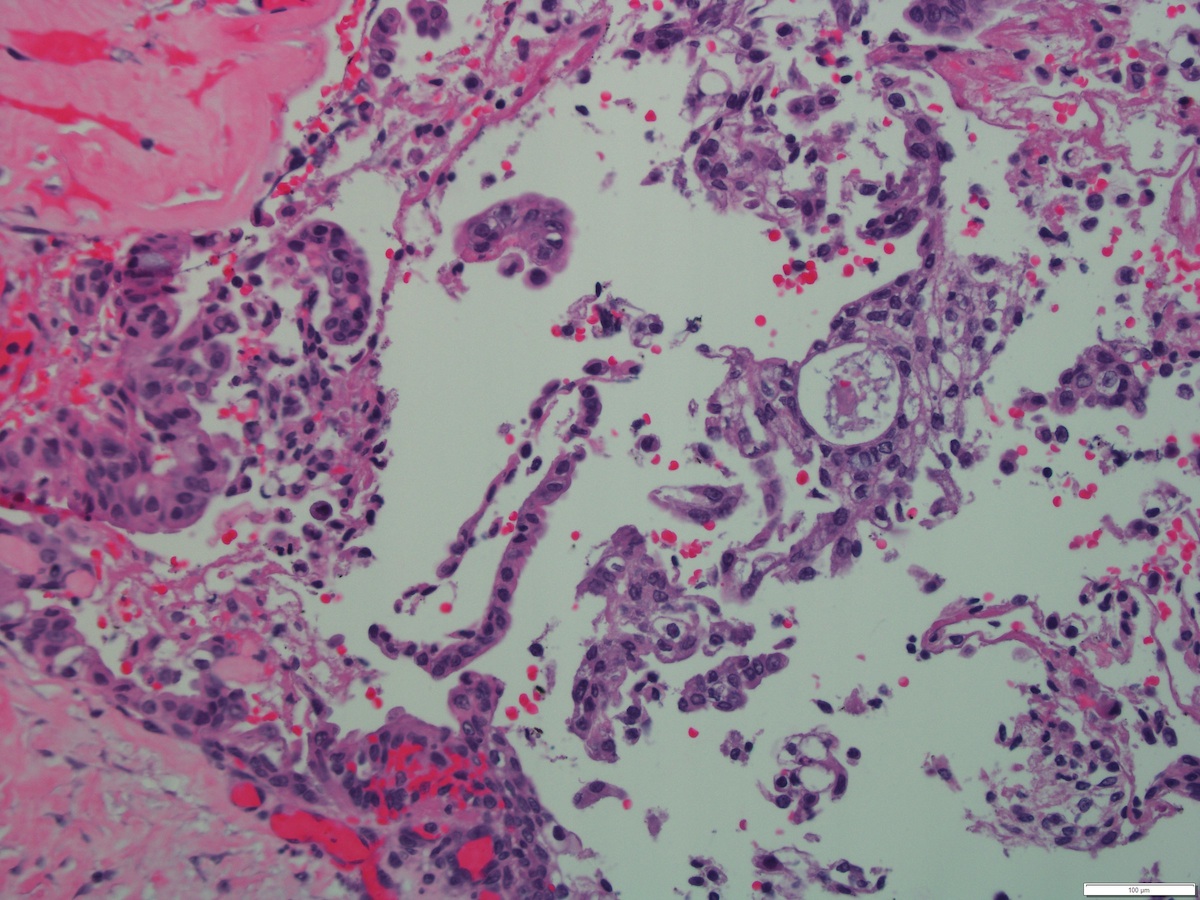
- Varying proportions of epidermoid cells, intermediate cells and mucocytes
- Solid nests, sheets or cords of epidermoid cells
- Overt keratinization is rare
- Mucous cells embedded in epidermoid cell nests or lining cystic spaces
- Intermediate cells found within epidermoid cell nests or forming separate nests
- Background stromal sclerosis
- Luminal or extracellular pools of mucin may be present
- Mitosis, necrosis and pleomorphism more commonly seen in high grade tumors
- Limited number of mucocytes and cystic spaces in high grade tumors
- Perineural and lymphovascular invasion possible (Wenig: Atlas of Head and Neck Pathology, 3rd Edition, 2016)
- Focal clear cell changes can occur due to accumulation of glycogen
- Histologic variants: clear cell, oncocytic, sclerosing, Warthin-like, ciliated, spindle cell and mucoacinar (Am J Surg Pathol 2015;39:1479, Am J Surg Pathol 2018;42:130, Int J Surg Pathol 2017;25:705, Am J Surg Pathol 2021;45:1028, Am J Surg Pathol 1999;23:523)
- Reference: J Stomatol Oral Maxillofac Surg 2020;121:713
Histopathologic grading:
- 4 histologic grading systems (2 quantitative and 2 qualitative)
- 2 different morphologic quantitative point systems, although histologic grading using any grading system appears to be inconsistent (Am J Surg Pathol 2019;43:885)
- Significant grading disparity between pathologists (Am J Surg Pathol 2019;43:885)
- Armed Forces Institute of Pathology (AFIP) grading scheme (quantitative) (Am J Surg Pathol 2019;43:885)
- Criteria:
- Intracystic component less than 20% (2)
- Neural invasion (2)
- Necrosis (3)
- 4 or more mitoses (3)
- Anaplasia (4)
- Grade:
- Low grade (0 - 4)
- Intermediate grade (5 - 6)
- High grade (7 or more)
- Criteria:
- Brandwein et al. grading scheme (quantitative) (Am J Surg Pathol 2001;25:835)
- Criteria:
- Intracystic component less than 25% (2)
- Tumor front invades in small nests and islands (2)
- Pronounced nuclear atypia (2)
- Lymphovascular invasion (3)
- Bony invasion (3)
- 4 or more mitoses (3)
- Perineural invasion (3)
- Necrosis (3)
- Grade:
- Low grade (0)
- Intermediate grade (2 - 3)
- High grade (4 or more)
- Criteria:
- Modified Healy grading system (qualitative)
- Low grade
- Macro and microcysts
- Rare intermediate cells
- Rare mitotic figures
- Absent or minimal nuclear pleomorphism
- Well circumscribed tumor with broad edges
- Extravasated mucin and fibrotic stroma present
- Intermediate grade
- Microcysts and solid component
- More intermediate cells
- Few mitotic figures
- Slight nuclear pleomorphism
- Uncircumscribed tumor
- Fibrotic stroma separating tumor nests
- High grade
- Predominantly solid, with or without microcysts
- Perineural invasion present
- Lymphovascular invasion present
- Surrounding soft tissue invasion present
- Many mitotic figures
- Nuclear pleomorphism, including presence of prominent nucleoli
- Predominance of intermediate cells
- Desmoplastic stoma
- Low grade
- Memorial Sloan Kettering Cancer Center (MSKCC) grading system (qualitative)
- Low grade
- Predominantly cystic growth pattern (> 80%)
- 0 - 1 mitotic figures/10 high power fields (HPF)
- Well circumscribed
- No necrosis
- Intermediate grade
- Predominantly solid growth pattern
- 2 - 3 mitotic figures/10 high power fields (HPF)
- Well circumscribed or infiltrative
- No necrosis
- High grade
- Any growth pattern but usually solid
- ≥ 4 mitotic figures/10 high power fields (HPF)
- Usually infiltrative
- Necrosis is present
- Low grade
Microscopic (histologic) images
Contributed by Rema A. Rao, M.D. and Saeed Asiry, M.D.

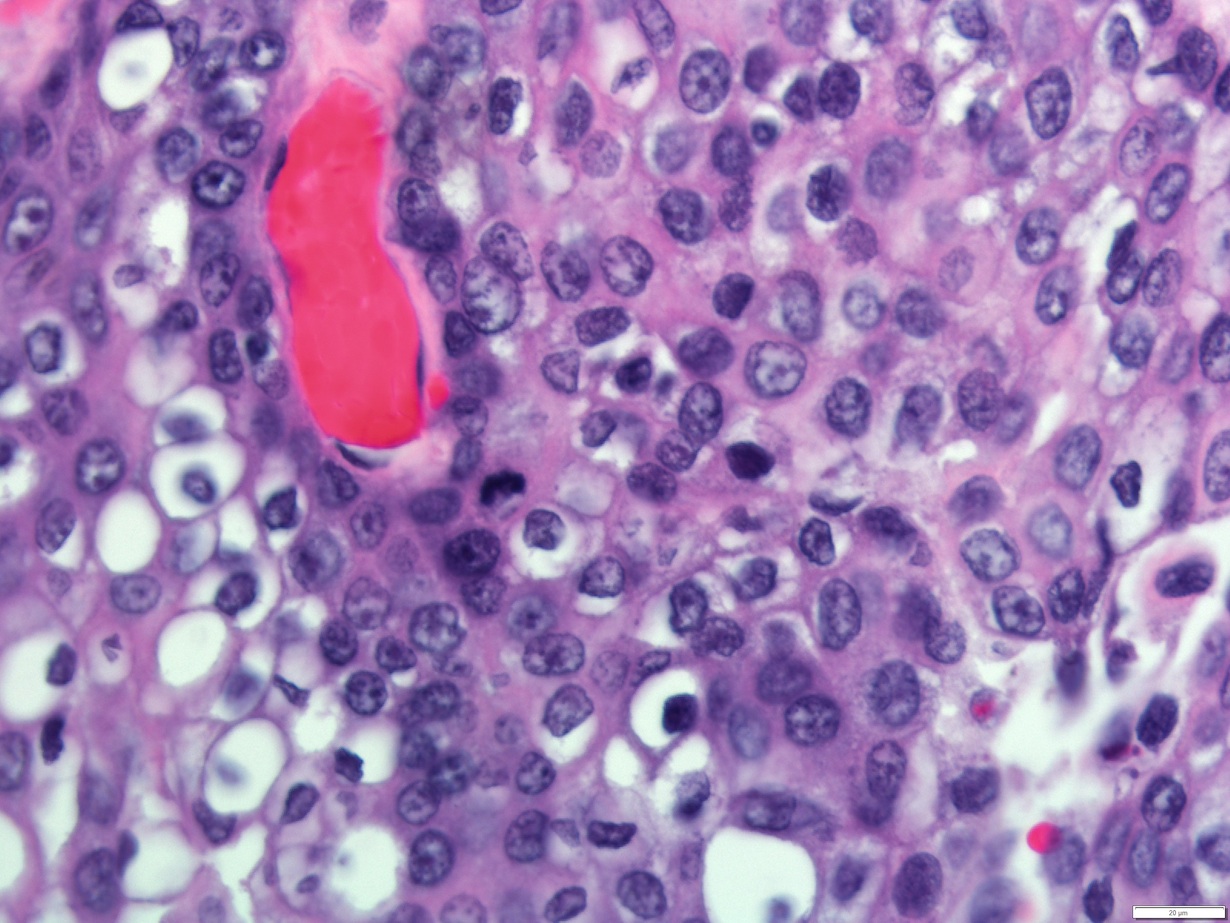
Tumor architecture
Tumor cell types
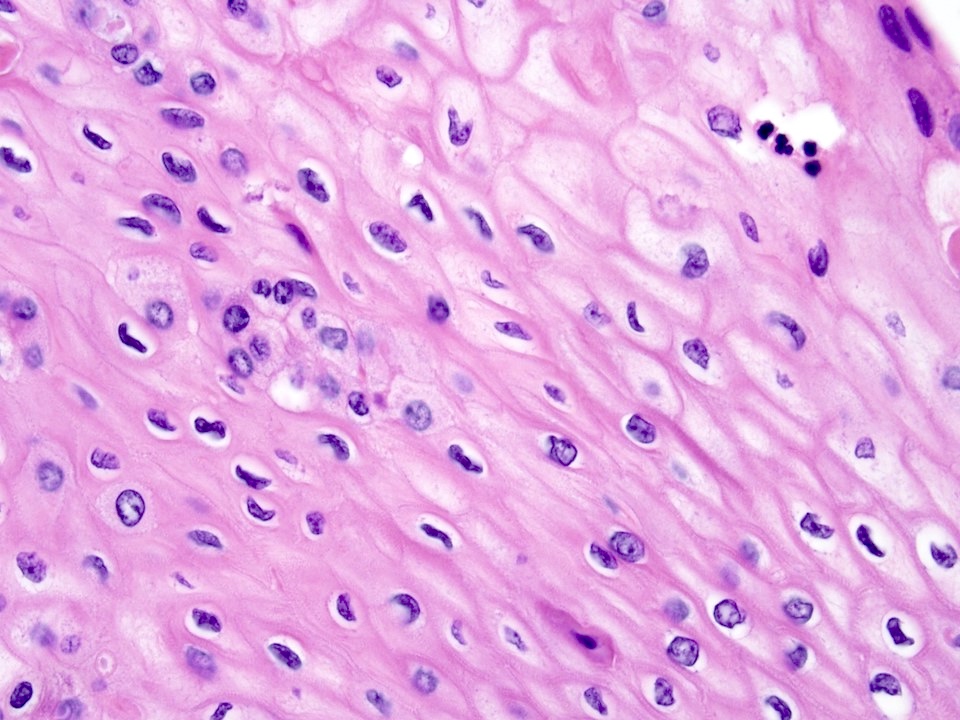
Epidermoid cells
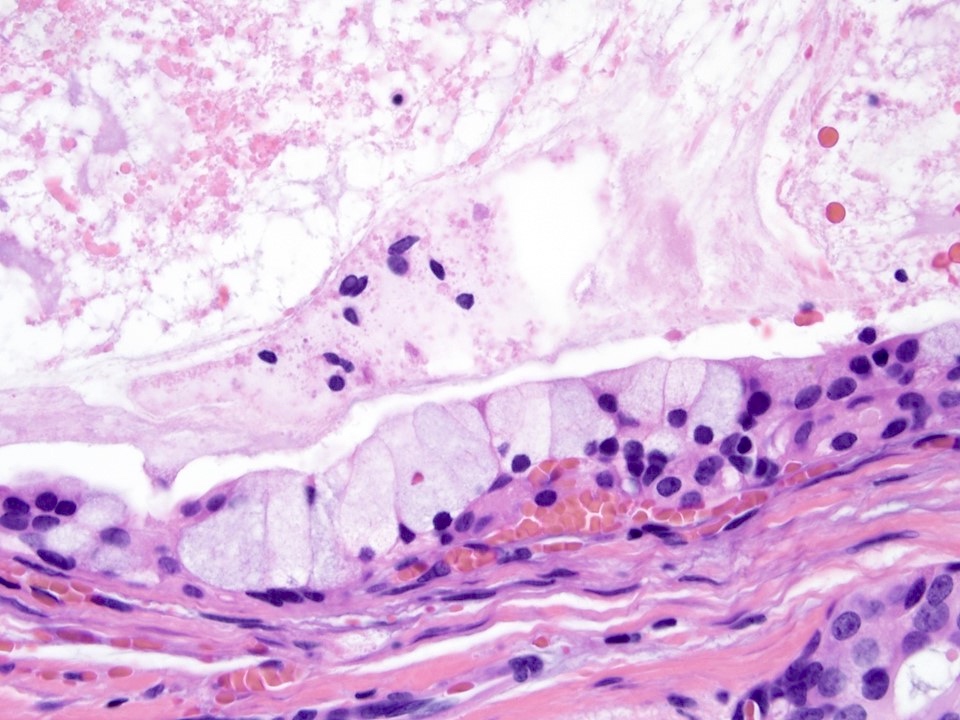
Mucus cells
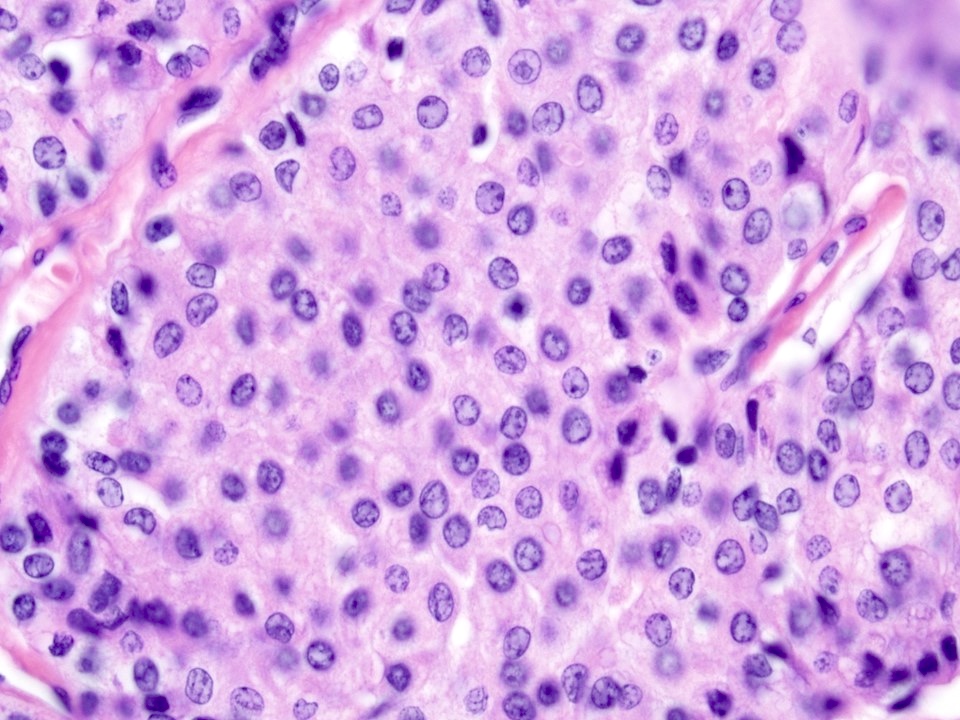
Intermediate cells
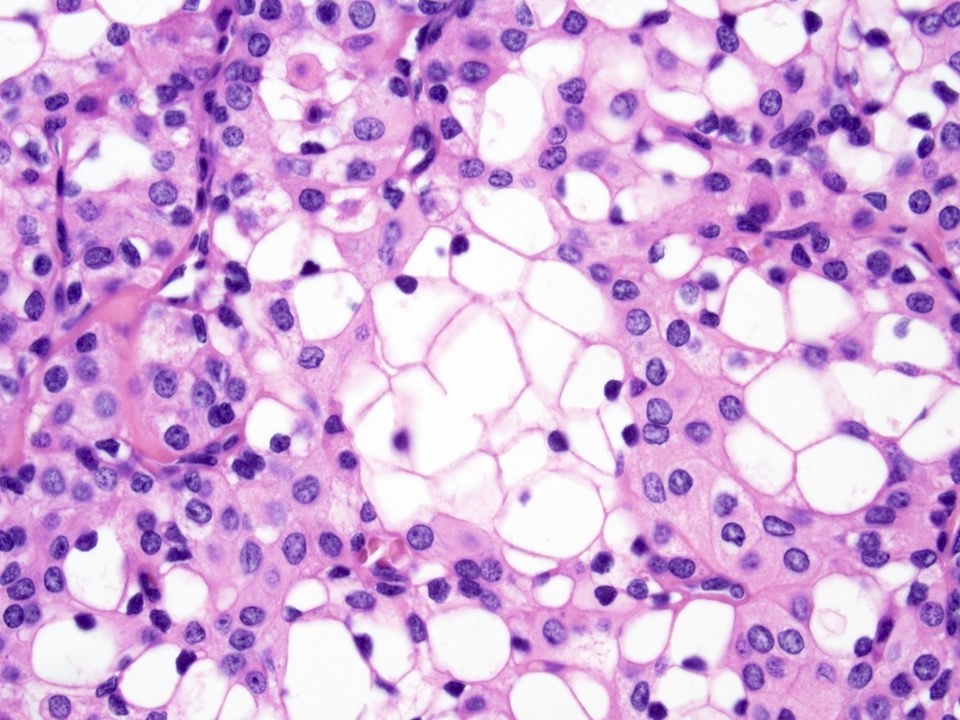
Clear cell changes
Case #346
4 year old boy

Ki67

Mucicarmine
Virtual slides
Images hosted on other servers:

Low grade mucoepidermoid carcinoma
Cytology description
- Most often graded as low grade or high grade on FNA
- Low to intermediate grade:
- Can be acellular or hypocellular smears
- Extracellular mucin may be the prominent feature
- Cystic background
- Aggregates of epidermoid cells, intermediate cells and mucocytes
- Epidermoid cells appear as bland cohesive flat sheets with squamoid / dense cytoplasm and well defined cellular borders
- Predominantly mucus cells floating in extracellular mucin (low grade)
- No keratinization seen
- Lympocytes present in about 20% of cases and are abundant
- High grade:
- Highly cellular aspirates
- High grade nuclear features with pleomorphic nuclei, prominent nucleoli
- Intermediate cells and mucous cells are rare
- Increased mitosis
- Necrotic background
- References: J Clin Diagn Res 2017;11:ER04, Cibas: Cytology - Diagnostic Principles and Clinical Correlates, 5th Edition, 2020
Cytology images
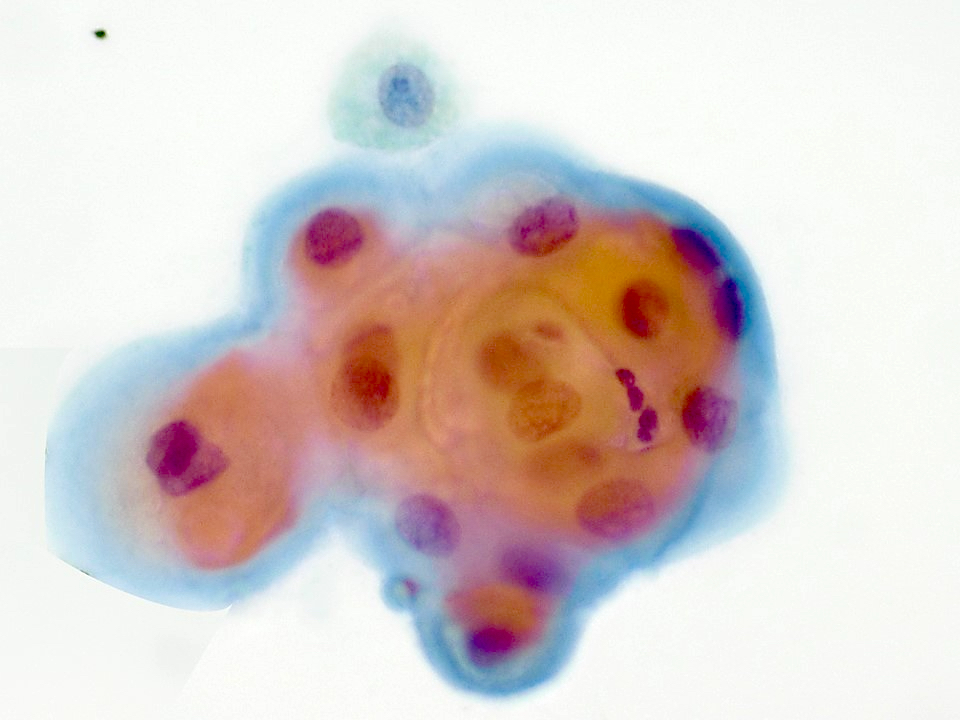
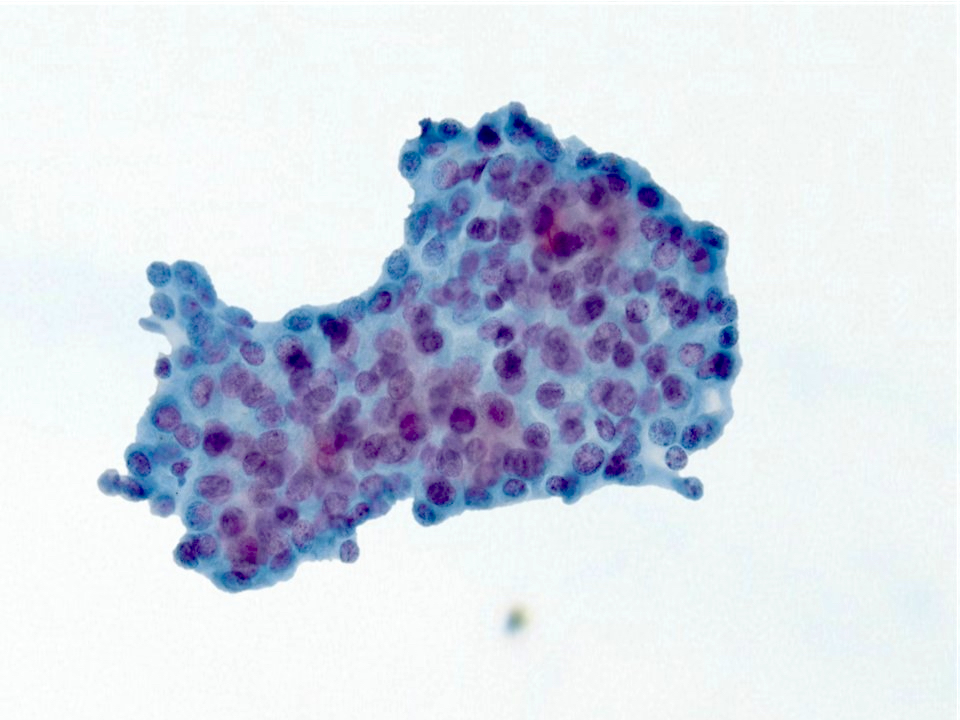
Contributed by Rema A. Rao, M.D. and Saeed Asiry, M.D.
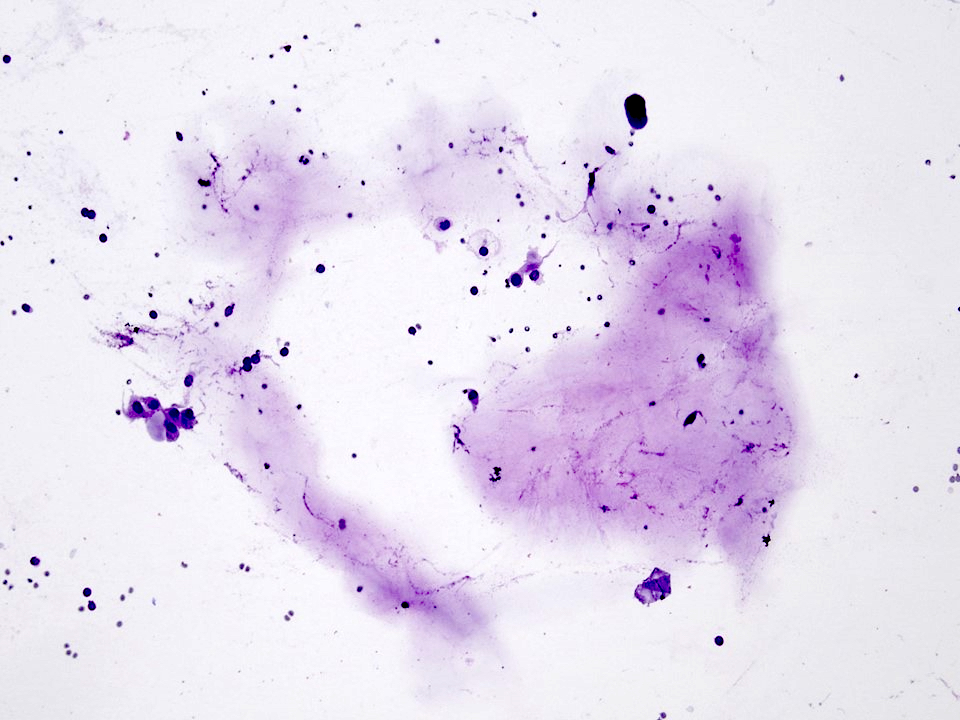
Background mucin
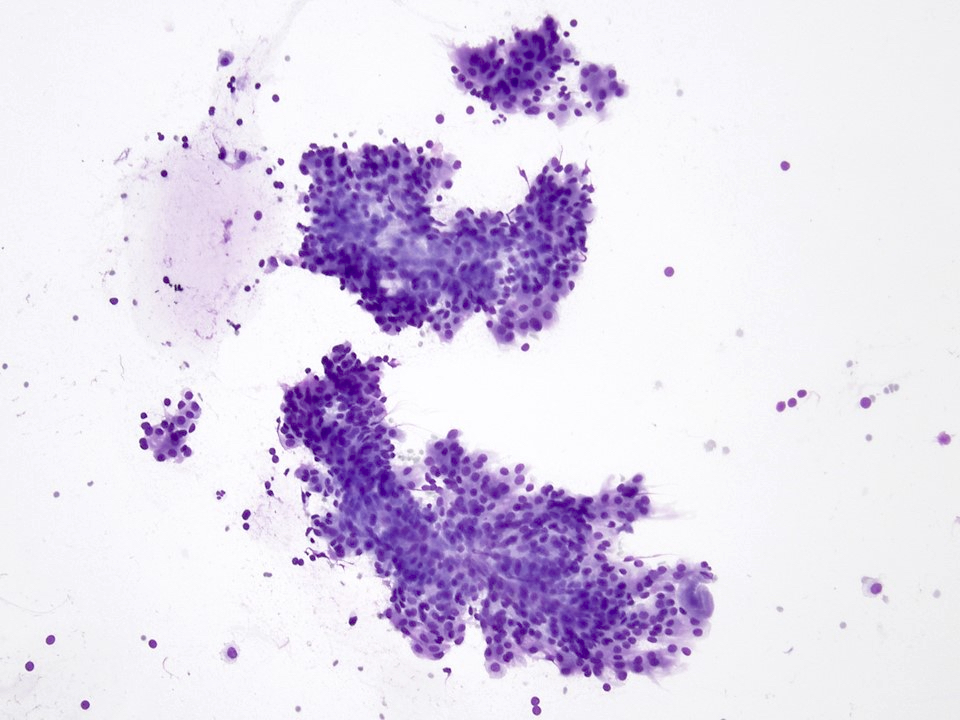
Neoplastic cells
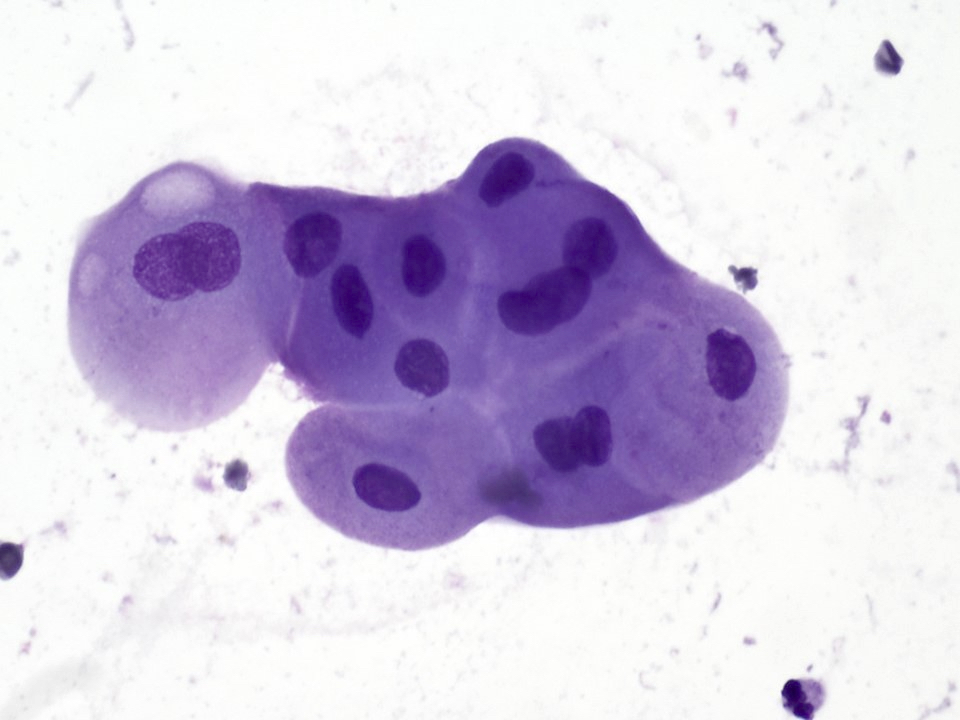
Mucus cells
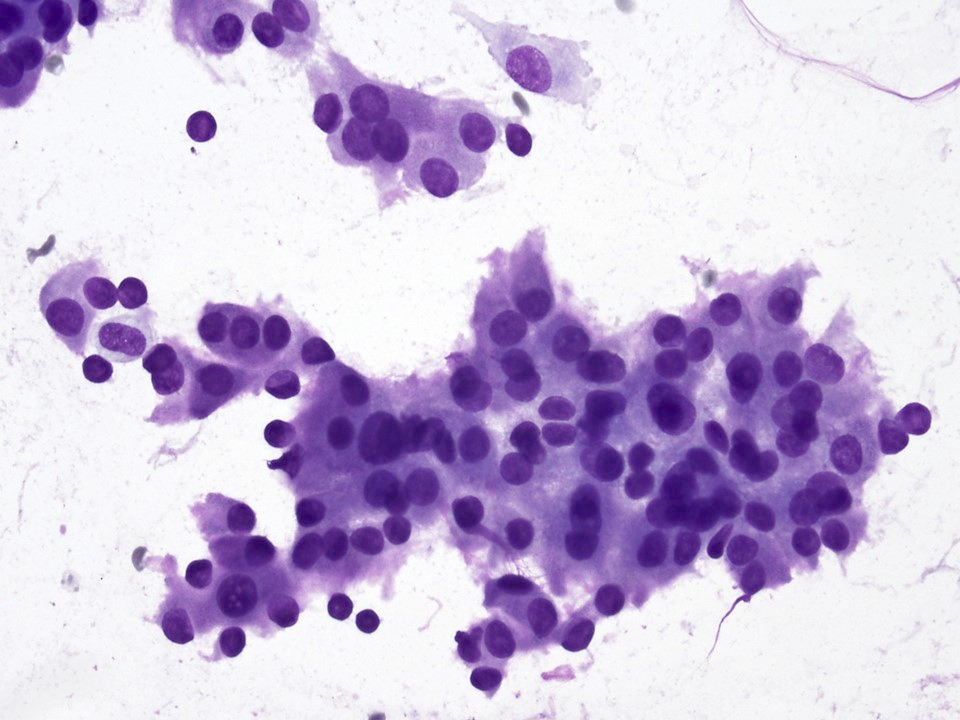
Neoplastic cells in sheets
Keratinizing cells
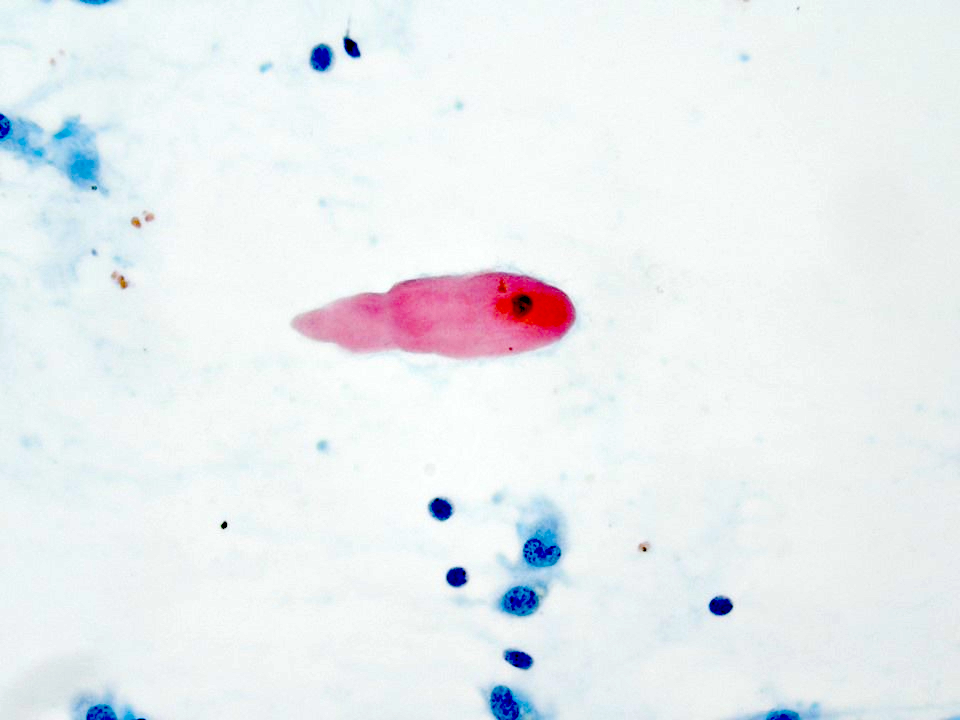
Single keratinizing cells
Crowded squamous cells
Images hosted on other servers:


Low grade and oncocytic tumors
Positive stains
- Pancytokeratin, CK5/6, p63, p40, EMA, CK7, CK14
- Membrane bound mucins: MUC1, MUC2, MUC4, MUC5AC and MUC5B
- Mucocytes: mucin positive for mucicarmine and PASD (diastase resistant) stains
- Reference: J Stomatol Oral Maxillofac Surg 2020;121:713
Negative stains
- S100, GFAP, calponin, muscle specific actin, androgen receptor, HER2, DOG1, CK20 (Arch Pathol Lab Med 2015;139:55)
- SOX10: rare cases may be positive (Hum Pathol 2016;56:134)
- Mammaglobin: some cases may show positive cells (Hum Pathol 2016;56:134)
- GATA3: occasional cells may be positive (Hum Pathol 2016;56:134)
Electron microscopy description
- Epidermoid cells attached to each other with desmosomes and mucus cells showing mucous globules with stellate mucoid material (Oral Surg Oral Med Oral Pathol 1979;47:247)
Molecular / cytogenetics description
- t(11;19)(q14-21;p12-13) with CRTC1(MECT1)-MAML2 fusion (Nat Genet 2003;33:208)
- Present in 80% of mucoepidermoid carcinoma (Am J Surg Pathol 2016;40:1151)
- Low to intermediate grade (78%), high grade (84%) (Am J Surg Pathol 2016;40:1151)
- Detected by fluorescence in situ hybridization (FISH) or RT-PCR (Am J Surg Pathol 2019;43:885)
Molecular / cytogenetics images
Images hosted on other servers:

FISH analysis of MAML2
Sample pathology report
- Parotid gland, right, parotidectomy:
- Mucoepidermoid carcinoma, intermediate grade (2.3 cm)
- The tumor is confined to the parotid gland.
- No lymphovascular or perineural invasion is identified.
- Three lymph nodes, negative for carcinoma (0/3).
- Surgical margins negative for carcinoma.
- Carcinoma 0.3 cm of closest margin, medial.
- See synoptic report.
Differential diagnosis
- For low to intermediate grade tumors:
- Necrotizing sialometaplasia (Acta Otorrinolaringol Esp 2020;71:328):
- Lobular pattern, lacks cystic pattern, no intermediate cells
- Pleomorphic adenoma with squamous and mucinous cell metaplasia (J Oral Maxillofac Pathol 2018;22:S69):
- Composed of epithelial and myoepithelial cells and extracellular matrix material
- Warthin tumor with squamous metaplasia (J Med Case Rep 2019;13:12):
- Lacks the translocations seen in mucoepidermoid carcinoma
- Shows bilayered oncocytic epithelium
- Acinic cell carcinoma (Eur Arch Otorhinolaryngol 2016;273:3511):
- Mammary analogue secretory carcinoma (MASC) (Bosn J Basic Med Sci 2016;16:237):
- S100 positive
- Necrotizing sialometaplasia (Acta Otorrinolaringol Esp 2020;71:328):
- For high grade tumors:
- Squamous cell carcinoma (primary or secondary) (J Cancer Res Ther 2015;11:664):
- Shows keratinization and intercellular bridges
- Lacks intermediate cells and mucocytes
- Salivary duct carcinoma (Head Neck Pathol 2017;11:288):
- GATA3, HER2 and androgen receptor positive
- Shows a Roman bridge pattern, comedonecrosis
- Squamous cell carcinoma (primary or secondary) (J Cancer Res Ther 2015;11:664):
Additional references
Practice question #1
Which of the following is true about mucoepidermoid carcinoma?
- Associated with t(12;15)(p12;q25) and ETV6-NTRK3 gene fusion
- Highly associated with smoking
- Most common malignant salivary tumor in children
- Positive for HER2 and AR by immunohistochemistry
- Prognosis is poor regardlesss of histologic grade
Practice answer #1
C. Most common malignant salivary tumor in children
Comment Here
Reference: Mucoepidermoid carcinoma
Comment Here
Reference: Mucoepidermoid carcinoma
Practice question #2
Which of the following histologic features is more commonly seen in low to intermediate grade mucoepidermoid carcinoma?
- 4 or more mitoses
- Bone invasion
- Intracystic component more than 30%
- Necrosis
- Perineural invasion
Practice answer #2
Practice question #3

The focal clear cell change seen in this mucoepidermoid carcinoma case is due to
- Accumulation of glycogen
- Accumulation of mucin
- Degradation of neoplastic cells
- Fixation artifact
- High grade transformation
Practice answer #3
