Thyroid & parathyroid
Cytology
Bethesda system
Benign
Author: Ayana Suzuki, Ph.D.
Editorial Board Member: Marc Pusztaszeri, M.D.
Deputy Editor-in-Chief: Andrey Bychkov, M.D., Ph.D.

Last author update: 3 June 2025
Last staff update: 3 June 2025
Copyright: 2014-2025, PathologyOutlines.com, Inc.
PubMed Search: Bethesda guidelines thyroid benign
Table of Contents
Definition / general | Essential features | Terminology | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Cytology description | Cytology images | Videos | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Suzuki A. Benign. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/thyroidbenign.html. Accessed August 18th, 2025.
Definition / general
- Cytologic sample that is adequate for evaluation and consists of colloid and benign appearing follicular cells in varying proportions (Ali: The Bethesda System for Reporting Thyroid Cytopathology, 3rd Edition, 2023)
- Most common fine needle aspiration (FNA) interpretation (60 - 70% of all cases) (Clin Lab Med 1993;13:699, Cancer 2007;111:508)
- Thyroid follicular nodular disease is the most common lesion, followed by chronic thyroiditis
- ~10 - 20% of patients with benign cytology require surgery due to clinical indications (large goiter, suspicious sonogram, rapid growth, coexistent nodule, etc.) and cosmetic reasons (Diagn Cytopathol 2000;23:233)
- Primary benefit of thyroid FNA is ability to reliably make a benign diagnosis, which spares many patients with nodular thyroid disease from unnecessary surgery (Ali: The Bethesda System for Reporting Thyroid Cytopathology, 3rd Edition, 2023)
Essential features
- Cytologic sample that is adequate for evaluation and consists of colloid and benign appearing follicular cells
- 60 - 70% of all thyroid FNA, resection rate 10 - 20%, risk of malignancy (ROM) 0 - 3%
- Role of benign diagnosis is to avoid unnecessary surgery
Terminology
- Negative for malignancy (noncancerous cells found) and nonneoplastic (no abnormal tissue growth)
- Term benign is preferred over negative for malignancy and nonneoplastic
- Category II in the Bethesda system
Radiology description
- Thyroid follicular nodular disease: multinodular goiter on ultrasound
- Chronic lymphocytic (Hashimoto) thyroiditis: heterogeneous appearance on ultrasound
Radiology images
Contributed by Ayana Suzuki, C.T.
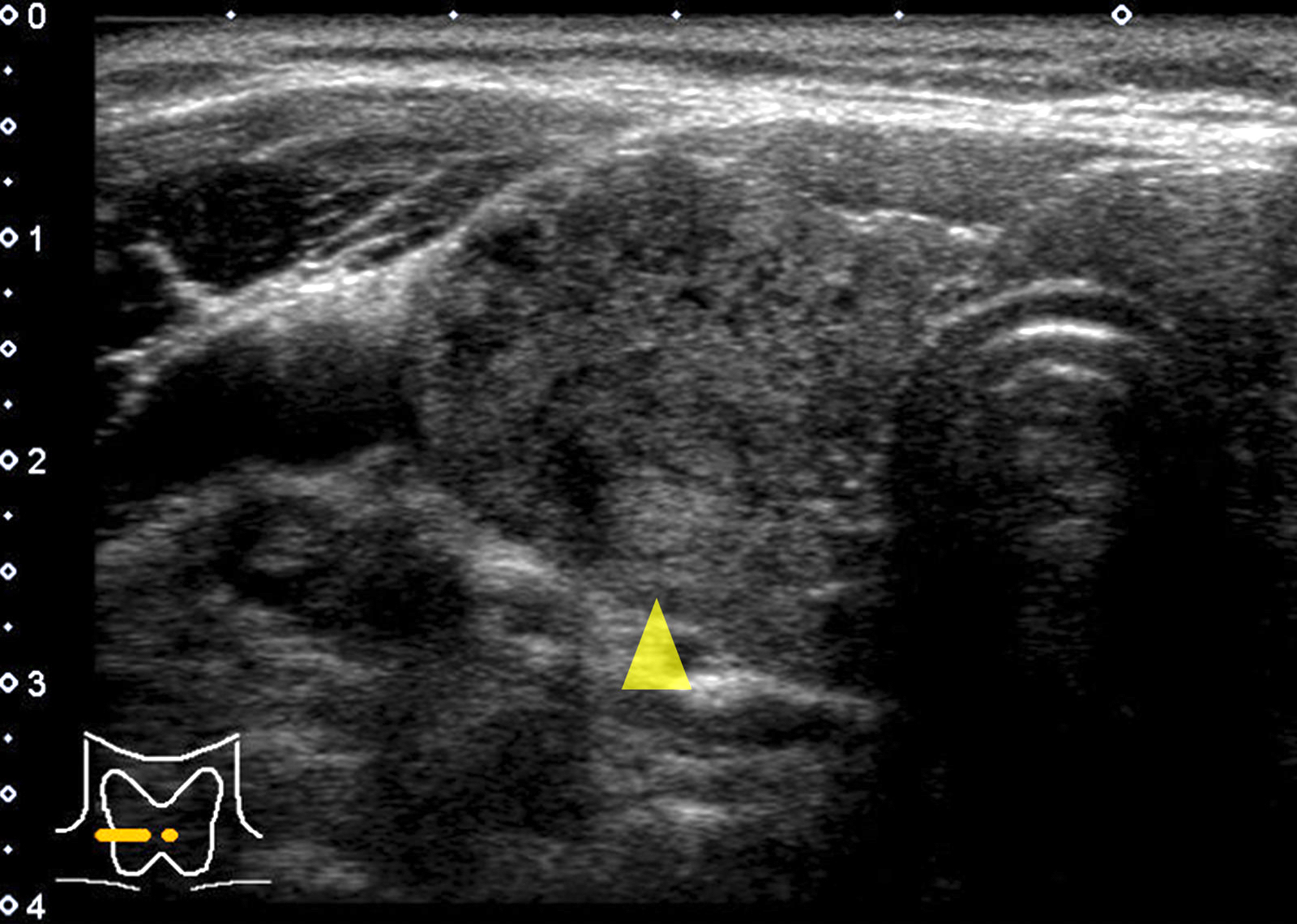
Isoechoic nodule
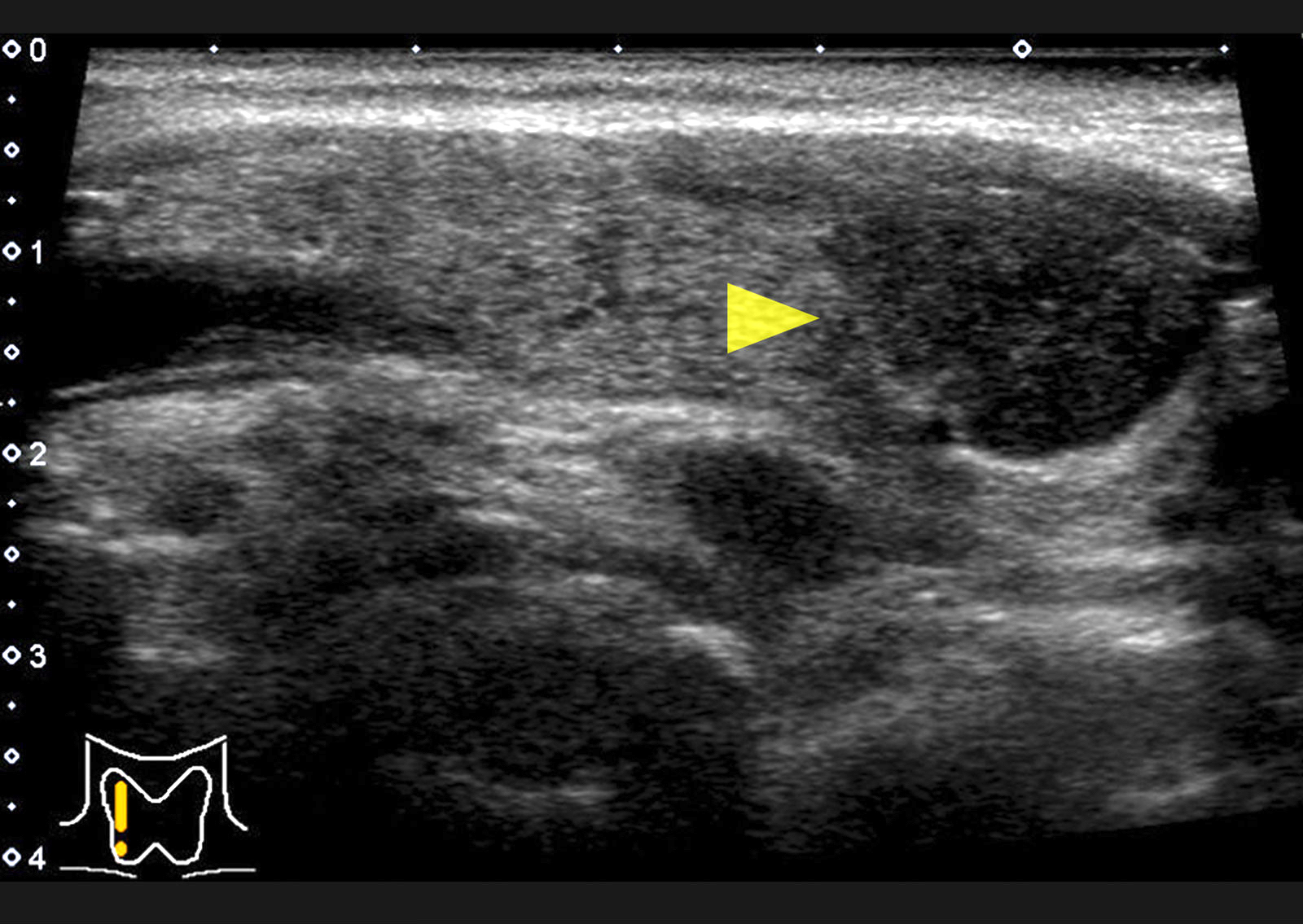
Hypoechoic nodule
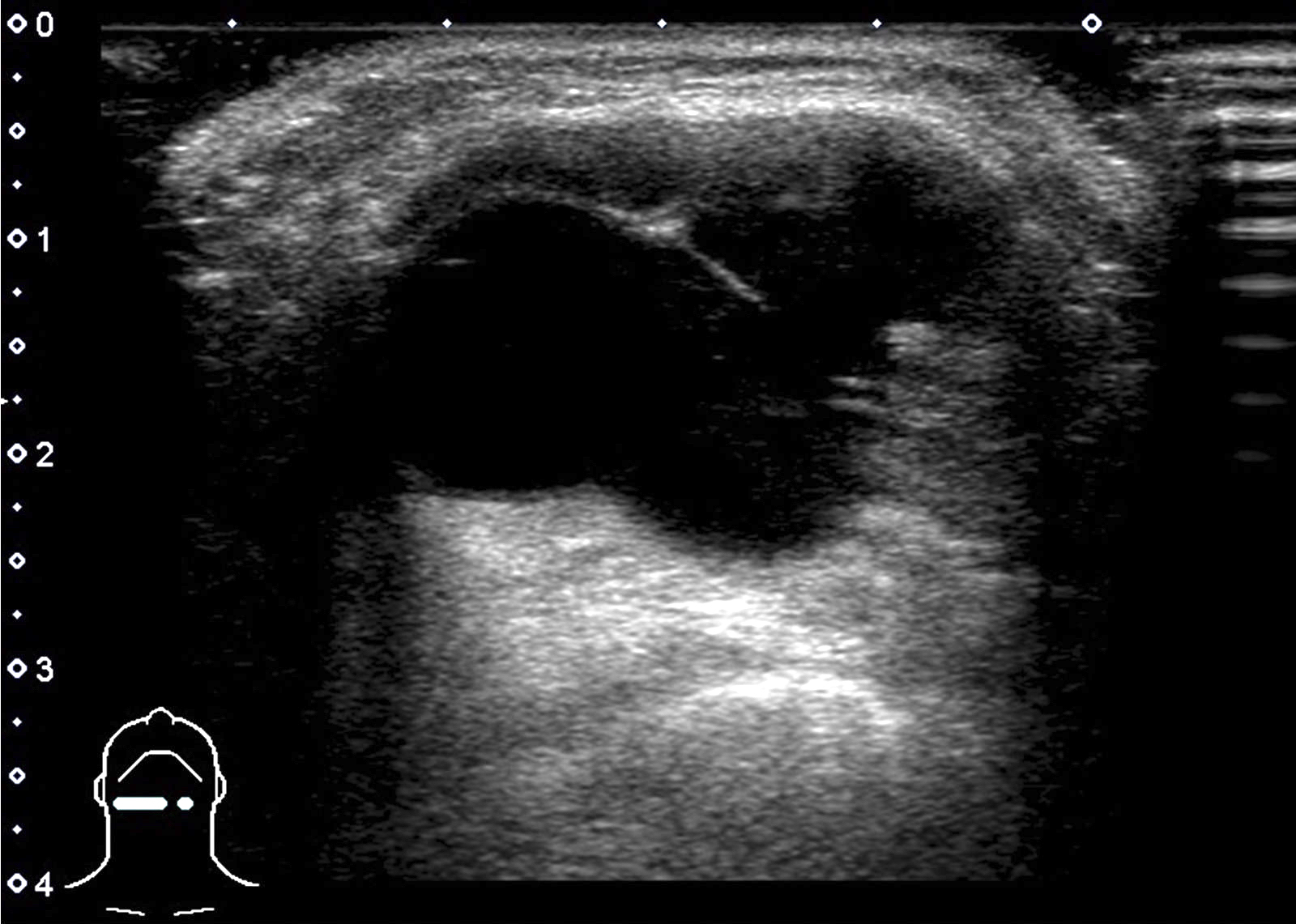
Large cyst
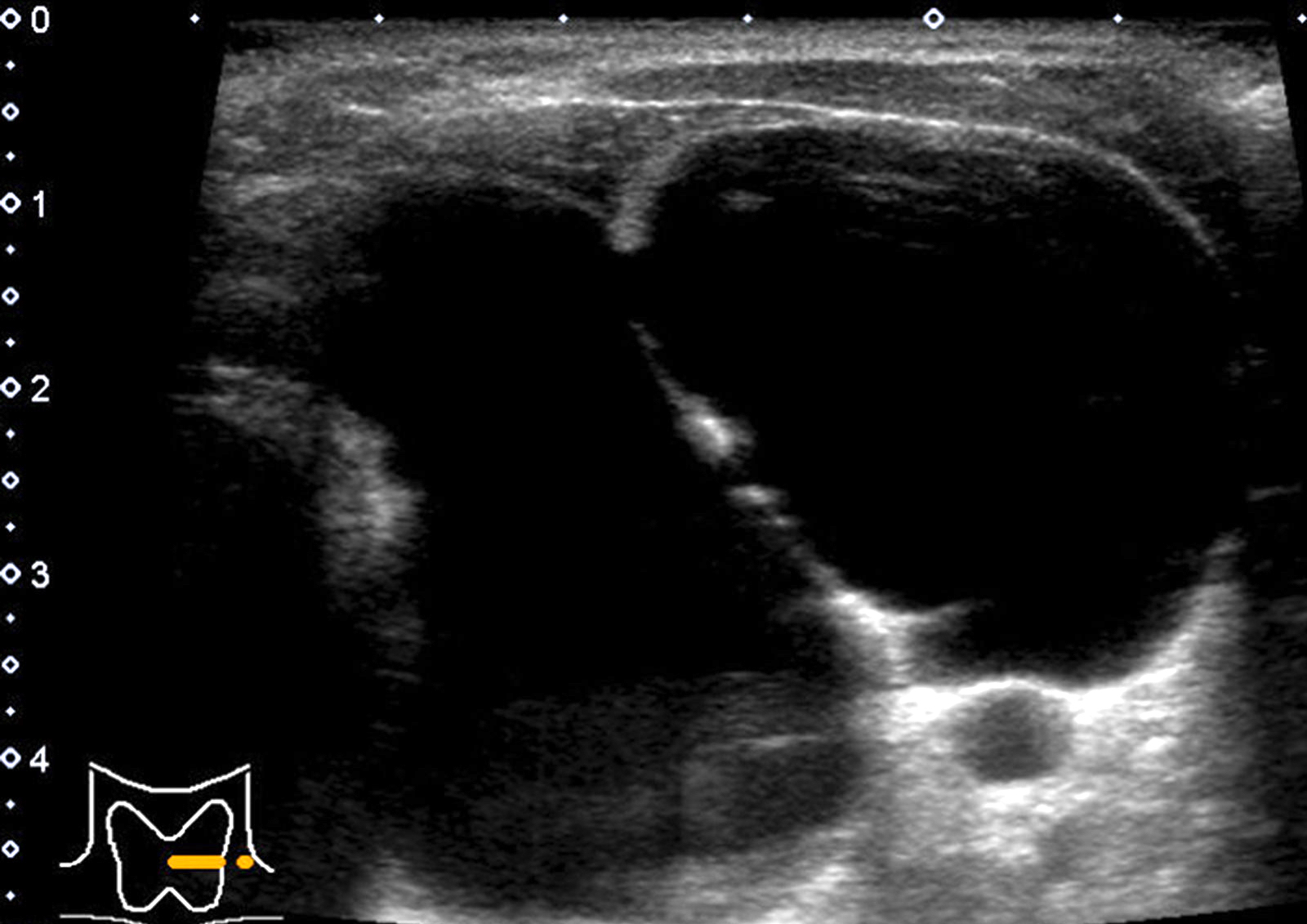
Large multilocular cyst
Prognostic factors
- 0 - 3% of cytologically proven benign thyroid nodules have a malignancy on resection; usually these nodules are clinically suspicious (Endocr Pract 2001;7:237, JAMA 2015;313:926, Thyroid 2007;17:1061)
Case reports
- 35 year old woman with IgG4 related thyroiditis (Korean J Intern Med 2016;31:399)
- 35 year old woman with microfilaria in aspirated thyroid nodule (Ci Ji Yi Xue Za Zhi 2016;28:27)
- 46 year old woman with Hashimoto thyroiditis associated with oncocytic adenoma (Rom J Morphol Embryol 2017;58:241)
- 48 year old woman with subacute thyroiditis mimicking malignancy (Diagn Cytopathol 2016;44:682)
- 69 year old man with acute exacerbation of Hashimoto thyroiditis mimicking anaplastic carcinoma (Ear Nose Throat J 2014;93:E18)
- 79 year old man with Riedel thyroiditis (Diagn Cytopathol 2019;47:512)
- 80 year old woman with acute suppurative thyroiditis (Clin Case Rep 2017;5:1238)
Treatment
- American Thyroid Association (ATA) recommends that followup should be determined by risk stratification based on ultrasound pattern
(Thyroid 2016;26:1)
- High suspicion: repeat ultrasound and FNA within 12 months
- Low to intermediate suspicion: repeat ultrasound 12 - 24 months → growth or development of new suspicious ultrasound features → repeat FNA
- Very low suspicion: ultrasound surveillance is not necessary; if ultrasound is repeated, it should be done after 24 months
- Repeat FNA or surgery is considered only for a selected subset including those that are large, symptomatic or have worrisome clinical or sonographic characteristics (Thyroid 2016;26:1)
Cytology description
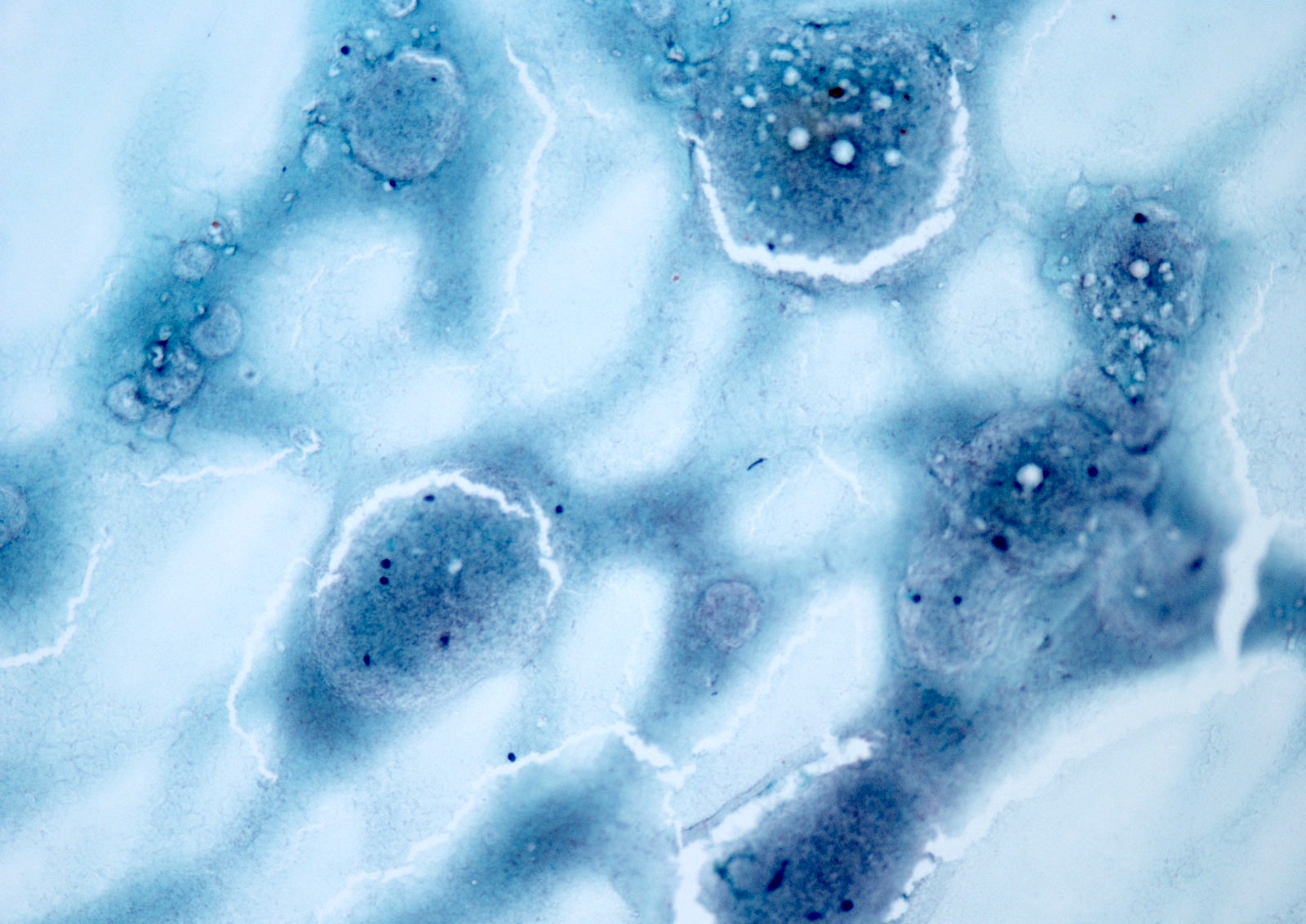
- Thyroid follicular nodular disease
- Adequate, consists of colloid and benign appearing follicular cells
- Cellularity: sparse to moderate
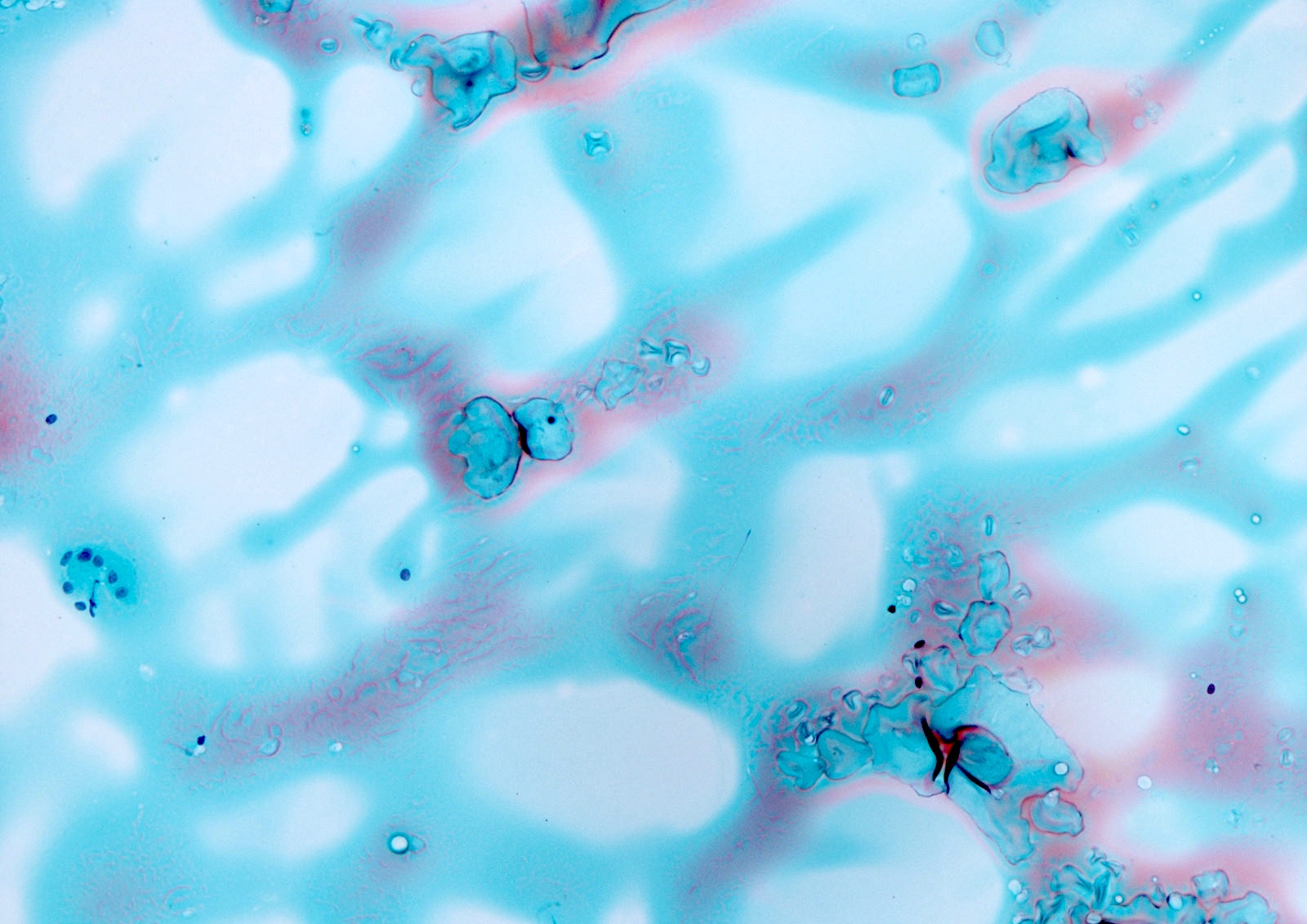
- Colloid: viscous, shiny, light yellow or gold (gross), dark blue-violet-magenta (Romanowsky stain), green or
orange-pink (Pap stain)
- Watery colloid: cellophane coating, film with frequent folds (crazy pavement, chicken wire or mosaic appearance)
- Thick (dense, hard) colloid: a hyaline quality, cracks
- Macrophages: common, containing hemosiderin pigment
- Follicular cells
- Appearance: monolayered sheets, spaces (honeycomb-like) within the sheets, intact 3D variably sized balls
- Cytoplasm: scant or moderate, stripped (may be misinterpreted as lymphocytes), paravacuolar granules (Cancer 2003;99:217)
- Nuclei: variable in size, low N:C ratio, round to oval, anisonucleosis, uniformly granular chromatin pattern
- In abundant colloid: shrunken, spindled, degenerated
- In cystic lesion: focal reparative changes (cyst lining cells with enlarged nuclei, finely granular chromatin, squamoid or spindle shaped appearance)
- Minor components: oncocytes, microfollicles, papillary hyperplasia (Cancer 2003;99:217, Cancer Cytopathol 2014;122:666)
- Liquid based cytology (LBC): decrease in the amount of colloid, superior nuclear details
- Graves disease
- Features similar to non-Graves benign follicular nodules (Acta Med Scand 1979;205:263)
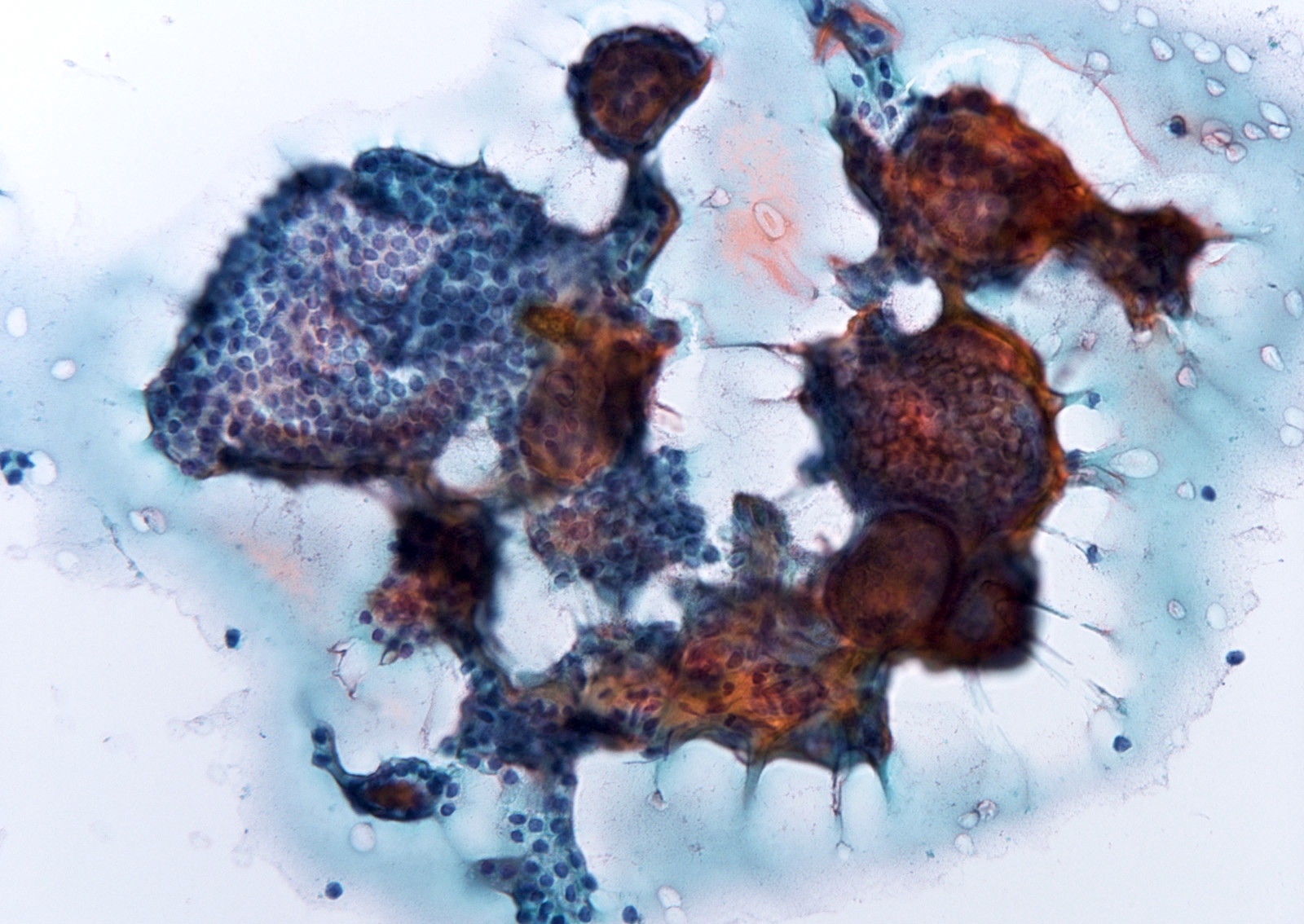
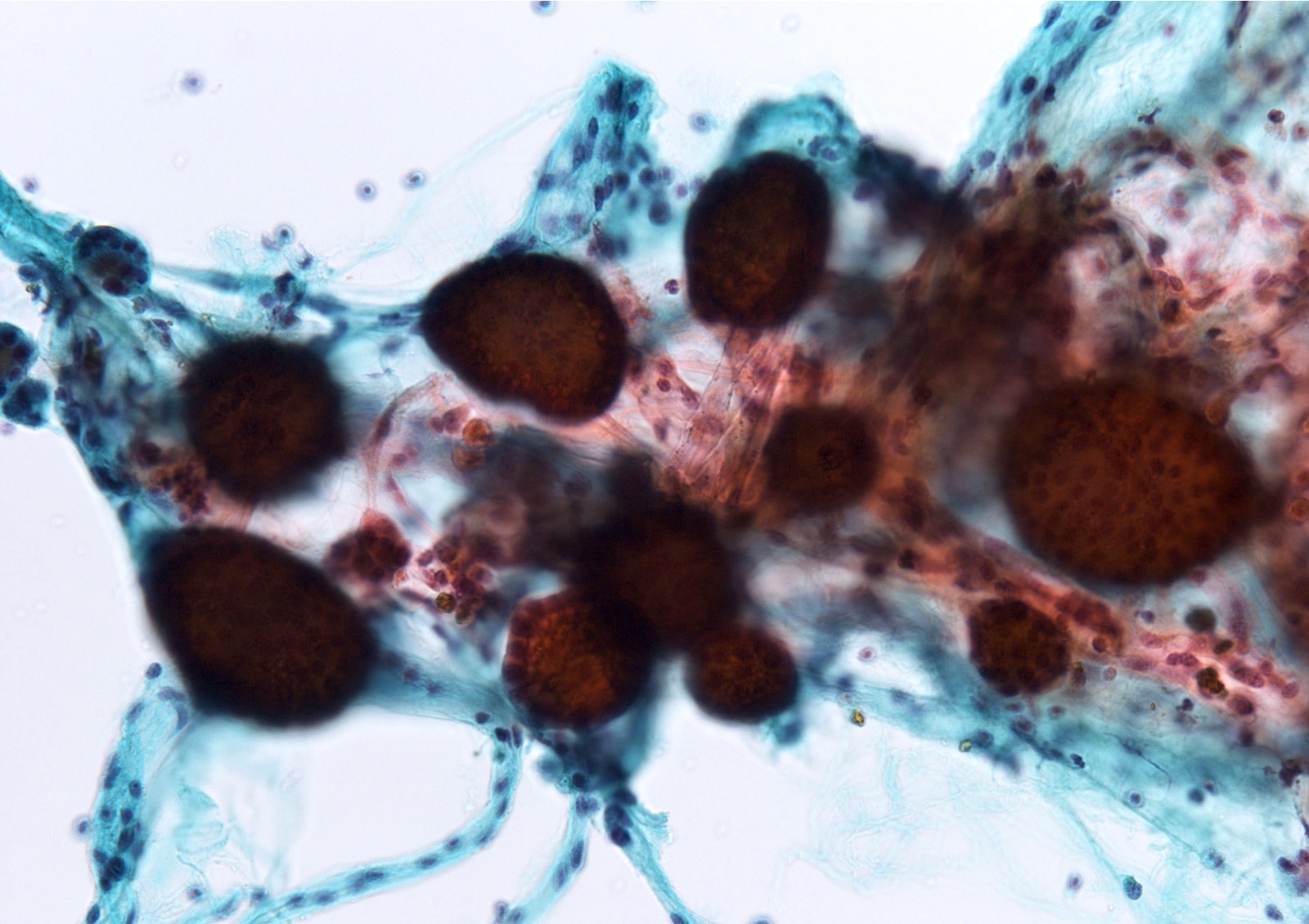
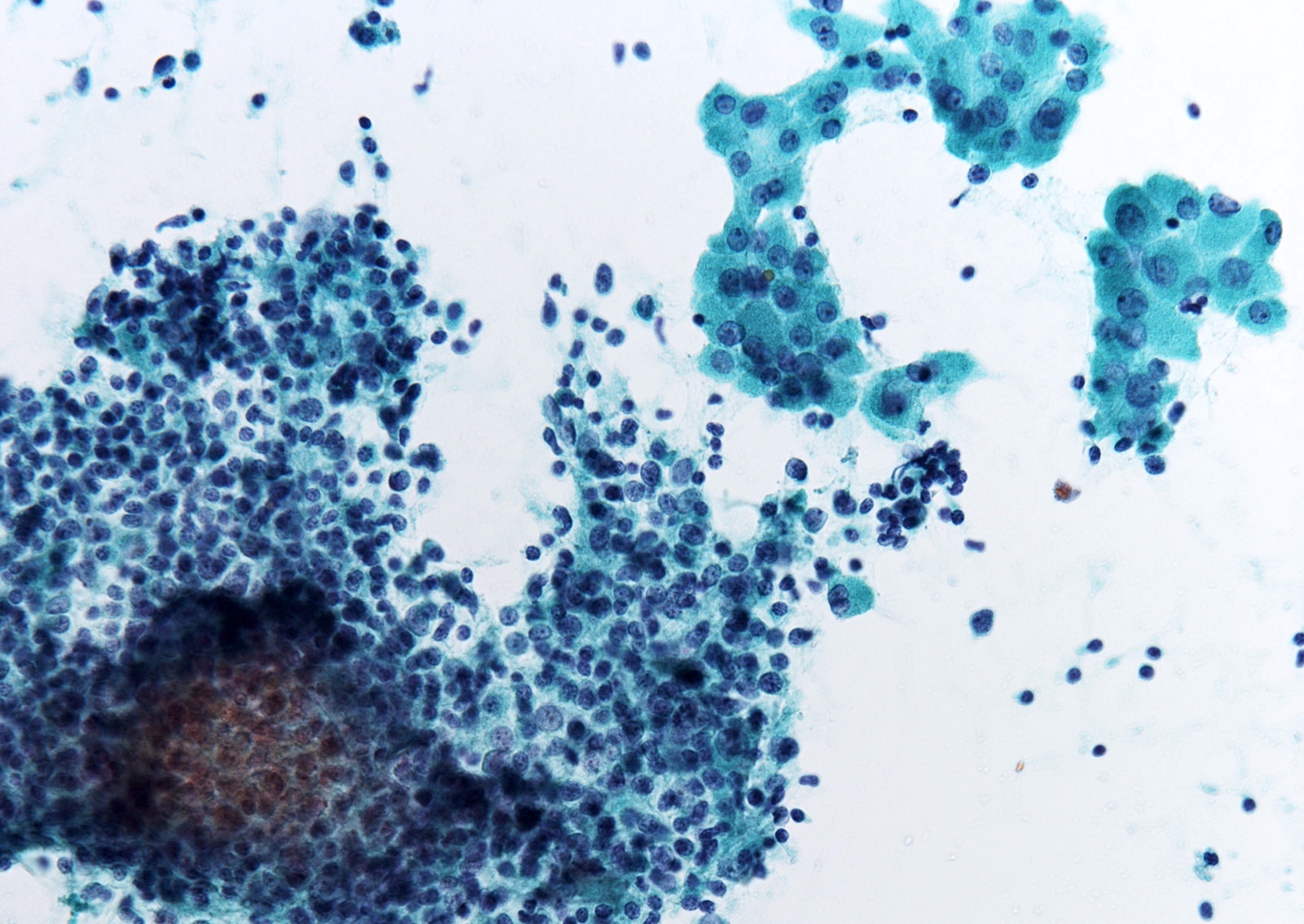
- Lymphocytic thyroiditis (Hashimoto thyroiditis)
- Many polymorphic lymphoid cells associated with benign thyroid follicular cells or oncocytes (Acta Cytol 1987;31:687)
- Oncocytes: flat sheets or isolated, abundant granular cytoplasm, large nuclei, prominent nucleoli, anisonucleosis, mild nuclear atypia (Acta Cytol 1999;43:400)
- Lymphocytes: background or infiltrating epithelial cell groups, polymorphic (small mature lymphocytes, larger reactive lymphoid cells, occasional plasma cells), variable chromatin pattern (rich and granular heterochromatin in small lymphocytes, diminished and fine in large lymphocytes)
- Monomorphic lymphoid population should prompt additional samples for flow cytometry if lymphoma suspected
- LBC: decrease in lymphocytes, oncocytes with irregular nuclei (Acta Cytol 2018;62:93, Diagn Cytopathol 2012;40:404)
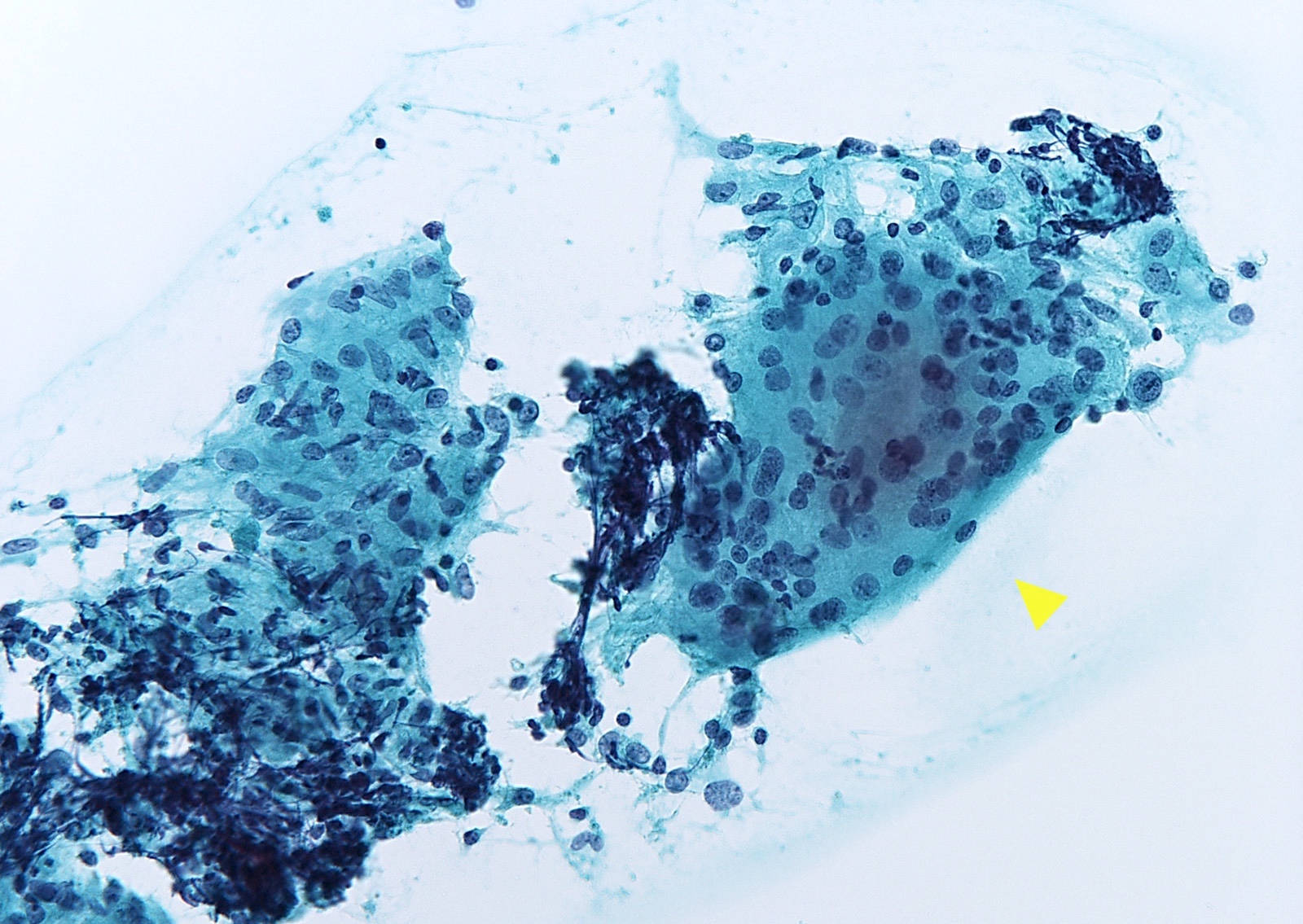
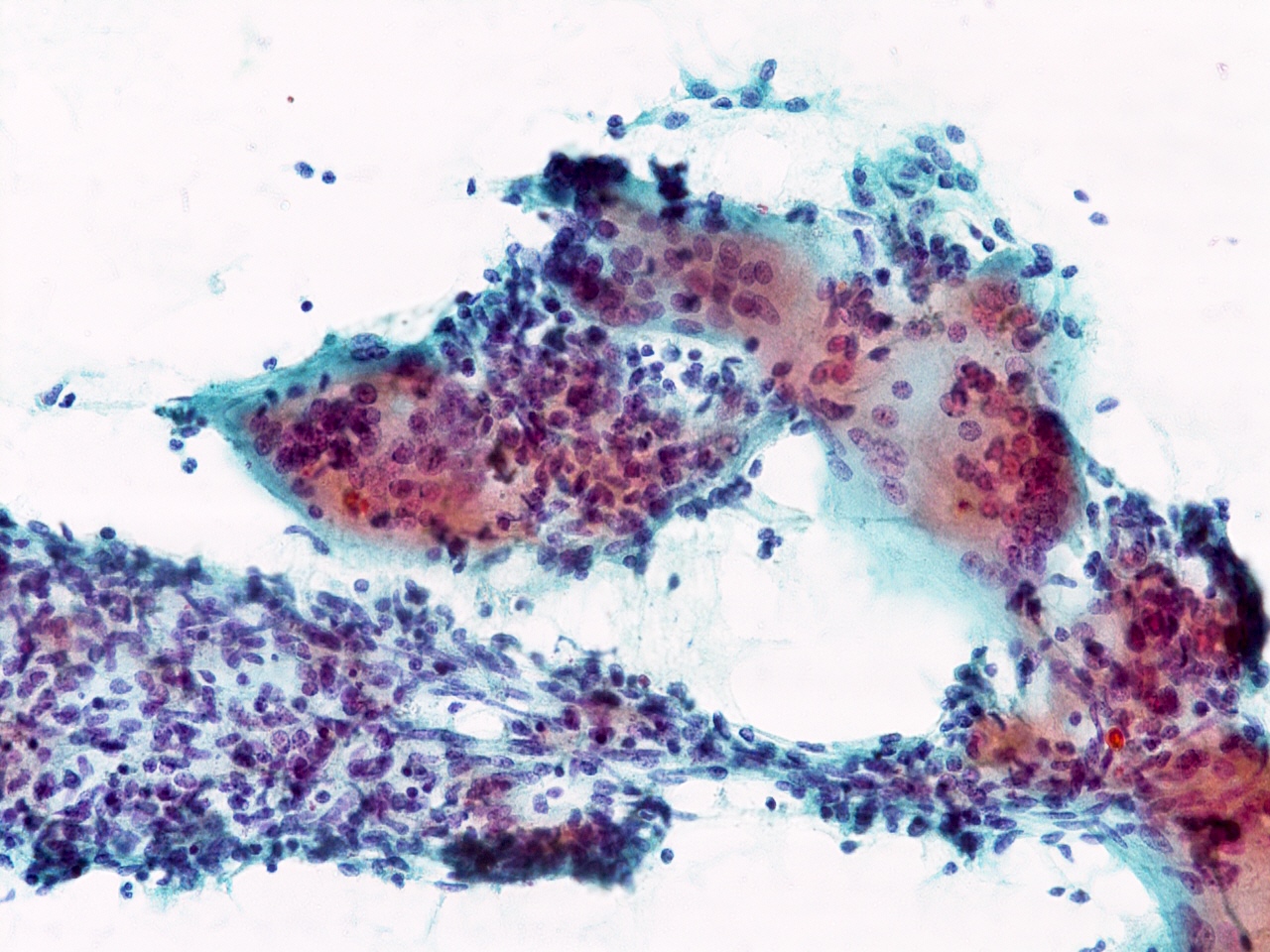
- Granulomatous (de Quervain) thyroiditis (Acta Cytol 1997;41:238)
- Cellularity: variable (depends on the stage of disease)
- Granulomas: clusters of epithelioid histiocytes, numerous multinucleated giant cells
- Early stage: many neutrophils and eosinophils, similar to acute thyroiditis
- Later stage: hypocellular, giant cells surrounding and engulfing colloid, epithelioid cells, lymphocytes, macrophages, scant degenerated follicular cells
- Involutional stage: absent giant cells and inflammatory cells
- Acute thyroiditis (Exp Ther Med 2015;9:860)
- Numerous neutrophils associated with necrosis, fibrin, macrophages, blood
- Scant reactive follicular cells and limited to absent colloid
- Bacterial or fungal organisms (immunocompromised patients)
- Riedel thyroiditis (Diagn Cytopathol 2004;30:193)
- Cellularity: acellular
- Collagen strands and bland spindle cells
- Rare chronic inflammatory cells, absence of colloid and follicular cells
- Black thyroid (Diagn Cytopathol 1991;7:640, Diagn Cytopathol 2006;34:106)
- Follicular cells with abundant dark brown cytoplasmic pigment (darker than hemosiderin, similar to melanin)
- Amyloid goiter
- Abundant purple to pink-orange amorphous material (Cytopathology 2006;17:262)
Cytology images
Contributed by Ayana Suzuki, C.T.
Colloid nodule
Adenomatous nodule

Adenomatous nodule
Hashimoto thyroiditis
Granulomatous thyroiditis

Thyroglossal duct cyst
Videos
Thyroid cytology: colloid nodule
Essential thyroid cytopathology
How to observe thyroid FNA
Differential diagnosis
- Differential with benign follicular nodule (Kini: Color Atlas of Differential Diagnosis in Exfoliative and Aspiration Cytopathology, 2nd Edition, 2011)
- Follicular neoplasm:
- Background: clean, sometimes hyaline colloid
- Follicular pattern: small, uniform
- Cytoplasm and nuclei: uniform, high N:C ratio, enlarged nuclei
- Oncocytic follicular neoplasm:
- Background: clean, sometimes cystic
- Presentation: isolated, in loosely cohesive groups, sheets, syncytial tissue fragments
- Cytoplasm and nuclei: uniform, high N:C ratio, enlarged nuclei, binucleation to multinucleation
- Papillary thyroid carcinoma:
- Nuclear pseudoinclusions (Orphan Annie nuclei)
- Follicular neoplasm:
- Differential with lymphocytic thyroiditis
- Papillary thyroid carcinoma:
- Nuclear pseudoinclusions (Orphan Annie nuclei)
- Oncocytic follicular neoplasm:
- Background: clean, sometimes cystic
- MALT lymphoma:
- Lymphoglandular bodies in the background (Acta Cytol 2018;62:93)
- Similar chromatin pattern of lymphoid cells regardless of the difference in size
- Absence of oncocytic cells (Acta Cytol 2018;62:93)
- Papillary thyroid carcinoma:
- Differential with granulomatous thyroiditis
- Papillary thyroid carcinoma:
- Nuclear pseudoinclusions (Orphan Annie nuclei) can mimic macrophages with enlarged nuclei, nuclear irregularity
- Lymphocytic thyroiditis:
- Absence of epithelioid histiocytes
- Papillary thyroid carcinoma:
- Differential with acute thyroiditis
- Anaplastic carcinoma:
- Carefully observe whether large atypical cells are present or absent
- Anaplastic carcinoma:
- Differential with thyroid cyst
- Thyroglossal duct cyst (Thyroid Res & Prac 2013;10:104):
- Cytology: proteinaceous material, inflammatory cells, rare degenerated squamous or ciliated columnar cells
- Appropriate clinical presentation (anterior midline neck cyst, above the thyroid isthmus, below the hyoid bone)
- Parathyroid cyst (Case Rep Surg 2015;2015:243527):
- Cyst fluid: characteristic watery, clear gross appearance
- Cytology: acellular or hypocellular
- Preoperative diagnosis: elevated parathyroid hormone levels in the cyst fluid
- Thyroglossal duct cyst (Thyroid Res & Prac 2013;10:104):
Practice question #1
What risk of malignancy is associated with benign thyroid cytology?
- 0 - 3%
- 5 - 10%
- 12 - 15%
- 20 - 30%
- 40 - 50%
Practice answer #1
A. 0 - 3% Most published studies reported that a benign FNA diagnosis is associated with a very low false negative rate, estimated
to be in the range of 0 - 3%. It should be noted that the precise risk of malignancy for cytologically benign nodules is
difficult to assess because only a minority of these patients undergo surgery. Answers B - E are incorrect because they overestimate or exaggerate the risk of malignancy associated with benign thyroid cytology.
Comment Here
Reference: Benign
Comment Here
Reference: Benign
Practice question #2
What is the most likely histological diagnosis of this thyroid aspirate consistent with benign category?
- Acute thyroiditis
- Follicular nodular disease
- Granulomatous thyroiditis
- Lymphocytic thyroiditis
- Riedel thyroiditis
Practice answer #2
C. Granulomatous thyroiditis. The absence of colloid and follicular cells in the background and the presence of multinucleated giant cells, lymphocytes and epithelioid cells suggest granulomatous thyroiditis.
Answer B is incorrect because follicular nodular disease shows colloid and foam cells in the background. Answer D is incorrect because lymphocytic thyroiditis shows lymphocytes and oncocytes. Answer A is incorrect because acute thyroiditis shows numerous neutrophils. Answer E is incorrect because in Riedel thyroiditis, few cells are aspirated.
Comment Here
Reference: Benign
Comment Here
Reference: Benign
