

Lung
Sarcomatoid carcinoma
Pulmonary blastoma
Editorial Board Member: Jefree J. Schulte, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 4 November 2022
Last staff update: 4 November 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Pulmonary blastoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gui H, Lamzabi I. Pulmonary blastoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumorpulmonaryblastoma.html. Accessed April 26th, 2024.
Definition / general
- Rare lung malignancy, 0.25 - 1% of lung cancers
- Biphasic components with admixed epithelium and primitive stroma
- Highly aggressive type of sarcomatoid carcinomas (BMC Res Notes 2014;7:294)
Essential features
- Peripheral solitary large mass, well circumscribed, unencapsulated
- Well differentiated glandular component and blastematous stroma
Terminology
- Separated from fetal adenocarcinoma (epithelium only) and pleuropulmonary blastoma (mesenchymal only)
ICD coding
- ICD-O: 8972/3 - pulmonary blastoma
Epidemiology
- Most common in fifth decade
- M:F = 1:1
- References: Lung Cancer 2011;73:127, Adv Respir Med 2021;89:511
Sites
- All lobes can be affected with upper lobe predominance (Lung Cancer 2011;73:127)
Pathophysiology
- Both components derived from single pluripotent cell clone (Lung Cancer 2011;73:127)
- TP53 and CTNNB1 mutations detected (Hum Pathol 1996;27:1117, Am J Surg Pathol 2004;28:921)
- Rare mutations such as EGFR, MET, BRAF and DICER1 mutation detected (Onco Targets Ther 2016;9:6915, Eur Respir J 2016;47:1879)
Etiology
- 80% associated with smoking (BMC Res Notes 2014;7:294)
Clinical features
- Nonspecific, 40% asymptomatic (Cancer 1991;67:2368)
Diagnosis
- Relies on tissue histology and IHC on biopsy or surgical resection
- Preoperative biopsy shows cytology of 2 cell patterns
- References: Lung Cancer 2011;73:127, Adv Respir Med 2021;89:511
Radiology description
- Large solitary peripheral mass with variable enhancement and necrosis (Lung Cancer 2011;73:127)
- 25% endobronchial growth (Respir Med 2006;100:1174)
Radiology images
Images hosted on other servers:

Mass near hilum

Compression of vena cava

Uptake within mass

Right mass
Prognostic factors
- Poor prognosis, 5 year survival 16% (Lung Cancer 2011;73:127)
- Poor prognostic factors: tumor recurrence, metastasis at initial presentation and size > 5 cm (Lung Cancer 2011;73:127)
Case reports
- 16 year old girl with a large, well defined, heterogeneously enhancing mass measuring 11 cm in right upper lobe (Case Rep Med 2012;2012:471613)
- 66 year old woman with smoking history presented with a mass in the posteromedial left hemithorax measuring 16 cm (Ann Thorac Surg 2019;107:e345)
- 67 year old male smoker with 9 cm necrotic mass from apical segments of right lower lobe (BMC Res Notes 2014;7:294)
- 68 year old man with tumor of 5.5 cm in the left upper lobe of the lung (Case Rep Oncol Med 2015;2015:842621)
- 71 year old female past smoker with 7 cm tumor in lower lobe (Crit Rev Oncol Hematol 2018;125:48)
Treatment
- Surgical resection (Lung Cancer 2011;73:127)
- Chemoradiation and neoadjuvant therapy have limited responses in a few cases (Lung Cancer 2011;73:127)
- Adjuvant chemotherapy cisplatin combined with etoposide may improve survival (Cureus 2018;10:e3586, Cancer 1998;82:462)
- Multikinase inhibitor reported having good response in case report (J Int Med Res 2020;48:300060520962394)
Gross description
- Mostly peripheral, large, well circumscribed, unencapsulated mass, average 9.1 cm (Lung Cancer 2011;73:127)
- Lobulated with cystic, necrotic and hemorrhagic degeneration
Gross images
Images hosted on other servers:

Solid mass

Hemorrhagic mass
Microscopic (histologic) description
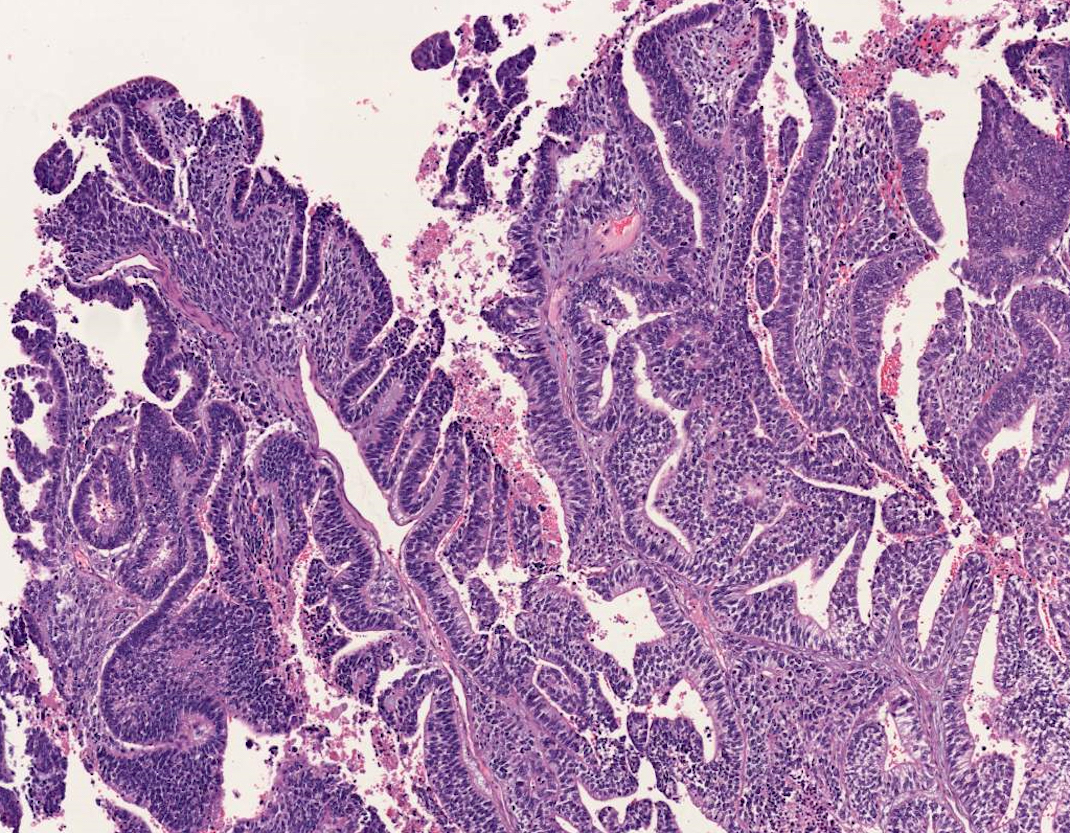
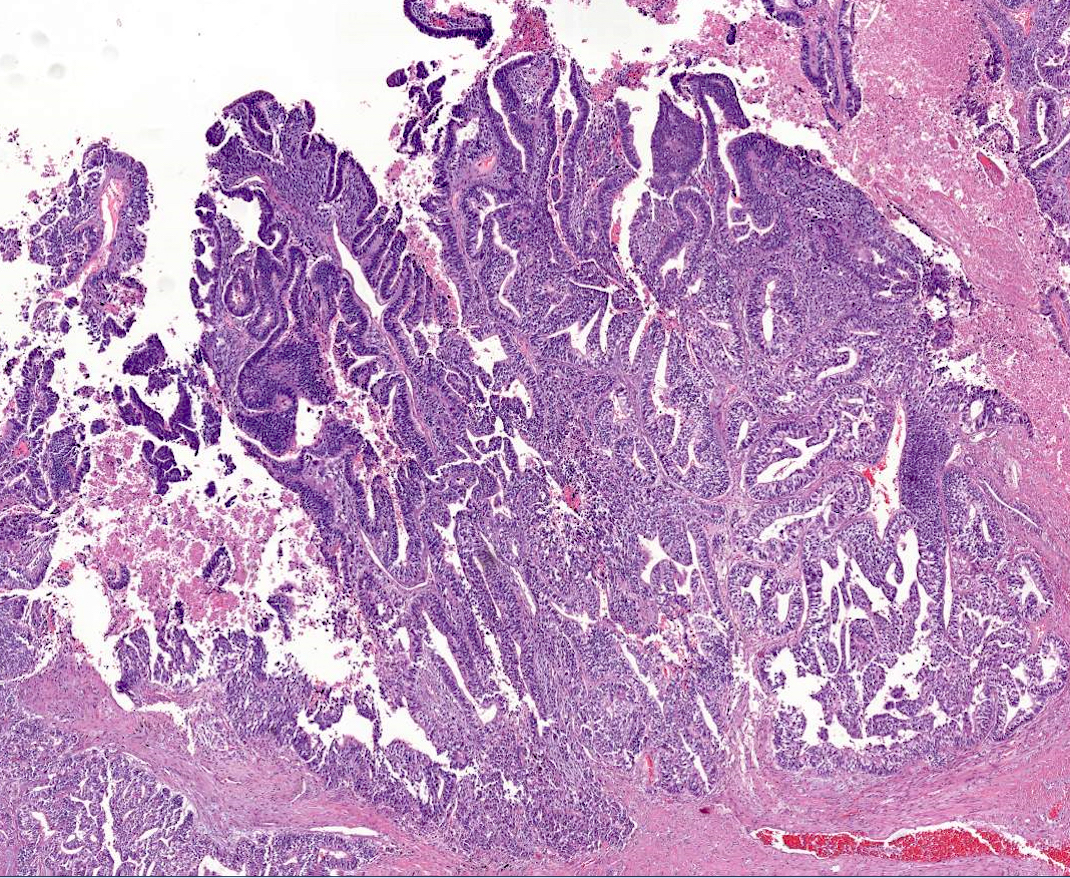
- Glandular branching tubules resembling fetal lung, lined by pseudostratified columnar cells with subnuclear and supranuclear glycogen vacuoles and little nuclear atypia (Lung Cancer 2011;73:127)
- Loose undifferentiated mesenchymal stroma with variable cellular atypia, possible heterologous differentiation (skeletal muscle, cartilage and bone) (Lung Cancer 2011;73:127)
- Morules and neuroendocrine cells in 67% of cases (Cancer 1991;67:2368)
- May have germ cell tumor or melanoma component (J Thorac Oncol 2008;3:1185, Arch Pathol Lab Med 1990;114:1076)
Microscopic (histologic) images
Contributed by Hongxing Gui, M.D., Ph.D. and University of Michigan Virtual Slide Box
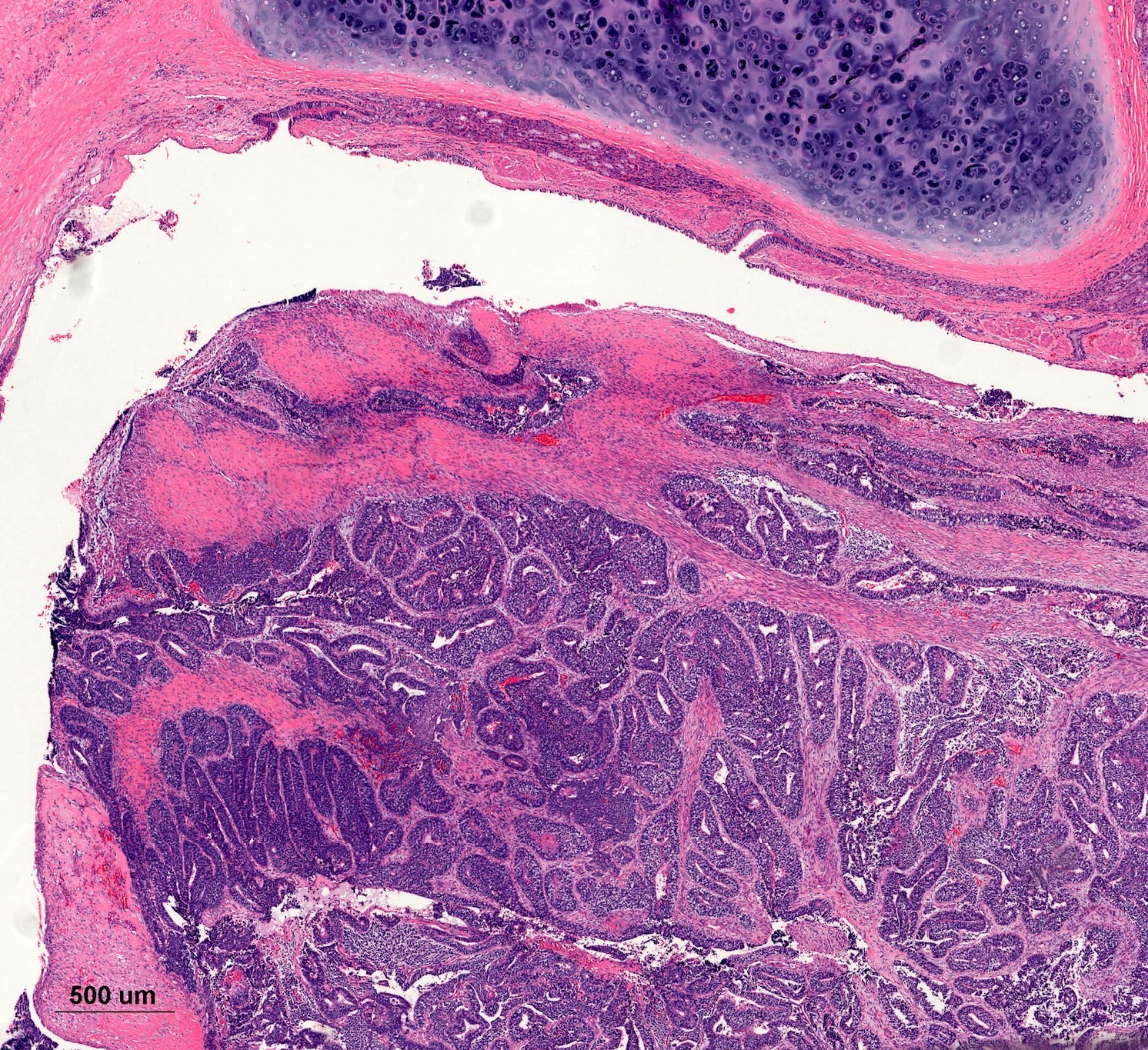
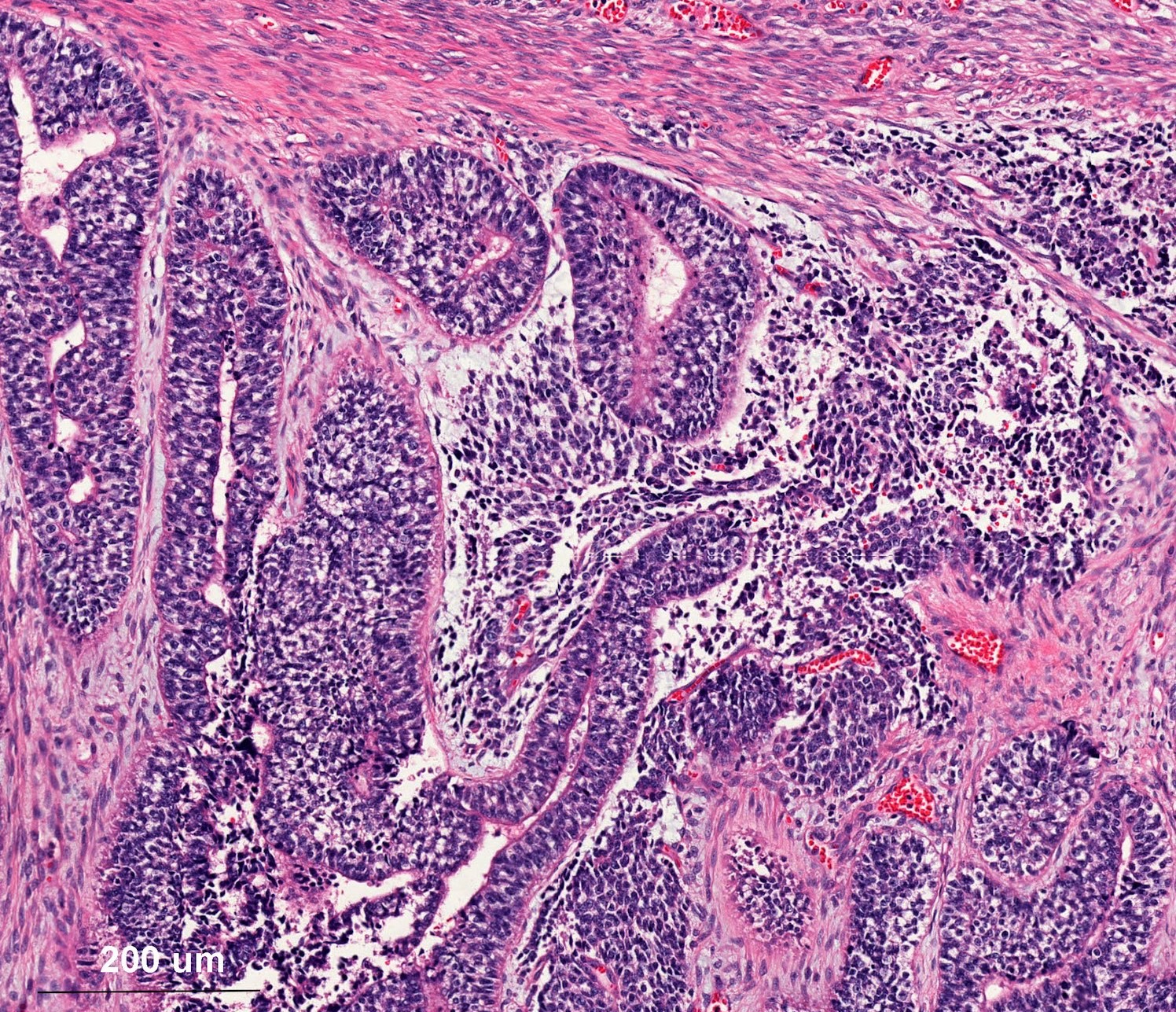
Epithelial and mesenchymal components
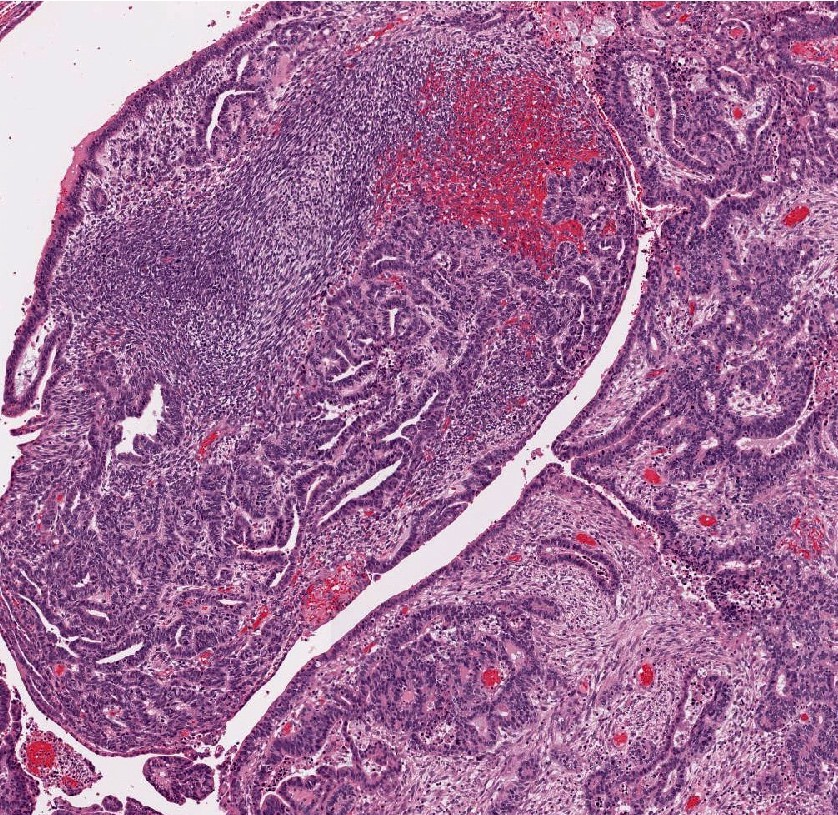

Glandular epithelium and blastematous stroma
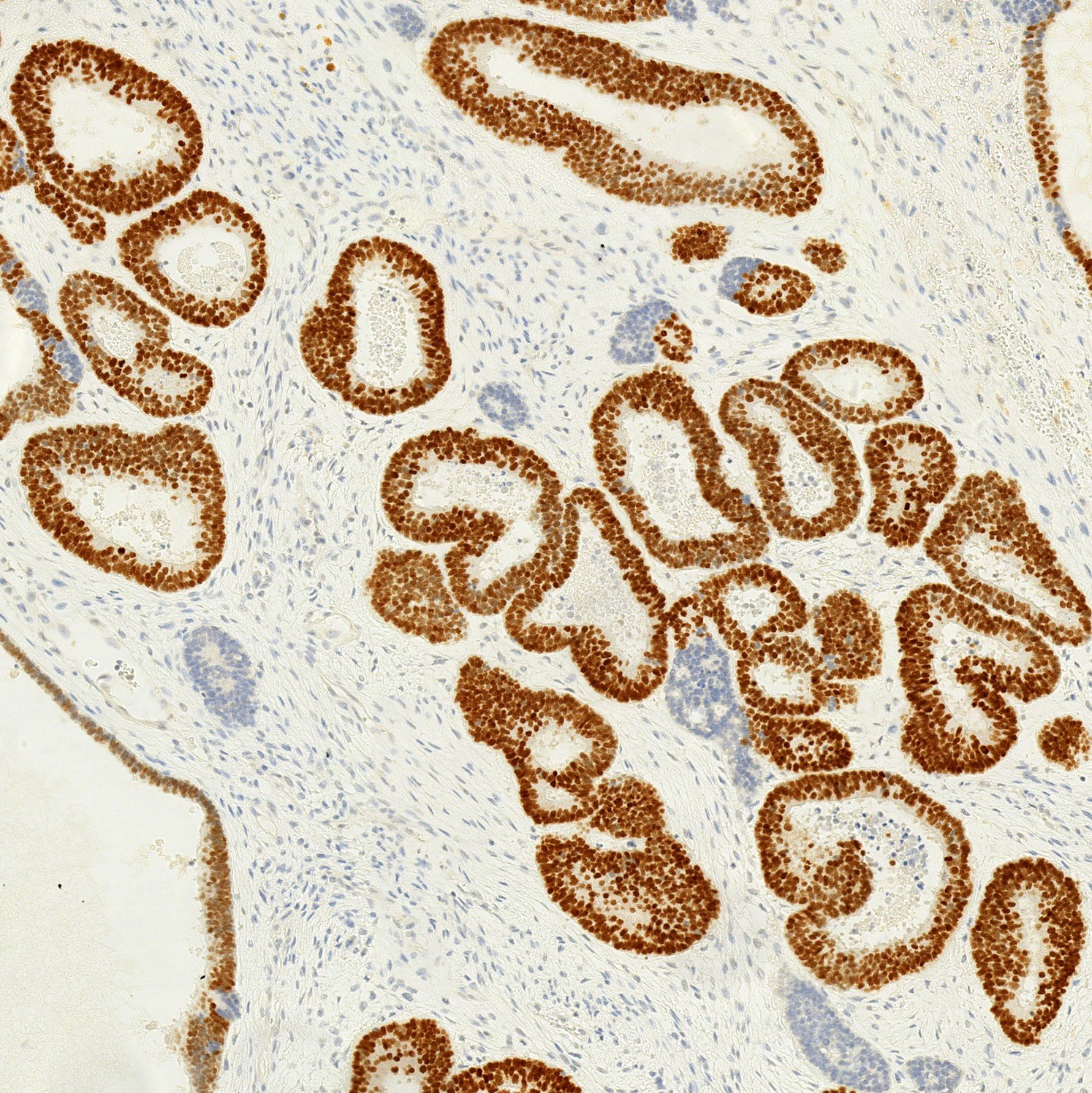
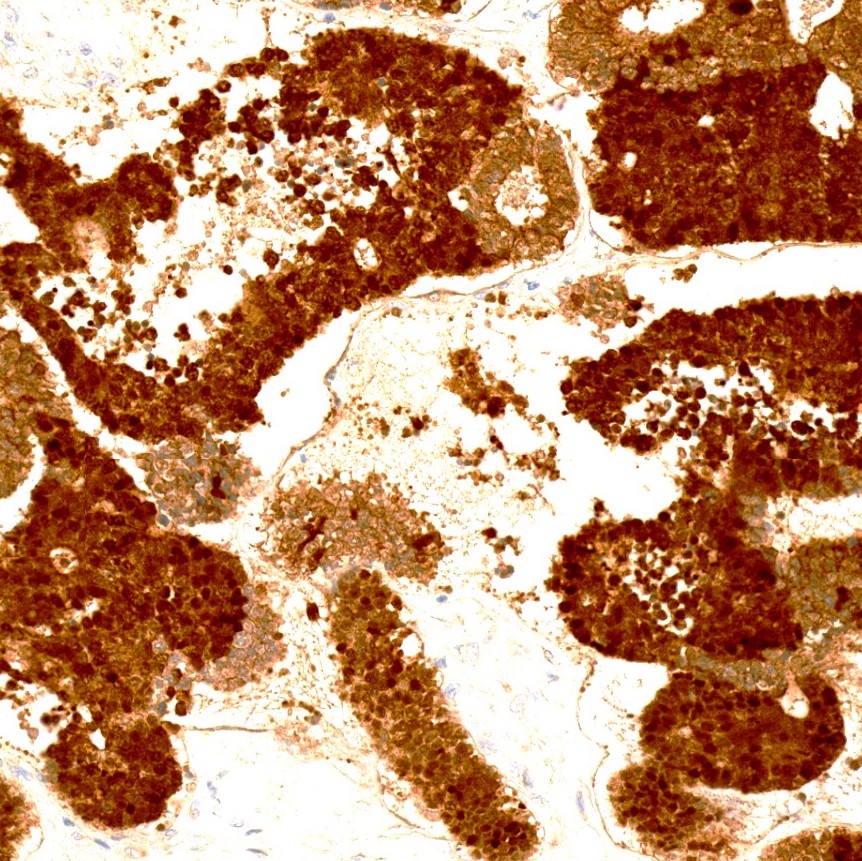
TTF1
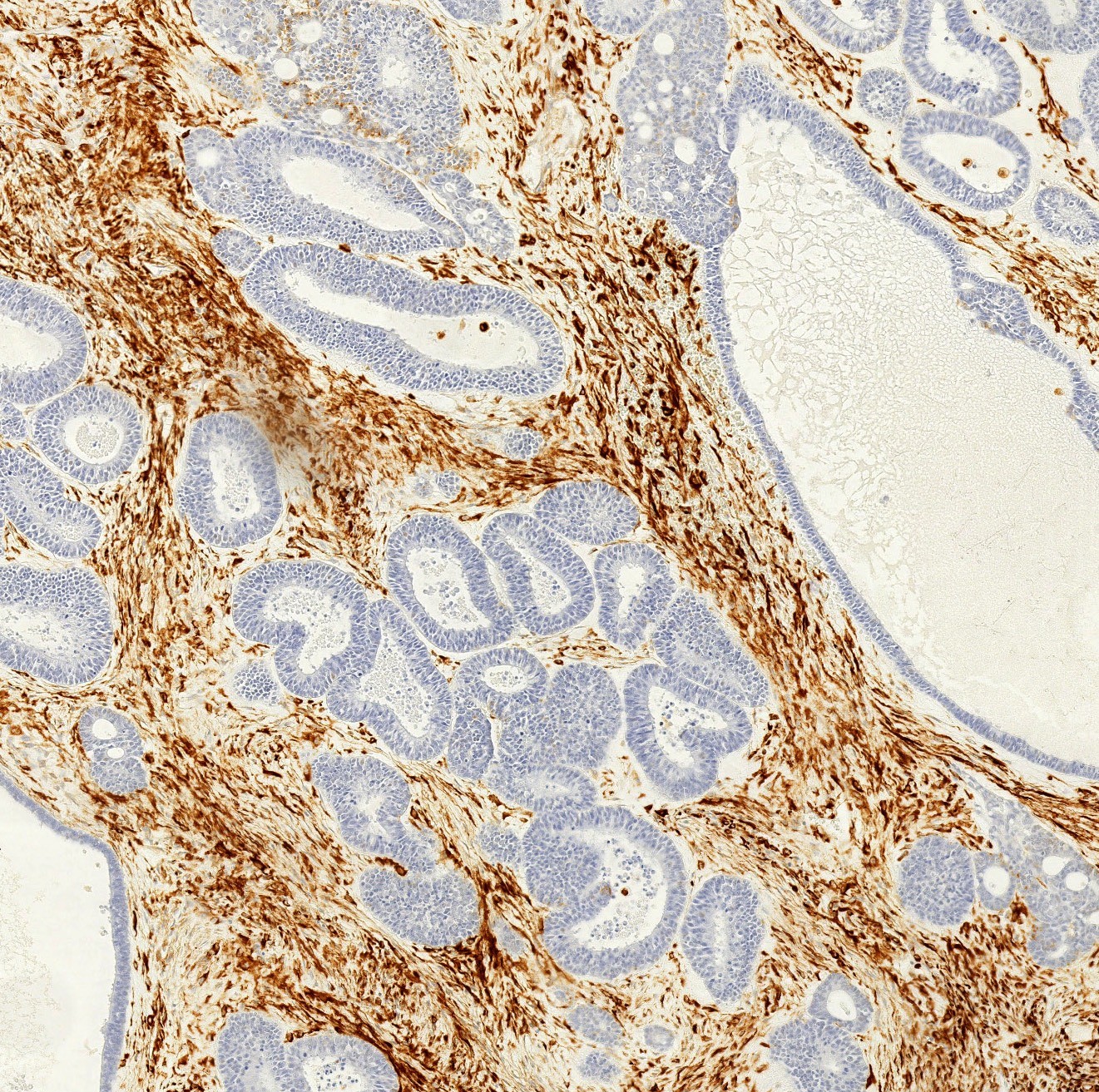
Vimentin
Beta catenin
Positive stains
- Glandular component: beta catenin (nuclear), CK7, AE1 / AE3, TTF1, CEA, synaptophysin, focal chromogranin (BMC Res Notes 2014;7:294, Lung Cancer 2011;73:127)
- Blastemal stromal component: beta catenin (nuclear), vimentin, SMA (BMC Res Notes 2014;7:294)
Negative stains
- Glandular component: vimentin (BMC Res Notes 2014;7:294)
- Blastemal stromal component: CAM 5.2, TTF1 (BMC Res Notes 2014;7:294)
Electron microscopy description
- Nuclear filaments and biotin rich products contribute to nuclear clearing (Ultrastruct Pathol 1995;19:501)
Molecular / cytogenetics description
- Exon 3 of CTNNB1 missense mutations, associated with morule formation (Am J Surg Pathol 2004;28:921, J Pathol 2003;200:214)
- 42% with TP53 mutation (Hum Pathol 1996;27:1117)
Sample pathology report
- Lung, right lower lobe, lobectomy:
- Pulmonary blastoma, 9 cm, margins negative for tumor (see comment)
- Comment: H&E sections demonstrate an admixture of malignant epithelial and mesenchymal components. Immunostains performed with adequate controls reveal that the glandular cells are strongly positive for pancytokeratin and TTF1. The stromal cells are vimentin positive. Beta catenin reveals nuclear staining in both epithelial and stromal components. The findings are consistent with the diagnosis of pulmonary blastoma, a subgroup of sarcomatoid carcinoma.
Differential diagnosis
- Fetal type adenocarcinoma:
- Epithelial component only, no blastematous stroma
- Pleuropulmonary blastoma:
- Pediatric tumor, most diagnosed before 4 years of age
- No epithelial component; admixture of blastematous and sarcomatoid components
- Epithelium (if seen) is benign entrapped respiratory type
- 40% with DICER1 mutation
- Biphasic synovial sarcoma:
- Glandular component lacks TTF1
- Focal cytokeratin, TLE1 positive, SS18::SSX fusion present
- Carcinosarcoma:
- Non-small cell carcinoma (squamous cell carcinoma or adenocarcinoma) and heterologous sarcomatous component
- Older age
- Absence of morules and no nuclear staining of beta catenin
Gene mutations commonly seen in different tumors
Note: +, present; -, absent
| CTNNB1 mutation | P53 mutation | DICER1 mutation | |
| Fetal adenocarcinoma | + | - | - |
| Pulmonary blastoma | + | + | Rare |
| Carcinosarcoma | - | + | - |
| Pleuropulmonary blastoma | - | + | + |
Additional references
Board review style question #1
- Which of the following is true for pulmonary blastoma?
- Associated with smoking
- Low to moderate grade tumor
- Lung counterpart of Wilms tumor
- Most common in young patients < 15 years old
- Mostly in a central location
Board review style answer #1
Board review style question #2
- What distinguishes pulmonary blastoma, shown here, from primary lung carcinosarcoma?
- Fewer mitotic figures
- Less common for metastasis
- Less cytologic atypia
- Less necrosis
- Nuclear immunostaining of beta catenin
Board review style answer #2
E. Pulmonary blastoma is positive for beta catenin, which is negative in lung carcinosarcoma
Comment Here
Reference: Pulmonary blastoma
Comment Here
Reference: Pulmonary blastoma
