Soft tissue
Skeletal muscle
Rhabdomyosarcoma
Pleomorphic rhabdomyosarcoma
Editorial Board Member: Nasir Ud Din, M.B.B.S.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 6 September 2022
Last staff update: 28 February 2024
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Pleomorphic rhabdomyosarcoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Kao E, Belzarena C. Pleomorphic rhabdomyosarcoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissuepleomorphicrhabdo.html. Accessed August 26th, 2025.
Definition / general
- High grade pleomorphic sarcoma composed of bizarre eosinophilic, round and spindle cells with skeletal muscle differentiation
- Exceedingly rare category of rhabdomyosarcoma (RMS) in adults
- Highly aggressive tumor associated with poor prognosis (Anticancer Res 2015;35:6213)
Essential features
- High grade sarcoma composed of atypical cells that display skeletal muscle differentiation, confirmed with immunohistochemistry for myogenin or myoD1
Terminology
- Pleomorphic rhabdomyosarcoma
ICD coding
- ICD-O: 8901/3 - pleomorphic rhabdomyosarcoma, NOS
- ICD-11: 2B55 & XH5SX9 - rhabdomyosarcoma, primary site & pleomorphic rhabdomyosarcoma, NOS
Epidemiology
- Usually in the sixth to seventh decade
- Male predominance (1.8:1) (Anticancer Res 2015;35:6213)
Sites
- Deep soft tissues
- Most common in extremities (Anticancer Res 2015;35:6213)
- Less common locations include the pelvis, abdomen, thorax and head and neck (Anticancer Res 2015;35:6213)
Pathophysiology
- Complex karyotype but no signature genetic alteration
Etiology
- Unknown
Clinical features
- Rapidly growing, painful deep mass, most commonly of lower extremity
- Nodal involvement uncommon (< 10%)
- Majority of patients (70%) with localized disease at presentation (Anticancer Res 2015;35:6213)
Diagnosis
- Pleomorphic cells with brightly eosinophilic cytoplasm (Mod Pathol 2001;14:595)
- Skeletal muscle differentiation as confirmed by desmin, myogenin or MyoD1 (Ann Diagn Pathol 2018;36:50)
- Thorough histologic sampling and evaluation are necessary for diagnostic confirmation
Radiology description
- In MRI T1 weighted sequences, the tumor appears iso or hypointense to muscle
- In T2 weighted and STIR sequences, the tumor is hyperintense with surrounding edema
- In postcontrast sequences, the mass shows heterogeneous enhancement; necrosis is usually present within
- Reference: AJR Am J Roentgenol 2007;189:371
Radiology images
Contributed by Erdener Özer, M.D., Ph.D.
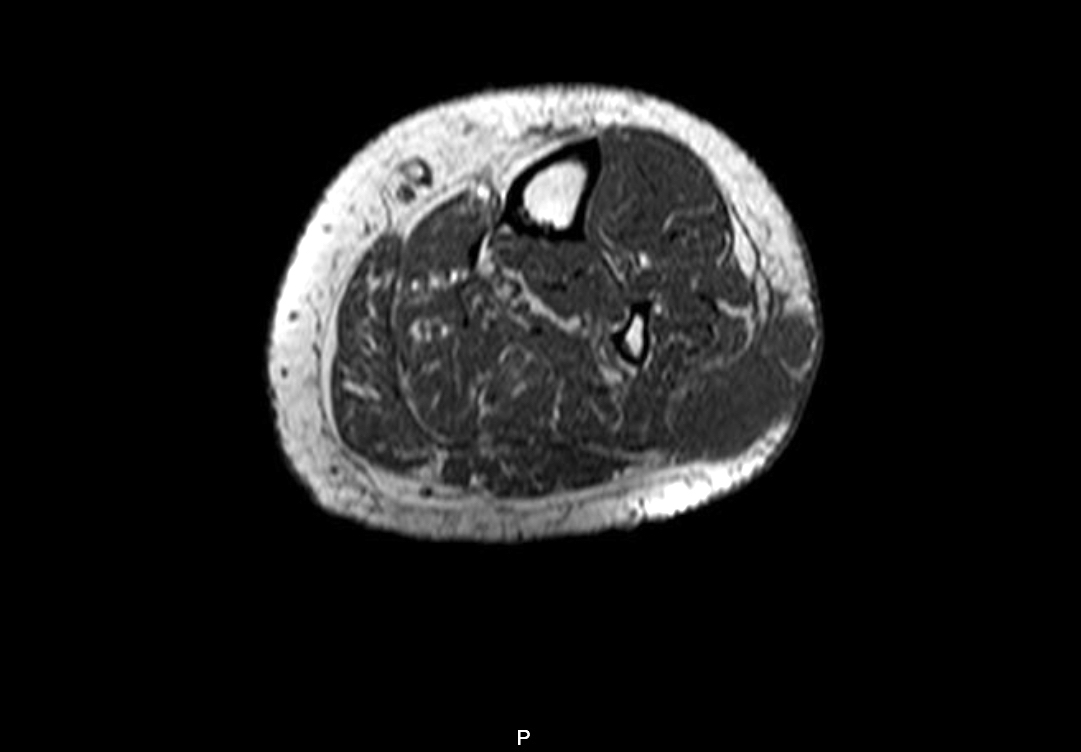
MRI
Images hosted on other servers:

MRI

Adductor brevis
Prognostic factors
- High propensity for metastatic spread
- Lungs are the most common site for metastases (77%)
- Positive margins associated with disease relapse (Anticancer Res 2015;35:6213)
- Tumors with superficial location (~20%) have a more favorable outcome
Case reports
- 28 year old man with pleomorphic rhabdomyosarcoma of the thigh (Oncol Lett 2016;12:1921)
- 50 year old man with pleomorphic rhabdomyosarcoma in subcutaneous tissue of the trunk (J Dermatol 2017;44:59)
- 53 year old woman with 3 synchronous lung metastasis from pleomorphic rhabdomyosarcoma (Cancer Treat Res Commun 2021;26:100282)
- 57 year old woman with pleomorphic rhabdomyosarcoma of the chest wall (Int J Surg Case Rep 2020;75:380)
- 60 year old man with pleomorphic rhabdomyosarcoma of the thigh (J Community Hosp Intern Med Perspect 2020;10:287)
- 73 year old woman with pleomorphic rhabdomyosarcoma of the uterus (Anticancer Res 2017;37:2509)
Treatment
- Clinical behavior and responsiveness to chemotherapy are similar to adult high grade soft tissue sarcomas
- Poor prognosis with median survival of 7 months
- Surgical resection with wide margins is mainstay of treatment
- Stereotactic body radiation therapy (SBRT) has been used for lung oligometastases (Cancer Treat Res Commun 2021;26:100282)
Gross description
- Can be variable in size (median 8 cm, range from 1 - 30 cm) (Am J Surg Pathol 2009;33:1850)
- Cut surface with variable hemorrhage and necrosis
- Appears circumscribed, often in deep soft tissue and involving striated muscle (Am J Surg Pathol 2009;33:1850)
Gross images
Contributed by Debra Zynger, M.D.
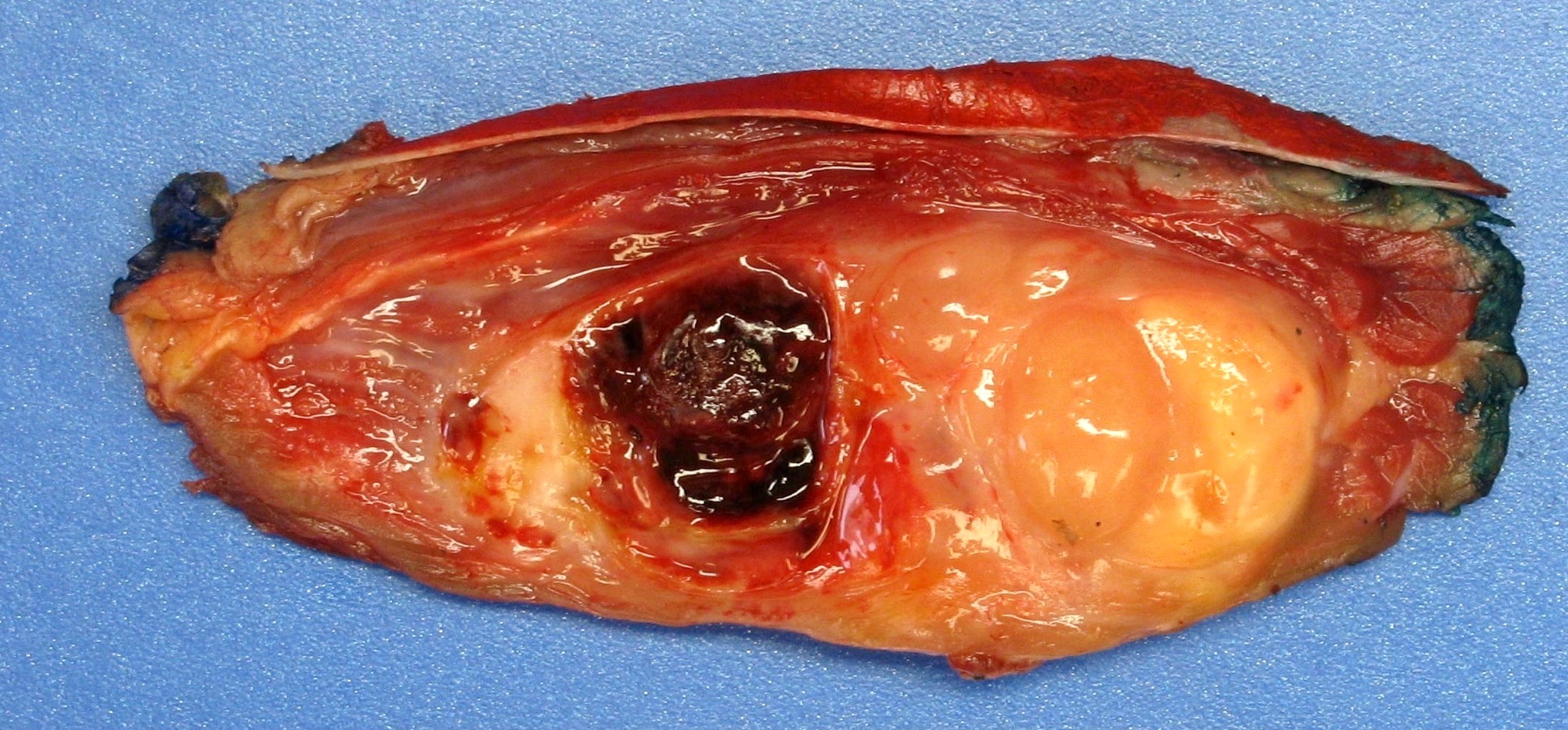
Seemingly circumscribed thigh mass

Variable hemorrhage

Variable necrosis
Images hosted on other servers:

Paratesticular tumors

Resected tumor
Microscopic (histologic) description
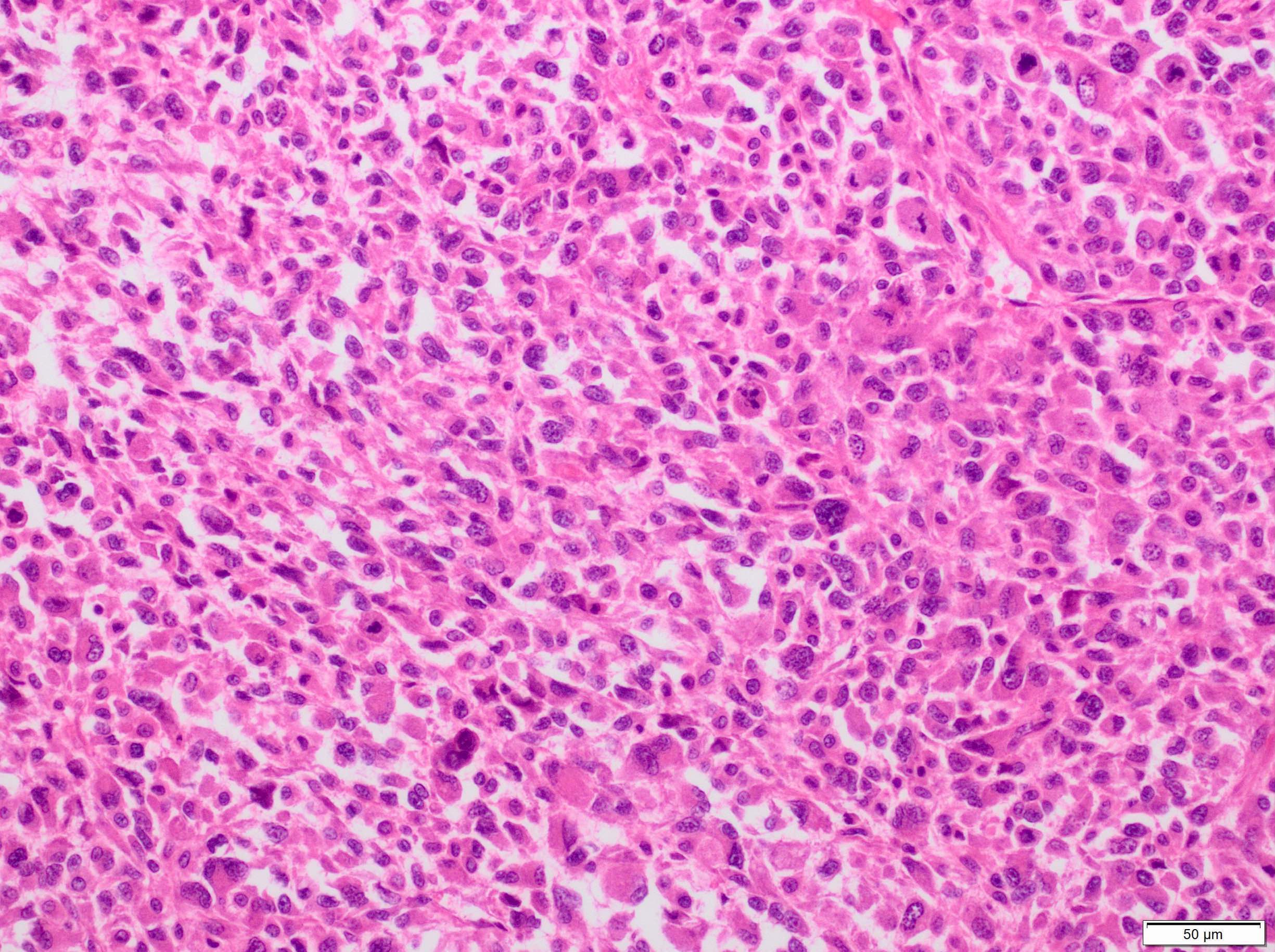
- Sheets of large, atypical and frequently multinucleated polygonal, spindled or rhabdoid eosinophilic cells (Am J Surg Pathol 2009;33:1850)
- Cross striations are seldom detected
Microscopic (histologic) images
Contributed by Burcin Tuna, M.D. and AFIP
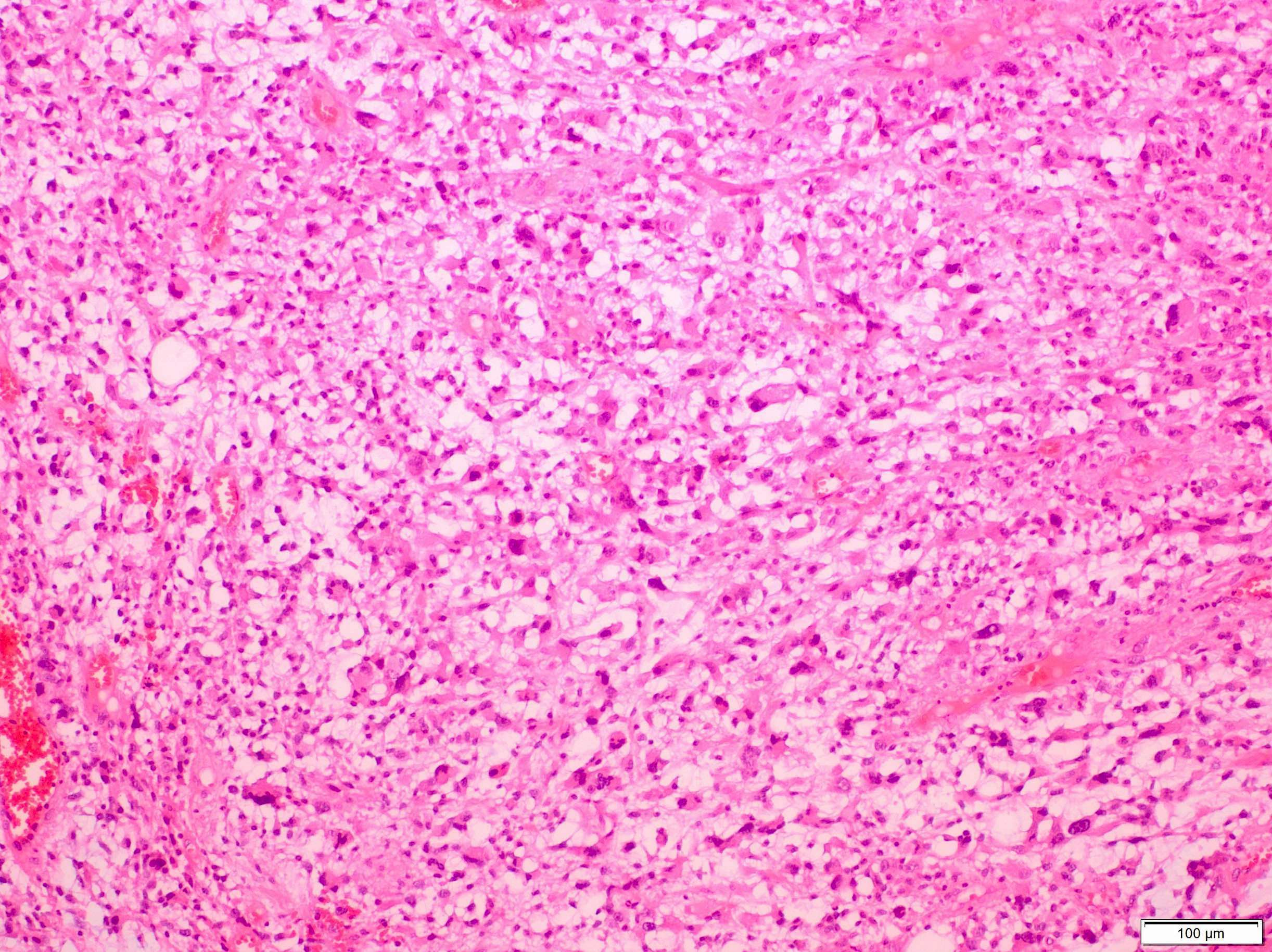
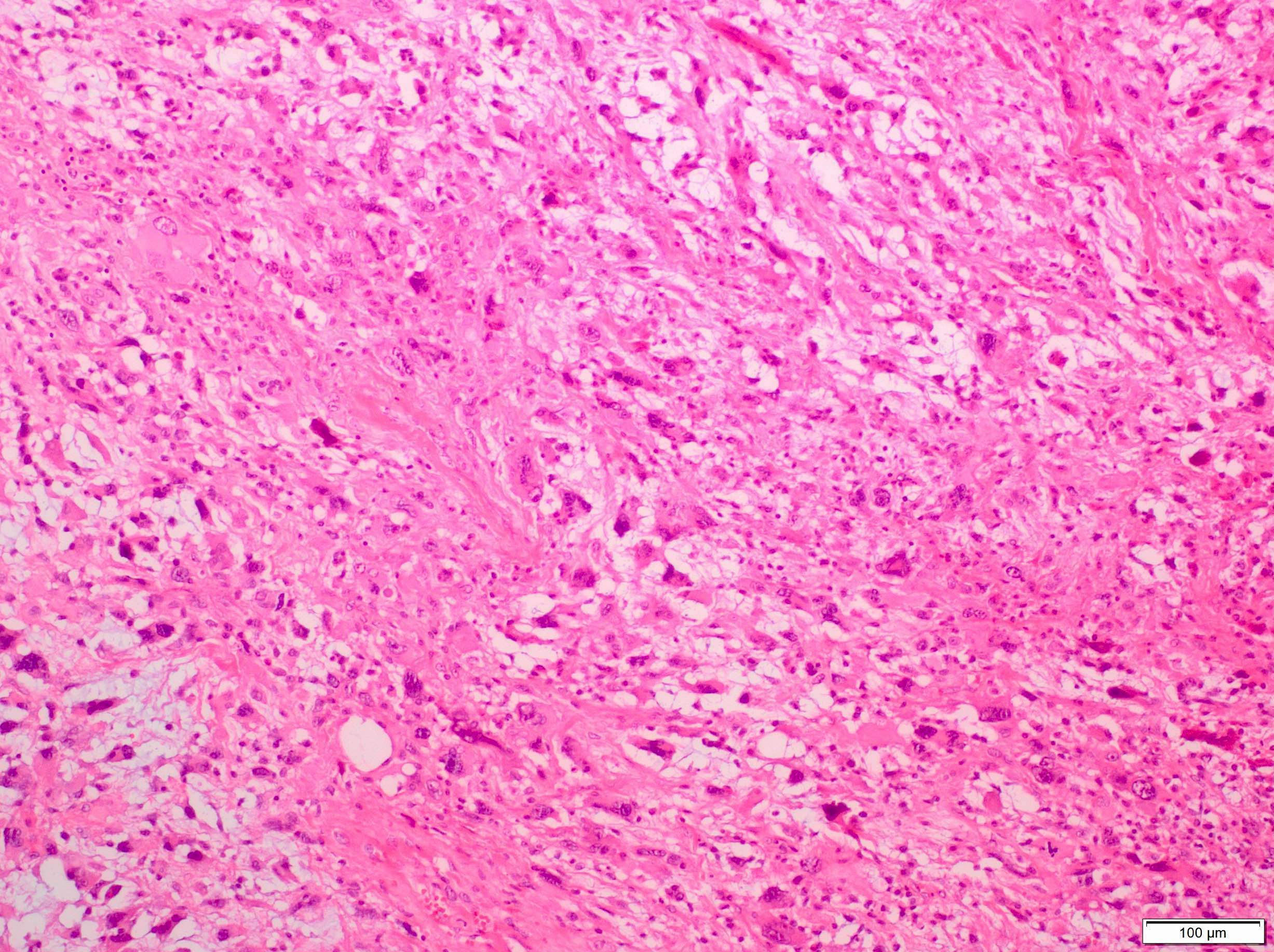
Bizarre, eosinophilic multinucleated cells
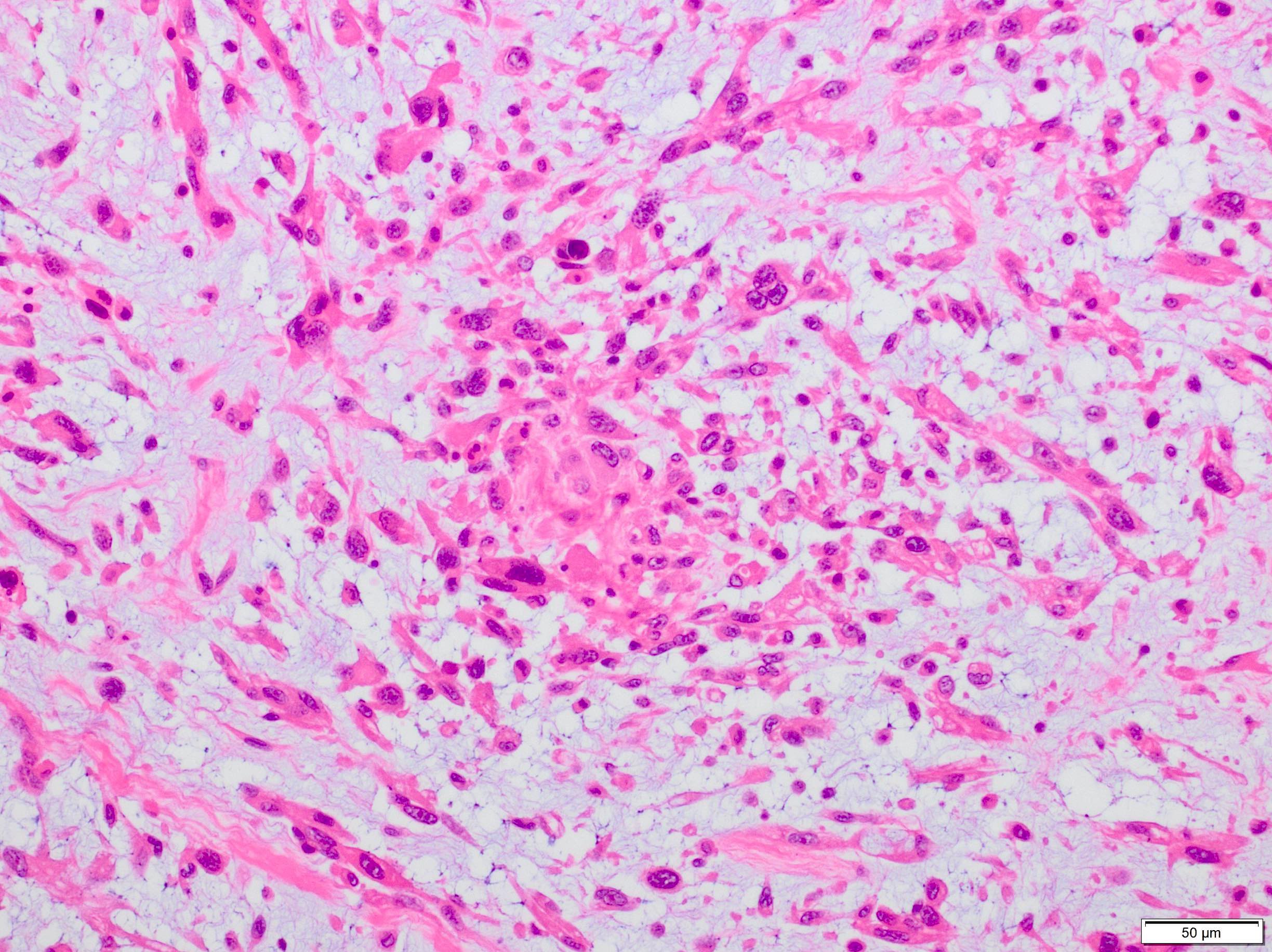
Rhabdomyoblasts
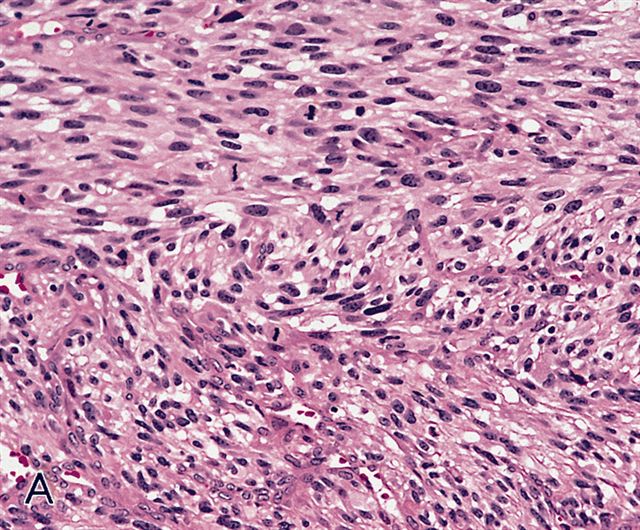
Fascicular pattern
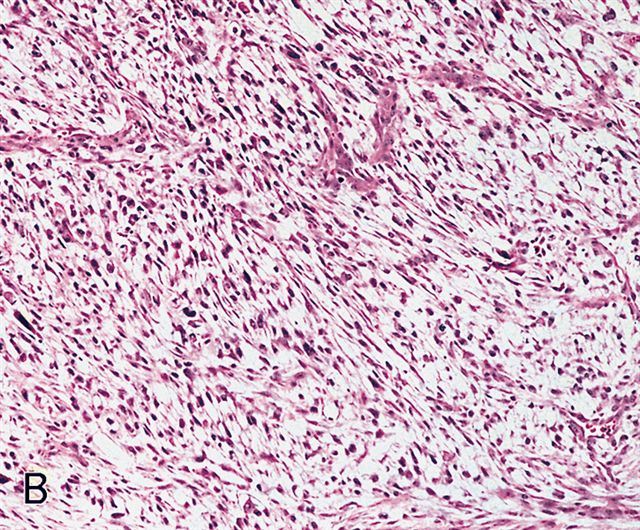
Storiform pattern
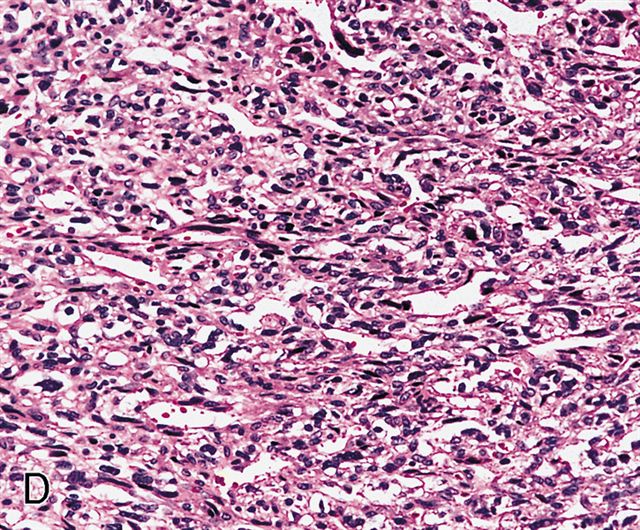
Patternless pattern

Spindle cells
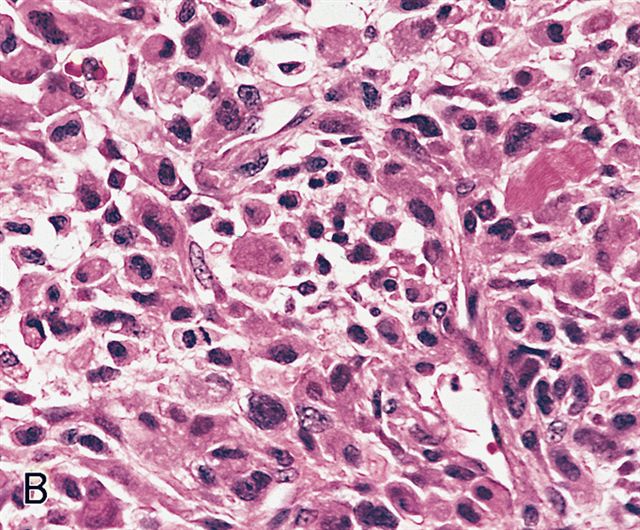
Pleomorphic and polygonal cells
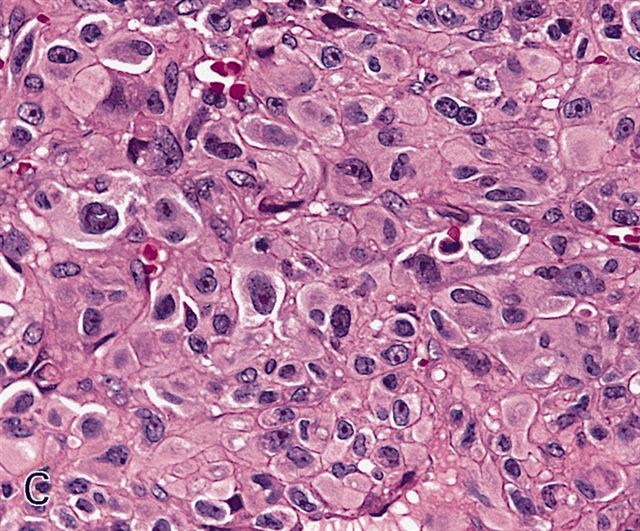
Epithelioid cells with abundant eosinophilic cytoplasm
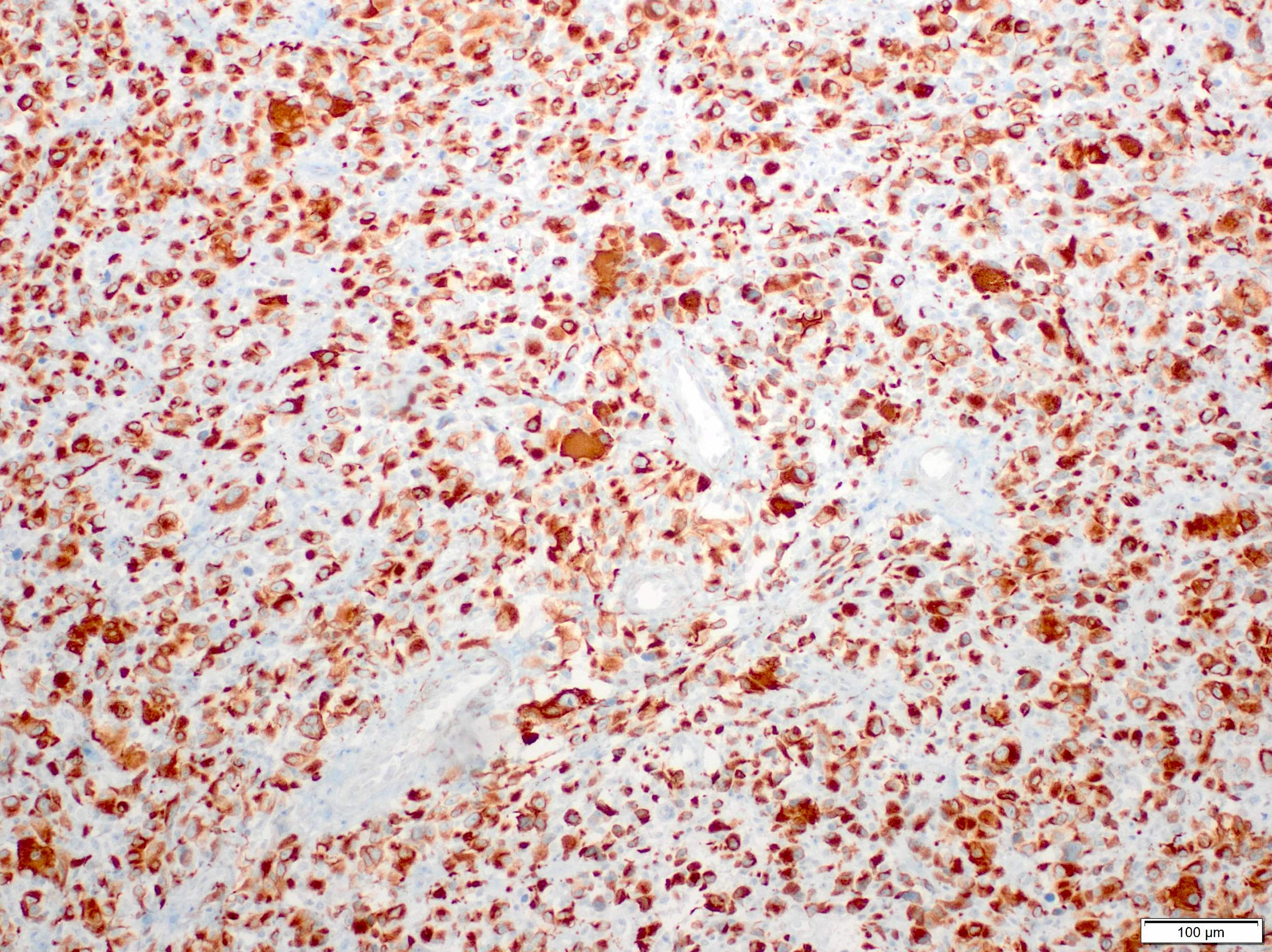
Desmin
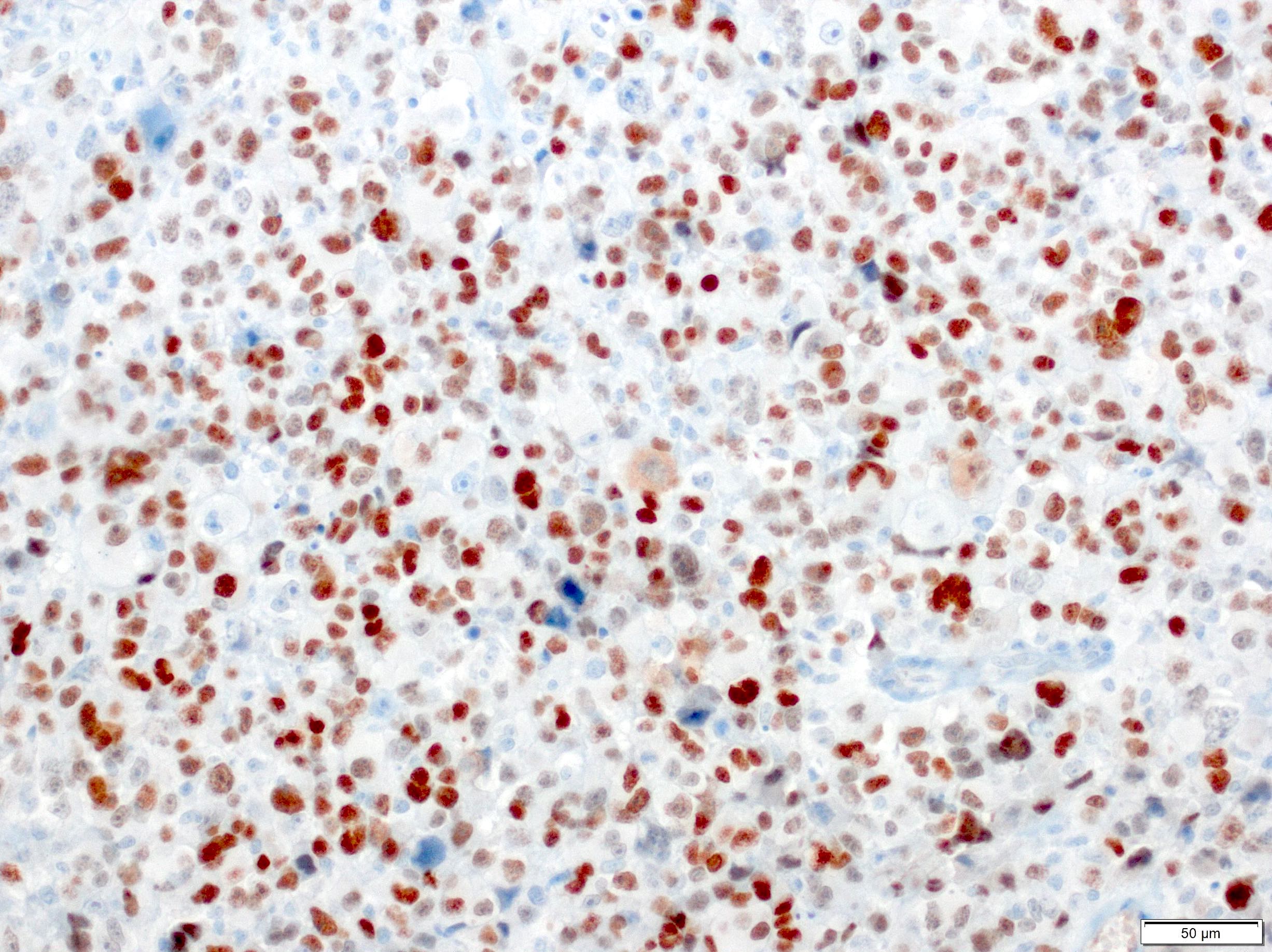
MyoD1
Positive stains
- Expresses desmin, MyoD1, skeletal muscle (fast) myosin and myogenin (Mod Pathol 2001;14:595)
- Variable SMA and may have focal keratin AE1 / AE3 and EMA positivity (Am J Surg Pathol 2009;33:1850)
Electron microscopy description
- Skeletal muscle differentiation with rudimentary sarcomeres containing Z bands or Z band material with thick and thin filaments (Mod Pathol 2001;14:595)
Molecular / cytogenetics description
- Complex karyotype (Cancer Genet Cytogenet 2009;192:1)
- Comparative genomic in situ hybridization (CGH) reveals 8 highly amplified regions at 1p36.1-p36.2, 1p31-p32, 1q21-q31, 8q12-q21, 8q24-qter, 11q12-q13, 12q13-q14 and 18q12-q22 (Am J Cancer Res 2012;2:141)
Sample pathology report
- Soft tissue, biopsy:
- Pleomorphic sarcoma with rhabdomyoblastic differentiation (see comment)
- Comment: These findings may represent a pleomorphic rhabdomyosarcoma, although heterologous differentiation cannot be excluded.
Differential diagnosis
- Embryonal or alveolar rhabdomyosarcoma with anaplastic features:
- No evidence of embryonal or alveolar component which may have scattered pleomorphic cells or solid foci of pleomorphic cells (Am J Surg Pathol 1993;17:601)
- Embryonal RMS has ovoid to spindle cells, typically occurs in the pediatric population but can be in adults, and has a predilection for the head and neck and genitourinary system (Pediatr Blood Cancer 2021;68:e28798)
- Alveolar RMS tumor cells are arranged in nests separated by fibrovascular septa, which frequently exhibit loss of cellular cohesion in the center, conferring a pattern of irregular alveolar spaces; the presence of either a PAX3::FOXO1 or a PAX7::FOXO1 fusion gene is detected in the majority of alveolar RMS cases
- Pleomorphic RMS prefers older adults and occurs in the extremities (Am J Surg Pathol 2009;33:1850)
- No evidence of embryonal or alveolar component which may have scattered pleomorphic cells or solid foci of pleomorphic cells (Am J Surg Pathol 1993;17:601)
- Undifferentiated pleomorphic sarcoma:
- Diagnosis of exclusion
- No evidence of skeletal muscle differentiation
- Pleomorphic liposarcoma:
- No evidence of skeletal muscle differentiation
- Carcinomas with rhabdomyosarcomatous differentiation, such as malignant mixed Müllerian tumor:
- Carcinomatous component present
- Melanoma with rhabdomyosarcomatous dedifferentiation (Am J Surg Pathol 2016;40:181):
- Presence of BRAF mutation, history of melanoma with current presentation of tumor in a characteristic site of metastasis (lymph node, lung, etc.)
- Sarcomas with heterologous rhabdomyoblastic differentiation, such as dedifferentiated liposarcoma or MPNST (malignant Triton tumor):
- Histologic or molecular evidence of another tumor (i.e., MDM2 amplification present for dedifferentiated liposarcoma or a well differentiated liposarcoma component present), loss of H3K27me3 in MPNST or areas of more classic appearing MPNST arising from a nerve
Additional references
Practice question #1
Which of the following is true for pleomorphic rhabdomyosarcoma?
- A t(2;13)(q36;q14) translocation is found in the majority of alveolar rhabdomyosarcoma
- Composed of an embryonal component
- May express pankeratin
- Tumor cells often display cross striations
- Usually are tumors of children
Practice answer #1
A. A t(2;13)(q36;q14) translocation is found in the majority of alveolar rhabdomyosarcoma
Comment Here
Reference: Pleomorphic rhabdomyosarcoma
Comment Here
Reference: Pleomorphic rhabdomyosarcoma
Practice question #2
Which rhabdomyosarcoma type is more predominant in adults in the sixth to seventh decades and is characterized by the presence of pleomorphic cells with a significant amount of bright eosinophilic cytoplasm?
- Alveolar rhabdomyosarcoma
- Embryonal rhabdomyosarcoma
- Pleomorphic rhabdomyosarcoma
- Spindle cell / sclerosing rhabdomyosarcoma
Practice answer #2
