

Bladder & urothelial tract
Glandular neoplasms
Villous adenoma
Author: Varsha Manucha, M.D.
Editorial Board Member: Maria Tretiakova, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 13 January 2021
Last staff update: 19 November 2021
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Villous adenoma[TIAB] bladder
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Manucha V. Villous adenoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bladdervillousadenoma.html. Accessed May 13th, 2024.
Definition / general
- Rare bladder tumor similar to colonic counterpart
Essential features
- Villous adenoma of the urinary tract is a rare but important lesion
- Morphologic features of these tumors are similar to those of colonic adenomas
- Villous adenoma of the urinary tract should be removed completely and sampled thoroughly to avoid missing a more aggressive component
Terminology
- Also called villous tumor
ICD coding
- ICD-O: 8261/0 - villous adenoma, NOS
Epidemiology
- Rare
- Older patients (Int J Urol 2008;15:551)
- M > F (Hum Pathol 2002;33:236)
- Wide age range (40 - 70 years)
Sites
- Urinary bladder, urachus, renal pelvis, ureter and urethra (Am J Surg Pathol 1999;23:764)
- In bladder, dome and the posterior wall, followed by urachus and trigone are common sites (Hum Pathol 2002;33:236)
Pathophysiology
- Mechanism underlying the origin of villous adenoma of the urinary bladder is still speculative (Mod Pathol 2009;22:1280)
- It has been suggested that a cloacal rest may remain in the bladder and subsequently proliferate into a glandular neoplasm (Am J Surg 1955;90:693)
- Alternative theory suggests that villous adenoma is the product of a chronic irritation metaplasia → dysplasia → carcinoma sequence (J Clin Pathol 1993;46:450)
Clinical features
- Hematuria, mucosuria and irritative symptoms (Am J Surg Pathol 1999;23:764, Hum Pathol 2002;33:236, BMC Urol 2013;13:36)
- May be associated with in situ or invasive adenocarcinoma at diagnosis, less often with in situ or invasive urothelial carcinoma
Diagnosis
- Cystoscopic findings with tissue resected
- Imaging or colonoscopy findings to rule out a colonic malignancy
- Thorough microscopic examination of excised tissue
Radiology description
- No specific findings on ultrasonography, CT or MRI
Prognostic factors
- Excellent prognosis if isolated, poorer if only in situ adenocarcinoma, poorest if in situ or invasive urothelial carcinoma (Hum Pathol 2002;33:236)
Case reports
- 45 year old woman with polypoid mass in posterolateral wall of urinary bladder (J Cancer Res Ther 2015;11:665)
- 63 year old woman with focal well differentiated adenocarcinoma of urethral orifice (World J Clin Cases 2019;7:891)
- 85 year old woman with nonmuscle invasive bladder cancer (BMC Urol 2013;13:36)
- 90 year old woman with tubulovillous architecture arising in the diverticulum (Pol J Pathol 2011;62:179)
- Villous adenoma arising in the native bladder mucosa and the upper urinary tract with coexisting neuroendocrine carcinoma (Int J Surg Pathol 2019;27:450)
Treatment
- Complete excision
- Excellent prognosis if isolated (Am J Surg Pathol 1999;23:764)
- Coexisting infiltrating carcinoma or urothelial carcinoma suggests a more aggressive course
Gross description
- Resembles papillary urothelial carcinoma
Microscopic (histologic) description
- Resembles colonic villous adenoma with pointed processes lined by pseudostratified columnar epithelium with nuclear stratification, nuclear crowding, nuclear hyperchromasia, occasional prominent nucleoli, occasional mitoses (Arch Pathol Lab Med 2016;140:91)
- Chronic cystitis with intestinal type glandular metaplasia and extensive cellular atypia (dysplasia) in the flat mucosa may be seen
- Must sample entire lesion to rule out adenocarcinoma (in situ or invasive)
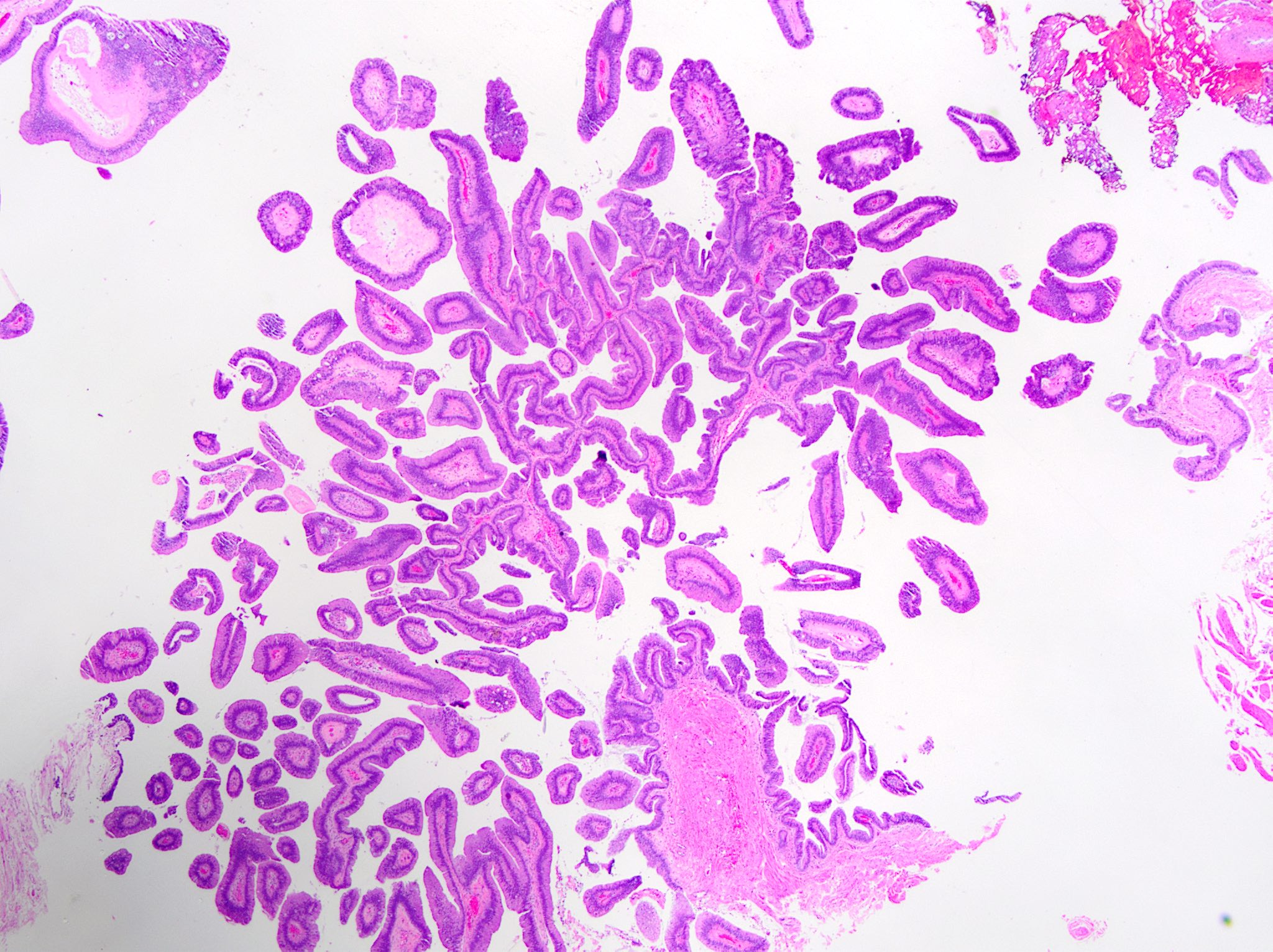
Microscopic (histologic) images
Contributed by Varsha Manucha, M.D.
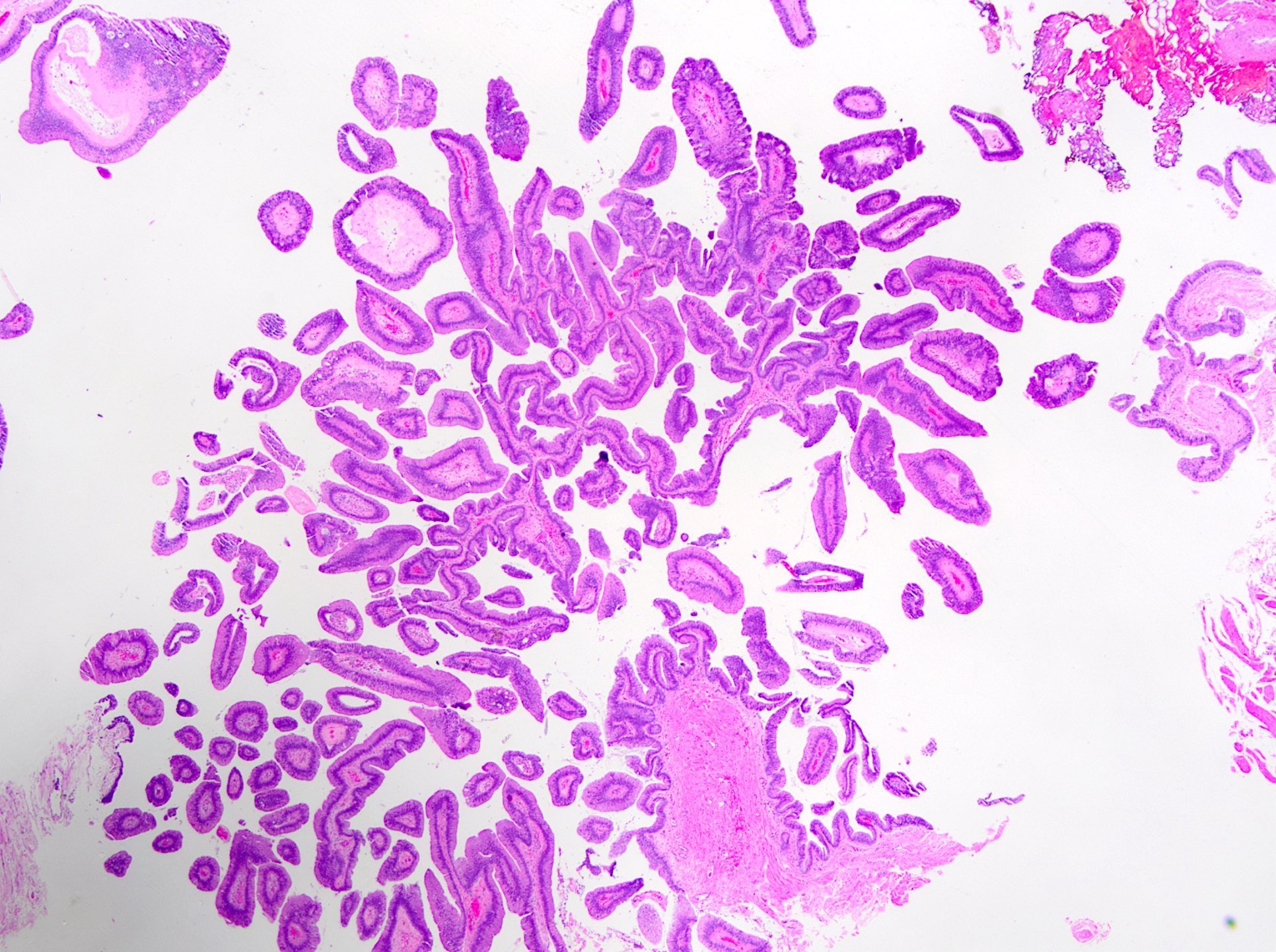
Villous adenoma
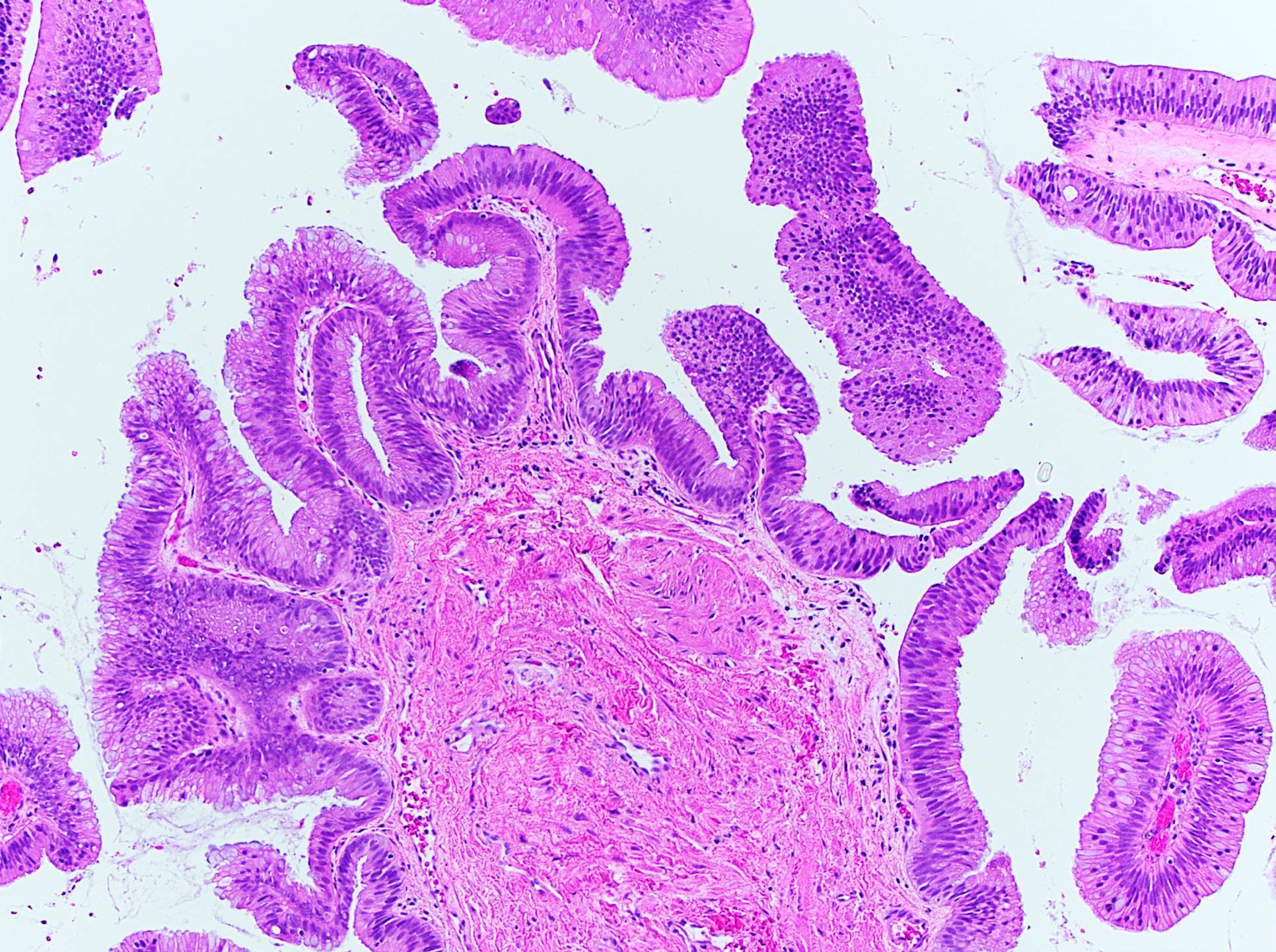
Villous pattern


Nuclear stratification
Cytology description
- Urine cytology may show mucin producing cells or cell clusters with gland formation or arrangement along basement membrane
- When glandular cells with columnar mucin filled goblet cells are seen in urine cytology, the presence of a primary glandular lesion of the urinary bladder, such as villous adenoma, should be considered possible (Diagn Cytopathol 2016;44:632)
Positive stains
- CK20 (100%)
- CDX2 (100%)
- CEA (luminal, 89%)
- Acidic mucins (Alcian blue)
- CK7 (56%) (Am J Surg Pathol 2008;32:1322)
Negative stains
- EMA, beta catenin (is not nuclear), thrombomodulin
- Variable PSMA
- GATA3, PAX8
Sample pathology report
- Bladder, transurethral resection:
- Villous adenoma (negative for carcinoma in situ or invasive carcinoma)
- Muscularis propria is present and is negative for neoplasia
Differential diagnosis
- Adenocarcinoma in situ arising in villous adenoma:
- Psuedostratification, loss of polarity, increased pleomorphism with vesicular and round nuclei
- Intraluminal cribriforming
- No invasion
- Colonic adenocarcinoma, well differentiated extending into bladder:
- Clinical history of colonic tumor
- Definite invasion identified
- Usually beta catenin nuclear positive
- Papillary urothelial carcinoma with villoglandular differentiation:
- Typically has concurrent high grade papillary urothelial carcinoma component
- GATA3 positive
- Nephrogenic adenoma, papillary variant:
- Has bland cytology
- PAX8 positive
Board review style question #1
A urinary bladder villous adenoma is most likely to show which of the following immunohistochemical profiles?
- CK7+, CK20+, beta catenin (nuclear)+, thrombomodulin+
- CK7-, CK20+, beta catenin (nuclear)+, thrombomodulin-
- CK7+, CK20+, beta catenin (nuclear)-, thrombomodulin-
- CK7+, CK20-, beta catenin (nuclear)-, thrombomodulin+
Board review style answer #1
C. CK7+, CK20+, beta catenin (nuclear)-, thrombomodulin-. The immunohistochemical profile of villous adenoma has been reported to be positive for CK20 and CEA, and ~50% of cases of urinary tract villous adenomas exhibit positive results for CK7. It is very important to distinguish from metastatic adenocarcinoma derived from the colon. Most of the cases of adenocarcinoma derived from the colon are reported to be positive for beta catenin (nuclear staining) and negative for thrombomodulin and CK7, while urothelial carcinoma cases are positive for CK7, thrombomodulin and negative for beta catenin (nuclear staining).
Comment Here
Reference: Villous adenoma
Comment Here
Reference: Villous adenoma
Board review style question #2
A 50 year old man with a long term history of urethral stricture and chronic cystitis presents with mucosuria. Cystoscopy reveals a papillary growth which is biopsied and is diagnosed as villous adenoma of the urinary bladder. What is the best treatment option for the patient?
- Bacillus Calmette-Guérin (BCG) therapy
- Chemotherapy
- Close followup
- Complete excision
Board review style answer #2
D. Complete excision. Pure and isolated villous adenomas have an excellent prognosis, even without radical resection. However, urinary tract villous adenomas have also been found in association with in situ or invasive adenocarcinoma, squamous cell carcinoma and flat in situ urothelial carcinoma. In these cases, the lesions have sometimes been clinically more aggressive, with disease recurrence or even distant metastasis. The heterogeneity of the lesions associated with urinary tract villous adenomas has important implications for diagnosis and management. Any urinary tract lesion diagnosed by biopsy as villous adenoma must be completely excised and thoroughly sampled.
Comment Here
Reference: Villous adenoma
Comment Here
Reference: Villous adenoma
